w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Review
Article
Fecal
incontinence
and
quality
of
life
assessment
through
questionnaires
Beatriz
Deoti
Silva
Rodrigues
a,b,∗,
Igor
Guedes
Nogueira
Reis
c,
Felipe
Marcondes
de
Oliveira
Coelho
c,
Kelly
Cristine
de
Lacerda
Rodrigues
Buzatti
b aAssociateProfessorofSurgery,SchoolofMedicine–DepartmentofSurgery–UniversidadeFederaldeMinasGerais(UFMG)bMemberoftheColoproctologyStaff,HospitaldasClínicas–UFMG
cMedicalStudent,UniversidadeFederaldeMinasGerais(UFMG)
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13May2017 Accepted25June2017
Keywords:
Fecalincontinence Qualityoflife Signsandsymptoms
Outcomeassessment(healthcare) FecalIncontinenceScore
Evaluationofresultsoftherapeutic interventions
a
b
s
t
r
a
c
t
Background:Fecalincontinencecausesabigimpactonpatient’squalityoflife.Ourstudy ana-lyzedthemainquestionnairesaboutfecalincontinenceavailableinternationally,aimingto delineatevantagesandlimitationsoftheseinstrumentsandtheirapplication,tomention theculturalaspectsinvolvedintheprocessofdevelopmentandvalidation,aswellasto suggestareflectionaboutthecomplexityofthismatter.Results:Fouroftheinstruments (Pescatoriscore,FISI,MSKCCbowelfunctioninstrument,andLARSscore)donotinclude qualityoflife,workingonlyasdiagnostictools.Twoothers,‘JorgeandWexnerFecal Inconti-nencescore’,and‘StMarks’Fecalincontinencegradingsystem’candiagnoseandgradefecal incontinence,howevertheyareverysubtleinassessingqualityoflife.The‘EORTC Colorec-talCancer-specific’,ontheotherhand,focusesexclusivelyonqualityoflife.Althoughthe ‘FIQL’questionnaireassessesqualityofliferelatedtofecalincontinence,itdoesnot mea-sureleakage.Lastly,the‘RAFIS’assessesbothaspectsbuttoosuperficially.Conclusion:None ofthequestionnairesanalyzedwereabletosimultaneouslyassessbothfecalincontinence andqualityoflifesuccessfully.Furthermore,theconceptsrelatedtofecalincontinencehave differentmeaningsdependingontheculturalandpsychosocialcontext.Thesedifferences areevengreaterwhenindividualsofdevelopedcountriesliketheoneswherethese ques-tionnairesweredevelopedarecomparedtotheonesofdevelopingcountries,suchasBrazil, whichmakesitsveryhardfortheseinstrumentstobeuseduniversally.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](B.D.Rodrigues).
http://dx.doi.org/10.1016/j.jcol.2017.06.008
Avaliac¸ão
da
incontinência
fecal
e
impacto
na
qualidade
de
vida
por
questionários
Palavras-chave:
Incontinênciafecal Qualidadedevida Sinaisesintomas Avaliac¸ãoderesultados (cuidadosdesaúde)
ÍndicedeIncontinênciaFecal Avaliac¸ãoderesultadosde intervenc¸ãoterapêutica
r
e
s
u
m
o
Contexto: A incontinênciaanalacarreta grandeimpactonaqualidadede vida(QV)dos pacientes.Nossoestudoanalisouosprincipaisquestionáriossobreotemadisponíveisna literaturainternacional,visandodelinearvantagenselimitac¸õesdessesinstrumentosede suacorretaaplicac¸ão,bemcomocitarosaspectosculturaisenvolvidosnoprocessodesua criac¸ãoevalidac¸ão,esugerirumareflexãosobreacomplexidadedotema.
Métodos:Nessarevisãoassistemática,utilizamostrêsbasesdedadoseletrônicas(MEDLINE, LILACS,eDeCS)paraencontraros9questionáriosmaisutilizadosnomundo,e palavras-chaverelacionadas.
Resultados:Quatrodosinstrumentosestudados(Pescatoriscore,FISI,MSKCCbowelfunction instrument,eoLARSscore)nãoabordamQV,funcionandoapenasparadiagnóstico.Outros dois,o‘JorgeandWexnerFIscore’,eo‘StMarks’FIgradingsystem’diagnosticamegraduam bemaincontinência,porémapenasavaliambrevementeaQV.O‘EORTCColorectal Cancer-specific’,porsuavez,focaexclusivamentenaQV.Oquestionário‘FIQL’apesardeconseguir avaliaraQVrelacionadaàfunc¸ãointestinal,nãoavaliavazamentos.Porfim,o‘RAFIS’avalia deformamuitosimplificadaessesaspectos.
Conclusão: Nenhum dos questionários analisados se mostrou eficiente na avaliac¸ão simultâneadaincontinênciaedaQV.Alémdisso,osconceitosqueenvolvemincontinência analapresentamsignificadosdiferentesdependendodocontextoculturalepsicossocial. Essasdiferenc¸assãoaindamaiores quandosecomparamindivíduosdospaíses desen-volvidosondeessesquestionáriosforamdesenvolvidos,comosdepaísessubdesenvolvidos comooBrasil,dificultandosuaaplicac¸ãodeformauniversal.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
The fecal incontinence (FI) is an anorectal dysfunction characterizedbystool,gasand/orliquidloss,whichhas seri-ous impact on the patient’s quality of life. Thiscondition frequentlyleadstoemotionalandsocialdisturbance, impair-mentoflaborrelations,lossofself-esteemanddepression.1,2
Duetotheseverityofthiscondition,itisnecessaryto system-aticallydiagnosepatientswithFIandassesstheirdegreeof impairment.Thereareseveraltoolsthatcanbeusedaiming thisevaluation,which areknownasfecalincontinence(FI) questionnaires.Inaddition toFIdiagnosis,the assessment ofquality oflife(QoL)hasalsobecomeanimportant mea-sureofmedicaltreatmentoutcomes.Andinordertoassessit, questionnairesareappliedtopatients.However,itisnotthat simplebecausemeasuringthefunctionaloutcomeofa treat-ment,throughascore,doesnotnecessarilytranslateintoa worseQoLevenifitrevealsthemostseverescore.
In 1958,John Kenneth Galbraith created the concept of QoL differentiatingfrom the classic quantitative economic perspective. Inhis concept, the improvementofmen’s liv-ing conditionsisthe focus ofthe political–economicaland socialgoals,insteadofeconomicalandmaterialgrowth.3
Sim-ilarly,LyndonJohnson,theAmericanpresidentin1964,said thatthegoalscannotbemeasuredbyabanksbalance,butby theQoLprovidedtopeople.HewasthefirsttouseQoLasan expression.4
QoLand“standardoflife”were conceptsthatinterested onlysocialscientists,philosophersandpoliticians.Whereas, the technological advancements in medical and scientific fields contributed evenmoretotheweakeningoftheclear definition of these concepts. However, the concern about QoL withinthe humanandbiological sciences,in orderto valueparameters broaderthan symptomcontrol,mortality decreaseandlifeexpectancyincrease,contributedtoitsuse in randomized clinical trials as animportant aspect tobe assessed,beyonddrugs’efficacyandsafety.Theoncology spe-cialty isagoodexample ofhow QoLisimportant,because treatmentsinitiallysoughtonlytoadd“yearsoflife”, neglect-ingtherelevanceofadding“lifetoyears”.4
Based on this subject’s importance and on the holistic understanding ofthe concepts surrounding this condition, this review discusses the specific questionnaires for fecal incontinenceevaluation.Theaimofthisstudywastosuggest areflectionaboutthecomplexityoftheinvolvedconcepts,the limitationofaproperquestionnaireapplication,the transcul-turalaspectand thecreation andvalidationprocess ofthe instruments.
Methods
byusingtheMeSHterm“fecalincontinence”andothersterms previouslydescribedinkeywords.
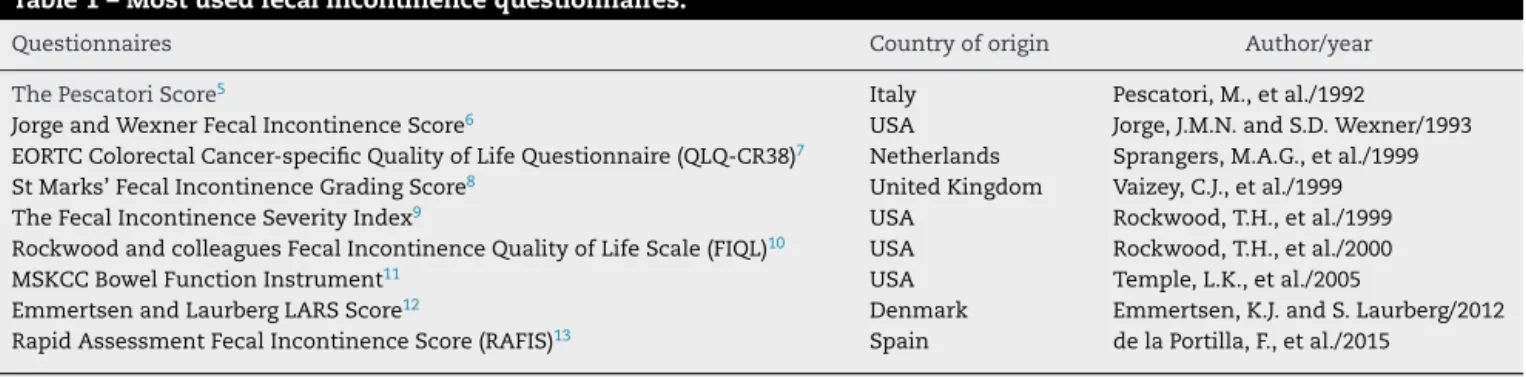
The most common available incontinence scores are showninTable1.Duetotheimportanceofearlydiagnosis of this condition in order to prevent long-term psychoso-cialimpairment,thisreviewdiscussesthemainincontinence scorediagnosticquestionnaires,theirimportanceandtheir limitations.
Conceptualaspects
Theconcept ofQoLorglobal healthstateevaluationisthe impactmeasureofapatient’sdiseaseontheirphysical,social relationsandpsychologicalhealth,whichhighlightswhatis taught in colleges about patients being the main concern beyondthediseaseitself.Etiologyisnowonlyacoexisting fac-tortobefought.14,15TheexpressionQoL,asithasbeenusedin
medicalliterature,doesnotseemtohaveonesinglemeaning andithassynonymsintheliteraturesuchas“Health condi-tions”and“socialfunctioning”.4Inaddition,QoL’sdefinition
itselfdoesnotappearinthemajorityofscientificjournalsthat useorproposeinstrumentsforitsassessment.Someauthors saythatQoLincludesendlesspossibilities,whichcanimpair notonlyhealthconditionandmedicalinterventionbut per-ception,behaviorandfeelingsrelatedtofulldailyactivities.4
ThedefinitionofhealthbytheWorldHealthOrganization (WHO)isthe complete stateofphysical,mentaland social wellbeingandnotonlydiseaseabsence.16However,morbidity
andmortalityareusuallythefocusofhealthpolicy.Nowadays otheraspectssuchasfunctionalstatus,healthperceptionand dailyactivitiesimpairmentareconsideredinordertoevaluate health.17–19
Fecalincontinencequestionnaires
Pedersenandcolleagues20werethefirstresearchersto
con-cern themselves with the anal function of patients who underwentlowanteriorresection(LAR)procedure.This pro-cedureisperformedtotreatrectalcancerandfrequentlyleads tofecalincontinence(FI)asacomplication,whichcannotbe neglected.
MOS36-ItemShort-FormHealthSurveypresentsthebasis tocreateanyqualityoflife(QoL)questionnaire,pointingout that it is important to assess physical, social and mental aspectsaswellasgeneralhealthperceptionsofthepatient.17
ThePescatoriscore,developedinUniversita’Cattolica,in Rome,Italy, wasoneofthe firstquestionnairestoevaluate fecalincontinence(FI).5Itevaluatesdegreesuchasfrequency
ofsymptomsinaveryeffectivegradingsystem.Thedegree ofincontinenceisclassifiedinA,BorCcategories,depending onthetypeofincontinence,respectivelyflatus/mucous,liquid stool,andsolidstool.Thefrequencyisclassifiedas1,2and3, indicatingrespectivelyoccasionally,weekly,anddaily incon-tinence.Alargenumberofpatientsparticipatedinthisstudy (335),anditallowedtheauthorstocomparetheirFI through-outtime.SincetheABC-123gradingsystemprovidedawayto diagrammaticallyrepresenttheresultsofatreatment,itwas veryhelpfultoanalyzetheoutcomesofsurgicalprocedures thatsomeofthesepatientsunderwent.Therefore,itis possi-bletoconcludethatthisquestionnairecanprovideaprecise
analysisofthepatient’sFI.However,thisquestionnairelacks anassessmentofthepatient’sownperceptionoftheir con-dition.Sincethefocusisonlyatthephysiologicalfunctionof thesphincter,thepatientsarenotquestionedaboutchanges intheirlifestyleandtheresultingimpactsofthesechanges. Itwouldbeadvisabletoassesswhetherornottheyarestill abletopracticesports,haveanormaldiet,havesocial rela-tionships,howtheyconsidertheirmentalhealthtobeand howtheirQoLwasaffected.
TheJorgeandWexnerScorewascreatedatClevelandClinic Florida,inFortLauderdale,USA6andisoneofthemost
fre-quently used to assess fecal incontinence. Regarding fecal incontinenceitself,thisscoreencompassesthesame ques-tionsofthePescatoriscore,howeverTheJorgeand Wexner Scorehasmoreoptionsforanswers,graduatingmoreprecisely thedegreeofincontinence.Inaddition,theconsiderationof lifestyle alterationand the use ofpads were implemented inthe score,bringingtheattention tothe patient’swelfare insteadofbeingapurelyquantitativequestionnairelikethe previous one. However, this questionnaire does not assess the presence ofurgency duringthe defecationnor the re-evacuation(clustering).
Someyearslater,in1999,aquestionnairemodulewas cre-atedtobeusedinconjunctionwiththeEuropeanOrganization forResearchandTreatmentofCancer(EORTC)QLQC30.7The
EORTCQLQC30isageneralquestionnairedevelopedtoassess theQoLofabroadspectrumofoncologicalpatients.Thisnew questionnairemodulewaspublishedintheNetherlandsand its aimwastodevelopasupplementaryquestionnaire spe-cificforpatientswithcolorectalcancer,coveringrelevantQoL issuesforthesepatients.7TheycalleditQLQ-CR38andit
con-sistsof38itemscoveringimportantaspectsofthepatient’s QoL,suchasbodyimage,sexuality,futureperspective, symp-tomsand side-effects todifferenttreatment modalitiesfor colorectalcancerpatients.7
Five cancerspecialists wereconsultedduring the devel-opmentofthe questionnaire.Then, thefirstversion ofthe questionnairewasappliedindividuallyin24colorectalcancer patients,sothatpotentialproblemscouldbeidentifiedand solved. Thepatients werealsoaskedtoindicate any omis-sions,andtogivetheiropinionaboutanyotherquestionthat shouldbeincludedinthefinalquestionnaire.7Patients
con-tributiontotheconstructionofthequestionnairealloweditto approachpatient’sQoLinarelativelysimpleand straightfor-wardway,sothatitcanbefilledoutbypatientsthemselves, withlittleornoassistance.7AnissuewiththeQLQ-CR38
how-everistheamountoftimenecessaryforreplying.Theauthors donotrecommendittobeusedasafree-standinginstrument forassessingQoLofcolorectalcancerpatients,butratherthat itbeusedtogetherwiththeEORTCQLQC30.Howeverittook anaveragetimeof10.3mintocompletebothofthem7andthat
amountoftimecouldbetoolongforverysickpatients,andnot easytobereproducedinlargescaleinadailyclinicalpractice. Anotherimportantissueinthisquestionnairewastheitems relatedtosexuality.Althoughitisanimportantsubject,3%of themenand12%ofthewomendeclinedtocompletethese itemsbecausetheywereconsideredtoointrusive.7
In the same year at the St Marks Hospital, UK, Vaizey andColleagues8developedanewquestionnaireknownasSt
Table1–Mostusedfecalincontinencequestionnaires.
Questionnaires Countryoforigin Author/year
ThePescatoriScore5 Italy Pescatori,M.,etal./1992
JorgeandWexnerFecalIncontinenceScore6 USA Jorge,J.M.N.andS.D.Wexner/1993
EORTCColorectalCancer-specificQualityofLifeQuestionnaire(QLQ-CR38)7 Netherlands Sprangers,M.A.G.,etal./1999
StMarks’FecalIncontinenceGradingScore8 UnitedKingdom Vaizey,C.J.,etal./1999
TheFecalIncontinenceSeverityIndex9 USA Rockwood,T.H.,etal./1999
RockwoodandcolleaguesFecalIncontinenceQualityofLifeScale(FIQL)10 USA Rockwood,T.H.,etal./2000
MSKCCBowelFunctionInstrument11 USA Temple,L.K.,etal./2005
EmmertsenandLaurbergLARSScore12 Denmark Emmertsen,K.J.andS.Laurberg/2012
RapidAssessmentFecalIncontinenceScore(RAFIS)13 Spain delaPortilla,F.,etal./2015
Source:MEDLINE.
establishedscales(Pescatori,Wexner,AmericanMedical Sys-tems)andthenewquestionnairewereprospectivelyevaluated bytwoindependentclinicalobserversina28-day-diary.8This
wasthefirsttimethesescales havebeencomparedwitha diarysystem,althoughthenumberofpatientsassessedwas reduced(twentythree),allfourscalescorrelatedhighlyand significantlywiththeclinicalimpressionofthetwo indepen-dentclinicians.8Furthermore,thisnewscoreincludeddetails
abouturgencyandantidiarrhealdrugs,whichwerenotfound inprevious questionnaires, and haveshown to behelpful. Atfirst,becausetheneedforantidiarrhealmedicationsmay maskandunderestimatetheunderlyingconditionand inter-fereonthepatient’sperceptionofsymptoms.Second,because thepresenceoffecalurgencyforcespatientstoremainclose toatoilet.8 Thishasalargeimpactontheir qualityoflife
sincetheabilitytopostponedefecationisessentialtoallow thepatienttobeinvolvedinmanysocialsituations,affecting theirpsychosociallifeandbehavior.
Apparently,atthat timeall majorscientistsofthe field hadrealizedthatlifestylechangeisofgreatimportanceon patient’squalityoflife,andthus,needstobeaddressedlike the anal dysfunction itself.However, despite the improve-mentswhencomparedtopreviousquestionnaires,StMarks’ Fecal Incontinence Grading Score does not make it clear whetheror notpatients areaskedabout theirown percep-tionoftheircondition,andhowtheyfeelaboutit,andhow welltheyaredealingwithit.Thesequestionsmightbereally importanttoassesstheQoL.
Alsoin1999Rockwoodetal.9 developedintheUSAthe
Fecal Incontinence Severity Index (FISI), based on patient andsurgeonrankingsoftheseverityofsymptomsassociated withfecalincontinence.Althoughtheindexevaluates ade-quatelythelevelofsphincterdysfunction,itdoesnotconsider patient’sQoLortheirpsychosocialsituation.Accordingtothe authors,differentpatientsareaffectedbythesamelevelof incontinenceindifferentwaysandconsequentlyQoL ques-tionswerenotincludedintheindex.Despitethatexplanation, anassessmentregardingpatient’sQoLshouldbeconsidered asanindicatorasfarasaseverityindexisconcerned.The indexcouldperhapsincludeaspecifictooltomeasurehow QoLisaffectedbytheFI.Suchatoolwouldallowthegathering ofdatathatcouldimprovetheaccuracyoftheindex.
Inaddition, theFISIisbasedonatypeversusfrequency matrix presented to surgeons and patients who evaluated anddefinedthelevelofseverityofeachtypeofdysfunction. The matrix was based on the four components of fecal
incontinence(gas,mucous,liquid andsolid stools),and on five frequencytimeframes.9 However, thetimeframes were
pre-established:twoormoretimesperday,onceperday,two ormoretimesperweek,onceperweek,andonetothreetimes permonth.9Thatisalimitationofthemethod,oncedifferent
frequenciesareplacedonthesametimeframe.Forexample, apatientwithasolidstoolincontinenceofoncepermonth has a very different condition when compared to another withasolidstoolincontinenceofthreetimespermonth,and stillthesetwocaseswerenotseparatelyconsidered.
Furthermore,12patientscompletedtheformthroughthe mail,while22completedtheforminasurgeryclinic.9Even
thoughtheauthorsaffirmedtherewasnosignificant differ-enceintherankingofthesetwogroups,itwouldbeexpected thatallparticipantsfilledouttheformunderthesame condi-tions,astherecouldbeinfluenceofoutsidefactors.9
In 2000, Rockwoodet al.10 developed another
question-naire, theFIQL,whichevaluatesthepsychosocialaspectof patients. Thequestionnaire iscomposedof4 categoriesof questions: Lifestyle (10 items), Coping/Behavior (9 items), Depression/Self-Perception(7items),andEmbarrassment(3 items). Rockwood and colleagues stated the importanceof patient’squalityoflifeinthispaper,startingthequestionnaire withanuncommonquestionsofar:“Ingeneral,wouldyousay yourhealthis–excellent,verygood,good,fairorpoor.”.9It
alreadyhavedepression,anxietyoranotherdisorder,before theFI.
Thereisarepeatedquestion,“Q2.f.WheneverIamaway fromhome,Itrytostayneararestroomasmuchas possi-ble”and“Q2.m.Itry topreventbowelaccidentsbystaying verynearabathroom”.Wasthisdeliberated?Ifso,thereisno explanationinthepaper.Wouldn’titgivemoreweighttothis sessionofthequestionnaire?
Thisscalealsoevaluatesthe changesinlifestyle asking aboutdifferent socialsituations,which canimpactsocially andpsychologically.However,itiscontroversialwhatisthe role of each social situation on the patient’s QoL. Which changesshouldweightmoreorless?Howdowegiveavalue forsomethingthatistotallysubjective?Socialsituationsthat impactonsomeone’slifevaryamongthepatients,even fur-ther,amongcountriesandcultures,whichstatestheneedof buildingaFIscorespecificforourpopulation,inBrazil.Part ofthisaspectwasalreadyflaggedintheirdiscussionandisa problemthatremains.
In New York, 2005, Temple and colleagues published theMSKCCBowelFunction Instrument.11 Their instrument
wasbuiltbasicallytoassessbowelfunction,especiallyafter sphincter-preserving surgeryfor rectal cancerand, accord-ingtothequestionnaire,itsquestionswereonlyaboutbowel movementrelatedsituations.11Itlookslikeamoredetailed
Wexner Incontinence Score, although it does not assess any aspectsof mentalhealth and quality oflife. However, they have used QoL questionnairesto compare with their instrument,11insteadofusingWexner’s.MSKCCBowel
Func-tionInstrumentisabletodeterminepoorbowelfunctionofthe patients,butitwashighlightedthattherewasnosignificant correlationsondivergentvalidity, inall subscales,withthe QoLinstrumentsusedintheirstudy.Itissuggestedthatbowel functionmight be confounding the studies on QoL instru-mentsthat assess bothQoL andfecal incontinence,which statesthe importanceof continuingthe studies on instru-mentslikeMSKCC.11Theseconclusionsneedtobeconsidered
whendevelopingaquestionnairefortheBrazilianpopulation. WestilldonothavespecificFecalIncontinenceScoresforthe Brazilianpopulation, whichmeans we are well behindthe studiesrequiredforit.
InDenmark,in2012,EmmertsenandLaurbergpublished theLARSScore.12Itwasdevelopedtoevaluatethelow
ante-riorresectionsyndrome,whichisanimportantcauseoffecal incontinenceafterrectalcancertreatment.Thisisalsoagood example of ascore that assess the patient’s symptoms in which the authors correlated their score tothe impacton QoL,althoughothergradingsystemshavealreadyshownthat thesecorrelations are not well understood and the results arevariable.TheLARS Scorewasspecificallymadeto clas-sifypatientsinthreecategories:without LARS,withminor LARSorwithmajorLARS.Allofthequestionsaskonlyabout fecalincontinence situations or about bowel habit,similar tothe questionsintheMSKCCBowelFunctionInstrument. However,MSKCC’sinstrumentisamuchlongerquestionnaire comparedwithLARSScore,whichisshorterandeasiertouse indailypractice.
Intheirstudy,EmmertsenandLaurberg12highlightedthe
importanceofaninstrumentthatcouldquantifyQoL,instead of onlysymptoms. Therefore they aimed to build a score
capableofassessingthe patientasawhole,specificallyfor boweldysfunctionafterlowanteriorresection(LAR).Despite pointing out importantaspects and deficiencies especially about the Wexner Incontinence Score, the RockwoodFecal IncontinenceSeverityIndexandtheStMark’sFecal Inconti-nenceGradingScore,theauthorsdidnotmentionavailable QoLscoresforvalidationsuchastheFIQL,whichwouldbe importantforcomparingtoLARSscore.
Finally,inSeville,Spain,theRAFISwaspublishedbydela Portillaetal.in2015.13Itisaninnovativeincontinencescore
and the most onerecently created to ourknowledge. Itis simpleandfasttobeused.Intheirarticle,delaPortillaand colleaguescomparedtheirinstrumenttobothJorge–Wexner andFIQLinordertoshowthereliabilityoftheirtooltoassess incontinenceandQoL.
The RAFIS is interesting because of its simplicity. It is composedofbasicallytwoaspects:thepatient’simpression abouttheirfeelingandthefrequencyofleaks(gas,liquidor solidstool).Thefirstquestioniscomposedbyavisualscale, in which the patient sees different facial expressions and choosesoneamongsixtorepresenttheirfeelingsabouttheir clinical condition.Itiseasy understandingandcorrelateto reality,whichwhollyfitsinto apurposeofcreatingarapid assessment.Thesecondquestionisimpressiveinsimplifying themeasureofleakageoncetheauthorsdonotdiscriminate betweengas,liquidandsolidstoolleakageandalso,donotask aboutdifferentsocialsituationsrelatedtofecalincontinence, useofmedicationsorurgency.Thepatientisbasicallyasked aboutfrequencyofleaks.
ThesimplicityofRAFISisadmirable.However,thesample sizeusedtodevelopthisinstrumentshouldbehigherinorder toimprovecorrelationandsignificancerates.Moreover,the test–retesttoolwasnotperformed,whichwasalready high-lightedbytheauthors.Despitethoselimitations,itwouldbe interestingtoseesuchasimpleinstrumentvalidatedinBrazil toanalyzeits performanceinourpopulation, inwhich the averageeducationalstatusislow.
Discussion
Many studies have been misusing questionnairesmade to assess the functional status of the anal sphincter, such as LARS Score, to measure QoL. Emmertsen and Laurberg themselves stated in their article that their instrument is a diagnostic one, nota QoL measurement.12 The concepts
whichitlives,andinregardstoitsobjectives,expectations,standards andconcerns”.21
Inparalleltotheconcept’scomplexity,therearethe limi-tationsofthequestionnaires,whicharesomanythatthereis noconsensusofwhetheritisbettertouseoneinstrumentto assessanddiagnoseQoLsimultaneouslyortwoinstruments, oneforeachaspect.Noneoftheavailablequestionnairesare abletopreciselymeasurebothFIdegreeandQoL.The Pesca-toriscore,FISI,MSKCCbowelfunctioninstrumentandLARS scoreareonlydiagnosticinstruments,whichaskstrictlyabout bowel function.5,9,11,12 The Jorge and Wexner FI score and
StMarks’ FIgradingsystem aregreat indiagnosingFIand gradingit,howeverareverysubtleinassessingQoLdespite showingsomeinterest inthistopic.6,8 TheEORTC
Colorec-talCancer-specificonlyassessesQoL,nodiagnosticfeatureof FIisconsidered.7TheFIQLisgreatinassessingQoLrelated
toFI,consideringmanyday-to-daycontextsrelatedtobowel function,howeveritdoesnotmeasureleakage.10AndRAFIS
measuresbothFIandQoL,howeveritissuchasimple ques-tionnairethatitisnotclearwhetherornotitisappropriate, requiringmorestudies.13
Inaddition,thereisthelimitationofapplyingthe question-nairesindifferentpopulations,groupsandcultures.Asstated before,QoLdependsonpeople’sbackgroundandchangeover time. It leads us to question if it is appropriate to apply thesequestionnaires,forexample,inpopulations fromthe intertropicalzonewhiletheyweremadeinstudieswith popu-lationsfromareasthathaveseverewinter.InBrazil,people are notusedto coldweatherlike inEuropeand therefore, there is no culture of using heavy clothing and covering the wholebody forlong periods, thenotionofbody expo-sureandbodyimageiscompletelydifferent.Andthebarrier betweendifferentgroupsgoesinallkindsofcontexts,habits, religions, sports, work, daily activities. It is even possible that within the same population, there are some groups, which havedifferent performanceson the same question-naire.
DuringthecreationprocessoftheidealFIquestionnaire,it isnecessarytoconsideralltheaspectsstatedabove,inorderto createatimelessandnoculturalinstrumentortorealizethat eachpopulationneedsitsownquestionnaire.Itisan undeni-ablefactthatthecreationandvalidationofinstrumentsfor differentlanguagesareaffectedbythetransculturalaspectof eachpopulation.
The patients need our empathy while we create ques-tionnaires to measureany of their conditions, which lead us to imaging how difficult it is to understand any ques-tionsometimesandhowdifficultit istoanswer aquestion when you are not completely sure you understand it. We use tointerpretthings basedon ourpsycho-social-cultural backgroundand, thatcan change betweenindividuals and betweendifferentregionsinthesamecountry(North, North-east,Southeast,SouthandMidwest),especiallyinacountryas bigasBrazil.Anddefinitelythereareremarkablecultural dif-ferencesbetweendevelopedanddevelopingcountries.Thus, thisdiscussionisimportant,asitishardfordoctorstouse atoolthat isnotadaptedtotheircountries’ epidemiology, hencemakingthequestions,applyingthequestionnairesand obtainingpreciseanswersandevaluationsisadifficult pro-cess.
Thecountriesoforiginofeachquestionnairewere inten-tionallycitedtohighlightthefactthatnoincontinencescore was ever created in Brazil. Until the present moment, no incontinencescorewas developedandpublishedby Brazil-ianinstitutions.Furthermore,alltheincontinencescoresused worldwidewerecreatedbystudiesinthedevelopedcountries. InBrazil,thereareonlythreeincontinencescoresvalidated inPortuguese,which arethe Wexnerscore, FIQLand LARS score.22–24Therefore,wearelimitedtothreetools,whichare
validatedtoourreality,toassessfecalincontinenceandFIQL, theonlyoneappropriateforQoL.Theothersweuseinour routine,wehavetoimprovise,totranslateanduseasprotocol, adaptthebestwecanforeachsituation.
AlthoughtheHumanDevelopmentIndex(HDI)isnotthe mostreliable indextodeterminea country’shuman devel-opment, itcanbeusedalong withotherparameterstosee thedifferencesbetweendevelopedanddevelopingcountries. Brazil,forexample,hasanHDIof0.755,75thintheworld,a GrossNationalIncome(GNI)percapitaofU$15,175.00,aGini coefficientof52.7.25Inaddition,inourcountryonly57.6%of
thepopulationhasinternetaccessand53.6%,above25years old,have atleastsomesecondaryeducation.On the other hand,theUnitedStatesofAmerica(USA),forexample,hasan HDIof0.915,9thintheworld,aGNIpercapitaofU$52,946.50,a Ginicoefficientof41.1,associatedwithapopulation,inwhich 87.4%hasinternetaccessand95%hasatleastsomesecondary education.TheUSApopulationhasagreatereducationallevel, internetaccess,anincomeatleastthreetimeshigheranda lowerlevelofinequality.25
Realproblemshavebeenbeingneglectedbyacademicsdue toovervaluationofrigor,whichisrelatedtotheincreasing useofsophisticatedmathematicaloreconometric quantita-tive techniques. In many centers,rigor hasacquired more importancethan practicalrelevance.Againstthis tendency, wescientists, havethedutytohighlight theconsequences of overvaluing rigorrather than relevance whileanalyzing biopsychosocial problems. According toGalbraith, real and practicalproblemsundereconomicalanalysis“needtoconsider theinformation fromother disciplinesas wellas politicalreality, noteasilylendingourselvestohighlytechnicalandmathematical treatment”.3
Inidealconditions,evenavalidatedquestionnairewould work properly,4 butinBrazilwehaveacompletelyvariable
reality.In2016,aPhDthesistovalidateLARSScoreto Por-tuguesefaceda12.6%rateofpatientsthatcouldnotreadand a52%rateofpatientsthatdidnothaveevenaprimaryschool education.24
These instruments have a wide variety of applications, includingindividualclinicalpracticeand,evaluationof treat-ment effectiveness and health service functioning among them.Life’scomplexityispicturedi0nthe existing difficul-ties in developing instruments and in understanding the concepts.4,26
owninstrument,assuggestedbythefactthatitisnotonly neededtovalidatefecalincontinencequestionnaires,itisalso necessaryasameanstogofurther?
Allofthefecalincontinencequestionnaireswerecreated inadevelopedcountryand,fouroutofnineanalyzedinthis reviewwerebuiltintheUnitedStatesofAmerica(USA). Com-paringthosedata fromBrazil totheUSA, it isnotdifficult toconclude that validating questionnairesfrom developed countriesindevelopingcountriesmightnotbeappropriate. Theworkinvolvedincreatingaquestionnaireismuchgreater thanthevalidationprocess.SoBrazilianresearchersand insti-tutionsneedstowork ondevelopingthis capacity.So,why notcreateourownquestionnaireswithourownscores?Our opinionasauthorsofthisarticleisthatsubjectivitymaynot becopied,butcreated.Therateofsuccesswouldbehigherif questionnairesaboutpatient’sintimacywerenotcopiedfrom acompletelydifferentculture,butdevelopedlocallyinstead. Ifthescenariowereideal,wecouldenvisionamedicalteam attendingapatientcapableofrespondingtoaquestionnaire inareliableway,evenifthisquestionnairewerevalidated.
We would like to congratulate all of the authors who dedicatetheirtime,studyingthisarea,producinghighlevel publications,whichwillalwaysserveasthestartingpointfor newresearch.
Conclusions
Theapplicationofquestionnairesforfecalincontinenceand QoLassessmenthasapositiveimpactbecausetheyinclude the improvement not only of individual clinical practice, but also ofevaluating the effectiveness oftreatments and thefunctioningofhealthservices. Inaddition, theycan be importantguidesforhealthpolicies.Certainly,thereare innu-merableconceptualandrealdevelopingdifficulties,duringthe developmentofthesetoolsinareliableandreproducibleway toevaluatequalityoflifeandthatthesechallengesneedto beaddressed.Despiteallthedifficultiesandrestrictions,itis alreadypossibletobetteridentifyandtreatpatientswhoare evaluatedusingquestionnairesthanwithoutapplyingthem. Thisreflectsthebeginningofanewunderstandingand expec-tation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. BravoGutierrezA,MadoffRD,LowryAC,ParkerSC,BuieWD, BaxterNN.Long-termresultsofanteriorsphincteroplasty.Dis ColonRectum.2004;47:727–31,discussion731–2.
2. GlasgowSC,LowryAC.Long-termoutcomesofanalsphincter repairforfecalincontinence:asystematicreview.DisColon Rectum.2012;55:482–90.
3. GalbraithJK.Asociedadeafluente.SãoPaulo:Editora Pioneira;1958.
4.FleckMPA,LealOF,LouzadaS,XavierM,ChachamovichE, VieiraG,etal.Desenvolvimentodaversãoemportuguêsdo instrumentodeavaliac¸ãodequalidadedevidadaOMS (WHOQOL-100).RevBrasPsiquiatr.1999;21:19–28.
5.PescatoriM,AnastasioG,BottiniC,MentastiA.Newgrading systemandscoringforanalincontinence.Evaluationof335 patients.DisColonRectum.1992;35:482–7.
6.JorgeJM,WexnerSD.Etiologyandmanagementoffecal incontinence.DisColonRectum.1993;36:77–97.
7.SprangersMA1,teVeldeA,AaronsonNK.Theconstruction andtestingoftheEORTCcolorectalcancer-specificqualityof lifequestionnairemodule(QLQ-CR38).European
OrganizationforResearchandTreatmentofCancerStudy GrouponQualityofLife.EurJCancer.1999;35:238–47.
8.VaizeyCJ,CarapetiE,CahillJA,KammMA.Prospective comparisonoffaecalincontinencegradingsystems.Gut. 1999;44:77–80.
9.RockwoodTH,ChurchJM,FleshmanJW,KaneRL, MavrantonisC,ThorsonAG,etal.Patientandsurgeon rankingoftheseverityofsymptomsassociatedwithfecal incontinence.DisColonRectum.1999;42:1525–31.
10.RockwoodTH,ChurchJM,FleshmanJW,KaneRL,
MavrantonisC,ThorsonAG,etal.FecalIncontinenceQuality ofLifeScale:qualityoflifeinstrumentforpatientswithfecal incontinence.DisColonRectum.2000;43:9–16,discussion 16–7.
11.TempleLK,BacikJ,SavattaSG,GottesmanL,PatyPB,Weiser MR,etal.Thedevelopmentofavalidatedinstrumentto evaluatebowelfunctionaftersphincter-preservingsurgery forrectalcancer.DisColonRectum.2005;48:
1353–65.
12.EmmertsenKJ,LaurbergS.Lowanteriorresectionsyndrome score:developmentandvalidationofasymptom-based scoringsystemforboweldysfunctionafterlowanterior resectionforrectalcancer.AnnSurg.2012;255:922–8.
13.delaPortillaF,Calero-LilloA,Jiménez-RodríguezRM,Reyes ML,Segovia-GonzálezM,MaestreMV,etal.Validationofa newscoringsystem:rapidassessmentfaecalincontinence score.WorldJGastrointestSurg.2015;7:203–7.
14.MartinezJE,FerrazMB,SatoEI,AtraE.Fibromyalgiavs rheumatoidarthritis:alongitudinalcomparisonofqualityof life.JRheumatol.1995;22:270–4.
15.BIREME.DeCS–DescritoresemCiênciasdaSaúde;2016.São Paulo.http://decs.bvs.br/
16.WHO.ConstitutionoftheWorldHealthOrganization.New York:W.H.Organization;1946.
17.WareJEJr,SherbourneCD.TheMOS36-ItemShort-Form HealthSurvey(SF-36).MedCare.1992;30:473–83.
18.BergnerM,BobbittRA,CarterWB,GilsonBS.Thesickness impactprofile:developmentandfinalrevisionofahealth statusmeasure.MedCare.1981;19:787–805.
19.FleckMPA,LousadaS,XavierM,ChachamovichE,VieiraG, SantosL,etal.Aplicac¸ãodaversãoemportuguêsdo instrumentodeavaliac¸ãodequalidadedevidada Organizac¸ãoMundialdaSaúde(WHOQOL-100).RevSaúde Públ.1999;33:198–205.
20.PedersenIK,ChristiansenJ,HintK,JensenP,OlsenJ, MortensenPE.Anorectalfunctionafterlowanterior resection.AnnSurg.1986;204:133–5.
21.TheWHOQOLGroup.TheWorldHealthOrganizationquality oflifeassessment(WHOQOL):positionpaperfromtheWorld HealthOrganization.SocSciMed.1995;41:1403–9.
22.FonsecaAM,MeinbergMF,LucasDV,MonteiroMV,Figueiredo EM,FonsecaL,etal.Culturaladaptationandvalidationofthe Wexnerscaleinpatientswithanalincontinenceina Brazilianpopulation.IntUrogynecolJ.2016;27:959–63.
validac¸ãodoquestionárioFIQL[Fecalincontinencequalityof life].ArqGastroenterol.2004;41:202–8.
24.RodriguesKCL.Validac¸ãoparaoBrasildoEscore“LARS”de Avaliac¸ãodaSíndromePós-Ressecc¸ãoAnteriordoReto.Belo Horizonte.Tese.UniversidadeFederaldeMinasGerais;2016. p.62.
25.UNDP,Brazil.Humandevelopmentreport2015.United Nations:undp.org;2015.