r e v b r a s r e u m a t o l . 2016;56(3):270–273
ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
IgA
nephropathy
in
systemic
lupus
erythematosus
patients:
case
report
and
literature
review
Leonardo
Sales
da
Silva,
Bruna
Laiza
Fontes
Almeida,
Ana
Karla
Guedes
de
Melo,
Danielle
Christine
Soares
Egypto
de
Brito,
Alessandra
Sousa
Braz,
Eutília
Andrade
Medeiros
Freire
∗SchoolofMedicine,UniversidadeFederaldaParaíba,JoãoPessoa,PB,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1August2014 Accepted19October2014 Availableonline16February2015
Keywords:
Systemiclupuserythematosus IgAnephropathy
Glomerulonephritis
a
b
s
t
r
a
c
t
Systemicerythematosuslupus(SLE)isa multisystemicautoimmunediseasewhichhas nephritisasoneofthemoststrikingmanifestations.Althoughitcancoexistwithother autoimmunediseases,anddeterminethepredispositiontovariousinfectious complica-tions,SLEisrarelydescribedinassociationwithnon-lupusnephropathiesetiologies.We reporttherareassociationofSLEandprimaryIgAnephropathy(IgAN),themostfrequent primaryglomerulopathyintheworldpopulation.ThepatientwasdiagnosedwithSLEdue totheoccurrenceofmalarrash,alopecia,pleuraleffusion,proteinuria,ANA1:1280,nuclear finespeckledpattern,andanticardiolipinIgMand280U/mL.Renalbiopsyrevealed mesan-gialhypercellularitywithisolatedIgAdeposits,consistentwithprimaryIgAN.Itwastreated withantimalarialdrug,prednisoneandinhibitorofangiotensinconvertingenzyme, show-inggoodprogress.Sincetheyarerelativelycommondiseases,thecoexistenceofSLEand IgANmayinfactbeanuncommonfindingforunknownreasonsoranunderdiagnosed con-dition.Thisreportfocusontheimportanceofthedistinctionbetweentheactivityofrenal diseaseinSLEandnon-SLEnephropathy,especiallyIgAN,adefinitionthathasimportant implicationsonrenalprognosisandtherapeuticregimenstobeadoptedinboththeshort andlongterms.
©2014ElsevierEditoraLtda.Allrightsreserved.
Nefropatia
por
IgA
em
paciente
portadora
de
lúpus
eritematoso
sistêmico:
relato
de
caso
e
revisão
de
literatura
Palavraschave:
Lúpuseritematososistêmico NefropatiaporIgA
Glomerulonefrite
r
e
s
u
m
o
Olúpuseritematososistêmico(LES)éumadoenc¸aautoimune multissistêmicaquetem comoumadasmanifestac¸õesmaismarcantesanefrite.Apesardepodercoexistircom out-rasdoenc¸asautoimunesedeterminarapredisposic¸ãoadiversascomplicac¸õesinfecciosas, oLESraramenteédescritoemassociac¸ãoanefropatiasdeetiologianãolúpica.Relatamos
∗ Correspondingauthor.
E-mail:[email protected](E.A.M.Freire).
http://dx.doi.org/10.1016/j.rbre.2014.10.011
rev bras reumatol.2016;56(3):270–273
271
ocasodararaassociac¸ãoentreLESenefropatiaporIgA(NIgA)primária,a glomerulopa-tiaprimáriamaisfrequentenapopulac¸ãomundial.ApacientefoidiagnosticadacomLES pelaocorrênciadeeritemamalar,alopecia,derramepleural,proteinúria,pancitopenia,FAN 1:1.280padrãonuclearpontilhadofinoeanticardiolipinaIgM280U/mL.Abiópsiarenal rev-elouhipercelularidademesangialcomdepósitosisolados deIgA, compatívelcomNIgA primária.Foitratadacomantimalárico,prednisonaeinibidorda enzimaconversorade angiotensinaeapresentouboaevoluc¸ão.Porconsistirememdoenc¸asrelativamente fre-quentes,acoexistênciadeLESeNIgApodeserdefatoumachadoincomumpormotivos desconhecidosouumacondic¸ãosubdiagnosticada.Esterelatoatentaparaaimportância dadistinc¸ãoentreaatividadededoenc¸arenaldoLESenefropatiasnãolúpicas,em espe-cialaNIgA,definic¸ãoquetemimplicac¸õesimportantessobreoprognósticorenaleregimes terapêuticosaseremadotadosemcurtoelongoprazo.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Systemiclupuserythematosus(SLE)isachronicdisease of theconnectivetissuecharacterizedbyanumberof immuno-logicaldisorderswhich resultinthe onsetofinflammatory lesionin variousorgan tissues. Lupusnephritis (LN)isthe mostcommonvisceralmanifestationofSLE,beingdiagnosed inapproximately37–45%ofthepatientsatsometime dur-ingthecourseofthediseaseintheBrazilianpopulation.1,2
Thedescription ofnephritis of other etiologies inpatients diagnosedwithSLE,however,isanuncommonfinding.3IgA
nephropathy(IgAN),althoughbeingthemostcommoncause ofglomerulopathyingeneralpopulation,4israrelyassociated
withSLE.5–10WereportedacaseofrarecoexistenceofIgANin
apatientwithSLE.
Case
report
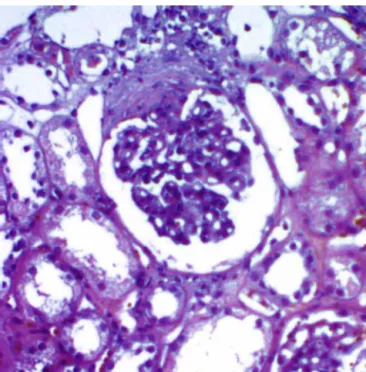
Forty-year-old female patient, complaining of generalized edema six months ago, associated with polyarthralgias, intermittentfever,alopecia,weightlossof7kg,andulcerated lesionontherightleg.Onexaminationthepatientwaspale, with bilateral periorbital edema, facial flushing, reduced vesicular murmur on the right, lower limb edema (2+/4+) andpyodermagangrenosuminthemiddlethirdoftheright leg,associatedwithstiffnessandswelling ofthe rightcalf. Additional assessment indicated hemoglobin of 8.9g/dL, leukopenia,mildthrombocytopenia,ANA1:1.280ofnuclear fine speckled pattern, CH50 of 88U/mL, C3 of 46mg/dL, C4 of9mg/dL,negative anti-dsDNA, anticardiolipin IgM of 211U/mL,proteinuriaof1045mg/24h,endogenouscreatinine clearanceof162mL/min,dysmorphichematuria,andgranular urinarycasts.Chestcomputedtomographyshowedbilateral pleuraleffusion,mildpericardialeffusion,andascites.Lower limb Doppler ultrasonography ruled out thrombotic event. Renal biopsy was performed, showing 16 intact glomeruli withmesangialgranulardepositionofIgA,negativeforother immune deposits, and mesangial hypercellularity (Fig. 1). Thepatientwas diagnosedwithSLEassociatedwithIgAN, and she was initially treated with prednisone 60mg/day, hydroxychloroquine 400mg/day, enalapril 10mg/day, and
Fig.1–Opticalmicroscopyofspecimenobtainedbyrenal biopsyrevealingmesnagialexpansionandhypercelullarity (HE,200×).
supplementationofcalciumand vitaminD,andantibiotics forskinlesion.Afterinitiatingtreatment,thepatientshowed improvementofthejoint,cutaneous,hematologic,andrenal status,beingreadyforhospitaldischarge.
Discussion
SLEisadiseasemarkedbyheterogeneityofclinical pheno-typesandunpredictablecourse.1,2Thesepropertiesmakethe
272
rev bras reumatol.2016;56(3):270–273Laboratory data may indicate SLE and LN activity, specifi-callyashightitersofanti-dsDNAantibodiesandcomplement consumption.11
TheIgAN,ontheotherhand,manifestsitselfaspersistent microscopic,orsporadicmacroscopichematuria,withflare triggeredbyinflammatorystress.Proteinuriaandother find-ingsmayormaynotbepresent,andserumcomplementlevels aretypicallynormal.12
Duetotherelativefrequencyofbothconditions,the coex-istenceofprimaryIgANandSLEcanbeanoccasionalfinding. BothLNandIgANareconditionswhicharecharacterizedby disordersofimmunefunction,withthepresenceofcirculating immunecomplexesandanti-C1qantibodies,inadditiontothe involvementofgeneticand environmentalriskfactors.12–14
Itisstilluncertainwhetherthe rarityoftheassociation of SLEwithnon-lupusnephritisoccursduetoaprotectivefactor presentedbypatientswithSLE,orifwefaceunderdiagnosed conditions.3,8,10 Thecoexistence ofSLEandIgAN hasbeen
recentlydescribed, with only eight casespublished in the world so far,5–10 with this being the first case reported in
Brazil.Mac-Mouneetal.firstreportedthisassociationin1995,5
withthree patientswho,similar to theone here inBrazil, hadglomerularlesionofindolentcourseassociatedwith exu-berant systemic presentations. Curiously, Basile et al. and Kobaketal.6,10 describedpatientswho,besidesthe
diagno-sisofIgANandSLE,hadHashimoto’sthyroiditis,arelatively commonassociationwithSLE,butthatrarelycoexistswith IgAN.
Thepatientdescribedwasadmittedtoourhospitalwith a suggestive multisystemic clinical picture, and antibody profile consistent with the diagnosis of SLE. The identifi-cation of histopathological findings suggestive of IgAN in SLEpatients was, as inmost of the casesreported in the literature,5,6,8,10 from renalbiopsy indicatedforhistological
classificationofprobableLN.Ontwooccasions the diagno-sisofIgANwassuggestedinpatientswithnoSLEactivity.7,9
ThisfactcanpointtoanIgANflaredeterminedbythe sys-temicinflammatory insult,a commoncharacteristicofthe disease,12 inthiscasecausedbySLE.Mostofthedescribed
casesrevealednormalcomplement,afactorfavoringthe diag-nosisofIgAnephropathy.Incontrast,thepatientdescribed herein, as well as those published by Corrado et al. and Kobak et al.8,10 showed complement consumption at
diag-nosis, possibly reflecting extrarenal lupus activity, such as thehematologicactivityreportedhere.Anothercommon fea-ture among the cases described is the indolent course of IgAN, withurinary sediment changes,variable proteinuria, andpreservationofglomerularfiltration,with immunosup-pressivetherapy,whenitisundertaken,beingindicateddue toextrarenallupusactivity.5,6,8,10
Histopathologicalexaminationshowedmesangial hyper-cellularityand glomerulardepositionofIgA intheabsence ofotherimmunedeposits.Theimmunohistologicalfindings of IgAN include mesangial deposits of IgA, C3, and pos-sibly, IgG and IgM in lesser extent.12 On the other hand,
the LN characteristicchanges includeglomerular, vascular and tubulointerstitiallesions with depositionof polyclonal immunoglobulins,mainlyIgG,andfractionsofcomplement C1q,C3andC4.14AlthoughmesangialIgAdepositioncanbe
consideredasubtypeofLN,theabsenceofIgG,C1q,C3and
C4depositsisnotanexpectedfindinginLN,beingmore com-patiblewiththediagnosisofIgAN.5,6,12
The distinction between IgAN and LN in SLE patients has important prognostic and therapeutic implications. The general recommendations for treatment of IgAN are focused on blood pressure control and proteinuria reduction with antihypertensive drugs that act on the renin–angiotensin–aldosterone system, with immunosup-pression being reserved to cases of crescentic glomeru-lonephritis,andcorticosteroidtherapyforlimitedtimeonly inpatientswithpersistentproteinuriagreater than1g/24h evenafter3–6monthsofoptimizedtherapy.15Ontheother
hand, inthe treatmentforLN, besidescontrolling protein-uriaandbloodpressure,basetherapywithantimalarialsfor allpatientsisrecommended,aswellasspecificprotocolsof immunosuppressionaccordingtothehistopathologicalclass ofthedisease.11
Finally, this report highlights the possibility of overex-posure of primary IgAN in patients withSLE, which is an associationthatmaybemorecommonthanitisfrequently describedintheliterature,andhasdirectimplicationsonthe follow-upandtreatmentoftheseindividualswiththeshort-, medium-andlong-termcomplications.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BezerraEL,VilarMJ,BarbosaOF,SantosSQ,CastroMA, TrindadeMC,etal.Lupuseritematososistêmico(LES):perfil clínico-laboratorialdospacientesdoHospitalUniversitário OnofreLopes(UFRN-Natal/Brasil)eíndicededanonos pacientescomdiagnósticorecente.RevBrasReumatol. 2005;45(6):339–42.
2.BorbaEF,AraujoDB,BonfáE,ShinjoSK.Clinicaland immunologicalfeaturesof888Braziliansystemiclupus patientsfromamonocentriccohort:comparisonwithother populations.Lupus.2013;22(6):744–9.
3.AndersH,WeeningJJ.Kidneydiseaseinlupusisnotalways ‘lupusnephritis’.ArthritisResTher.2013;15:108.
4.McGroganA,FranssenCF,VriesCS.Theincidenceofprimary glomerulonephritisworldwide:asystematicreviewofthe literature.NephrolDialTranspl.2011;26:414–30.
5.Mac-MouneLF,LiEK,TangLN,LiPK,LuiSF,LaiKN.IgA nephropathy:ararelesioninsystemiclupuserythematosus. ModPathol.1995;8:5–10.
6.BasileC,SemeraroA,MontanaroA,GiordanoR,DePadovaF, MarangiAL,etal.IgAnephropathyinapatientwithsystemic lupuserythematosus.NephrolDialTranspl.1998;13:1891–2.
7.FujikuraE,KimuraT,OtakaA,ArimaS,SatohH,ItohS,etal. IgAnephropathyinthepatientwithsystemiclupus erythematosusinremission.NipponNaikaGakkaiZasshi. 2002;11:3282–4.
8.CorradoA,QuartaL,DiPalmaAM,GesualdoL,CantatoreFP. IgAnephropathyinsystemiclupuserythematosus.ClinExp Rheumatol.2007;25:467–9.
9.HorinoT,TakaoT,TeradaY.IgAnephropathyinapatient withsystemiclupuserythematosus.Lupus.2010;19:650–4.
rev bras reumatol.2016;56(3):270–273
273
IgAnephropathyinthesamepatient.ModRheumatol. 2011;21:89–91.
11.HahnBH,McMahonMA,WilkinsonA,WallaceWD,DaikhDI, FitzgeraldJD,etal.Americancollegeofrheumatology guidelinesforscreening,treatment,andmanagementof lupusnephritis.ArthritisCareRes.2012;64(6):797–808.
12.BarrattJ,FeehallyJ.IgAnephropathy.JAmSocNephrol. 2005;16(7):2088–97.
13.GunnarssonI,RönnelidJ,LundbergI,JacobsonSH.Ocurrence ofanti-C1qantibodiesinIgAnephropathy.NephrolDial Transpl.1997;12(11):2263–8.
14.SinniahR,FengPH.Lupusnephritis.Correlationbetween light,electronmicroscopic,andimmunofluorescentfindings andrenalfunction.ClinNephrol.1976;6(2):340–51.