KNOW LEDGE ON DI ABETES MELLI TUS I N THE SELF CARE PROCESS
1Ana Em ilia Pace2 Kat t ia Och oa- Vigo3 Mar ia Helena Lar cher Calir i2 Ana Paula Mor ais Fer nandes2
Pace AE, Ochoa- Vigo K, Calir i MHL, Fer nandes APM. Know ledge on Diabet es Mellit us in t he self car e pr ocess. Rev Lat ino- am Enfer m agem 2 0 0 6 set em br o- out ubr o; 1 4 ( 5 ) : 7 2 8 - 3 4 .
This descript ive st udy in t he int erior of São Paulo aim ed t o verify diabet es m ellit us pat ient s’ knowledge abou t t h e disease, cau ses an d com plicat ion s, h igh ligh t in g it s im por t an ce in self car e. Dat a w er e collect ed t h r ou gh in t er v iew s w it h 8 4 per son s an d an aly zed t h r ou gh descr ipt iv e st at ist ics. Av er age age w as 5 3 . 3 ± 1 3 years, t im e of disease 12.9± 9 years and 58% of t he part icipant s did not finish basic educat ion. Only 28.6% of t he par t icipant s gav e cor r ect answ er s t o “ w hat is diabet es” and “ w hat ar e it s causes” ; 71% w er e diagnosed w it h ou t p r esen t in g classic sy m p t om s an d 6 4 % h ad alr ead y b een h osp it alized d u e t o an acu t e or ch r on ic com plicat ion . We in dicat ed aspect s t h at t u r n t h e lear n in g pr ocess m or e difficu lt ; lit t le k n ow ledge abou t t h e disease, it s causes and sym pt om s, t hus affect ing t he prevent ion and early diagnosis and ent ailing predisposit ion t ow ar ds com plicat ion s. Fu r t h er m or e, t h e in t er f er en ce of biopsy ch osocial f act or s in t h e self car e pr ocess is h igh ligh t ed.
DESCRI PTORS: nur sing; diabet es m ellit us; k now ledge and self car e
EL CONOCI MI ENTO SOBRE DI ABETES MELLI TUS EN EL PROCESO DE AUTOCUI DADO
Est udio descript ivo realizado en el int erior de São Paulo, cuyo obj et ivo fue verificar el conocim ient o de las per son as con diabet es m ellit u s en r elación con la en f er m edad, cau sas y com plicacion es su bsecu en t es, dest acan do su im por t an cia en el au t ocu idado. Los dat os f u er on r ecolect ados en 8 4 per son as por m edio de ent r ev ist a y analizados m ediant e est adíst ica descr ipt iv a. La edad m edia fue de 5 3 , 3 ± 1 3 años, t iem po de la enferm edad de 12,9± 9 años y 58% de los part icipant es t enían prim aria incom plet a. Apenas 28,6% respondieron cor r ect am ent e sobr e “ qué es diabet es” y “ cuáles sus causas” ; 71% fuer on diagnost icados sin la pr esencia de los sínt om as clásicos y , 6 4 % y a habían sido int er nados por alguna com plicación aguda o cr ónica. Se indicó aspect os que dificult an el pr oceso de apr endizaj e, poco conocim ient o en r elación con la enfer m edad, et iología y sínt om as, com pr om et iendo la pr evención y el diagnóst ico pr ecoz, pr edisponiéndolos a las com plicaciones. Se r esalt an la int er fer encia de los fact or es biopsicosociales en el pr oceso de aut ocuidado.
DESCRI PTORES: enfer m er ía; diabet es m ellit us; conocim ient o y aut ocuidado
O CONHECI MENTO SOBRE DI ABETES MELLI TUS NO PROCESSO DE AUTOCUI DADO
Est udo descr it ivo r ealizado no int er ior paulist a, cuj o obj et ivo foi ver ificar o conhecim ent o das pessoas com diabet es m ellit us em r elação à doença, causas e com plicações adv indas, dest acando sua im por t ância no aut ocuidado. Os dados foram colet ados de 84 pessoas por m eio de ent revist a e analisadas m ediant e est at íst ica descrit iva. A m édia de idade foi 53,3± 13 anos, t em po de doença 12,9± 9 anos e 58% dos part icipant es t inham ensino fundam ent al incom plet o. Verificou- se que apenas 28,6% incluíram - se na cat egoria corret a sobre “ o que é diabet es” e “ quais suas causas” ; 71% foram diagnost icados sem apresent ar sint om as clássicos e 64% foram int er nados por algum a com plicação aguda ou cr ônica. I ndicou- se, aqui, aspect os que dificult am o pr ocesso de apr endizagem , pouco conhecim ent o em r elação à doença, et iologia e sint om as, com pr om et endo a pr ev enção e diagn óst ico pr ecoce, além da pr edisposição par a as com plicações. Ressalt a- se a in t er fer ên cia dos fat or es biopsicossociais n o pr ocesso de au t ocu idado.
DESCRI TORES: enfer m agem ; diabet es m ellit us; conhecim ent o e aut ocuidado
D isponible e n ca st e lla no/ D isponíve l e m língua por t ugue sa SciELO Br a sil w w w .scie lo.br / r la e
1
I NTRODUCTI ON
C
hronic healt h condit ions are responsible for6 0 % o f t h e g l o b al d i sease b u r d en . I n d ev el o p i n g count ries, t reat m ent adherence reaches a m ere 20% , generat ing negat ive healt h st at ist ics and ent ailing high cost s for fam ilies, societ y and gov er nm ent s( 1).
I n t h is gr ou p of h ealt h con dit ion s, diabet es m ellit u s st an d s ou t b ecau se of h ig h m or b id it y an d m ort alit y rat es, as well as increasing prevalence levels. Diabet es m ellit us requires clinical care and perm anent educat ion t o prevent acut e and chronic com plicat ions( 2). Am b ig u it ies an d u n cer t ain t ies p r ov ok ed b y diabet es m ellit us lie at t he basis of pat ient s’ dem ands/ n eed s, w h ich can b e im m ed iat e or lon g t er m . Th e d em an d s/ n eed s d er iv in g f r om d iab et es h av e b een cat egor ized as psy chosocial, self- car e and r elat ed t o k now ledge and sk ills( 3).
Th u s, i n t e g r a l ca r e f o r d i a b e t e s p a t i e n t s sh o u l d co v e r p sy ch o so ci a l a n d cu l t u r a l a sp e ct s. Th e r a p e u t i c e d u ca t i o n i s f u n d a m e n t a l t o i n f o r m , m ot ivat e and st rengt hen pat ient s and fam ilies t o live w it h t he chr onic condit ion. Each car e session needs t o reinforce healt h risk percept ion, skills developm ent and m ot iv at ion t o ov er com e t his r isk( 4).
Acco r d i n g t o l i t e r a t u r e , h e a l t h ca r e t h a t p r o v i d e s a d e q u a t e i n f o r m a t i o n , s u p p o r t a n d m onit oring can im prove adherence, w hich w ill reduce t he burden of chronic condit ions and provide a bet t er qualit y of life t o diabet es pat ient s( 1). I n t his sense, it is im port ant t o be able t o det ect and act on t he pat ient ’s signs of readiness for behavior and lifest yle changes( 3). Wit h a v iew t o suppor t ing car e for diabet es m ellit us pat ient s and ident ifying probable fact ors t hat intervene in this process, this study aim ed to verify these pat ien t s’ k n ow ledge abou t t h e disease, cau ses an d com plicat ions, highlight ing it s im port ance in self- care.
METHODOLOGY
We ca r r i e d o u t a d e scr i p t i v e a n d cr o ss-sect ional st udy at t he Endocr inology and Met abology Ou t p a t i e n t Cl i n i c o f t h e Cl i n i ca l H o sp i t a l a t t h e Univ er sit y of São Paulo at Ribeir ão Pr et o College of Nu r sin g ( HCFMRP- USP) , Br azil, b et w een Ap r il 2 0 0 0 an d Ap r il 2 0 0 1 . Du r in g t h is p er iod , 6 5 9 m ale an d fem ale pat ient s wit h diabet es m ellit us were at t ended, who were older t han 20. Eight y- four of t hese pat ient s v olunt eer ed for t he st udy.
Pa r t i c i p a n t s w e r e s e l e c t e d t h r o u g h t h e ou t pat ien t car e files an d w er e in v it ed t o par t icipat e
when t hey cam e t o t he clinic. Volunt eers received and signed t he fr ee and infor m ed consent t er m .
Dat a w er e collect ed t h r ou g h an in t er v iew , h eld in a p r iv at e r oom . Th e r esear ch er an d / or h er assist ant applied a sem i- st ruct ured inst rum ent before or aft er t he m edical appoint m ent . I nt erview s t ook an av er age of 45 m inut es.
The inst r um ent w as pr ev iously subm it t ed t o face and cont ent validat ion by professionals act ive in t his area and t est ed during t he pilot st udy. Modificat ions w e r e m a d e o n t h e b a si s o f t h e su g g e st i o n s a n d difficult ies/ lim it at ions t hat had been ident ified. The first p ar t of t h e in st r u m en t in clu d ed d em og r ap h ic d at a, abou t sm ok in g an d seden t ar in ess; t h e secon d par t covered dat a relat ed t o knowledge about t he disease, su ch as: w h at is diabet es an d w h at ar e it s cau ses, l ab o r at o r y t est s f o r d i ag n o si s an d co n t r o l an d , i n addit ion, acut e and chronic com plicat ions.
Answ er s r elat ed t o know ledge and causes of diabet es w er e classified in t h e follow in g cat egor ies: correct, partially correct, wrong and does not know. For the correct category, a m inim um of two correct answers w as consider ed, against one for t he par t ially cor r ect cat eg or y ; t h e w r on g cat eg or y r ef er r ed t o in cor r ect answers and those not related to the question; does not know was used when the patient expressed this phrase. Dat a w er e an aly zed t h r ou g h cat eg or izat ion an d t r an scr ipt ion in t o a st r u ct u r ed dat abase, u sin g Ex cel . Th en , d at a w er e p r o cessed i n EPI I NFO, b y m eans of descr ipt iv e st at ist ics.
Th is st u d y w as ap p r ov ed b y t h e Resear ch Et hics Com m it t ee at t he HCFMRP- USP.
RESULTS
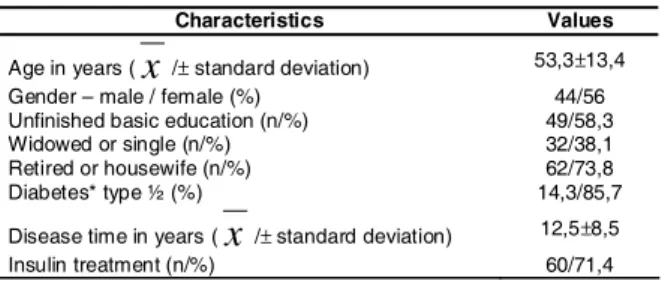
Th e st u d y p o p u l a t i o n ’ s a v e r a g e a g e w a s 5 3 . 3 ± 1 3 . 4 y ear s, 5 8 . 5 % possessed less t h an eigh t y ear s of educat ion and 38. 1% w er e w idow ed/ single. Av er age disease t im e as in dicat ed by pat ien t s w as 12.5± 8.5 y ear s ( Table 1) .
Table 1 - Sociodem ographic and clinical charact erist ics ( n= 84) . Ribeir ão Pr et o- SP, 2001
%JCTCEVGTKUVKEU 8CNWGU
#IGKP[GCTU
Z
rUVCPFCTFFGXKCVKQP r)GPFGTŌOCNGHGOCNG
7PHKPKUJGFDCUKEGFWECVKQPP
9KFQYGFQTUKPINGP
4GVKTGFQTJQWUGYKHGP
&KCDGVGUV[RG
&KUGCUGVKOGKP[GCTU
Z
rUVCPFCTFFGXKCVKQP r+PUWNKPVTGCVOGPVP
Ta b l e 2 s h o w s a n s w e r c a t e g o r i e s a b o u t w h a t i s d i a b e t e s ? a n d w h a t a r e i t s c a u s e s ?
Table 2 - Know ledge about diabet es and it s causes ( n= 84) . Ribeir ão Pr et o, 2001
An sw e r s w e r e cr o sse d t o h i g h l i g h t p a r t i ci p a n t s’ k n o w l e d g e .
W h e n p a r t i c i p a n t s w e r e a s k e d a b o u t
n or m al b lood g lu cose lev els, on ly 2 4 ( 8 . 6 % ) g av e
a cor r ect an sw er, i. e. b et w een 7 0 an d 1 1 0 m g / d l,
w h ile 2 1 ( 2 5 % ) m en t ion ed on ly on e of t h ese lev els.
Tw e n t y - t w o p a r t i ci p a n t s’ a n sw e r s ( 2 6 . 2 % ) w e r e
con sid er ed in cor r ect b ecau se t h ey d id n ot f it in t o
t h i s r a n g e a n d 1 7 ( 2 0 . 2 % ) p a t i e n t s c o u l d n o t
a n sw e r.
I n v i ew o f t h e i m p o r t a n ce o f r eco g n i zi n g
s i g n s a n d s y m p t o m s o f t h e d i s e a s e a n d e a r l y
d i a g n o s i s , w h i c h c a n m o t i v a t e p e o p l e t o s e e k
p r o f essi o n al h eal t h car e, p ar t i ci p an t s w er e ask ed
abou t t h e m ain com plain t s t h at led t o t h e diabet es
d iag n osis ( Tab le 3 ) .
Table 3 - Sy m pt om s t h at led t o diabet es diagn osis
( n= 83) . Ribeir ão Pr et o, 2001
* Annual rout ine consult at ion
We also v er if ied w h et h er par t icipan t s k n ew
t h a t b a d l y c o n t r o l l e d d i a b e t e s c a n c a u s e o t h e r
h e a l t h p r o b l e m s . Ei g h t y - o n e ( 9 6 . 4 % ) g a v e a
p o si t i v e a n sw e r a n d i n d i ca t e d a cu t e a n d ch r o n i c
co m p l i ca t i o n s. Ta b l e 4 d i sp l ay s t h e 2 7 6 a n sw e r s
w e o b t a i n ed .
Tab le 4 - Healt h p r ob lem s r elat ed t o or cau sed b y diabet es ( n= 81) . Ribeir ão Pr et o, 2001
s e t e b a i d n a c s m e l b o r p t a h W ? h t l a e h r u o y o t e s u a c s r e w s n a e l p i t l u M y c n e u q e r
F % Accumulated a i m e c y l g r e p y
H 47 56,0 47 a i m e c y l g o p y
H 38 45,2 85 a
m o
C 11 13,1 96 s i s o d i c a o t e
K 5 6,0 101 s m e l b o r p y e n d i
K 26 31,1 127 s m e l b o r p e y
E 40 47,6 167 l a u x e S l a n it s e t n i o r t s a g / e c n e t o p m i s m e l b o r p 6
2 31,0 193
s m e l b o r p r a l u c s a
V 29 34,5 222 s m e l b o r p t o o
F 39 46,4 261 r
e h t
O 15 17,9 276 ? s e t e b a i d s i t a h W s e t e b a i D f o s e s u a C t c e r r o
C Partially correct Wrong Doesnotknow
l a t o T , y r a t i d e r e H s s e r t s , e l y t s e f i
l Hereditaryorlifestyle
e h t o t d e t a l e r t o N e s a e s i
d Doesnotknow
t c e r r o C s e o d , s m e l b o r p s a e r c n a P s e o d , n il u s n i e c u d o r p t o n r a g u s n r u b t o n 4
2 - - - 24
t c e r r o c y ll a it r a
P Highbloodsugarlevel 15 15 - 6 36 g
n o r
W Notrelatedtothedisease - - - 6 6 w o n k t o n s e o
D Doesnotknow - - - 18 18 l
a t o
T 39 15 - 30 84
y b d e n o i t n e m s t n i a l p m o C s t n a p i c i t r a p s r e w s n a e l p i t l u M y c n e u q e r
F % Accumulated s m e l b o r p t h g i
S 11 13,3 11 a i s p i d y l o
P 21 25,3 32 a i r u y l o
P 14 16,9 46 e
u g it a
F 6 7,2 52
h t u o m y r
D 4 4,8 56
s m e l b o r p h tl a e h r e h t
O 59 71,1 115 * s n o s a e r r e h t
O 5 6,0 120
DI SCUSSI ON
We found a relat ively young adult populat ion, including m or e w om en ( 56% ) , r et ir ed or housew iv es ( 7 3 . 8 % ) , w it h u n f in ish ed basic edu cat ion ( 5 8 . 3 % ) ; av er ag e d isease t im e of m or e t h an t en y ear s, an d 85.7% w er e t y pe 2 diabet es m ellit us pat ient s.
A r ecent st udy( 5) of t y pe 2 diabet es m ellit us p at ien t s of lon g d u r at ion , aim ed at d escr ib in g t h e clinical, psychological and social fact or s int er fer ing in k now ledge, ident ified unsat isfact or y k now ledge about t h e d i sease, st r o n g l y i n f l u en ced b y ag e, y ear s o f educat ion, t reat m ent t im e, cognit ive funct ion, gender an d depr ession lev el.
variables able t o influence m et abolic cont rol, and t hat lifest y le and beliefs can also ex er t st r ong im pact on people’s beh av ior.
Low ed u cat ion lev els can cer t ain ly lim it ed infor m at ion access, due t o possible r eading, w r it ing, co m p r e h e n si o n o r e v e n sp e e ch p r o b l e m s( 7 ). Th i s con d it ion can r ed u ce access t o h ealt h - car e r elat ed learning opport unit ies, especially when acknowledging t hat , in general, adult pat ient s are responsible for t heir ow n daily car e.
Per sons w it h t his educat ion lev el also seem t o at t ach less value t o disease prevent ion act ions and t en d t o seek m ed ical car e w it h som e d elay, w h ich e n t a i l s a g r e a t i m p a ct o n a n d h i g h d e m a n d s f o r f i n a n ci a l r e so u r ce s d i r e ct e d a t h e a l t h ca r e( 7 ). I n addit ion , t h is delay can st im u lat e t h e w or sen in g of t h e disease.
I n t h i s sen se, d i a b et es p a t i en t ed u ca t i o n st an ds ou t as a fu n dam en t al car e aspect t o con t r ol t he disease and, t hus, prevent or delay t he appearance of acut e and chr onic com plicat ions, helping pat ient s t o prom ot e qualit y of life.
The disease’s ear ly developm ent and nat ur al h i st o r y sh o u l d b e su f f i ci e n t l y w e l l u n d e r st o o d t o i d e n t i f y d i s e a s e p r o g r e s s i o n m e a s u r e m e n t p ar am et er s. Ev en if st u d ies d em on st r at e a st r on g r elat ion b et w een t h e in cid en ce of d iab et es, f ast in g hyperglycem ia and glucose int olerance, ot her fact ors, independent ly associat ed wit h t he developm ent of t he disease, such as age, fam ily hist or y, w aist - hip rat io, body m ass in dex , ar t er ial pr essu r e an d lipid lev els, should also be t aken int o account( 2).
The gener al populat ion needs t o under st and t hese r isk fact or s, w het her separat ely or j oint ly, w it h a view t o t he inclusion of pr im ar y pr event ion act ions in daily behav ior. Dat a in Table 2 r eveal t he fragilit y of t his aspect , as only 24 ( 28.6% ) pat ient s gave correct answ er s about diabet es and it s causes.
We could also observe lack of knowledge about t he sam e quest ions in t he st udy populat ion’s relat ives( 8), w hich r epr esent s y et anot her com plicat ing fact or for diabet es m anagem ent , as r elat ives ar e consider ed t o be t he closest support for chronic disease pat ient s.
A n o t h e r r e l e v a n t a s p e c t i s p a t i e n t s ’ k n ow led g e of d esir ab le st an d ar d s of n or m alit y f or g l u c o s e , i d e n t i f i e d i n 2 4 ( 2 8 . 6 % ) p a r t i c i p a n t s . Know ledge about t hese levels can st im ulat e pat ient s’ involvem ent in self- car e, if t hey ar e aw ar e t hat t heir g lu cose lev el can v ar y w it h in a cer t ain r an g e, an d t hus help in daily glucose m onit or ing.
On t h e o n e h a n d , w e i d en t i f i ed a l a ck o f k n ow led g e, associat ed w it h d isease t im e, ag e an d educat ion. On t he ot her, t here is t he com plex process of ob t ain in g in f or m at ion an d k n ow led g e ab ou t t h e pat hogeny of diabet es, as w ell as t heir incor por at ion in car e. Th is ch ar act er izes a p r ob lem in t h e st u d y populat ion, which deserves em phasis and st rengt hens t h e n eed f or in n ov at iv e st r at eg ies t o p r om ot e t h is p o p u l a t i o n ’ s a d h e r e n ce t o t r e a t m e n t a n d o b t a i n gr eat er par t icipat ion in educat ion pr ogr am s.
D u r i n g t h e l o n g c o u r s e o f t h e d i s e a s e , d iab et es p at ien t s m ay h av e r eceiv ed som e k in d of in f or m at ion ab ou t it s p at h og en y. How ev er, f act or s int ervening in t he process of obt aining t his inform at ion m ay h av e lim it ed/ im peded it s in cor por at ion . I n t h is sen se, socioecon om ic an d cu lt u r al fact or s facilit at e/ difficult k now ledge, besides per sonal aspect s ( social/ f am ily su p p or t , p sy ch olog ical asp ect s an d d isease per cept ion) and healt h ser v ice access.
On e w ay of addr essin g r elev an t aspect s of d i a b e t e s c a r e i s t h e c o n s t i t u t i o n o f s y s t e m i z e d or ient at ion gr oups or educat ion pr ogram s. How ever, it is im port ant for t hese program s t o t ake int o account t he charact erist ics of t he t arget populat ion, which will m ake t hem look for st rat egies t hat are useful t o each g r o u p , c o n s i d e r i n g a g e , c o g n i t i v e l e v e l , s k i l l s , lim it at ions, av ailabilit y and int er est s.
I n o u r s t u d y, 2 0 ( 2 3 . 8 % ) p a r t i c i p a n t s infor m ed t hey had par t icipat ed or w er e par t icipat ing in an or ient at ion gr oup ( dat a not included) . A st udy a t t h e sa m e o u t p a t i e n t u n i t , a i m e d a t a n a l y zi n g difficult ies t hese pat ient s m ent ioned t o par t icipat e in educat ion gr oups, also found low par t icipat ion levels. Relat ed causes were: lack of int erest , inadequat e t im e and t r anspor t difficult ies, w hile m or e t han 40% w er e not aware t hat t his group exist ed( 9).
The above fact ors should be considered when t r an sm it t in g in f or m at ion t o p at ien t , w it h a v iew t o f a v o r i n g k n o w l e d g e i n co r p o r a t i o n a n d a d e q u a t e t r eat m en t f ollow - u p , w h ich sh ou ld b e p r op osed in p a r t n e r sh i p b e t w e e n t h e p a t i e n t a n d t h e h e a l t h p r of ession al, in accor d an ce w it h in d iv id u al n eed s. Ed u cat ion g r ou p p r og r am s sh ou ld b e d issem in at ed a p p r o p r i a t e l y a n d co n t i n u o u sl y, m a k i n g a v a i l a b l e m eet ing t im es, t o obt ain bet t er recept ion in t he t arget popu lat ion .
t im e, 72 ( 85.7% ) pat ient s indicat ed blood and ur ine t est s and ( 8.3% ) only blood t est s ( dat a not included) . Ot her t est s, such as cholest er ol dosage ( HDL, LDL) , t r igly cer ides and k r eat inin, ar e im por t ant par am et er s t o assess m et abolic cont rol but receive lit t le em phasis in car e for diabet es pat ient s.
An ot h er aspect t h at does n ot r eceiv e m u ch at t ent ion is blood pressure cont rol, considering art erial hypert ension as a com m on com orbidit y of diabet es( 2). A r an dom ized pr ospect iv e clin ical st u dy( 1 0 ) of abou t 7 0 0 0 r ecen t ly d iag n osed t y p e 2 d iab et es p at ien t s sh ow ed a sign ifican t r elat ion bet w een t h e in ciden ce o f m a c r o a n d m i c r o v a s c u l a r c o m p l i c a t i o n s a n d in cr eased sy st olic b lood p r essu r e. Each 1 0 m m Hg d e c r e a s e i n a v e r a g e s y s t o l i c b l o o d p r e s s u r e co r r e sp o n d e d t o a 1 2 % d e cr e a se i n r i sk f o r a n y diabet es- r elat ed com plicat ion .
D a t a r e l a t e d t o c h r o n i c m i c r o a n d m acr ovascular com plicat ions of t he populat ion in t his st udy w er e discussed in a pr ev ious ar t icle( 11).
Classical sy m pt om s t h at m ade people seek h ealt h car e in clu d ed p oly d ip sia an d p oly u r ia, t o a r educed ext ent ( Table 3) . How ever, in m ost pat ient s, diabet es w as diagn osed as a con sequ en ce of ot h er h ealt h pr oblem s.
Bet w een n in e an d 1 2 y ear passes bet w een t h e st ar t of h y per gly cem ia an d t h e t y pe 2 diabet es m e l l i t u s d i a g n o si s, d u e t o t h e f a ct t h a t g l u co se concent rat ion is not sufficient ly high for t he appearance of classical sy m pt om s( 1 2 ). Th is in cr eases t h e r isk of m icr o and m acr ov ascular com plicat ions( 2, 13- 14).
As t o t h e p r e se n ce o f a cu t e a n d ch r o n i c c o m p l i c a t i o n s o f d i a b e t e s , Ta b l e 4 s h o w s h y p er g l y cem i a , ey e p r o b l em s, f o o t p r o b l em s a n d h y p o g l y c e m i a . Th e s e s u g g e s t t h a t t h e s t u d y populat ion has received inform at ion about t he severit y of t he disease.
Dat a not included here dem onst rat ed t hat 54 ( 6 4 . 3 % ) par t icipan t s h ad alr eady been h ospit alized f o r o n e o f t h e se co m p l i ca t i o n s, w i t h a n a v e r a g e hospit alizat ion t im e of 3.1 days. Consider ing m ult iple a n s w e r s , t h e m o s t f r e q u e n t p r o b l e m s w e r e h y p e r g l y c e m i a ( 6 3 . 0 % ) , c o m a ( 1 4 . 8 % ) , h y pogly cem ia ( 1 3 . 0 % ) an d f oot pr oblem s ( 1 1 . 1 % ) . Th ese dat a can be r elat ed t o t h e du r at ion an d bad cont rol of diabet es, indicat ing a populat ion at risk for com p licat ion s.
Appr ox im at ely 33% of diabet es pat ient s ar e hospit alized dur ing t he fir st year s of t he disease due t o a cu t e co m p l i ca t i o n s, w h i ch ca n b e p r e v e n t e d
t h r ou g h ad eq u at e g lu cose con t r ol. Hy p er g ly cem ia, h y p o g l y cem i a an d d i ab et i c k et o aci d o si s r ep r esen t 24% of pr oblem s at em er gency ser v ices( 14).
I n su m m ar y, t h ese dat a r eveal t h e fr agilit y of pr event ive act ions, due t o scar ce basic know ledge a b o u t t h e d i s e a s e , c a u s e s , s i g n s / s y m p t o m s , m an ag em en t an d p r ev en t ion of acu t e an d ch r on ic com p licat ion s.
Th e co n t e n t s e x a m i n e d h e r e a r e u su a l l y in clu d ed in d iab et es ed u cat ion p r og r am s. How ev er, par t icipat ion lev els ar e low , possibly du e t o access difficult ies, av ailabilit y and per sonal m ot iv at ion.
Som e r easons for low par t icipat ion in t hese groups can be at t ribut ed t o t he fact t hat t hese pat ient s on ly seek m ed ical car e in acu t e sit u at ion s. On t h e o t h e r h a n d , t h e n u m b e r o f h e a l t h p r o f e ssi o n a l s av ailab le f or ex clu siv e d ed icat ion t o ed u cat ion an d prevent ion act ivit ies is st ill insufficient . Anot her fact or i s p r o f essi o n al t r ai n i n g , w h i ch p r i o r i t i zes cu r at i v e act ions t o t he det r im ent of pr ev ent ion.
Pr ofession als act iv e in edu cat ion / pr ev en t ion should be fam iliar wit h educat ion st rat egies t hat allow t h e m t o a d a p t t o t h e n e e d s a n d l i m i t a t i o n s o f par t icipat in g adu lt s, u n der st an din g t h at , in gen er al, t h is gr ou p possesses low edu cat ion lev els an d m ay n ot b e in t er est ed in t h is t y p e of car e. I n f or m at ion con t en t s n eed t o b e t r an sm it t ed in a sim p le w ay, however, guarant eeing im pact in t he t arget populat ion, m ot iv at in g p eop le t o lear n ab ou t t h e d isease an d act i v el y assu m e t h ei r r ol e i n t r eat m en t an d car e, i n t e g r a t i n g t h e i r p e r so n a l st r u ct u r e , b e l i e f s a n d psy ch osocial st at e.
Som e st r at egies f or t h is t y pe of popu lat ion in clu de t h eor ies r elat ed t o t h e h ealt h belief m odel, se l f - e f f i ca cy, co n t r o l l o cu s, co g n i t i v e d i sso n a n ce , diffusion, lear ning st ages and finally, adult t heor y( 7).
Ea c h o f t h e s e t h e o r i e s r e q u i r e s b r o a d k n o w l e d g e a n d p r a ct i ce , i n l i n e w i t h t h e h e a l t h p r o f e s s i o n a l ’ s a n d t h e t a r g e t p o p u l a t i o n ’ s u n d e r st a n d i n g . Th e se st r a t e g i e s f o r i n t e r r e l a t i o n bet ween part icipant s and professionals can be of help i n p a r t i ci p a n t s’ l e a r n i n g . Th i s ca n l e a d t o b e t t e r t r e a t m e n t f o l l o w - u p , h i g h l i g h t i n g p a t i e n t s a s pr ot agonist s in car e for t heir disease.
t o be pr ogr am m ed accor ding t o t he ident ified needs an d each sit u at ion con t ex t , in clu din g r isk lev els for com p licat ion s.
Knowledge about diabet es and it s im port ance in t he self- car e pr ocess allow s us t o v alue t he need t o cr eat e aw ar en ess i n t h e p o p u l at i o n ab o u t r i sk fact or s for t h e dev elopm en t of diabet es, as w ell as chr onic com plicat ions am ong pat ient s. These aspect s should be included in educat ion program s and diabet es m ellit us t r ack ing cam paigns, w it h a v iew t o ar ousing m ot iv at ion and int er est .
CONCLUSI ONS
This st udy indicat ed aspect s t hat difficult t he learning process, such as age ( m ean 53.3± 13 years) , disease t im e ( m ean 12.9± 9 years) and low educat ion lev el ( 5 8 % h ad u n f in ish ed b asic ed u cat ion ) . Th ese condit ions can lim it t he incor por at ion of infor m at ion i n t h i s p o p u l a t i o n a n d , co n se q u e n t l y, j e o p a r d i z e pr ev ent ion and ear ly diagnosis, besides pr edisposing t o com plicat ions.
We also revealed ot her aspect s int erfering in t he lear ning pr ocess, such as biopsy chosocial fact or s and healt h ser v ice access.
Wit h r esp ect t o k n ow led g e ab ou t “ w h at is diabet es?” and “ w hat are it s causes?”, w e found t hat on ly 2 4 ( 2 8 . 6 % ) par t icipan t s gav e cor r ect an sw er s, while 24 ( 28.6% ) pat ient s gave wrong answers or did not know t he answ er.
Con sid er in g m u lt ip le an sw er s, 7 1 % of t h e st u dy popu lat ion w as diagn osed w it h ou t pr esen t in g classical diabet es sy m pt om s, an d 6 4 % h ad alr eady b e e n h o s p i t a l i z e d d u e t o a c u t e o r c h r o n i c com plicat ions, such as hyper glycem ia ( 63.0% ) , com a ( 1 4 , 8 % ) , h y pogly cem ia ( 1 3 . 0 % ) an d f oot pr oblem s ( 1 1 . 0 % ) .
These result s shows t he fragilit y of knowledge about diabet es, causes and com plicat ions for disease m anagem ent , which can be relat ed t o fact ors int rinsic t o pat ien t s an d t o t h e h ealt h sy st em , com plicat in g access t o basic inform at ion. This reveals t he need for healt h pr ofessionals t o r edir ect st r at egies for car e t o diabet es pat ient s, in v iew of biopsy chosocial fact or s and exist ing r esour ces at t he healt h unit .
ACKNOW LEDGEMENTS
This art icle result s from t he I nt egrat ed CNPq p r o j e c t - N a t i o n a l Co u n c i l f o r S c i e n t i f i c a n d Technological Developm ent , 520309/ 98- 7, called “ The nur se in t he pr ev ent ion and ear ly det ect ion of low er l i m b co m p l i ca t i o n s i n d i a b et es m el l i t u s p a t i en t s”, car r ied out bet w een Mar ch 1999 and Febr uar y 2001. Thanks t o Prof. Moacyr Lobo da Cost a Junior, for his advice in t he st ruct uring of t he dat a collect ion inst rum ent . To nurse Andréa Mat hes Faust ino, for her collabor at ion in dat a collect ion as an under gr aduat e st u d en t , an d t o D r. Mi y ek o Hay ash i d a, l ab o r at o r y specialist nurse at EERP- USP, for her st at ist ical support .
REFERENCES
1. Or ganização Mundial da Saúde. Cuidados inovador es par a
c o n d i ç õ e s c r ô n i c a s : c o m p o n e n t e s e s t r u t u r a i s d e a ç ã o .
Relat ór io Mu n dial. Br asília: OMS; 2 0 0 3 .
2. Am er ican Diabet es Associat ion. I m plicat ions of t he Unit ed
Kin gdom Pr ospect iv e Diabet es St u dy. Diabet es Car e 2 0 0 4 ;
2 7 ( Su p p l 1 ) : 2 8 - 3 2 .
3. Arm st rong N. Coping w it h diabet es m ellit us: a full t im e j ob.
Nu r s Clin Nor t h Am 1 9 8 7 ; 2 2 ( 3 ) : 5 5 9 - 6 8 .
4 . Gar cia R, Su ar ez R. La edu cación en diabet es: algu n as
r ef lex ion es p ar a la p r áct ica. Rev Asoc Am Diab et es 1 9 9 9 ;
7 ( 3 ) : 1 7 0 - 7 .
5. Mur at a GH, Shah JH, Adam KD, Wendel CS, Bok har i SU,
Solvas PA et al. Fact ors affect ing diabet es knowledge in t ype
2 d iab et ic v et er an s. Diab et olog ia 2 0 0 3 ; 4 6 : 1 1 7 6 - 8 .
6. Coat es VE. Educat ional issues relat ing t o people w it h
long-t er m heallong-t h pr oblem s. I n. Coalong-t es VE Educalong-t ion for palong-t ienlong-t s
an d clien t s. Lon don : Ru t ledge; 1 9 9 9 . p. 1 3 5 - 6 0 .
7 . Doak CC, Doak LG, Root JH. The lit er at ur e pr oblem . I n.
Doak CC, Doak LG, Root JH Teaching pat ient s w it h low lit eracy
sk ills. 2n d ed. Ph iladelph ia: JB Lippincot t ; 1 9 9 5 . p. 1 - 9 . 8 . Pace AE, Nu nes PD, Och oa- Vigo K. O conhecim en t o dos
f am iliar es acer ca da pr oblem át ica do por t ador de diabet es
m e l l i t u s. Re v La t i n o - Am En f e r m a g e m 2 0 0 3 m a i o - j u n h o ;
1 1 ( 3 ) : 3 1 2 - 9 .
9 . Cazar in i RP, Zan et t i ML, Rib eir o KP, Pace AE, Foss MC.
Ad esão a u m g r u p o ed u cat i v o d e p esso as p o r t ad o r as d e
d iab et es m ellit u s: p or cen t ag em e cau sas. Med icin a 2 0 0 2 ;
3 5 : 1 4 2 - 5 0 .
1 0 . Ad ler AI , St r at t on I M, Neil HAW, Yu d k in JS, Mat t h ew s
DR, Cu ll CA, et al. Associat ion of sy st olic b lood p r essu r e
w it h m acr ov ascular and m icr ov ascular com plicat ions of t y pe
2 d iab et es ( UKPDS 3 6 ) : p r osp ect iv e ob ser v at ion al st u d y.
BMJ 2 0 0 0 ; 3 2 1 : 4 1 2 - 9 .
11. Pace AE, Foss MC, Ochoa- Vigo K, Hay ashida M. Fat or es
de r isco par a com plicações em ex t r em idades in f er ior es de
pessoas com diabet es m ellit us. Rev Br as Enfer m agem 2002;
12. Har r is MI , Klein R, Welbor n TA, Knuim an MW. Onset of
NI D D M o ccu r s a t l e a st 4 - 7 Yr. b e f o r cl i n i ca l d i a g n o si s.
Diab et es Car e 1 9 9 2 ; 1 5 ( 7 ) : 8 1 5 - 9 .
13. Nazim ek- Siew niak B, Moczulski D, Gr zeszczak W. Risk of
m acr ov ascu lar an d m icr ov ascu lar com p licat ion s in t y p e 2
d i ab et es r esu l t s o f l o n g i t u d i n al st u d y d esi g n . J D i ab et es
Com p licat ion s 2 0 0 0 ; 1 6 : 2 7 1 - 6 .
1 4 . Cl e m e n t S . D i a b e t e s s e l f - m a n a g e m e n t e d u c a t i o n .
Di ab et es Car e 1 9 9 5 ; 1 8 ( 8 ) : 1 2 0 4 - 1 4 .