w w w . r b o . o r g . b r
Case
Report
Knee
osteoarthrosis
secondary
to
ochronosis
–
clinical
case
夽
,
夽夽
Andreia
Maria
da
Silva
Martins
Ferreira
a,∗,
Filipe
Lima
Santos
a,
André
Miguel
Castro
Costa
a,
Bruno
Miguel
Pereira
Barbosa
b,
Rui
Miguel
Reis
Rocha
a,
Joaquim
Fernando
Fontes
Lebre
aaVilaNovadeGaiaHospitalCenter/EspinhoHospital,VilaNovadeGaiaandEspinho,Portugal
bTrás-os-MontesandAltoDouroHospitalCenter,VilaReal,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received5October2013 Accepted11November2013 Availableonline27October2014
Keywords:
Alkaptonuria Ochronosis Knee Arthroplasty
a
b
s
t
r
a
c
t
Alkaptonuriaisararemetabolicdiseaseinwhichadeficiencyoftheenzymehomogentisate dioxygenasecausesanaccumulationofhomogentisicacid.Ochronosisconsistsof exces-sivedepositionofhomogentisicacidintheconnectivetissueandpresentsasachestnut brownorblackpigmentation.Withaging,theaccumulationofpigmentsfromhomogentisic acidinthejointscausesosteoarthrosis.Thereisnospecifictreatmentforthediseaseand theapproachissymptomatic.Arthroplastyisthesolutionforseverecasesof osteoarthro-siscausedbythispathologicalconditionandpresentsresultscomparabletothosefrom patientswithprimaryosteoarthrosis.Here,thecaseofa67-year-oldpatientwhounderwent severalarthroplastyproceduresbecauseofosteoarthrosiscausedbythisrarepathological conditionispresented.Thelastsurgicalinterventionconsistedoftotalrightknee arthro-plasty.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Osteoartrose
do
joelho
secundária
a
ocronose
–
Caso
clínico
Palavras-chave:
Alcaptonúria Ocronose Joelho Artroplastia
r
e
s
u
m
o
A alcaptonúria é uma doenc¸ametabólica rara em quea deficiência da enzimaácido homogentísico-oxidaseprovocaumaacumulac¸ãodeácidohomogentísico.Aocronose con-sistenadeposic¸ãoexcessivadeácidohomogentísiconotecidoconjuntivoeapresenta-se comoumapigmentac¸ãoacastanhadaoupreta.Comoenvelhecimento,aacumulac¸ãode pigmentosdeácidohomogentísiconasarticulac¸õesprovocaosteoartrose.Nãoexisteum tratamentoespecíficoparaadoenc¸aeaabordagemésintomática.Aartroplastiaéasoluc¸ão
夽
Pleasecitethisarticleas:daSilvaMartinsFerreiraAM,LimaSantosF,CastroCostaAM,PereiraBarbosaBM,ReisRochaRM,Fontes LebreJF.Osteoartrosedojoelhosecundáriaaocronose–Casoclínico.RevBrasOrtop.2014;49:675–680.
夽夽
WorkdevelopedintheVilaNovadeGaiaHospitalCenter,VilaNovadeGaia,Portugal,andEspinhoHospital,Espinho,Portugal.
∗ Correspondingauthor.
E-mail:[email protected](A.M.daSilvaMartinsFerreira).
http://dx.doi.org/10.1016/j.rboe.2013.11.001
paracasosgravesdeosteoartrosecausadaporessapatologiaeapresentaresultados com-paráveis aosdoentescomosteoartroseprimária.Os autoresapresentamocasode um doentede67anossubmetidoaváriasartroplastias,emvirtudedaosteoartrosecausada poressararapatologia.Aúltimaintervenc¸ãocirúrgicafoiumaartroplastiatotaldojoelho direito.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Alkaptonuriaisararerecessiveautosomalmetabolicdisease causedbyabsenceoftheenzymehomogentisicoxidase.This enzymeisresponsiblefordegradationofhomogentisicacid, which isan intermediate product from metabolism ofthe aminoacids tyrosine and phenylalanine. If this enzyme is defective,thisleadstoaccumulationofhomogentisicacidin tissuesandblood.
The incidence of alkaptonuria is less than one in one million.1
Overtime,thedepositsofhomogentisicacidaccumulate inthetissuesandpresentasadarkpigmentation.This con-dition is called ochronosis and it may affect notonly the musculoskeletalsystembutalsothecardiovascularand gen-itourinarysystems,thescleraandtheskin.2,3
Mostofthesymptomsofalkaptonuriaareonlyobserved startinginthefourthorfifthdecade oflife,4exceptforthe
appearanceofdarkurine,whichisdetectedduringchildhood, resultingfromexcretionandoxidationofhomogentisicacid. Alkaptonuria causes progressiveochronotic arthropathy ofthemajor jointsthat are subjecttoweight-bearing. The
Fig.1–Darkpigmentinthesclera,earsandfirstinterdigitalcreaseofthelefthand.Thelastfiguredemonstratesthe darkenedappearanceoftheurine.
knee is the joint that is most affected, followed by the hip.4–6
Thetreatment forthedisease issymptomaticand total arthroplasty is the preferred treatment in severe cases of osteoarthrosis.7,8
Clinical
case
Thepatientwasa67-year-oldmanwhosediagnosisof alkap-tonuriahadbeenmadeattheageof40years.Thefirstsigns ofthediseaseweredarkeningoftheurineandappearanceof darkpigmentsinthesclera,earsandfirstinterdigitalcrease of the left hand (Fig. 1A–D). There were no other relevant antecedentsoranyfamilyhistoryofthedisease.
Attheageof60years,thepatientunderwentasurgical interventiontoextractabladderstone oflargedimensions (Fig.2).
Joint complaints arose some years later and initially affectedthelefthip,followedbytheleftkneeandlastlythe rightknee.
Fig.2–Bladderstone.
lefthip,performedfiveyearsbeforethepresentcase(Fig.3A andB).
Twelvemonthsbeforethepresentcase,thepatient under-wenttotal arthroplastyoftheleft knee(Fig.4A–C).Both of thesesurgicalprocedureswereperformedatanother hospi-talinstitution.Sofar,therehavenotbeen anymentionsof postoperativecomplications.
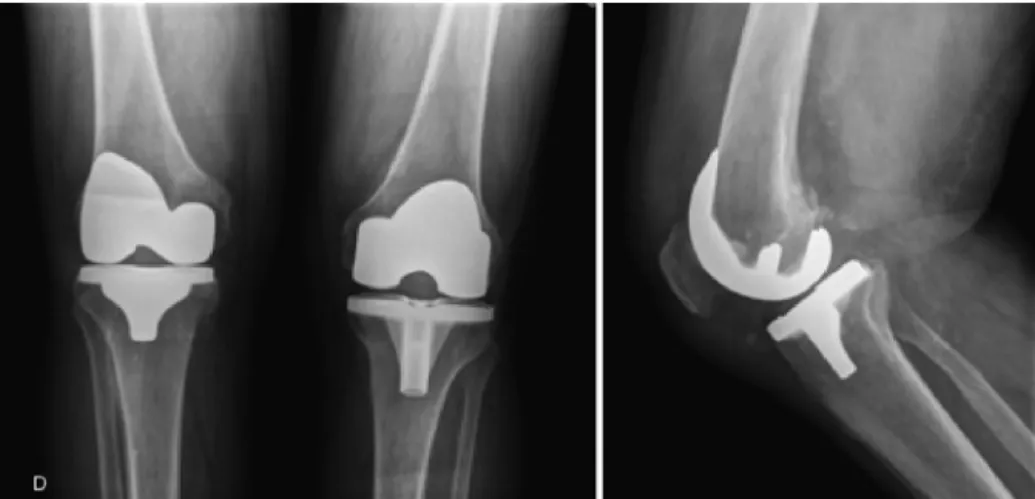
Attheconsultationofthepresentcase,thepatient pre-sentedcomplaintsofpaininhisrightknee,withavarusknee andradiologicallyobservedthree-compartmentgonarthrosis ofAhlbäckgradeIV(Fig.4AandB).
The patient underwent total arthroplasty of the right knee(Fig.5AandB)atourhospital.Thecomplaintsofpain improvedimmediatelyaftertheoperation.
Aftersixmonthsoffollow-up,thepatientisnow asymp-tomaticandabletowalkwithoutgaitsupports.Hismobility isfrom0◦to110◦ intherightkneeand0◦to120◦ intheleft
knee.Hecontinuestobefollowedupasanoutpatient.
Discussion
Alkaptonuriawasfirstdescribedin1584,inchildrenwithdark urine.
Atthe endof the 1990s,it wasobserved that the gene forthispathologicalconditionwaspresentatthelocus 3q21-23.9
Ochronosis consists of deposition of pigments from homogentisicacidinalltypesofconnectivetissueand par-ticularly incartilage. Itmainly affects the musculoskeletal system,butcanalsoaffectthecardiovascularand genitouri-narysystems,thescleraandtheskin.2,3
The first clinical manifestation of alkaptonuria is the appearanceofdarkurine.10Otheralterationsthatareoften
neglectedincludechangestothecolorofthescleraandears. Thesesignscouldalsobeidentifiedinourpatient.
Ochronoticarthropathyfundamentallyaffectsindividuals from theageof40yearsonwards,asseeninthecase pre-sentedhere.Thepaincomplaintsaffectthemajorjointsand especiallytheknees,followedbythe hips,shoulders,spine andeventheribs.11Inourcase,thefirstjointtobeaffected
wasthelefthip.
Thepigmentationalsoaffectsthetendonsandligaments, becauseoftheirhighcollagencontent,anditcauses inflam-matoryalterationsthatmayleadtotearing.7
Likeinpatientswithprimaryosteoarthrosis,narrowingof the interlineandsclerosis ofthe jointspaceare frequently seen.However,theradiologicalalterationsmaybemuchless exuberantthantheclinicalmanifestations.
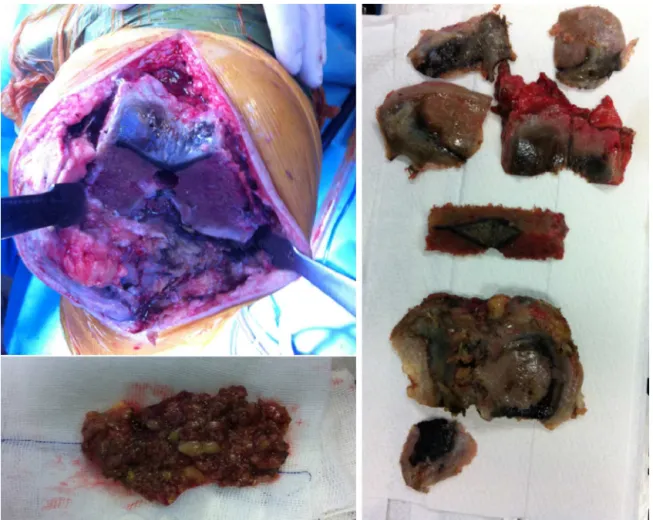
Macroscopically, patientsaffected byochronosis present small particles resembling soot, encrusted in the menisci, tendonsandligaments,whichconfers thetypicaldark col-orationofthejoints.Thiscouldbeseenintheintraoperative imagesofthepresentcase(Fig.6A–C).The anatomopatholog-icalexaminationontheoperativespecimensconfirmedthe diagnosis.
There is no specificmedical treatmentfor alkaptonuria and therefore thetherapeuticapproachis symptomatic.In
Fig.4–Totalarthroplastyoftheleftkneeperformed12monthsbeforethepresentcase.Rightkneewiththree-compartment gonarthrosisofAhlbäckgradeIV.
Fig.6–Intraoperativeimagesdocumentingthetypicaldarkcolorationofthejointthatresultedfromdepositionofpigments fromhomogentisicacidinthejointcartilage,menisci,tendonsandligaments.
severecasesofosteoarthrosis,totalarthroplastyisthe pre-ferredtreatment.7,8
Fewstudieshavereportedthemechanicaldifferencesthat mayoccurintheboneandsofttissuesofpatientswhoundergo arthroplasty, or the complications during the operationor postoperativefollow-up.
In patients undergoing total knee arthroplasty, Spencer etal.12werefacedwithintraoperativedifficultiesindisplacing
thepatella,becausethequadricepsandpatellartendonswere extremelyhard.Althoughwedidnothavethisdifficulty,we observedduringtheoperationthatboththehipspresentedan unusuallyhardconsistency.
Inthesame study,nocomplicationsrelating toimplant failureweredetectedinpatientswithochronosiswho under-went total arthroplasty on different joints, with 12 years offollow-up. Other studieshavepresentedresults compat-iblewith performingarthroplasty inpatients withprimary osteoarthrosis.13–15
Earlytreatmentforalkaptonuriamaybeachallenge,given thattheapproachissymptomatic.
Cases of ochronotic arthrosis that are more advanced requiresurgicaltreatment.
Asalreadyreportedtotalkneearthroplastypresentsgood resultsinpatientswithgonarthrosis secondarytothisrare pathologicalcondition.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.SmithRJ.Disordersofaminoacidmetabolism.In:HumesHD, editor.Kelley’stextbookofinternalmedicine.4thed. Philadelphia:LippincottWilliams&Wilkins;2000.p.2788–93.
2.NasK,GürA,AkdenizS,CevikR,HarmanM,Sarac¸AJ. Ochronosis:acaseofsevereochronoticarthropathy.Clin Rheumatol.2002;21(2):170–2.
3.WauthyP,SeghersV,MathonetP,DeuvaertFE.Cardiac ochronosis:notsobenign.EurJCardiothoracSurg. 2009;35(4):732–3.
4.GainesJJJr.Thepathologyofalkaptonuricochronosis.Hum Pathol.1989;20(1):40–6.
5.AlbersSE,BrozenaSJ,GlassLF,FenskeNA.Alkaptonuriaand ochronosis:casereportandreview.JAmAcadDermatol. 1992;27(4):609–14.
6.LaDuBNJr.Alcaptonuriaandochronoticarthritis.MolBiol Med.1991;8(1):31–8.
8. BormanP,BodurH,CilizD.CilizOchronoticarthropathy. RheumatolInt.2002;21(5):205–9.
9. Fernández-Ca ˜nónJM,GranadinoB,Beltrán-ValerodeBernabé D,RenedoM,Fernández-RuizE,Pe ˜nalvaMA,etal.The molecularbasisofalkaptonuria.NatGenet.1996;14(1):19–24.
10.ResnickD.Alkaptonuria.In:ResnickD,NiwayamaG,editors. Diagnosisofboneandjointdisorders.2nded.Philadelphia: Saunders;1988.p.1787–803.
11.O’BrienW,LaDuBN,BunimJJ.Biochemical,pathologicand clinicalaspectsofalcaptonuria,ochronosis,and
ochronoticarthropathy.AmJMed.1963;34:813–38.
12.SpencerJM,GibbonsCL,SharpRJ,CarrAJ,AthanasouNA. Arthroplastyforochronoticarthritis:nofailureof11
replacementsin3patientsfollowed6–12years.ActaOrthop Scand.2004;75(3):355–8.
13.AydogduS,CulluE,OzsoyMH,SurH.Cementlesstotalknee arthroplastyinochronoticarthropathy:acasereportwitha 4-yearfollow-up.JArthroplasty.2000;15(4):
539–43.
14.MoslavacA,MoslavacS,CopR.Casereportofapatientwith ochronosisandarthroplastyofthehipandbothknees. Reumatizam.2003;50(1):26–8.