DAI LY LI FE OF PATI ENTS W I TH CHRONI C RENAL FAI LURE RECEI VI NG
HEMODI ALYSI S TREATMENT
Kar in a Viv ian i Bezer r a1
Jair Lício Fer r eir a Sant os2
Bezer r a KV, Sant os JLF. Daily life of pat ient s w it h chr onic r enal failur e r eceiv ing hem odialy sis t r eat m ent . Rev Lat ino- am Enfer m agem 2 0 0 8 j ulho- agost o; 1 6 ( 4 ) : 6 8 6 - 9 1 .
Th is an aly t ical d escr ip t iv e st u d y aim ed at assessin g t h e p er cep t ion of p eop le w it h ch r on ic r en al f ailu r e in
r elat ion t o t heir daily and occupat ional act ivit ies. The sam ple w as for m ed by 35 m en and 35 w om en r eceiving
hem odialysis t r eat m ent w it h ages bet w een 17 and 60 year s. The inst r um ent used w as t he SAOF ( Self Assessm ent
of Occupat ional Funct ioning) . The dat a w er e subm it t ed t o st at ist ical analysis and t he ar eas w it h gr eat er choice
of t he alt er nat iv e “ need t o im pr ov e” w er e habit s ( 2 0 % ) and v alues ( 2 0 . 5 % ) . I n t hese ar eas, t he pr opor t ion
r elat ed w it h difficult ies w as m or e ev ident r egar ding or ganizat ion of t he daily life, t he changes of r out ines and
t h e ex pect at ion s abou t t h e fu t u r e. Th er efor e, occu pat ion al t h er apy , as it pr esen t s in st r u m en t al r esou r ces t o
r eor ganize daily life of t hese pat ient s, can cont r ibut e for t heir car e as w ell as w it h infor m at ion for nur sing.
DESCRI PTORS: r enal insufficiency , chr onic; r enal dialy sis; act iv it ies of daily liv ing
EL DÍ A A DÍ A DE PERSONAS CON I NSUFI CI ENCI A RENAL CRÓNI CA EN TRATAMI ENTO
DE HEMODI ÁLI SI S
Est e est udio analít ico- descr ipt iv o t iene com o obj et iv o ev aluar la per cepción de las per sonas con insuficiencia
r en al cr ón ica en r elación con las act iv id ad es cot id ian as y ocu p acion ales. El an álisis f u e com p u est o p or 3 5
hom br es y 35 m uj er es en t r at am ient o de hem odiálisis con edad ent r e 17 y 60 años. El cuest ionar io ut ilizado
fue el SAOF ( Self Asesm ent of Occupat ional Funct ioning) . Los dat os fuer on som et idos a análisis est adíst ico y las
opciones que fuer on las m ás escogidas en la alt er nat iv a “ necesidad de m ej or ar ” fuer on la de hábit os ( 20% ) y
v alor es ( 2 0 , 5 % ) . En esas ár eas la pr opor ción r elacion ada a las dif icu lt ades f u e m ás ev iden t e en lo qu e se
r efier e a la or ganización de lo cot idiano, a cam bios de r ut inas y las ex pect at ivas sobr e el fut ur o. Por lo t ant o,
la t er apia ocupacional, por pr esent ar r ecur sos inst r um ent ales par a la r eest r uct ur ación de lo cot idiano de esos
pacient es, puede cont r ibuir par a asist ir los, así com o ent r egar infor m aciones im por t ant es par a la enfer m er ía.
DESCRI PTORES: insuficiencia r enal cr ónica; diálisis r enal; act iv idades cot idianas
O COTI DI AN O DE PESSOAS COM I N SUFI CI ÊN CI A REN AL CRÔN I CA EM
TRATAMENTO HEMODI ALÍ TI CO
Est e est udo analít ico- descr it iv o obj et iv ou av aliar a per cepção das pessoas com insuficiência r enal cr ônica em
r elação às at iv idades cot idian as e ocu pacion ais. A an álise f oi com post a por 3 5 h om en s e 3 5 m u lh er es em
t r at am ent o hem odialít ico com idade ent r e 17 e 60 anos. O quest ionár io ut ilizado foi o SAOF ( Self Assesm ent of
Occupat ional Funct ioning) . Os dados for am subm et idos à análise est at íst ica e as ár eas com m aior escolha da
alt er nat iv a “ necessidade de m elhor a” for am de hábit os ( 20% ) e v alor es ( 20, 5% ) . Nessas ár eas, a pr opor ção
r elacion ada às dif icu ldades f oi m ais ev iden t e n o qu e se r ef er e à or gan ização do cot idian o, a m u dan ças de
r ot inas e às expect at ivas quant o ao fut ur o. Por t ant o, a t er apia ocupacional, por apr esent ar r ecur sos inst r um ent ais
p ar a a r eest r u t u r ação d o cot id ian o d esses p acien t es, p od e con t r ib u ir p ar a a assist ên cia d eles assim com o
in f or m ações par a a en f er m agem .
DESCRI TORES: insuficiência r enal cr ônica; diálise r enal; at iv idades cot idianas
1 Occupat ional Ther apist , M.Sc. in Com m unit y Healt h, e- m ail: kar [email protected] .br ; 2 Full Pr ofessor, e- m ail: j air lfs@fm r p.usp.br. Univer sit y of São Paulo at Ribeir ão Pr et o Medical School, Br azil.
I NTRODUCTI ON
F
or a bet t er under st anding of t he im por t ance of k idney s, som e of t heir funct ions ar e: ex cr et ion ofm et abolic w ast e pr odu ct s, pr odu ct ion an d ex cr et ion
of hor m ones and enzy m es, and hor m one m et abolism
( insulin) . Chr onic Renal Failur e ( CRF) is consider ed a
com plex disease t hat leads t o loss, usually slow and
p r og r essiv e, of t h e cap acit y of k id n ey s t o ex cr et e.
Th is con cep t m ay b e t r an slat ed b y t h e p r og r essiv e
r edu ct ion in glom er u lar f ilt r at ion w h ich is t h e m ain
m echanism t o ex cr et e t ox ic m et abolit es pr oduced by
t he body( 1).
Th e m a i n s i g n s o f r e n a l l o s s a r e b l o o d
hypert ension and anem ia. There are also neurological
s i g n s ( i r r i t a b i l i t y a n d t r e m o r s ) , c a r d i o v a s c u l a r
( p u lm on ar y ed em a) , en d ocr in e ( h y p er g ly cem ia an d
w e i g h t l o ss) , a n d m e t a b o l i c ( w e a k n e ss)( 1 ). Ot h e r im port ant inform at ion supplied by t he Br azilian Societ y
o f Ne p h r o l o g y( 2 ) a r e t h e m a n i f e st a t i o n s o f r e n a l d i se a se t h a t p e o p l e ca n p r e se n t su ch a s p a i n a t
ur inat ion, low back pain, w eak ness, and nausea.
Suscept ibilit y of people w it h CRF t o infect ions
d u e t o b l o o d t r a n sf u si o n i s m u ch g r e a t e r i n t h e
pr esence of diseases such as B and C Hepat it is and
AI DS( 1). Most com m on diseases t hat m ay lead t o CRF a r e : d i a b e t e s , b l o o d h y p e r t e n s i o n a n d
g l o m e r u l o n e p h r i t i s . Be c a u s e o f t h a t , c o n t r o l l i n g
p r e s s u r e i s e x t r e m e l y i m p o r t a n t t o p r e v e n t
hy per t ension, as w ell as cont r olling diabet es w hich is
one of t he m ain causes for k idney failur e( 2).
Regar ding CRF t r eat m ent , nor m ally, it occur s
in t h e m ost d ev elop ed st ag es of t h e d isease, in a
p er iod w h er e loss of r en al f u n ct ion is alm ost t ot al,
r equ ir in g eit h er dialy sis or t r an splan t( 1 ). Tr eat m en t s av ailable in t er m in al r en al diseases ar e: Con t in u ou s
Am b u lat or y Per it on eal Dialy sis ( CAPD) , Au t om at ed
Pe r i t o n e a l D i a l y si s ( APD ) , I n t e r m i t t e n t Pe r i t o n e a l
D i a l y s i s ( I PD ) , H e m o d i a l y s i s ( H D ) , a n d r e n a l
t r an sp lan t . We m u st r em em b er t h at all t r eat m en t s
ar e t o r eliev e p at ien t s´ sy m p t om s p at ien t s, n ot t o
heal( 3).
Re g a r d i n g d i a l y s i s , h e m o d i a l y s i s i s a
pr ocedur e t hat depends on a dialyzer ( capillar y filt er )
t o filt er t he blood. I n t he procedur e, pat ient s’ blood is
w it h dr aw n fr om on e v ein , t h r ou gh an ar t er iov en ou s
fist ula or a cat het er and t aken dir ect ly by t ubes t o a
filt er connect ed t o a m achine. This filt er can ex t r act
b lood , w ast e an d ex cess of w at er an d salt s. Af t er
filt er ing, clean blood is t hen r et ur ned t o pat ient s( 4).
Regar din g st at ist ical dat es, Cen su s of 2 0 0 5
of t he Br azilian societ y of Nephr ology w it h t he suppor t of 83% of t he exist ent dialysis unit s, r epor t s t hat t her e a r e 5 4 , 3 1 1 p a t i e n t s u n d e r g o i n g d i a l y si s, 4 8 , 3 6 2 pat ient s in HD, 3,638 in CAPD, 2,073 in APD, and 238 in I PD. Annual incidence in pat ient s undergoing HD is ar ou n d 1 0 0 cases per m illion in h abit an t s; h ow ev er, r eg ar d in g an n u al cost , t r an sp lan t h as a low er cost w hen com par ed t o dialy sis and hem odialy sis( 5).
CRF i s a d i sea se w i t h h i g h m o r b i d i t y a n d
m o r t a l i t y. Th e r e i s p r o g r e s s i v e i n c r e a s e i n t h e incidence and pr ev alence of pat ient s w it h end st age renal disease in Brazil, t hus, renal disease is a m aj or public healt h pr oblem . Pr ev alence r at es of end st age renal disease t reat ed in Brazil are 4 t im es low er t han t hose of t he Unit ed St at es ( USA) and Japan, and half of t he r at es of I t aly, Fr ance, and Ger m any( 6).
Reg ar d i n g r i sk f act o r, t h e m o st i m p o r t an t on es ar e d iab et es an d ad v an ced ag e. Accor d in g t o st at ist ical dat a fr om 1999, in Br azil, 52% of dialy sis pat ient s w er e m ale and, as for age gr oup, 26% w er e
ov er 60, w it h an est im at e of incr ease in t his age in t he last year s; 2.2% w er e less t han 18 and only 297 of t hese pat ient s had age equal t o or below 10 year s old( 6). I n t he last years, t he Minist ry of Healt h in Brazil has inv est ed in hem odialy sis m achines, in supply ing m edicat ion and per for m ing t r ansplant s( 7).
Because of all t he above m ent ioned r egar ding
d ef in it ion , sig n s, sy m p t om s, an d t r eat m en t of t h e disease, w e under st and t hat pat ient s w it h CRF suffer sev er al p h y sical, social, an d em ot ion al lim it at ion s, i n cl u d i n g d i f f i cu l t i es i n o ccu p a t i o n a l p er f o r m a n ce,
w a t e r r e s t r i c t i o n s , s p e c i a l d i e t s , m e d i c a l ap p o i n t m en t s, an d h em o d i al y si s sect i o n s, m ak i n g people fr agile and affect ing t heir ever y day lives. Wit h t h is r egar ds, t alk in g abou t t h e em ot ion al aspect of
r en al pat ien t s is, abov e all, t alk in g abou t a pat h of losses t hat goes bey ond losing r enal funct ion. Fr om t he m om ent of diagnoses t o t he possible per for m ance of t r an sp lan t ( t h e on ly r eal ex p ect at ion of “ cu r e” ) ,
t he pat h of chronic renal failure pat ient s is filled w it h sev er al ot h er issu es t h at pu t t h eir pr oblem an d t h e fam ily dy nam ics int o ev idence( 8).
Because of t hat , it is necessar y t o assess t he
ever y day life of people w it h CRF, by t hat w e m ean t h e ev er y d ay act iv it ies, su ch as g et t in g u p at t h e r ig h t t im e, g oin g t o w or k , g oin g t o sch ool, m ak in g br eak f ast , lu n ch , pr act icin g spor t . Th at is, act iv it ies
aspect s such as w or k, language, t hinking, and feeling,
act ions and r eflect ions of m en( 10).
Th e d i f f i cu l t i es f aced b y t h ese p eo p l e ar e
cou n t less, an d t h ey in f lu en ce t h eir r ou t in e an d t h e
w ay t h ey r elat e, eit h er becau se of t h e depen den cy on t h e m ach i n e, or t h e v i si t s t o t h e d oct or, t h u s,
h i n d e r i n g t h e p e r f o r m a n ce o f t h e i r o ccu p a t i o n a l
act ivit ies, t hat , in t urn, disrupt s t heir every day lives( 11). Based on w hat w as r epor t ed on t he r out ine,
w e u n d e r s t a n d t h a t p e o p l e w i t h CRF m a y h a v e
d if f icu lt ies in t h eir ev er y d ay ch or es. On t h e ot h er h a n d , o c c u p a t i o n a l t h e r a p y h a s t h e g o a l o f
rest ruct uring t he rout ine of people as one of it s m ain o b j ect i v es, a s w el l a s t o f a v o r t h ei r o ccu p a t i o n a l
per for m ance and t o pr om ot e st r at egies t hat favor t heir con n ect ion w it h t h e social env ir on m en t . To dev elop
t h i s w o r k , i t i s i m p o r t a n t t o r e p o r t o n a r e a s o f occu p at ion al d ev elop m en t . Occu p at ion al t h er ap y is
t he ar t and science of helping people t o per for m daily a ct i v i t i es t h a t a r e i m p o r t a n t t o t h em d esp i t e t h e
inabilit ies or deficiencies. “ Occupat ion” in occupat ional
t h e r a p y d o e s n o t r e f e r o n l y t o p r o f e s s i o n s o r pr ofessional t r aining, it r efer s t o act iv it ies t hat t ak e
people’s t im e and giv e m eaning t o t heir liv es( 12). I n occupat ional t herapy t hese areas ar e called
occu pat ion al per f or m an ce, an d t h ey can be div ided int o act ivit ies of daily living, pr ofessional, and leisur e
an d play act iv it ies. For a bet t er u n der st an din g, t h e a r e a s o f Occu p a t i o n a l Pe r f o r m a n ce a r e d e scr i b e d
below accor ding t o t he Ter m inology of AOTA( 13): - Act ivit ies of Daily Living ( ADL) : it r efer s t o dr essing,
clean in g m ou t h , sh ow er in g, t oilet h y gien e, car e f or
on e’s ow n b od y , f eed in g , m ed ical r ou t in e, k eep in g
h e a l t h , s o c i a l i z a t i o n , f u n c t i o n a l m o b i l i t y , a n d
com m u n it y m obilit y ;
- Pr o f e s s i o n a l a c t i v i t i e s : h o m e m a n a g e m e n t
( m a i n t a i n i n g c l o t h e s , c l e a n i n g , p r e p a r i n g f o o d ,
s h o p p i n g , m a n a g i n g m o n e y , m a i n t a i n i n g t h e
household, safet y pr ocedur es) , t aking car e of ot her s,
educat ional act iv it ies, v ocat ional act iv it ies ( v ocat ional
ex p l o r at i o n , acq u i r i n g a j o b , p l an n i n g r et i r em en t ,
v olu n t ar y par t icipat ion ) ;
- Leisur e and Play act iv it ies: leisur e ex plor at ion and
fun, play ing gam es, leisur e and ent er t ainm ent .
OBJECTI VES
Th e ob j ect iv e of t h e p r esen t st u d y w as t o
assess t h e p er cep t ion of p eop le w it h CRF on t h eir rout ine, regarding t heir occupat ional funct ioning in t w o
pu blic h ealt h ser v ice: UTR ( Hem odialy sis an d Ren al
Transplant Unit ) of t he Hospit al das Clínicas in Ribeirão
Pr et o - HCRP and at SENERP ( Nephr ology Ser v ice of
Ribeir ão Pr et o) .
MATERI ALS AND METHODS
Th e pr oj ect w as seen an d appr ov ed by t h e
Et hical Resear ch Com m it t ee of t he HCRP and of t he
Sch ool of Medicin e of Ribeir ão Pr et o- USP, f ollow in g,
t h e r e f o r e , t h e e t h i ca l g u i d e l i n e o n r e se a r ch w i t h
h u m an b ei n g s. Su b j ect s w er e ask ed t o g i v e t h ei r
w r it t en con sen t an d w e ex plain ed t h at par t icipat ion
w ould be v olunt ar y and t hat subj ect s could giv e up.
This is a cross- sect ional analyt ical- descript ive
quant it at iv e st udy.
Th e s a m p l e w a s f o r m e d b y 7 0 p a t i e n t s
u n der goin g h em odialy sis at UTR an d at SENERP. At
SENERP, pat ien t s w er e in t er v iew ed t o com plet e t h e
sam ple ( n = 7 0 ) , w e did n ot t r y t o com par e ser v ices
and our pur pose w as not for sam ples t o be pr opor t ional
an d r epr esen t at iv e of ser v ices.
Regar ding inclusion cr it er ia, in bot h ser vices,
pat ient s w it h CRF under going hem odialysis, w it h ages
r anging fr om 15 t o 60 year s old and t hat could answ er
t h e qu est ion n air es t ook par t in t h e st u dy. Exclu sion
cr it er ia w er e: n ot bein g t h e age def in ed, n ot bein g
able t o under st and quest ionnair es, and pr esence of a
m or e sev er e disease ot her t han CRF.
A p r e v i o u s st u d y w a s co n d u ct e d w i t h 1 0
indiv iduals fr om t he sam e gender w it h ages r anging
f r om 1 5 t o 7 0 , 5 f r om each ser v ice, an d w e h av e
a p p l i e d t h r e e q u e s t i o n n a i r e s f o r e a c h , o n e w a s
sociodem ogr aphic, one w as t he WHO Qualit y of Life
( WHOQOL- br ef ) and one w as SAOF - Self Assessm ent
o f Occu p a t i o n a l Fu n ct i o n i n g . Qu est i o n n a i r es w er e
individually and self - applied. I n t his st udy, w e not iced
t h at som e par t icipan t s h ad pr oblem s u n der st an din g
som e quest ions, because of t hat , w e hav e ex cluded
t hese quest ionnair es fr om t he definit iv e sam ple and
d ecid ed t h at t h e ap p licat ion w ou ld b e d on e b y t h e
r esear cher and t he age w as lim it ed at 60 y ear s old.
I nit ially, inform at ion of all pat ient s from
UTR-h e m o d i a l y si s t UTR-h a t m e t t UTR-h e i n cl u si o n cr i t e r i a w a s
gat her ed, t her e w er e 16 pat ient s t hat , t oget her w it h
t he 5 4 fr om SENERP, t ot aled 7 0 pat ient s, w it h ages
r an g in g f r om 1 7 t o 6 0 y ear s old . I n t er v iew s f r om
SENERP w er e per for m ed t hr ough a dr aw , consider ing
and t hat also m et t he inclusion crit eria. Research w as conduct ed fr om June 14t h t o Sept em ber 27t h, 2005. SAOF i s t h e i n st r u m en t w h o se t h eo r et i cal bases is t he m odel of hum an occupat ion and it w as
developed in 1990, in t he Depar t m ent of Occupat ional Ther apy of t he Univ er sit y of I llinois( 14), Chicago, w it h recent validat ion, in 2000 in Brazil. This m odel supplies a w ay t o t hink on t he occupat ional behavior of people
an d t h eir occu p at ion al d y sf u n ct ion . Th eir con cep t s involve encour aging people t o t ake up an occupat ion, w it h st andar ds of occupat ional behav ior r out ine, w it h t h e n a t u r e o f t h e w o r k p e r f o r m e d a n d w i t h t h e
influence of t he env ir onm ent on t he occupat ion( 15). Th i s i n s t r u m e n t m a y b e u s e d b y p e o p l e bet w een 14 and 85 and pr esent s as t he m ain pur pose ident ify ing t he per cept ion of pat ient s r egar ding t heir
occupat ional funct ioning, including underst anding t heir st r e n g t h s, su i t a b i l i t y a r e a , a n d l i m i t a t i o n s. SAOF p r e s e n t s a n a p p l i c a t i o n f o r m e n c o m p a s s i n g 2 3 q u est ion s, cov er in g sev en con t en t ar eas: p er son al
causat ion, v alues, int er est s, r oles, habit s, sk ills, and e n v i r o n m e n t . To t h a t e n d , a s c a l e w i t h t h r e e cl a ssi f i ca t i o n g r a d es i s u sed : st r en g t h , a d eq u a t e, needs im pr ov em ent t hat quant ifies t he per cept ion of
p a t i e n t s o n a r e a s o f o c c u p a t i o n a l f u n c t i o n i n g . Per f or m an ce of p at ien t s is assessed as: v er y g ood ( s t r e n g t h ) , g o o d ( a d e q u a t e ) a n d p r e s e n c e o f
difficult ies ( needs im pr ov em ent )( 1 6 ).
s a e r A n a e
M StandardDeviation
s h t g n e r t
S Adequate Needs
t n e m e v o r p m
I Strengths Adequate
s d e e N t n e m e v o r p m I y tl a u s a c l a n o s r e P .
1 60.5 24.3 15.2 35.6 30.5 25.8
s e u l a V .
2 56.7 22.8 20.5 34.2 26.9 27.4
s t s e r e t n I .
3 60 32.4 7.7 38.3 36.3 20.6
s e l o R .
4 62.8 29.00 8.1 31.4 31.0 17.4
s t i b a H .
5 46.2 33.8 20 36.0 35.2 26.8
s ll i k S .
6 57.7 27.1 15.1 28.7 25.3 18.0
t n e m n o r i v n E .
7 74.3 20 5.7 44.0 40.3 23.4
DATA ANALYSI S
For each v alue of t he scale self assessm ent
w as w r it t en dow n and in each ar ea t he per cent age of
t h eir an sw er s classif ied as St r en g t h s, Ad eq u at e or
pr esent s difficult ies. For t he set of pat ient s m ean of
p e r c e n t a g e s w a s c a l c u l a t e d , t o g e t h e r w i t h t h e
r e s p e c t i v e d e v i a t i o n s t o f i n d d i f f e r e n c e s a n d
sim ilar it ies.
RESULTS AND DI SCUSSI ON
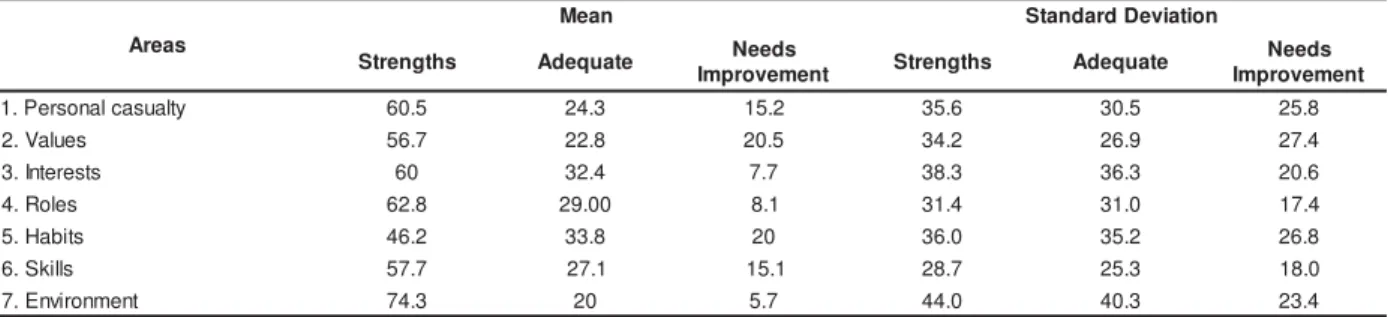
Tab le 1 p r esen t s t h e p er cen t ag e r esu lt s of
m e a n a n d s t a n d a r d d e v i a t i o n o b t a i n e d b y t h e
applicat ion of inst r um ent s. We have obser v ed t hat in
all ar eas “ St rengt hs” w as t he m ost com m only select ed
opt ion. The ar ea called Env ir onm ent pr esent ed m ean
7 4 . 3 % an d it w as t h e g r eat est ar ea. Th e sm allest
m e a n , 4 6 . 2 % , r e f e r r e d t o a r e a 5 ( H a b i t s ) , s t i l l
con sid er in g t h e alt er n at iv e St r en g t h s. Ar eas w h er e
d i f f i cu l t y w as ch o sen w er e ar ea 2 ( 2 0 . 5 % ) an d 5
( 20% ) . Regar ding ar ea 5 ( habit s) , t her e is sim ilar it y
w it h st udies developed in 2000( 16), because it w as one of t h e ar eas w it h g r eat er scor e p er cen t ag e in t h e
opt ion “ n eeds im pr ov em en t ”.
Table 1 – Means and st andar d deviat ion of individual r esponses obt ained by t he applicat ion of SAOF quest ionnair e,
accor din g t o each r efer en ce ar ea
For a bet t er under st anding, each t opic of t he
i n st r u m en t w a s i n d i v i d u a l l y a ssessed : 1 - Ar ea o f
Per son al Cau sat ion : t h e alt er n at iv e “ st r en gt h s” w as
one of t he m ost com m only chosen ( 60.5% ) , t her efor e,
m ost int erview ees believe in t heir skills and capacit ies;
2 - A r e a o f Va l u e s : t h e a l t e r n a t i v e “ n e e d s
im p r ov em en t ” accou n t ed f or 2 0 . 5 % of t h e ch oices,
an d d esp i t e t h e sm al l p er cen t ag e, i t w as t h e o n e
p a t i e n t s p r e s e n t e d d i f f i c u l t i e s r e g a r d i n g h a v i n g
obj ect ives and expect at ions for t he fut ur e; 3- Ar ea of
in t er est : t h er e w as n o dif f icu lt ies, w it h 6 0 % in t h e
opt ion “ st r engt hs”. Thus, ev en w it h lim it at ions, t hese
p eop le t r y t o b e in t er est ed in d oin g som et h in g ; 4
-Roles: m ost people could per for m t heir r oles, eit her
as w or k er s, st u d en t s or f am ily m em b er, r eg ar d less
of t he difficult ies; 5- Ar ea of habit s: t hese people find
it har d t o or ganize t heir t im e, schedules, and t o accept
t he changes in t heir r out ine. I n t his ar ea, t he opt ion
“ n e e d s i m p r o v e m e n t ” a cco u n t e d f o r 2 0 % o f t h e
social life, ex pr ess t hem selv es, solv e pr oblem s, and per for m ever y- day t asks w it hin t heir abilit ies; 7- Ar ea
o f En v i r o n m e n t : i t w a s t h e o n e w i t h g r e a t e s t per cent age of “ St r engt hs” ( 74.3% ) , show ing t hat m ost
people w ant t o be in places t hey feel good.
Th e dif f icu lt y poin t ed ou t in t h e v alu e ar ea
e n a b l e d t h e se p e o p l e t o g e t i n t o u ch w i t h m o r e
subj ect ive issues and w it h t heir cur r ent r ealit y, such as, for exam ple, having obj ect ives for t he fut ur e and
per for m act iv it ies t h at ar e m ean in gfu l. Th is m ay be relat ed w it h losses t hat occur w it h t hese people, t here
ar e social an d f in an cial losses, an d t h ey also lose phy sical capacit y and leisur e act iv it ies, t hat can lead
t o self - pit y an d ov er r eact ion s. I n t h ese cases, it is
necessar y t o help pat ient s cont r ol t he sit uat ion( 4). I t i s o b se r v e d i n a su m m a r i ze d w a y t h a t
Hab it s an d Valu es ar e t h e t w o ar eas w it h g r eat er percent age of “ needs im provem ent ”. We see here t he
o p p o r t u n i t y a n d t h e n e e d f o r t h e co n t r i b u t i o n o f Occu p at ion al Th er ap y t o r est r u ct u r e t h e r ou t in e of
pat ient s: suppor t a new or ganizat ion of t im e, change in r out ine, per sonal r elat ions and, t hus, r einfor ce t he
con t r ol on bot h t h e social loss an d loss in ph y sical cap acit y.
Nat u r ally, it is ex pect ed t h at act iv it ies w it h
body involvem ent and t hose r ecr eat ional ar e t he daily act ivit ies t hat are m ost involved( 3), and in t his cont ext , t he out com es of t he pr esent st udy point out t o t hat healt h professionals need t o use individualized act ions
t o help individuals adj ust t o and live w it h inabilit ies. Re g a r d i n g S A O F q u e s t i o n n a i r e , s o m e
p a r t i ci p a n t s h a d d i f f i cu l t i e s u n d e r st a n d i n g so m e qu est ion s. Ov er all, m ost par t icipan t s u n der st ood it ,
h ow ev er, som e of t h em r eq u ir ed ex p lan at ion f r om t h e r esear ch er an d ad j u st m en t of som e q u est ion s,
such as in ar ea 4, quest ion num ber 10 w hich asks if t he per son is inv olv ed w it h his/ her r ole ( eit her as a
st u den t or w or k er ) , it w as n ecessar y t o ex plain t h e
m e a n i n g o f r o l e . Th e r e w a s a l so d i f f i cu l t y i n t h e presence of m ore t han one var iable in t he sam e it em ,
such as for ex am ple, in t he it em 21 ( t ak ing car e of p er son al h y g ien e, cook an d lau n d r y ) , w h ich m ad e
p e o p l e t h i n k i n a l l t h e s e v a r i a b l e s , w i t h o u t under st anding t hey w er e only exam ples. This fact w as
also r epor t ed in 2000( 16).
I n 2004( 17), it w as suggest ed t hat it w ould be easier if t he st at em ent s w er e pr esent ed as quest ions and t he opt ions of answ er s w er e r eplaced by : a lot ,
sor t of, and difficult y. Relat ing t his com m ent t o w hat
w as applied on t he r esear ch, t his r eplacem ent w ould a l so b e co n si d e r a b l e si n ce , m a n y t i m e s, a n d t h e
r esea r ch er h a d t o m a k e t h i s ch a n g e f o r a b et t er u n d er st an d in g .
CONCLUSI ONS
The use of SAOF quest ionnair e show ed t hat
in t he ar eas of v alues and habit s, aspect s r egar ding t he or ganizat ion of t im e, flex ibilit y, r out ine changes,
obj ect ives, and expect at ions for t he fut ur e, t hey w er e n o t s t r u c t u r e d i n r e l a t i o n t o t h e o c c u p a t i o n a l
f u n c t i o n i n g o f t h e s e p e o p l e . H o w e v e r, w e m u s t r em em b er t h at t h e p er cen t ag e w as n o t v er y h i g h
r egar din g t h e dif f icu lt ies an d t h at t h e ov er all r esu lt w as sat isf act or y. Th er ef or e, w e u n d er st an d t h at in
t he pr esent st udy, people t hat under go hem odialy sis
ar e not t ot ally incapable of per for m ing t heir daily t asks. Fr om t his, w e can not ice t hat even in face of
dif f icu lt ies, w it h a r ou t in e ch an ged by h em odialy sis h ou r s, f ood r est r ict ion s, an d in m an y case, loss of
w or k / st u d y, in d iv id u als w it h CRF can , if n ecessar y, and with the help of professionals, develop a routine of
t asks, build proj ect s, and do som et hing m eaningful for them selves, that is, they can rebuild their daily lives.
ACKNOW LEDGMENTS
We like t o t hank t he suppor t of all t he t eam
of bot h public healt h ser vices: UTR ( Hem odialysis and Renal Transplant Unit ) of t he Hospit al das Clínicas in
Rib eir ão Pr et o an d SENERP ( Nep h r olog y Ser v ice of
Ribeir ão Pr et o) .
REFERENCES
1 . D r a i b e SA. I n su f i ci ê n ci a Re n a l Cr ô n i ca . I n : Sch o r N, or g an izad or. Gu ia d e Nef r olog ia. São Pau lo ( SP) : Man ole; 2 0 0 2 .
2 . Sociedade Br asileir a de Nef r ologia ( SBN) [ h om epage n a I nt er net ] . Censo 2005, Cent r o de Diálise no Br asil; [ Acesso em 1 3 d e m a r ço d e 2 0 0 6 ] . D i sp o n ív el em : URL: h t t p : / / w w w . sbn. or g. br / censo.
3. Mar t ins MRI , Cesar ino CB. Qualidade de v ida de pessoas com doença r enal cr ônica em t r at am ent o hem odialít ico. Rev Lat in o- am En f er m ag em 2 0 0 5 ; 1 3 ( 5 ) : 6 7 0 - 6 .
s e u s f a m i l i a r e s . Re v La t i n o - a m En f e r m a g e m 2 0 0 3 ; 1 1 ( 6 ) : 8 2 3 - 3 1 .
6. Sesso R. Epidem iologia da I nsuficiência Renal Cr ônica no Br asil. I n: Schor N, or ganizador. Guia de Nefr ologia. São Paulo ( SP) : Man ole; 2 0 0 2 .
7 . Min ist ér io d a Saú d e. [ h om ep ag e n a I n t er n et ] . Doen ças Renais; [ Acesso em 18 de out ubr o de 2002] . Disponível em : URL: ht t p: / / w w w. por t alw eb05saude. gov. br / por t al/ saúde. 8. Lim a AMC. I nsuficiência r enal cr ônica: a t r aj et ór ia de um a pr át ica. I n: Bellk iss WR, or ganizador. A Pr át ica da Psicologia n os Hospit ais. São Pau lo ( SP) : Pion eir a; 1 9 9 4 . p. 7 7 - 9 2 . 9. Net t o JP, Car valho MC. Cot idiano: Conhecim ent o e Cr ít ica. 4ª ed. São Paulo ( SP) : Cor t ez; 1996.
1 0 . Lu ck á cs. On t o l o g i a d o se r so ci a l I e I I . Sã o Pa u l o : Ciên cias h u m an as; 1 9 7 9 .
1 1 . Bezer r a K, Piant ino D, Mor ais L. Relat o de ex per iência: gr upo de t er apia ocupacional dur ant e hem odiálise. Rev Cent r o de Est u dos de Ter apia Ocu pacion al – CETO 2 0 0 5 ; 9 ( 9 ) : 2 9 -3 5 .
Recebido em : 5.7.2007 Apr ovado em : 15.6.2008
12. Neist adt C. I nt r odução a Terapia Ocupacional. I n Willar d HS, Spack m an CS or ganizador es. Ter apia Ocupacional Rio de Janeir o ( R.J) : Guanabar a Koogan; 2002 p. 3- 9.
1 3 . A OTA A m e r i c a n Oc c u p a t i o n a l Th e r a p y A s s o c i a t i o n . Ocupat ional t her apy associat ion pr act ice fr am ew or k : dom ain an d pr ocess. Am J Ocu pat ion al Th er apy 2 0 0 2 ; 4 8 : 1 0 4 7 - 5 4 . 14. Bar on KB, Cur t in C. The Self Assesm ent of Occupat ional Fu n ct ion in g ( SAOF) . Ch icago: Un iv er sit y of I llin ois; 1 9 9 0 . 15. Kielhofner G, Bar r et L. O Modelo da Ocupação Hum ana. I n : Willar d HS, Spack m an CS. Ter apia Ocu pacion al. Rio de Janeir o ( R. J) : Guanabar a Koogan; 2002. p. 490- 2.