Depart ment of Neurology, Psychiat ry and M edical Psychology, Ribeirão Pret o School of M edicine, Universit y of São Paulo, Ribeirão Pret o SP, Brazil: 1Head of t he M ovement Disorders Sect ion, 2Resident in Neurology, 3Associat e Prof essor.
Received 25 M arch 2004. Accept ed 17 July 2004.
Dr. Vit or Tumas - Depart ment of Neurology, Psychiat ry and M edical Psychology - Ribeirão Pret o School of M edicine, Universit y of São Paulo - 14049-900 Ribeirão Pret o SP - Brasil. E-mail: t [email protected] mrp.usp.br
INTERNAL CONSISTENCY OF A BRAZILIAN
VERSION OF THE UNIFIED HUNTINGTON’S
DISEASE RATING SCALE
Vit or Tumas
1, Sarah Teixeira Camargos
2, Paulo Samandar Jalali
2,
Adriano de Paula Galesso
2, Wilson M arques Jr
3ABSTRACT - We evaluated the reliability of a translated Brazilian version of the Unified Huntington’s Disease Rat ing Scale (UHDRS) t o est ablish t he reproducibilit y of t he scale in a populat ion t hat diff ers subst ant ial-ly f rom t hat on w hich t he scale w as originalial-ly validat ed. Af t er a t raining period w it h t he video and guide-lines request ed f rom t he Hunt ingt on St udy Group, w e applied t he UHDRS, except f or t he cognit ive t est s, t o a group of 21 Brazilian pat ient s w it h a molecular diagnosis of Hunt ingt on’s disease (HD). We f ound a high degree of int ernal consist ency of t he mot or sect ion of t he UHDRS (Cronbach’s alpha= 0.841). There w as a negat ive correlat ion bet w een t he t ot al mot or score and t he f unct ional assessment , t he independ-ence scale and t he f unct ional capacit y. There w as a posit ive correlat ion bet w een t hese 3 scales of f unc-t ional evaluaunc-t ion and a negaunc-t ive correlaunc-t ion beunc-t w een unc-t he age of onseunc-t of unc-t he disease and unc-t he number of CAG repeat s. The behavioral scale and disease durat ion w ere not correlat ed w it h any f act or. The clinical charact erist ics of t his sample of pat ient s as described by t he UHDRS w ere roughly similar t o t hose report -ed in t he original validat ion st udies and t he correlat ions describ-ed w ere similar t o t hose report -ed previ-ously. We conclude t hat t he Brazilian version of t he UHDRS is reliable and valid t o st udy pat ient s w it h HD in t he Brazilian set t ing, t hat t his sample of Brazilian pat ient s had clinical charact erist ics similar t o t hose observed in ot her w orld regions, as expect ed, and t hat t he clinical t raining met hod used f or t he applica-t ion of applica-t he UHDRS w as eff ecapplica-t ive applica-t o insure a high degree of clinical reproducibiliapplica-t y.
KEY WORDS: Hunt ingt on’s disease, Unif ied Hunt ingt on’s disease rat ing scale, Brazilian version, reliabilit y.
Consistência interna da versão brasileira da escala unificada para avaliação da doença da Huntington
RESUM O - Nosso est udo avaliou a conf iabilidade da versão brasileira da escala unif icada para avaliação da doença de Hunt ingt on (UHDRS) com o objet ivo de est abelecer a reprodut ibilidade dessa escala em uma população que dif ere signif icat ivament e daquela em que f oi originalment e validada. Após um período de t reinament o com um vídeo divulgado para esse objet ivo e um manual solicit ado aos idealizadores da escala, nós aplicamos a UHDRS, com exceção dos t est es cognit ivos, em um grupo de 21 pacient es brasileiros com diagnóst ico molecular de doença de Hunt ingt on (DH). Nessa amost ra nós encont ramos uma elevada con-sist ência int erna na seção que avalia os sint omas mot ores (alf a de Cronbach= 0,841). Observamos uma cor-relação negat iva ent re o escore t ot al da escala mot ora e as escalas de avaliação f uncional, de independên-cia e de capacidade f uncional t ot al; uma correlação posit iva ent re essas 3 últ imas escalas; e uma correlação negat iva ent re a idade de início dos sint omas e o número de repet ições CAG. As caract eríst icas clínicas dessa amost ra de pacient es descrit as segundo a UHDRS é de maneira comparat iva similar às descrit as nos est u-dos originais de validação da escala, assim como as correlações descrit as são semelhant es às descrit as pre-viament e. Concluimos que a versão brasileira da UHDRS é conf iável e válida para est udar pacient es com DH aqui no Brasil, que essa amost ra, como era esperado, t em caract eríst icas semelhant es às descrit as em out ras regiões do mundo, e que o mét odo ut ilizado para t reinament o da aplicação da escala é válido.
PALAVRAS-CHAVE: doença de Hunt ingt on, escala unif icada, versão brasileira, conf iabilidade.
Hunt ingt on’s disease (HD) is a heredit ary neuro-degenerat ive disease w it h w orldw ide dist ribut ion result ing f rom a CAG repeat expansion in t he IT15 gene locat ed on 4p16.31. The progressively
com-plex clinical pict ure includes mot or manif est at ions, psychiat ric sympt oms and cognit ive abnormali-t ies2. Abnormal movement s are one of t he most
post ural dist urbances, oculomot or abnormalit ies, changes in muscular t onus and bradykinesia. It seems t hat t he disease originat ed and w as more f requent in Caucasians, and w as probably dissem-inat ed t hroughout t he w orld by European migra-t ions in migra-t he 17migra-t h and 18migra-t h cenmigra-t uries2. Accordingly,
t he same CAG repeat expansion is ident if ied in pa-t ienpa-t s all over pa-t he w orld3. New mut at ions are rare,
but t hey can occur due t o t he inst abilit y in t he pa-t ernal pa-t ransmission of an inpa-t ermediapa-t e allele w ipa-t h 27-35 CAG repeats4. It is well accepted that the
phe-not ypical aspect s of t he disease are very similar in dif f erent populat ions. The molecular aspect s of Brazilian HD pat ient s have been recent ly report -ed and w ere f ound t o be similar t o t he f indings obt ained f or ot her et hnic groups5,6. Consequent ly
w e expect t he phenot ypical present at ion of t hese pat ient s t o be similar t o t he classical descript ions.
The Unif ied Hunt ingt on’s Disease Rat ing Scale (UHDRS)7 is a clinical rat ing scale developed t o
standardize the clinical examination of HD patients, scoring in det ail t he f our main domains of impair-ment : mot or perf ormance, behavior abnormalit ies, cognit ive perf ormance and f unct ional capacit y. It s reliability and consistency have been clearly
demon-st rat ed in Nort h-American pat ient s7, but so f ar no
study has been reported to validate the scale in oth-er et hnic groups. Af t oth-er t ranslat ing t he UHDRS int o Port uguese w e applied it t o a group of Brazilian pat ient s f ollow ed at our universit y hospit al t o de-t ermine de-t he reliabilide-t y of de-t he de-t ranslade-t ed scale and t o est ablish it s reproducibilit y in a populat ion t hat dif f ers subst ant ially f rom t hat w here it w as origi-nally st udied in t erms of linguist ic and cult ural aspect s. We also int ended t o det ermine if t he phe-not ypical charact erist ics of t his sample of Brazilian HD pat ient s are similar t o t he classical descript ions t hroughout t he w orld, and if t his small sample is a represent at ive cross-sect ional view of t he disease.
M ETHOD
We have included in t his st udy all pat ient s w it h a mo-lecular diagnosis of Hunt ingt on’s disease f ollow ed at t he Movement Disorder outpatient clinic of our university hos-pit al, St at e of São Paulo, Brazil. All pat ient s and parent s gave informed consent for blood and clinical analysis, and t he prot ocol w as approved by t he local et hics commit t ee. For molecular diagnosis, DNA w as ext ract ed f rom pe-ripheral leucocyt es according t o st andard prot ocols. The pert inent region of chromosome 4p w as expanded by PCR with primers HD3F and HDE, as previously described8.
Table 1. Charact erist ics of 21 Brazilian pat ient s w it h Hunt ingt on’s disease accord-ing t o t he UHDRS.
M ean SD Range
Age at examinat ion 46.57 13.00 25-70
Age at HD onset 38.71 13.22 16-61
M ale/f emale 8/13
In use of neurolept ics 16/21
Durat ion of HD (years) 7.85 4.50 2-20
Abnormal CAG repeat s 46.95 5.21 41-58
Tot al mot or score (0-124) 46.55 23.90 17-89 Tot al behavior score (0-224) 22.66 25.58 0-75
Behavioral milest ones
Conf used (% ) 38%
Dement ed (% ) 33%
Depressed (% ) 42%
Requiring an ant idepressive (% ) 33%
Funct ional checklist score (0-25) 10.71 7.47 0-22
PCR product s w ere elect rophoresed in an aut omat ed 377 Sequencer and analyzed w it h t he Genescan sof t w are. Individuals w it h more t han 36 CAG repeat s w ere consi-dered t o have a posit ive molecular diagnosis of Hun-t ingHun-t on’s Disease4.
The UHDRS guidelines and t he videot ape of t he mo-tor examination were obtained from the Huntington Stu-dy Group7. Af t er being adapt ed and t ranslat ed t o
Bra-zilian pat ient s by one of t he aut hors (VT) t hey w ere used in t raining sessions w it h all f our clinical invest igat ors (VT, STC, APG, PSJ) unt il a consensus about t he examina-t ion examina-t echnique and examina-t he grades of each moexamina-t or abnormal-it y w as reached. At t he end of t he t raining period a resonably unif orm agreement about score rat e w as obt a-ined f rom t he 4 invest igat ors. The int errat er reliabilit y of the translated version will be accessed in another study. Af t er t his period of t raining all pat ient s w ere evaluat ed by t he same invest igat or (STC), w ho used t he adapt -ed version of t he UHDRS t o score t he mot or, behavioral and f unct ional assessment s, t he independence scale and t he f unct ional capacit y score. The cognit ive assessment w ere not applied in t his st udy due t o t he w ide variat ions in t he cult ural and educat ional background of t he pa-t ienpa-t s, and pa-t o pa-t he absence of validapa-t ion spa-t udies f or pa-t he cognit ive t est s in our normal populat ion. The Luria t est w as also excluded f rom t he analysis because it w as not rat ed in many pat ient s f or dif f erent reasons.
In t he UHDRS, t he mot or perf ormance is described by t he t ot al mot or score w hich is calculat ed by adding t he scores f or each of t he 15 it ems of mot or f unct ion (grading 0=normal t o 4=severely impaired). M any of t hese it ems are scored in more t han one condit ion or body region t o make up a t ot al of 33 scores t o be added t o achieve t he w orst perf ormance of 132. The exclusion of t he Luria t est result ed in a maximum possible mot or score of 128. The remaining 14 it ems of t he mot or
exam-inat ion w ere grouped int o 9 dimensions f or st at ist ical analysis as f ollow s: 1) abnormalit ies of ocular mot or cont rol (ocular pursuit , saccade init iat ion, saccade veloc-it y) 2) dysart hria, 3) mot or impersist ence (t ongue prot ru-sion), 4) bradykinesia (f inger t aps, pronat e-supinat e hands, body bradykinesia), 5) rigidit y, 6) dyst onia, 7) chorea, 8) abnormalit ies of gait (gait , t andem gait ), and 9) post ural inst abilit y. The dimensions w ere est ablished by t heir clinical cont ent s and not by previous scale princi-pal component analysis.
The behavioral assessment of t he UHDRS is calculat -ed by adding dif f erent it ems, and each one is def in-ed by t he product of t he severit y (0=absent t o 4=severe) and t he f requency (0=almost never, 4 almost alw ays) of t he psychiat ric sympt om. In anot her session, t hree it ems w ere used t o assess if t he pat ient has reached cert ain behavioral milest ones (depression, dement ia, conf u-sion) according to the examiner. The cognitive performan-ce t hat w as not invest igat ed in our st udy w as described in t he scale by verbal f luency, symbol digit and St roop t est s. The score on t he f unct ional assessment scale w as t he sum of 25 daily t asks t hat t he pat ient could st ill per-f orm. The independence scale ranged per-f rom 100 (no spe-cial care needed) t o 10 (t ube f eeding, t ot al bed care). The f unct ional capacit y w as t he sum of 5 it ems w it h a t ot al score of 0 (unable) t o 13 (normal). Thus, t he functio-nal scales score higher f or bet t er pat ient condit ion, t his being t he inverse of t he ot her subscales.
The number of abnormal CAG repeat s, age at disea-se ondisea-set and durat ion of didisea-seadisea-se w ere recorded. We ana-lyzed t he int ernal consist ency of t he mot or scale dat a using Cronbach’s alpha and calculat ed an it em-t ot al and it em-it em correlat ion.
We also studied the correlations between total motor score, behavioral score, f unct ional assessment , indepen-dence scale, f unct ional capacit y score, number of
abnor-Table 2. Analysis of t he reliabilit y of t he mot or scale of t he UHDRS: correlat ion mat rix of it em-t ot al and it em-it em correlat ion.
TOTAL OM C DYSART TONGUE BRADY RIGID DYST CHOR GAIT RETR
TOTAL 1.00
OM C 0.776 1.00
DYSART 0.890 0.704 1.00
TONGUE 0.870 0.792 0.853 1.00
BRADY 0.910 0.818 0.877 0.842 1.00
RIGID 0.527 0.420 0.505 0.641 0.566 1.00
DYST 0.645 0.721 0.814 0.738 0.769 0.545 1.00
CHOR 0.435 0.379 0.501 0.427 0.499 0.139 0.115 1.00
GAIT 0.906 0.710 0.824 0.845 0.885 0.577 0.642 0.592 1.00
RETR 0.823 0.605 0.685 0.722 0.775 0.544 0.475 0.633 0.890 1.00
mal CAG repeat s, age at disease onset , and disease dura-t ion using dura-t he Pearson’s correladura-t ion madura-t rix.
The working hypothesis was that the clinical characte-rist ics w ould be similar t o t hose of t he pat ient s described in t he original UHDRS st udy and t hat t he t ranslat ed version w ould be reliable, validat ing t he Brazilian ver-sion of t he UHDRS.
RESULTS
We examined 21 pat ient s f rom 20 f amilies w it h a molecular diagnosis of HD w ho w ere f ollow ed at our Hospit al. At t he t ime of evaluat ion, most of t hem w ere t aking neurolept ics. Table 1 show s t he demographic dat a and t he clinical charact erist ics of t his group of pat ient s according t o t he UHDRS, except f or t he cognit ive sect ion and t he Luria t est . An it em-t ot al correlat ion w as calculat ed bet w een t he scores f or each of t he 9 dimensions of t he mo-t or examinamo-t ion and mo-t he mo-t omo-t al momo-t or score, and w e also calculat ed an it em-it em correlat ion (Table 2). We f ound t hat chorea (0.435), rigidit y (0.527) and dyst onia (0.645) w ere t he clinical dimensions less correlat ed w it h t he t ot al mot or score and also w it h t he ot her it ems. The dimensions w hich w ere less correlat ed w ere rigidit y and chorea (0.139) and chorea and dyst onia (0.115). The most correla-t ed clinical dimensions w ere poscorrela-t ural inscorrela-t abilicorrela-t y and gait (0.890), bradykinesia and gait (0.885) and bradykinesia and dysart hria (0.877)
The Cronbach’s alpha value of t he mot or sec-tion of the UHDRS was 0.841, which indicates a high degree of int ernal consist ency. The variat ion in alpha value, if each it em w as delet ed f rom t he mo-t or scale, show ed mo-t hamo-t mo-t he exclusion of mo-t he chorea dimension f rom t he mot or scale w as t he only one t hat result ed in an increase of Cronbach’s alpha (0.893), w hile t he exclusion of t he bradykinesia di-mension result ed in t he great est reduct ion in t he scale alpha value (0.786).
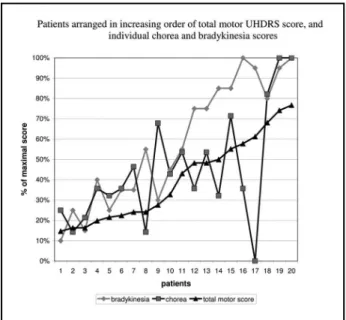
To show t hat t he t ot al mot or score represent s a linear curve of t he t heoret ical const ruct of t he mot or examinat ion, as w as expect ed by it s high in-t ernal consisin-t ency, w e graphically ploin-t in-t ed in-t he in-t oin-t al mot or scores of t he 21 pat ient s in increasing order. The scores w ere t ransf ormed t o t he percent age of t he t ot al mot or score (Fig 1). Furt hermore, in t he same graphic and using t he same met hodology w e present ed t he 2 sub-it ems of mot or examinat ion of each pat ient , chorea and bradykinesia (Fig 1). As can be seen, t he t ot al mot or score present ed an almost linear ascending curve and t he 2 dimen-sions of t he mot or examinat ion f ollow ed a more irregular course. The chorea curve f ollow ed a more irregular ascending course t han t he bradykinesia curve as it w as t he least correlat ed it em t o t he t ot al mot or score.
The Pearson correlation matrix showed a negati-ve correlat ion bet w een t ot al mot or score and f unc-t ional assessmenunc-t (-0.709, p&lunc-t;0.001), independence scale 0.745, p<0.001) and f unct ional capacit y (-0.686, p<0.001), a posit ive correlat ion bet w een t he 3 scales of f unct ional evaluat ion (p<0.001), and a negat ive correlat ion bet w een t he age at onset of t he disease and t he number of CAG repeat s (-0.695, p<0.0001). The behavioral subscale and disease du-rat ion w ere not correlat ed w it h any f act or.
DISCUSSION
The UHDRS is a reliable clinical rat ing scale de-veloped t o assess mot or perf ormance, cognit ive f unct ioning, behavioral abnormalit ies and f unct io-nal capacity of HD patients7,9. It may be used as a tool
f or evaluat ing t he progression of t he disease and so f or det ermining t he nat ural hist ory of t he disease and t he eff ect s of t herapeut ic int ervent ions10.
We have adapt ed t he UHDRS t o Brazilian pat i-ents taking care to preserve its original purpose and obt ained many indicat ions of it s reliabilit y in t his study. It is supposed that cultural and linguistic char-act erist ics of dif f erent populat ions may alt er t he result s obt ained w it h a clinical scale developed
f or a specif ic et hnic group, so t hat t he validat ion and reliabilit y of a clinical rat ing scale may not be t he same across diff erent populat ions11.
Accordin-gly, it is alw ays import ant t o validat e t he scale in populat ions t hat diff er subst ant ially f rom t he orig-inal one in t erms of linguist ic and cult ural aspect s11.
In t he present st udy w e f ound in t his st udy a high int ernal consist ency in t he mot or scale of t he UHDRS w hen t he adapt ed version w as applied t o a Brazilian sample of 21 HD pat ient s (Cronbach’s alpha= 0.893). This result is very similar t o t hat d escr i b ed i n t h e o r i g i n al val i d at i o n st u d y11.
Cronbach’s alpha may be int erpret ed as t he aver-age correlat ion bet w een t w o halves of a t est w hen the test is split into all possible combinations of two half t est s11. A high alpha indicat es t hat t here is at
least one homogeneous dimension underlying t he summed score and t hat at least some of t he it ems correlat e subst ant ially w it h one anot her11. In
clin-ical set t ings, an alpha bet w een 0.80 and 0.90 ought t o be t he goal11.
There are several ot her met hods available t o evaluat e t he int ernal consist ency or reliabilit y of a linear composit e scale as t he UHDRS. In it em-t ot al correlat ion, each it em is correlat ed w it h t he sum of t he remaining it ems. In our st udy almost all items of motor examination showed high item-total correlat ions except f or chorea, rigidit y and dyst o-nia in increasing order of correlat ion w it h t he t ot al mot or score. Also, chorea show ed very low correlat ions w it h most of t he ot her examinat ion it ems and if excluded f rom t he scale result ed in an increase in it s int ernal consist ency. This seems par-adoxical in t he case of HD w here chorea is one of t he main mot or sympt oms and should be an obli-gat e part icipant in t he t heoret ical const ruct of a clinical rat ing scale f or t he disease. The possible ex-planat ion f or t his f inding w as t hat almost all of our pat ient s w ere examined w hile t aking neurolept ics t o cont rol abnormal movement s. This could be an indicat or t hat in our medical set t ing t here is a t en-dency t o prescribe f reely t hese medicat ions even t o pat ient s w it h mild chorea. The low correlat ion bet w een chorea and rigidit y may be relat ed t o t he f act t hat t he UHDRS does not measure t onus properly, it w ould be also necessary t o include measures of hypot onia in t he mot or scale. Figure 1 w hich represent s each pat ient ordered accord-ing t o t ot al mot or score is a usef ul illust rat ion t hat t he sample spans t he spect rum of t he illness and t hat t his st raight ascending line w ould be expect -ed if t he scale measur-ed a linear const ruct .
Cons-t rucCons-t s are absCons-t racCons-t concepCons-t s abouCons-t Cons-t he disease Cons-t haCons-t are mat erialized in a number of observable indi-cat ors of t he abst ract ion11. An ordinal composit e
scale such as t he UHDRS may f ollow t he model of a linear composit e scale, w here, w hen t he it ems are summed, t he t race line plot t ing t ot al scores against t he const ruct being measured w ill approx-imat e a st raight line. This is expect ed in a linear model of a const ruct t hat measures t he mot or sympt oms of a disease. The individual it ems t end t o have a slight ly dif f erent curve w hen plot t ed against t he const ruct . We can see in Figure 1 t hat t he pat ient ’s t ot al mot or score ranged f rom 10% t o 80% of t he t ot al possible score, and t heref ore w e may speculat e t hat our small sample corre-sponds t o a valid cross-sect ional clinical represent a-t ion of HD paa-t iena-t s.
We det ect ed a very low correlat ion bet w een chorea and dystonia in our patients, supporting oth-er obsoth-ervat ions t hat indicat e t hat t hese mot or ab-normalit ies may evolve separat ely12. The most
cor-relat ed clinical dimensions in our st udy w ere pos-t ural inspos-t abilipos-t y and gaipos-t (0.890), bradykinesia and gait (0.885) and bradykinesia and dysarthria (0.877). This may indicat e t hat t hese clinical aspect s meas-ure a homogeneous clinical f act or w it h relat ed pat ophysiological mechanisms.
The high correlat ion bet w een t he t ot al mot or score and t he f unct ional scales t hat w ere also high-ly int errelat ed, and t he absence of a correlat ion bet w een t he behavioral assessment and t he ot h-er subscales are f indings similar t o t hose report ed by ot hers7. This indicat es t hat t he behavioral
symp-t oms f ollow a separasymp-t e and independensymp-t pasymp-t ophy-siological mechanism or t hat t he neurolept ical t herapy w ould be int erf ering w it h t he clinical pres-ent at ion of t hese sympt oms, since most of t he pa-t ienpa-t s w ere in use of pa-t hese drugs. Also, pa-t he nega-t ive correlanega-t ion benega-t w een nega-t he age anega-t onsenega-t of nega-t he disease and t he number of CAG repeat s observed in our st udy is similar t o t hat det ect ed in many ot h-er st udies. These f indings corroborat e t he reprodu-cibility of the scale and of the HD clinical manifesta-t ions in our medical semanifesta-t manifesta-t ing.
w e should have expect ed a low int ernal consist en-cy. Int ernal consist ency is a f orm of reliabilit y, i. e. t he proport ion of variat ion in scores due t o t rue variat ion and not t o error, and it s measure is sensi-t ive sensi-t o unreliabilisensi-t y asensi-t sensi-t ribusensi-t able sensi-t o consensi-t ensensi-t sam-pling as error variance11.
Finally, if w e compare t he clinical and UHDRS charact erist ics of our sample of Brazilian HD pa-t ienpa-t s pa-t o pa-t hose of pa-t he opa-t her validapa-t ion spa-t udies w ipa-t h a large number of Nort h-American and Dut ch pa-t ienpa-t s7,9, w e can see t hat our populat ion is closely
similar. The most obvious dif f erence compared t o t he f irst st udy7is t hat conf usion is more f requent
(38% ) in our populat ion (17% ). Because w e are comparing only t he global score of t he mot or exa-minat ion w e cannot exclude t hat some diff erences in the phenotypical presentation of the disease may exist . But t hese possible dif f erences could also be an eff ect of t he small size of our sample. Excluding t he Luria t est of t his analysis seems t o have had a small ef f ect on t he t ot al mot or score. It is a com-ponent of t he mot or scale and it scores 4 at w orst performance, and this could not change significant-ly t he t ot al mot or score of t he sample.
We may conclude t hat t he Brazilian version of t he UHDRS is reliable and valid f or t he st udy of pa-t ienpa-t s w ipa-t h HD in pa-t he Brazilian sepa-t pa-t ing and pa-t hapa-t pa-t he clinical t raining met hod used f or t he applicat ion of t he UHDRS w as eff ect ive t o insure a high degree of
clinical reproducibilit y. We also conclude t hat , as expect ed, t he phenot ypical present at ion of HD in our count ry is similar t o t hat in ot her w orld regions.
REFERENCES
1. Huntington’s Disease Collaborative Research Group. A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington’s disease chromosomes. Cell 1993;72:971-983.
2. Bruyn GW, Went LN. Huntington’s chorea. In: Vinken PJ, Bruyn GW, Klawans HL (eds). Handbook of clinical neurology vol 49, Extrapyramidal Disorders. Amsterdam: Elsevier Science Publishers, 1986:267-313.
3. Kremer B, Goldberg P, Andrew SE, et al. A worldwide study of the Huntington’s disease mutation: the sensitivity and specificity of meas-uring CAG repeats. N Eng J Med 1994;330:1401-1406.
4. American College of Medical Genetics, American Society of Human Genetics, Huntington Disease Genetic Testing Working Group. Laboratory guidelines for Huntington disease testing. Am J Hum Genet 1998;62:1243-1247.
5. Silva TCL, Serra HG, Bertuzzo CS, Lopes-Cendes IL. Molecular diag-nosis of Huntington disease in Brazilian patients. Arq Neuropsiquiatr 2000;58:11-17.
6. Raskin S, Allan N, Teive HG, et al. Huntington disease: DNA analysis in Brazilian population. Arq Neuropsiquiatr 2000;58:977-985. 7. Huntigton Study Group. Unified Huntington’s disease rating scale:
reli-ability and consistency. Mov Disord 1996;11:136-142.
8. Davis MB, Bateman DM, Quinn NP, Marsden CD, Harding AE. Mutation analysis in patients with possible but apparently sporadic Huntington’s disease. Lancet 1994;344:714-717.
9. Siesling S, Zwinderman KAH, Van Vugt JPP, Kieburtz K, Roos RAC. A shortened version of the motor section of the unified Huntington’s disease rating scale. Mov Disord 1997;12:229-234.
10. Siesling S, Van Vugt JPP, Zwinderman KAH, Kieburtz K, Roos RAC. Unified Huntington’s disease rating scale: a follow up. Mov Disord 1998;13:915-919.
11. Larocca NG. Statistical and methodological considerations in scale construction. In: Munsat TL (ed). Quantification of neurologic deficit. Boston: Butterworths, 1989:49-67.