www.jped.com.br
ORIGINAL
ARTICLE
Health
promoting
behaviors
in
adolescence:
validation
of
the
Portuguese
version
of
the
Adolescent
Lifestyle
Profile
夽
Pedro
Sousa
a,b,∗,
Pedro
Gaspar
a,b,
Helena
Fonseca
c,d,
Constance
Hendricks
e,
Carolyn
Murdaugh
faSchoolofHealthSciences,InstitutoPolitécnicodeLeiria,Leiria,Portugal bHealthResearchUnit(UIS),InstitutoPolitécnicodeLeiria,Leiria,Portugal cSchoolofMedicine,UniversidadedeLisboa,Lisbon,Portugal
dPediatricObesityClinic,DepartmentofPediatrics,HospitaldeSantaMaria(HSM),Lisbon,Portugal eSchoolofNursing,AuburnUniversity,Auburn,UnitedStates
fCollegeofNursing,UniversityofArizona,Tucson,UnitedStates
Received14April2014;accepted10September2014 Availableonline26February2015
KEYWORDS
Lifestyle; Adolescents; Instrument validation; Portuguese; Health-promoting; Psychometric
Abstract
Objective: Reliableand valid instruments areessential for understandinghealth-promoting
behaviorsinadolescents.Thisstudyanalyzedthepsychometricproperties ofthePortuguese
versionoftheAdolescentLifestyleProfile(ALP).
Methods: AlinguisticandculturaltranslationoftheALPwasconductedwith236adolescents
fromtwodifferentsettings:acommunity(n=141)andaclinicalsetting(n=95).Internal
con-sistencyreliabilityandconfirmatoryfactoranalysiswereperformed.
Results: Results showed an adequate fit to data, yielding a 36-item, seven-factor
struc-ture (CMIN/DF=1.667, CFI=0.807, GFI=0.822, RMR=0.051, RMSEA=0.053, PNFI=0.575,
PCFI=0.731).The ALPpresented ahighinternal consistency (␣=0.866),with thesubscales
presentingmoderatereliabilityvalues(from0.492to0.747).Thehighestvalueswerein
Inter-personalRelations(3.059±0.523)andPositiveLifePerspective(2.985±0.588).Somegender
differenceswerefound. Findingsshowedthatadolescentsfromtheclinicreportedan
over-allhealthierlifestylethanthosefromthecommunitysetting(2.598±0.379vs.2.504±0.346;
t=1.976,p=0.049).
夽
Pleasecitethisarticleas:SousaP,GasparP,FonsecaH,HendricksC,MurdaughC.Healthpromotingbehaviorsinadolescence:validation
ofthePortugueseversionoftheAdolescentLifestyleProfile.JPediatr(RioJ).2015;91:358---65.
∗Correspondingauthor.
E-mail:[email protected](P.Sousa). http://dx.doi.org/10.1016/j.jped.2014.09.005
Conclusion: TheALPPortugueseversionisapsychometricallyreliable,valid,anduseful
mea-surement instrument for assessing health-promoting lifestyles in adolescence. The ALP is
cross-culturallyvalidatedandcandecisivelycontributetoabetterunderstandingofadolescent
healthpromotionneeds.Additionalresearchisneededtoevaluatetheinstrument’spredictive
validity,aswellasitsclinicalrelevanceforpracticeandresearch.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Estilodevida; Adolescentes; Validac¸ão instrumental; Português;
Promoc¸ãodasaúde; Psicometria
Comportamentosdepromoc¸ãodasaúdenaadolescência:validac¸ãodaversãoem portuguêsdoPerfildoEstilodeVidaAdolescente
Resumo
Objetivo: Osinstrumentosconfiáveiseválidossãofundamentaisparaentenderosestilosde
vidadepromoc¸ãodasaúdedeadolescentes.Esteestudoanalisaaspropriedadespsicométricas
daversãoemportuguêsdoPerfildoEstilodeVidaAdolescente(ALP).
Métodos: Foirealizadaumatraduc¸ãolinguísticaeculturaldoALPcom236adolescentesdeduas
configurac¸õesdiferentes: uma configurac¸ãode comunidade(N=141)e umaclínica (N=95).
Foramrealizadas uma análisedaconfiabilidadedacoerência internae umaanálisefatorial
confirmatória.
Resultados: Osresultados mostraram-se adequados aosdados, gerandouma estruturade 7
fatores com 36 itens (CMIN/DF=1,667,IAC=0,807, GFI=0,822, RMR=0,051, RMSEA=0,053,
PNFI=0,575, PCFI=0,731). O ALP apresentou grande coerência interna (␣=0,866), com
as subescalas apresentando valores de confiabilidade moderados (de 0,492 a 0,747). Os
maioresvaloresforamdeRelac¸õesInterpessoais(3,059±0,523)ePerspectivadeVidaPositiva
(2,985±0,588).Foramencontradasalgumasdiferenc¸asentreossexos.Osachadosmostraram
que os adolescentes da clínica relataram um estilo de vida mais saudável em geral que
osdaconfigurac¸ãodacomunidade(2,598±0,379em comparac¸ãoa2,504±0,346;t=1,976,
p=0,049).
Conclusão: AversãoemportuguêsdoALPéuminstrumentodemensurac¸ãopsicometricamente
confiável,válidoeútilparaavaliarosestilosdevidadepromoc¸ãodasaúdenaadolescência.
OALPé validadoem diferentesculturasepodecontribuir deformadecisivapara um
mel-horentendimentodasnecessidadesdepromoc¸ãodasaúdenaadolescência.Énecessáriauma
pesquisaadicionalparaavaliaravalidadepreditivadoinstrumento,bemcomosuarelevância
clínicaparaapráticaepesquisa.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos
reservados.
Introduction
AvitalcomponentforattainingthegoalsofHealthyPeople 2020isthepromotionofhealthylifestyles.Healthpromotion continuestobeconsideredthemostcosteffectiveapproach toimprovingwell-beingandqualityoflife.1Ithasbeen esti-matedthatasmuchas60%ofthequalityofanindividual’s healthandlifedependsonhis/herbehaviorandlifestyle.1
Results fromthe 2009/2010 HealthBehavior in School-aged Children survey2 indicate variations in patterns of healthanditssocialdeterminantsbetweencountries. Sig-nificantinequalitiesinhealthandsocialindicatorsaccording toage,gender,andsocialeconomicstatusarealsoevident. Manyeffectsofhealth-riskfactorsamongadultsare avoid-ableifthesebehaviorsareidentifiedandchangedatanearly stage.3Therefore,itisessentialtounderstandandevaluate health-promotingbehaviorsamongadolescentsin orderto promotetheirhealthygrowth.
Health-promoting behaviors (HPB) are defined as a positiveapproachto living,increasingwell-being,and
self-actualization.4 Health promoting activities are defined as thoseactivitiesthatcontributetohealth,whilepreventive behaviors are actions to avoid or forestall the develop-ment of disease. Pender described a healthy lifestyle as incorporating the complementary components of both healthpromotionandprevention.HPBdevelop theenergy necessary toincreasehuman potential.4 Use of HPB com-plements the stabilizing tendency of disease prevention, which is directed toward early detection. Rather than stabilization and avoidance of disease, HPB develop the tensionnecessarytoincreasehumanpotential.4
HPB in adolescence have been linked with the psy-chological attributes of self-esteem, self-efficacy, and hope.5 However,therearefew studies onadolescentHPB and a scarce number of instruments have been devel-opedspecificallyforthispurpose:theAdolescentLifestyle Questionnaire,6 the Adolescent Health-Promoting Scale,7 andtheAdolescentLifestyleProfile(ALP).8
highlightsthe active roleof individuals in managing their own health behavior, widely used for understanding the predictorsof health behaviorsandlifestyles, namely with adolescentsfromtheUSA.9TheALPwasdesignedto mea-sure the frequency of HPB in adolescents (early, middle, andlate)in sevendomains: health responsibility,physical activity,nutrition, positive life perspective, interpersonal relations,stressmanagement,andspiritualhealth.This cur-rentversionofALPhasbeentestedinnumerousadolescent (11-20years)sampleswithdocumentedreliabilityand valid-ity(alphacoefficientof0.929).8
AlthoughtheALPhasnotbeenusedinstudiesinvolving othersthan Americanadolescents,theadult version from whichtheALPwasderived(theHealth-PromotingLifestyle Profile) has been translated into Persian,10 Japanese,11 Spanish,12 Turkish,13 Portuguese,14 and Chinese,15 andhas beenappliedtohealthypeopleaswellaspeoplewith clin-ical disorders, such as cancer, neurologic, and metabolic syndromes.12
A reliable and valid instrument for the measurement of healthy lifestyles is essential tounderstand the needs of health promotion among adolescents.16,17 Obtaining an accurate and equivalent cross-cultural assessment of a psychological construct has been considered a key ele-ment of research, since the same construct may differ acrosscountriesandcontexts.18 Moreover,nostudysofar hasapplieda standardized instrumentfor examiningsuch behaviorsinaPortugueseadolescentpopulation.Giventhat Portugueseisthefifthmostspokenlanguageintheworld, andthethirdmostspokenintheWesternHemisphere,with about 272.9 million speakers, the purpose of the present studywastoexaminethereliabilityandconstructvalidity ofthePortugueseversionoftheALP.
Methods
Participants
Adescriptivecross-sectionalstudywithPortuguese adoles-centswasconducted.Theeligibilitycriteriawereasfollows: I)age12-18years;II) abletocommunicatein writing;III) Portuguese nationality; IV) provided informed consent to participateinthestudy.Exclusioncriteriawerethepresence ofseverepsychopathologyandtheinabilitytocompletethe questionnairesbecauseoflanguagebarriers.
Awiderangeofrecommendationsregardingsamplesize infactoranalysishavebeenmade.Someauthors19 suggest that100 respondents isthe absolute minimumnumber to beabletoundertakefactoranalysis.Otherswouldsuggest thatanadequatesamplesizeforconfirmatoryfactor analy-sis(CFA)consideredn≥200.20Thereisalsoaruleofthumb offiverespondentsperitem.21 Therefore,itwasnecessary torecruitatleast220adolescents(5×44items).
A convenience sample (n=236) was selected based on theeligiblepopulationresponsetotheonlinequestionnaire. Adolescents were recruited from two different settings: settingA)studentsfromacommunitysetting(apublichigh school); setting B) adolescents from a pediatric obesity clinic. Addressing promotionof healthy lifestyles requires a broad approach that includes both health promotion and prevention.4 The option to select a wide variety of
participants has the purpose of increasing the external validityoftheinstrumentandaddressingthisdemand.
ParticipantsofsettingA(n=141)wererecruitedwiththe supportof the teachers,according totheresearch proto-colpreviouslygiven.ParticipantsofsettingB(n=95)were recruitedwith thesupportof theclinical staff, according tothe researchprotocol previously given.Datacollection in both samples occurred in 2012. Baseline comparison indicatedthatbothsettingswereequivalentregarding ado-lescents´sociodemographiccharacteristics.
Instrument
The ALP8 was designed to measure the frequency of health promoting behaviorsin adolescents(early, middle, andlate).The revisedHealth-PromotingLifestyleProfile-II servedastheprototypefortheinitialgenerationoftheALP. Itbecameapparentthatitemsusedforadultsdidnot‘‘fit’’ adolescents. Internal consistency reliabilityand construct validityindicatedthattheALPwasreliableandvalid.8
The ALP has undergone some minor revisions since its development.TheALPcurrentversion(ALP-R2©)isa44-item summated behaviorratingscalethatemploys afour-point Likert-type responseformat, ranging from1=‘‘Never’’to 4=‘‘Always’’,withapossiblescorebetween44and176.
Hendricks et al.8 reported Cronbach’s alphas for the sevensubscales:HealthResponsibility(HR;0.825),Physical Activity(PA;0.773),Nutrition(N;0.648),PositiveLife Per-spective (PLP;0.810), Interpersonal Relations (IR; 0.769), Stress Management (SM; 0.656), and SpiritualHealth (SH; 0.824).ThetotalALPreliabilityscorewas0.929.A princi-palaxisfactoranalysissupportedthepresenceoftheseven factors usedassubscales. The higher thescore ona sub-scale, the greater the health behavior for that domain. Both subscales and a total scale score can be obtained. Strong correlations between the ALP and the Adolescent HopeScaleandbetweentheALPandtheSelf-EfficacyScale were identified in a previous study with a sample of 168 student-athletes.9
Procedures
TheculturaladaptationofALPtothePortugueselanguage wasauthorizedbytheauthorsoftheoriginalversion.Two bilingual translators, specialists in health sciences, sepa-ratelytranslatedtheEnglishoriginalversionintoEuropean Portuguese, reaching a consensual version after two iter-ations. Next,twoother bilingualtranslators(independent of the firstpair), also specialists in health sciences, back translatedthescaleintoEnglish,obtainingafinalversionby consensusaftertwoiterations.22 Thetranslationprocedure wasevaluatedforconceptual,semantic,content,technical, andcriterion equivalencesbyapanel offiveinvestigators withextensivebackgroundinhealthinterventionresearch, behavioralmodification,andhealthpromotion.Thetwo ver-sions were sent to the ALP authors, who considered the versionsequivalent.
rated the instructions and scale items as either clear or unclear.Nodifficultiesinunderstandingandcompletingthe instrumentwereidentified.
The research protocol was formally approved by the EthicsCommitteeandtheHospitalAdministration,andby the Portuguese Department of Education (Direc¸ão Geral de Inovac¸ão e de Desenvolvimento Curricular). All proce-duresrespectedtheDeclarationofHelsinki23andtheethical principlesof theAmericanPsychological Association.24 All participantshadaccesstothedescriptionofthestudyand itsobjectives,andwereinformedofalltheethicalaspects inherenttotheconfidentialityandvoluntarybasis oftheir participation.
DataAnalysis
TheonlinequestionnairedatawasanalyzedwithStatistical PackageforSocialSciences(SPSSInc.StatisticsforWindows, version17.0,Chicago,USA)andAMOS(SPSSInc.Computer Program,version20.0,Chicago,USA)software.Descriptive statisticswerecalculatedforeachitem.TheALPtotalscore wasobtainedby averagingtheresponses toallitems.The sameprocedurewasadoptedforallthesubscalesscores.
Internal consistency using Cronbach’s alpha was cal-culated for the total scale aswell as for each subscale. Thehomogeneityindiceswasalsoanalyzedinorderto deter-minewhichitemstoconsiderforelimination.Accordingto Hairetal.,25 an itemwitha correcteditem-total correla-tionlessthan0.20shouldbedeleted.Anacceptablealpha reliabilitycoefficientisconsideredtobe0.80orgreaterfor atestedscale.26
A confirmatory factor analysis (CFA) was used to test theadequacyofthemodelunderlyingtheoriginalstructure of theALP proposedby the authors.Once themodel was
defined,themultivariatenormality wasanalyzedwiththe Mardiacoefficient(99.974).Therefore,assumingthe exist-enceofmultivariatenormality,themodelparameterswere estimatedusingthemaximumlikelihoodprocedure.TheCFA criteriaforanacceptablemodelwere:
- chi-squared/degreesoffreedom(CMIN/DF)<3.0; compar-ativefitindex(CFI)andgoodnessoffitindex(GFI)>0.80; root mean squareresidual (RMR)and root meansquare errorofapproximation(RMSEA)<0.05;25,27
- parsimonynormedfitindex(PNFI)andparsimony compar-ativefitindex(PNFI)>0.50.28
Following the recommendations of Marsh et al.,29 the criteria applied in the selection of items to develop a short-formofALPwere:factorloadings,correcteditem-test correlation, Cronbach’s alpha, skewness/kurtosis (sk/ku) values,andthetheoreticalimportanceinitselfofthe dif-ferentitems.
Results
Sociodemographicandbehavioralcharacteristics
The study sample included 236 adolescents, 45.8% male and54.2% female. The mean age of the participants was 15.15±1.583. The mean overall lifestyle score reported by adolescents was 2.542±0.362. On the ALP domains, adolescents scored highest on IP (3.059±0.523) and PLP (2.985±0.588),andscoredlowestonSH(1.860±0.640).
Table 1 presents the descriptive statistics of the total scale and subscales. Total and subscale mean scores dif-fered between males and females. Females reported an overall healthier lifestyle than males (2.591±0.350 vs.
Table1 DescriptivestatisticsofPortugueseversionoftheAdolescentLifestyleProfile (36items)accordingtogender and
clinical/communitysetting.
Variable Male(n=108) Female(n=128) p
HR 2.100±0.587 2.309±0.524 0.004(t=-2.887)
PA 2.558±0.645 2.273±0.569 0.000(t=3.613)
N 2.628±0.496 2.667±0.462 0.530(t=-0.629)
PLP 2.905±0.602 3.052±0.570 0.056(t=-1.917)
IR 2.831±0.463 3.250±0.495 0.000(t=-6.678)
SM 2.789±0.543 2.876±0.483 0.194(t=-1.302)
SH 1.745±0.603 1.957±0.657 0.011(t=-2.570)
TOTAL 2.483±0.369 2.591±0.350 0.023(t=-2.288)
School(n=141) POC/HSM(n=95)
HR 2.178±0.558 2.266±0.567 0.243(t=1.170)
PA 2.399±0.588 2.410±0.668 0.887(t=0.143)
N 2.550±0.456 2.796±0.474 0.000(t=4.000)
PLP 2.936±0.564 3.056±0.618 0.124(t=1.544)
IR 3.039±0.509 3.087±0.545 0.487(t=0.697)
SM 2.767±0.483 2.939±0.538 0.011(t=2.559)
SH 1.895±0.651 1.807±0.624 0.303(t=-1.032)
TOTAL 2.504±0.346 2.598±0.379 0.049(t=1.976)
HR,healthresponsibility;PA,physicalactivity;N,nutrition;PLP,positivelifeperspective;IR,interpersonalrelations;SM,stress
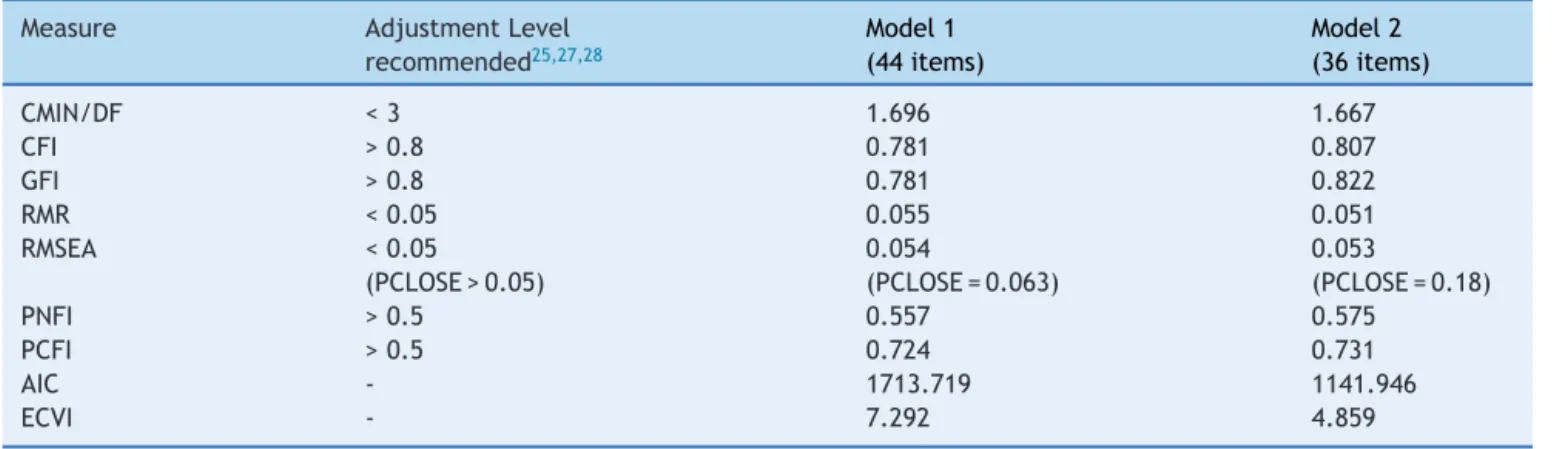
Table2 SummaryoftheadjustmentindicesofthePortugueseversionoftheAdolescentLifestyleProfile.
Measure AdjustmentLevel
recommended25,27,28
Model1 (44items)
Model2 (36items)
CMIN/DF <3 1.696 1.667
CFI >0.8 0.781 0.807
GFI >0.8 0.781 0.822
RMR <0.05 0.055 0.051
RMSEA <0.05
(PCLOSE>0.05)
0.054
(PCLOSE=0.063)
0.053
(PCLOSE=0.18)
PNFI >0.5 0.557 0.575
PCFI >0.5 0.724 0.731
AIC - 1713.719 1141.946
ECVI - 7.292 4.859
CMIN/DF,chi-squared/degrees offreedom;CFI, comparativefitindex; GFI,goodnessoffitindex; RMR,rootmeansquare residual;
RMSEA,rootmeansquareerrorofapproximation;PNFI,parsimonynormedfitindex;PCFI,parsimonycomparativefitindex;AIC,Akaike
informationcriterion;ECVI,expectedcrossvalidationindex;PCLOSE,pvalueofclosefit.
2.483±0.369; t=-2.288, p=0.023). Adolescents fromthe clinicreportedanoverallhealthierlifestylethanthosefrom the community setting (2.598±0.379 vs. 2.504±0.346; t=1.976,p=0.049).Theyalsoreportedhighervaluesonthe Nsubscale(t=4.000,p=0.000)andlowervaluesontheSM subscale(t=2.559,p=0.011).
Constructvalidity(CFA)
CFA was performed to test how well the correlations betweentheitemscorresponded totheoriginalALP scale structure.The resultsof theCFAdidnotprovide satisfac-toryfitindexesfortheinitialmodel(CFI=0.781,GFI=0.781, RMR=0.055,RMSEA=0.054;Table2).
Therefore,ashorterversionwasdeveloped,takinginto considerationthepredefinedcriteria.Eightitemswere elim-inated:threeitemswithlowfactorloadsorlowitem-total correlations,andfiveitemswithsk/kuvalueseitherbelow -1orabove1.Twoitemswerekeptattendingtotheir theo-reticalimportance(ALP4andALP13).TheHR,SH,SM,and PAsubscaleslostoneitemeachandthePLPandIRsubscales losttwoitemseach.
Themodel2structurecomprisedsevenlatentvariables, 36observedvariables,and36errorterms.Therefinementof model2wasbasedonmodificationindices.Thecorrelations trajectorieswereallowed betweentheerrorterms e4-e6, ande19-e20.
The goodness-of-fit values were adequate attesting thefactorial validity ofALP Portuguese version (Table2): CMIN/DF=1.667, CFI=0.807, GFI=0.822, RMR=0.051, RMSEA=0.053, PNFI=0.575, PCFI=0.731. Analysing com-parative measures of fit with the Akaike information criterion(AIC)andexpectedcrossvalidationindex(ECVI), bothestimatedmodelswerecompared.Model1(44items) scoreswere:AIC=1,713.719 andECVI=7.292.Model2(36 items) scores were: AIC=1,141.946 and ECVI=4.859. As lowervaluesindicateabetterfit,Model2wasconsidered thebestfittingmodel.
Reliability
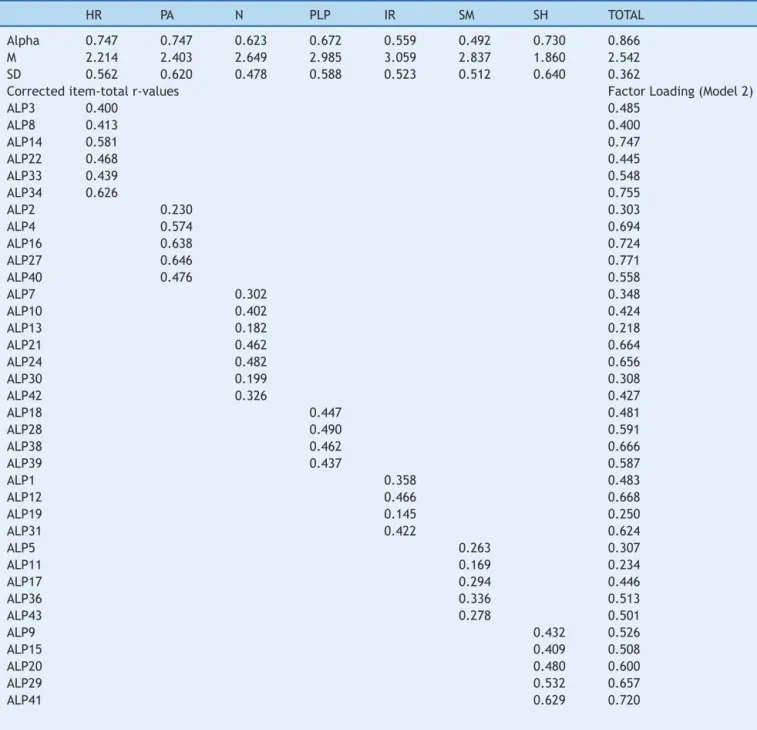
Cronbach’salphawasusedasanestimateofinternal consis-tencyreliability.Thetotalalphawas0.866andthereliability values of the seven subscales ranged from 0.492 (SM) to 0.747 (HR and PA). Corrected item-total r-values ranged between0.145 (ALP19)and0.646(ALP27);factor loadings rangedbetween0.218(ALP13)and0.771(ALP27;Table3).
All subscales had significant, moderate-to-strong cor-relations with the total scale, meeting minimal criteria (Table 4). Correlations ranged from 0.506 (SH) to 0.727 (HR). Subscale tosubscale correlationswere also statisti-cally significant (p<0.05),ranging from0.131 (SH---SM) to 0.524(SM---IR).
Discussion
In orderto assess adolescent lifestyle behaviorsand help planningappropriateinterventions, acomprehensive,easy to administer, both psychometrically sound and clinically usefulinstrumentisneeded.8Thepurposeofthisstudywas toreportthepsychometricpropertiesofthePortuguese ver-sionoftheALP.
Constructvaliditywastested throughCFA.The Revised CFAresultedinabetterfitofthemodelforthePortuguese version (36 items), when compared tothe original struc-ture.Theexclusionofeightitemsmayreflectthefactthat someitemshavemeaningsthatoverlapwithmorethanone concept.Thedifficultiesperceivedintranslatingsomeofthe itemsintoPortuguesewerenoteworthy,whichmayexplain thedifferencesencountered.
Table3 Descriptivestatistics,correcteditem-totalr-values,factorloadings,andCronbach’salphaofthePortugueseversion
oftheAdolescentLifestyleProfile(ALP;36items).
HR PA N PLP IR SM SH TOTAL
Alpha 0.747 0.747 0.623 0.672 0.559 0.492 0.730 0.866
M 2.214 2.403 2.649 2.985 3.059 2.837 1.860 2.542
SD 0.562 0.620 0.478 0.588 0.523 0.512 0.640 0.362
Correcteditem-totalr-values FactorLoading(Model2)
ALP3 0.400 0.485
ALP8 0.413 0.400
ALP14 0.581 0.747
ALP22 0.468 0.445
ALP33 0.439 0.548
ALP34 0.626 0.755
ALP2 0.230 0.303
ALP4 0.574 0.694
ALP16 0.638 0.724
ALP27 0.646 0.771
ALP40 0.476 0.558
ALP7 0.302 0.348
ALP10 0.402 0.424
ALP13 0.182 0.218
ALP21 0.462 0.664
ALP24 0.482 0.656
ALP30 0.199 0.308
ALP42 0.326 0.427
ALP18 0.447 0.481
ALP28 0.490 0.591
ALP38 0.462 0.666
ALP39 0.437 0.587
ALP1 0.358 0.483
ALP12 0.466 0.668
ALP19 0.145 0.250
ALP31 0.422 0.624
ALP5 0.263 0.307
ALP11 0.169 0.234
ALP17 0.294 0.446
ALP36 0.336 0.513
ALP43 0.278 0.501
ALP9 0.432 0.526
ALP15 0.409 0.508
ALP20 0.480 0.600
ALP29 0.532 0.657
ALP41 0.629 0.720
HR,healthresponsibility;PA,physicalactivity;N,nutrition;PLP,positivelifeperspective;IR,interpersonalrelations;SM,stress
man-agement;SH,spiritualhealth.
difficulty of Portuguese adolescentsin accepting theseas HPB.The PLP concept,SH, and SMstrategies maynot be sufficientlyusedor understood by Portuguese adolescents yet.
However, the need for elimination of the items ALP44 (Avoidbehaviorsthatdamage myhealth-smoking, drink-ing, doing drugs, sexual activity) and ALP32 (Play active games with my friends - basketball, softball, volleyball, tennis, etc.) may be explained differently. The complex-ity of the items, as they contain multiple behaviors, might have contributed to the difficulty encountered in answering.
Despite presenting a low factor loading (ALP13: Eat breakfast)andhighsk/kuvalues(ALP4:Engageinvigorous physicalactivityfor20minutesormorethreedaysaweek), itwasdecidedtokeepthesetwoitems,duetotheir theoret-icalimportance.Infact,theyprovidevaluableinformation onnutritionand physical activity behaviorstrategies that areessentialforlearningaboutlifestylechoices.8
Table4 PearsoncorrelationsbetweenthePortugueseversionoftheAdolescentLifestyleProfilefactorsandtotalscore.
HR PA N PLP IR SM SH
HR 1
PA 0.321a 1
N 0.384a 0.423a 1
PLP 0.376a 0.319a 0.322a 1
IR 0.433a 0.221a 0.336a 0.486a 1
SM 0.444a 0.279a 0.429a 0.491a 0.524a 1
SH 0.281a 0.216a 0.149b 0.174a 0.254a 0.131b 1
TOTAL 0.727a 0.631a 0.690a 0.654a 0.664a 0.693a 0.506a
HR,healthresponsibility;PA,physicalactivity;N,nutrition;PLP,positivelifeperspective;IR,interpersonalrelations;SM,stress
man-agement;SH,spiritualhealth.
ap<0.001.
b p<0.05.
model (36 items) presented an adequate fit to thedata, yielding a seven-factor structure. Previous studies have notedthatmajorcautionmustbeadoptedwhenassuming asingle‘criticalcut-offpoint’value,especiallyusingGFI, TLI,IFI,andCFI,consideringthesusceptibilityofindicesto modelcomplexityanddatadistribution.
TheCronbach’salphaobtainedwasadequate(␣ =0.866)
but lower than in the original study (0.929),8 which may reflect the cultural difference for items originally in the ALP. Moreover, some authors consider that the maximum expected value is 0.90. Above this value, either there is redundancyor duplication,orseveralitemsaremeasuring thesameelementofaconstruct.30
Thepresentresultssuggestastrongrelationshipbetween the concepts represented by each subscale, particularly betweenIRandSM,which isconsistentwiththefactthat both subscales analyze cognitive and emotional aspects. Theconceptofstressmanagementinvolvesidentifyingand mobilizingpsychologicalandphysicalresourcesforreducing andmanaging stress effectively.The IRsubscale refersto theuse of communication toachieve a senseof intimacy and closeness in meaningful relationships, involving shar-ingofthoughtsandfeelings,throughverbalandnonverbal messages.4
Findings also suggests that these adolescents tend to engageinmeaningfulandhealthyrelationships,maximizing theirhumanpotentialfor wellnessthroughfindingasense of purpose, and working toward a goal in life. However, theymayhavedifficultyinconsideringspiritualaspectsas protective,andasHPB.
Interestingly, some gender differences were found. FemaleadolescentsreportedhighermeanscoresinHR,IR, and SH, with maleadolescents reporting higher PA mean scores.
Thesefindingsalsodemonstratedthatadolescentsfrom theclinicreportedhigherscoresinHPB,probablyreflecting thefactthattheyareregularlyexposedtomultidisciplinary medical, psychological, nutritional, and physical activity support.
Among the limitations of this study is the sampling technique,namely use of anon-random sample from two settings,which prevents generalizability of the results to other samples of Portuguese adolescents and may have caused some bias. Another limitation concerns the small
samplesize(n=236),whichmaylimittheinterpretationof theCFIresults.
ThePortugueseversionoftheALPshowedgood psycho-metricproperties,bothinterms ofvalidityandreliability. The current study supports the cross-cultural utility of theALP asatoolfor assessinghealth-promoting lifestyles among adolescents, representing a crucial instrument to understandandmeetadolescents’healthpromotionneeds. Futureresearchisneededtoexaminethepredictivevalidity ofthePortugueseversionofthescale.
Funding
ThisworkwaspartiallyfundedbyFundac¸ãoparaaCiência e a Tecnologia (PTDC/DTP-PIC/0769/2012) and supported by the Polytechnic Institute of Leiria, Portugal and the DepartmentofPediatricsatHospitaldeSantaMaria,Lisbon, Portugal.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
ThisworkwaspartiallyfundedbyFundac¸ãoparaaCiência e a Tecnologia (PTDC/DTP-PIC/0769/2012) and supported by the Polytechnic Institute of Leiria, Portugal and the DepartmentofPediatricsatHospitaldeSantaMaria,Lisbon, Portugal. The authors gratefullyacknowledge the clinical staff of the Pediatric Obesity Clinic for their dedication. They also thankall the adolescents andparents for their participationandcollaboration.
References
1.WorldHealth Organization. TheWHO cross-nationalstudyof health behaviourin school-aged childrenfrom 35 countries: findingsfrom2001-2002.JSchHealth.2004;74:204---6.
2.CurrieC,ZanottiC,MorganA, CurrieD,LoozeM,RobertsC,
etal.Socialdeterminantsofhealthandwell-beingamongyoung
people.HealthBehaviourinSchool-agedChildren(HBSC)study:
WHORegionalOfficeforEurope;2012(HealthPolicyfor
Chil-drenandAdolescents,No.6).
3.WangD,OuCQ,ChenMY,DuanN.Health-promotinglifestyles ofuniversity studentsinmainlandChina. BMCPublicHealth. 2009;9:379.
4.PenderN,MurdaughC,ParsonsM.Health promotionin nurs-ingpractice.6thed.UpperSaddleRiver:Pearson/Prentice-Hall; 2010.
5.HendricksC,MurdaughC,TavakoliA,HendricksD.Health pro-motingbehaviorsamongruralsouthernearlyadolescents.ABNF Journal.2000;11:123---8.
6.GillisA.TheAdolescentLifestyleQuestionnaire:development andpsychometrictesting.CanJNursRes.1997;29:29---46.
7.ChenM,WangE,YangR,LiouY.Adolescenthealthpromotion scale: development and psychometric testing. PublicHealth Nurs.2003;20:104---10.
8.HendricksC,MurdaughC,PenderN.TheAdolescentLifestyle Profile:developmentandpsychometriccharacteristics.JNatl BlackNursesAssoc.2006;17:1---5.
9.HendricksD,HendricksC.Therelationshipofhopeand self-efficacytohealthpromotingbehaviorsamongstudent-athletes attendinghistoricallyblackcollegesanduniversities.JMulticult NursHealth.2005;11:23---34.
10.ZeidiI, Hajiagha A, ZeidiB. Reliability and validity of Per-sianversionoftheHealth-PromotingLifestyleProfile.JMUMS. 2012;22:S103---13.
11.WeiC,YonemitsuH,HaradaK,MiyakitaT,OmoriS,Miyabayashi T,etal.AJapaneselanguageversionoftheHealthPromoting LifestyleProfile.JapJHyg.2000;54:597---606.
12.Pérez-FortisA,DíezS,PadillaJ.Psychometricpropertiesofthe Spanishversionofthehealth-promotinglifestyleprofileII.Res NursHealth.2012;35:301---13.
13.PinarR,CelikR,BahcecikN.Reliabilityandconstructvalidity oftheHealth-PromotingLifestyleProfileIIinanadultTurkish population.NursRes.2009;58:184---93.
14.SousaP,GasparP,VazD,SílviaH, DixeM. Health-Promoting LifestyleProfileII:psychometricpropertiesofthePortuguese (European)version.AtenPrimaria.2013;45:S128.
15.MeihanL,Chung-NgokW.Validationofthepsychometric prop-ertiesofthehealth-promotinglifestyleprofileinasampleof Taiwanesewomen.QualLifeRes.2011;20:523---8.
16.MallanKM, Liu WH, MehtaRJ, Daniels LA, Magarey A, Bat-tistuttaD.Maternalreportofyoung children’seating styles. ValidationoftheChildren’sEatingBehaviourQuestionnairein threeethnicallydiverseAustraliansamples.Appetite.2013;64: 48---55.
17.SilvaF,SilvaC,BragaL, NetoA.PortugueseChildren’sSleep HabitsQuestionnaire-validationandcross-culturalcomparison. JPediatr(RioJ).2014;90:78---84.
18.HambletonR.Issues,designsandtechnicalguidelinesfor adapt-ingtestsintomultiplelanguagesand cultures.In:Hambleton R, MerendaP,Spielberger C,editors.Adapting psychological and educational testsfor crosscultural assessment. Mahwah, NJ:LawrenceErlbaum;2005.p.3---39.
19.FergusonE,CoxT.Exploratoryfactoranalysis:auser’sguide. IntJSelectAssess.1993;1:84---94.
20.ShahR,GoldsteinS.Useofstructuralequationmodelingin oper-ationsmanagementresearch:Lookingbackandforward.JOper Manag.2006;24:148---69.
21.BrymanA,CramerD.QuantitativedataanalysiswithSPSSfor Windows.London:Routledge;1997.
22.BeatonD,BombardierC,GuilleminF,FerrazM.
Recommenda-tionsforthecross-culturaladaptationoftheDASH&QuickDASH
Outcome Measures. Institute for Work & Health; Toronto,
Canadá;2007.[cited2014Mar01].Availablefrom:http://www.
dash.iwh.on.ca/system/files/X-CulturalAdaptation-2007.pdf 23.WorldMedicalAssociationWMADeclarationofHelsinki.
Ethi-calprinciplesfor medicalresearchinvolvinghumansubjects. In: 59th WMA General Assembly, Seoul, Korea; 2008. [Cited 2015 Feb 02]. Available from: http://www.wma.net/en/ 30publications/10policies/b3/
24.AmericanPsychological Association.Ethicalprinciplesof psy-chologistsandcodeofconduct.AmPsychol.2010;65:493. 25.HairJ,AndersonR,TathamR,BlackW.MultivariateData
Anal-ysis.7thed.NewJersey:Prentice-Hall;2010.
26.StreinerD,NormanG.Healthandmeasurementscales.A practi-calguidefortheirdevelopmentanduse.4thed.Oxford:Oxford UniversityPress;2008.
27.Biza-Khupe S. An Exploration of New Frontiers in Personal Finance using Structural Equation Modelling (SEM)---Towards ImprovedResearch.ReviewofFinancialandAccountingStudies. 2012;2:17---27.
28.ByrneB. StructuralequationmodelingwithAmos:basic con-cepts,applications,andprogramming.2nded.NewYork,NY: TaylorandFrancisGroup;2010.
29.MarshHW, Martin AJ,Jackson S.Introducinga short version ofthephysicalself-descriptionquestionnaire:newstrategies, short-formevaluativecriteria,andapplicationsoffactor anal-yses.JSportExercPsychol.2010;32:438---82.