EVOLUTI ON OF NURSI NG DI AGNOSES FOR CHI LDREN
W I TH CONGENI TAL HEART DI SEASE
1Viv iane Mar t ins da Silv a2 Thelm a Leit e de Ar auj o3 Mar cos Venícios de Oliv eir a Lopes3
Silva VM, Arauj o TL, Lopes MVO. Evolut ion of nursing diagnoses for children wit h congenit al heart disease. Rev Lat ino- am Enfer m agem 2006 j ulho- agost o; 14( 4) : 561- 8.
We aim ed t o descr ibe t he ev olut ion in nur sing diagnoses for childr en w it h congenit al hear t disease. This longit udinal st udy w as car r ied out fr om July t o Nov em ber of 2004. The sam ple consist ed of 45 childr en int er ned in a public hospit al in For t aleza, Br azil, follow ed dur ing fift een day s. I n t his per iod, w e accom plished six diagnost ic ev aluat ions and found 2 1 nur sing diagnoses. Six of t hese show ed gr eat er oscillat ions in t heir o ccu r r en ce o v er t i m e: I n ef f ect i v e b r ea t h i n g p a t t er n , Act i v i t y i n t o l er a n ce, I n ef f ect i v e a i r w a y cl ea r a n ce, Hypert herm ia, Sleep pat t ern dist urbance, Risk for act ivit y int olerance. Five param et ric m odels were const ruct ed in t he t im e dom ain, w it h a v iew t o pr edict ing t he occur r ence of t he nur sing diagnoses. Know ledge about t he t em por al ev olut ion in indiv iduals’ r esponses can guide nur sing car e t ow ar ds t he client ’s r eal needs.
DESCRI PTORS: hear t defect s, congenit al; nur sing diagnosis; cont inuit y of pat ient car e
EVOLUCI ÓN DE LOS DI AGNÓSTI COS ENFERMEROS
DE NI ÑOS CON CARDI OPATÍ AS CONGÉNI TAS
Se obj et iv ó descr ibir la ev olución de los diagnóst icos enfer m er os en niños por t ador es de car diopat ías con gén it as. Est u dio lon git u din al desar r ollado en los m eses de j u lio a n ov iem br e del 2 0 0 4 . La m u est r a f u e com puest a por 45 niños ingresados en un hospit al de la red pública del m unicipio de Fort aleza, Brasil, acom pañados durant e quince días de int ernam ient o. En el período, llevam os a cabo seis evaluaciones diagnóst icas, encont rando 21 diagnóst icos enfer m er os. Ent r e los diagnóst icos, seis evidenciar on m ayor es oscilaciones en sus t r ayect or ias de ocur r encia en el t iem po: Pat r ón r espir at or io ineficaz, I nt oler ancia a la act iv idad, Lim pieza ineficaz de las vías aéreas, Hipert erm ia, Det erioro del pat rón de sueño y Riesgo de int olerancia a la act ividad. Se const ruyeron cinco m odelos param ét ricos en el dom inio del t iem po, con vist as a predecir la ocurrencia de esos diagnóst icos enfer m er os. Concluim os que el conocim ient o de la ev olución t em por al de las r espuest as del indiv iduo puede dir igir los cuidados de enfer m er ía par a las r eales necesidades del client e.
DESCRI PTORES: car diopat ías congénit as; diagnóst ico de enfer m er ía; cont inuidad de la at ención al pacient e
EVOLUÇÃO DOS DI AGNÓSTI COS DE ENFERMAGEM
DE CRI ANÇAS COM CARDI OPATI AS CONGÊNI TAS
Ob j et i v o u - se d escr ev er a ev o l u ção d o s d i ag n ó st i co s d e en f er m ag em em cr i an ças p o r t ad o r as d e car diopat ias congênit as. Est udo longit udinal desenvolvido nos m eses de j ulho a novem br o de 2004. A am ost r a foi com post a por 45 crianças int ernadas em um hospit al da rede pública do m unicípio de Fort aleza, acom panhadas durant e quinze dias de int ernam ent o. No período efet ivaram - se seis avaliações diagnóst icas. Foram encont rados 21 diagnóst icos de enferm agem . Ent re os diagnóst icos, seis evidenciaram m aiores oscilações em suas t raj et órias de ocor r ência no t em po: Padr ão r espir at ór io ineficaz, I nt oler ância à at iv idade, Desobst r ução ineficaz das v ias aéreas, Hipert erm ia, Padrão de sono pert urbado e Risco para int olerância à at ividade. Foram const ruídos cinco m od elos p ar am ét r icos n o d om ín io d o t em p o, com v ist as a p r ed izer a ocor r ên cia d esses d iag n óst icos d e enfer m agem . Conclui- se que o conhecim ent o da evolução t em por al das r espost as do indivíduo pode dir ecionar os cuidados de enfer m agem par a as r eais necessidades do client e.
DESCRI TORES: car diopat ias congênit as; diagnóst ico de enfer m agem ; cont inuidade da assist ência ao pacient e
1
Art icle ext ract ed from t he m ast er's t hesis, as part of t he Proj ect PAI SC/ CNPQ 50639/ 03- 5; 2 RN, Doct oral St udent in Nursing, CAPES grant holder, e- m ail: vivianem art insdasilva@hot m ail.com ; 3 RN, PhD in Nursing. Facult y, e- m ail: t helm [email protected], e- m ail: m [email protected]. Federal Universit y of Ceará
I NTRODUCTI ON
A
p p r o x i m a t e l y 9 9 % o f i n f a n t s w i t h con gen it al h ear t disease m an if est ch ar act er ist ics ofheart defect s wit hin t he first year of life. A diagnosis
is est ablished w it hin t he fir st w eek of life in 40% of
pat ient s and wit hin one m ont h in 50%( 1). The neonat al
period can be crit ical for pat ient s wit h congenit al heart
d i sease, d u e t o t h e g r av i t y o f co m m o n l y p r esen t
sym pt om s and t o physiological changes fr om fet al t o
n e o n a t a l ci r cu l a t i o n . Co n g e n i t a l h e a r t d i se a se i s
su sp ect ed i n t h e n eo n at al p er i o d w h en f o u r m ai n
clin ical sig n s ar e p r esen t : h ear t m u r m u r, cy an osis,
br eat h lessn ess an d ar r h y t h m ia( 2 ).
N u r s i n g c a r e d e l i v e r y t o c h i l d r e n w i t h
con g en it al h ear t d isease m u st b e est ab lish ed an d
accom p lish ed as soon as a d iag n osis of con g en it al
h ear t d ef ect is su sp ect ed . I n or d er t o d ev elop t h e
c a r e p l a n , a c a r e f u l i n f o r m a t i o n s u r v e y i s
fundam ent al, m ainly direct ed at assessing t he cardiac
f u n c t i o n a n d d e t e c t i n g c h a r a c t e r i s t i c s i g n s a n d
sy m p t om s of com p licat ion s of t h e con g en it al h ear t
d i sease.
Li t e r a t u r e h a s i n d i ca t e d v a r i o u s n u r si n g
d i ag n o ses f o u n d i n ch i l d r en w i t h co n g en i t al h ear t
d i s e a s e w h o a r e h o s p i t a l i z e d i n c l i n i c a l a n d
post surgical recovery unit s: I m balanced nut rit ion: less
t han body requirem ent s, Risk for infect ion, I neffect ive
a i r w a y c l e a r a n c e , I m p a i r e d g a s e x c h a n g e ,
Hypert herm ia, Risk for im balanced body t em perat ure,
Acut e Pain, Delay ed gr ow t h and dev elopm ent , Sleep
p a t t e r n d i s t u r b a n c e , Ri s k f o r c o n s t i p a t i o n a n d
I m p air ed sk in in t eg r it y( 3 - 5 ). Collab or at iv e p r ob lem s
gener ally include pot ent ial com plicat ions: Pneum onia,
H y p o x e m i a a n d A d v e r s e e f f e c t s o f m e d i c a t i o n
t her apy( 6 ). Som e st udies of childr en w it h congenit al
hear t disease assessed a specific aspect of car e for
t his client ele, such as delayed growt h and developm ent
for ex am ple( 7 ).
Mor eov er, l i t er at u r e h i g h l i g h t s st at i st i cal l y
im por t ant associat ions, m ainly bet w een t he follow ing
n u r si n g d i a g n o se s: Hy p e r t h e r m i a a n d I n e f f e ct i v e
airway clearance, I m balanced nut rit ion: less t han body
r equir em ent s and Delay ed gr ow t h and dev elopm ent ,
I n effect iv e br eat h in g pat t er n an d I n effect iv e air w ay
clear ance, and bet w een I neffect iv e br eat hing pat t er n
and Hy per t her m ia( 6 ).
On t he ot her hand, t hese are punct ual st udies
t hat assessed t he diagnost ic profile at one single t im e
du r in g h ospit alizat ion . We h av e n ot f ou n d r esear ch
t hat analyzed t he evolut ion in nur sing diagnoses and
possible changes ov er t im e.
Det ailed and t hor ough clinical dat a analy sis
is needed t o underst and t he healt h- disease processes
t hat are present in a given sit uat ion. And t his analysis
has been a const ant t ask in nursing work( 8). However,
as m ent ioned above, few st udies have analyze nursing
diagnoses in childr en w it h congenit al hear t disease,
and one of t he r easons for t his lack is pr obably t he
n e e d f o r a c o m p l e x c l i n i c a l a n a l y s i s . Mo r e o v e r,
alt hough nursing diagnoses have been used in different
count r ies, nur ses ar e not fam iliar w it h t he diagnost ic
r eason in g pr ocess( 9 ).
Bef o r e d ef i n i n g a r est r i ct ed f r am ew o r k o f
n u r sin g diagn oses in ch ildr en w it h con gen it al h ear t
disease, w e f elt t h e n eed t o dev elop a lon git u din al
s t u d y i n o r d e r t o a n a l y z e t h e e v o l u t i o n i n t h e
diagnost ic pict ure in great er dept h. This w ill allow us
t o offer bet t er direct ions for nursing act ions involving
ch i l d r e n w i t h co n g e n i t a l h e a r t d i se a se , a n d t h e n
cont inue wit h t he ot her st eps of t he nursing process,
t o accom plish effect iv e int er v ent ions t hat ar e based
on scient ific r eflect ion and pr act ice.
I n o u r o p i n i o n , t h i s k i n d o f r e s e a r c h i s
im port ant , as it point s t owards for nursing care needs
relat ed t o a person or group t hat is t he obj ect of care.
The use of it s result s benefit t he client - nurse binom ial,
as it guides nursing care t owards client s’ act ual needs
a n d , t h u s , m a k e s i t e a s i e r t o c h o o s e a d e q u a t e
in t er v en t ion s. By clar if y in g t h e ph en om en a n u r sin g
w or k s w it h , t h ese st u dies of t en in dicat e car e ar eas
t h a t a r e l a ck i n g i n t e r v e n t i o n s. Th u s, w e a i m t o
descr ibe t he t em por al ev olut ion of nur sing diagnoses
for childr en w it h congenit al hear t disease.
MATERI AL AND METHODS
Th e s t u d y d e s i g n i s o b s e r v a t i o n a l a n d
longit udinal. I n obser v at ional st udies, t he r esear cher
assum es a passiv e r ole in obser v ing t he phenom ena
t h at occu r r ed w it h t h e st u dy su bj ect s( 1 0 ). As t o t h e
t em por alit y of t he dat a pr oduct ion pr ocess, w e hav e
decided on a longit udinal st udy, as we want t o obt ain
dat a on a t em por al f ollow - u p scale, w h ich depen ds
on t he st udy obj ect ives. I nit ial t rends and changes in
t he v ar iables of int er est ar e assessed ov er t im e( 11).
The st udy was carried out at a public hospit al
in For t aleza Cear á, w h ich is par t of t h e SER VI
r ef er en ce cen t er f or car d iop u lm on ar y d iseases an d
at t en d s t o p at ien t s f r om all ov er Cear á St at e. Th e
st udy populat ion consist ed of children, wit h a m edical
diagnosis of congenit al hear t disease, hospit alized at
t his specialized inst it ut ion. The sam ple was det erm ined
by applying t he form ula n = [ ( zα+ zβ)
2
. 2 . p( 1 - p) ] /
d2, w h er e n = sam ple size; zα= adopt ed r eliabilit y
coefficient , expressed as st andard deviat ion; zβ= t est
p o w e r ; p = o ccu r r e n ce p r o p o r t i o n o f t h e st u d y
phenom enon; d = difference t o be det ect ed bet w een
pr ior it y nur sing diagnoses and ot her diagnoses( 12).
We adopt ed t he following param et ers: a 95%
reliabilit y coefficient ( zα = 1.96) and an 80% t est power
( zβ = 0 . 8 4 ) . Th e est im at ed pr opor t ion , r epr esen t ed
by t he occurrence proport ion of t he nursing diagnoses,
found in an earlier st udy, corresponded t o 70% ( p =
0 . 7 ) , con sid er in g t h e h ig h est d et ect ed p r ev alen ce
am ong t he nursing diagnoses included in t he diagnosis
list( 3,6). We est ablished a 40% frequency difference in
nur sing diagnoses bet w een childr en w it h and w it hout
priorit y diagnoses ( d = 0.4) . For t his purpose, we used
t he m ean difference bet w een t he prevalence rat es of
t he m ost fr equent diagnoses ( 63. 63% ) and of ot her
diagnoses t hat w er e found ( 26.98% )( 3,6).
Based on t hese par am et er s, w e calculat ed a
sam ple of 41 childr en w it h congenit al hear t disease.
During dat a collect ion, t he st udy sam ple was expanded
t o 4 5 ch i l d r e n w h o w e r e h o sp i t a l i ze d d u r i n g t h e
co l l ect i o n p er i o d an d co m p l i ed w i t h t h e f o l l o w i n g
inclusion crit eria: Up t o 12 m ont hs of age; Confirm ed
m edical diagnosis of acy anot ic or cy anot ic congenit al
heart disease; Not having been subm it t ed t o definit ive
o r p a l l i a t i v e co r r e ct i v e h e a r t su r g e r y ; Pr e v i o u sl y
ob t ain ed accep t an ce b y t h e r esp on sib le p er son t o
part icipat e in t he st udy; Having been adm it t ed at t he
unit for at least 48 hours.
Th ese cr it er ia w er e est ablish ed t o obt ain a
m o r e u n i f o r m p a r t i ci p a n t p r o f i l e a n d a l l o w f o r a
t em poral analysis of t he ident ified nursing diagnoses.
We decided t o w or k w it h childr en in t he fir st y ear of
lif e becau se, at t h e place of st u dy, h ospit alizat ion s
ar e m o st f r eq u en t i n t h i s ag e r an g e. A m i n i m u m
hospit alizat ion per iod of 48 hour s w as det er m ined t o
av oid losses d u r in g t h e d at a collect ion p r ocess, as
ph y sician s decide on w h at clin ical con du ct is t o be
a d o p t e d d u r i n g t h i s p e r i o d . Th e a v e r a g e
hospit alizat ion period for children at t he place of st udy
is approxim at ely 20 days. I n order t o m inim ize losses
d u r in g d at a collect ion , w e est ab lish ed a f ollow - u p
period of 15 days for part icipat ion in our st udy.
The following exclusion crit eria were defined:
sit uat ions t hat det erm ined incom plet e com pliance wit h
st udy inclusion cr it er ia, a child’s ex it fr om t he place
of st udy because of dischar ge, t r ansfer ence or deat h
w it hin less t han 15 day s and follow - up by a per son
w ho w as unable t o pr ov ide all necessar y dat a.
To elaborat e t he dat a collect ion inst r um ent ,
w e car r ied out a bibliogr aphic sur v ey t o ident ify t he
si g n s a n d sy m p t o m s t h a t co n st i t u t e t h e d e f i n i n g
ch ar act er i st i cs an d f act o r s r el at ed t o t h e n u r si n g
d i a g n o se s t h a t m a y b e p r e se n t i n ch i l d r e n w i t h
co n g en i t a l h ea r t d i sea se. Nex t , w e g r o u p ed d a t a
according t o t he eight dom ains present ed by NANDA’s
Tax o n o m y I I( 1 3 ), i n v o l v i n g p h y si cal / p h y si o l o g i cal
hum an responses. These were: Nut rit ion, Elim inat ion,
Act ivit y / Rest , Percept ion / Cognit ion, Coping / St ress
Tolerance, Safet y / Prot ect ion, Com fort and Grow t h /
Dev elopm ent . The r em aining dom ains w er e ex cluded
because t hey are hard t o observe in t he age range of
t he st udy populat ion. I n order t o validat e it s cont ent s
and appearance, t he inst rum ent was present ed t o four
f a cu l t y w h o d o r esea r ch o n n u r si n g d i a g n o ses i n
pat ien t s w it h h ear t diseases, t w o of w h om dir ect ly
work wit h children wit h congenit al heart disease. These
facult y m em ber s’ suggest ions w er e incor por at ed int o
t he inst rum ent , which was t hen applied t o five children
w i t h c o n g e n i t a l h e a r t d i s e a s e . H o w e v e r, a s n o
inadequacies w er e found in t he t est , t he inst r um ent
w as con sider ed appr opr iat e.
D a t a c o l l e c t i o n o c c u r r e d f r o m Ju l y t o
Nov em ber 2 0 0 4 . I n it ially, t h e r esear ch er pr esen t ed
herself t o t he child’s responsible, explained about t he
st udy purpose and request ed aut horizat ion t o include
t he child. Dat a w er e collect ed aft er confident ialit y of
in f or m at ion an d id en t it y h ad b een g u ar an t eed an d
aft er part icipant s signed t he free and inform ed consent
t erm . Once t he child’s part icipat ion had been allowed,
t he r esear cher applied t he dat a collect ion inst r um ent
by m eans of an int er view , aim ed at answ er ing it em s
r elat ed t o in f or m at ion ab ou t t h e m ot h er. Af t er t h e
int erview, t he researcher carried out a careful clinical
n u r s i n g e x a m , b a s e d o n t h e d a t a c o l l e c t i o n
inst r um ent , and consult ed t he r esult s of biochem ical
and r adiological ex am s, as w ell as pr escr ipt ions and
ev olut ions by all healt h t eam m em ber s.
Th e 4 5 c h i l d r e n i n t h e s a m p l e w e r e
accom panied dur ing 15 hospit alizat ion day s, count ed
from t he adm ission dat e. I n t his period, six diagnost ic
ev aluat ions w er e accom plished at 48- hour int er v als,
an d in f er r in g diagn oses an d collabor at iv e pr oblem s
f o l l o w e d t h e s t e p s r e c o m m e n d e d i n s p e c i a l i z e d
lit er at ur e( 1 4 ): collect ion , in t er pr et at ion / gr ou pin g of
i n f o r m a t i o n a n d n a m i n g o f ca t e g o r i e s. We u se d
NANDA’s Taxonom y I I( 13) for nam ing t he diagnoses.
Du r in g diagn ost ic in f er en ce, w e in div idu ally
a s s e s s e d c l i n i c a l h i s t o r i e s . D i a g n o s e s t h a t a l l
r esear ch er s agr eed u pon w er e accept ed. I n case of
disagreem ent , clinical hist ories were reevaluat ed unt il
a co n sen su s w as o b t ai n ed . Par t i cu l ar l y d i ag n o ses
r e l a t e d t o a c t i v i t y t o l e r a n c e p r e s e n t e d p e c u l i a r
charact erist ics in t he st udy sam ple. This capacit y was
assessed b y id en t ify in g ab n or m al h ear t f r eq u en cy,
br eat hing fr equency and ar t er ial pr essur e r esponses
t o t h e ch ild ’s n or m al act iv it ies, sp ecif ically d u r in g
br east feeding or bot t le feeding. Risk for int oler ance
w as considered by t he presence of circulat ory and/ or
r esp ir at or y p r ob lem s t h at ar e ch ar act er ist ic of t h e
basic congenit al disease. I n all ident ified diagnoses,
w e c o n s i d e r e d d i r e c t o b s e r v a t i o n o f s i g n s a n d
sy m pt om s an d h ealt h t eam m em ber s’ r ecor din gs in
t h e p at ien t f iles. I n f or m at ion p r ov id ed b y r elat iv es
and com panions w as alw ay s confir m ed by t hese t w o
m anners in order t o consider t he hum an response as
p r esen t .
Dat a were organized in elect ronic worksheet s
an d st or ed in a * . x ls f ile. Th e t im e ser ies an aly sis
and graphs were developed by m eans of Excel 2003©
sof t w ar e. Absolu t e an d per cen t age f r equ en cies an d
co n f i d e n ce i n t e r v a l s ( 9 5 % ) w e r e co n si d e r e d f o r
descr ipt iv e an aly sis.
We const r uct ed t hr ee disper sion graphs w it h
t h e t em por al dist r ibu t ion of t h e n u r sin g diagn oses.
Du e t o t h e f act t h at m an y d iag n oses ev id en ced a
co n st a n t o ccu r r e n ce p a t t e r n , w e co n si d e r e d t h e
analy sis of a t r end m odel for all t o be unnecessar y.
The six diagnoses w it h t he gr eat est v ar iabilit y w er e
sel ect ed t o d ef i n e a t r en d r eg r essi o n m o d el . Th e
definit ion of t he highest var iabilit y w as based on t he
analy sis of t he disper sion gr aphs const r uct ed for all
d i ag n o ses an d o f t h e est i m at ed v ar i an ce o f t h ei r
proport ions. As children wit h congenit al heart disease
rem ain hospit alized at t he pediat ric unit for a relat ively
sh or t t im e, season al an d cy clical f act or s w er e n ot
t aken int o account for defining t he regression m odels.
D a t a f o r t h e si x sel ect ed d i a g n o ses w er e
plot t ed isolat edly for a m or e pr ecise analy sis, w it h a
v iew t o ob t ain in g a t r en d r eg r ession eq u at ion t h at
w o u l d b e t t e r a d j u st t o t h e d a t a f o r t h e sa k e o f
f or ecast in g. We dev eloped f iv e param et r ical m odels
in t h e t im e d om ain of eq u at ion s f or each select ed
d i a g n o s i s , w i t h t h e r e s p e c t i v e d e t e r m i n a t i o n
coef f i ci en t s ( R2) : l i n ear, secon d or d er p ol y n om i al ,
logarit hm ic, power and exponent ial. The choice of t he
m o s t a d e q u a t e m o d e l c o n s i d e r e d t h e s m a l l e s t
d i s p e r s i o n o f d a t a i n r e l a t i o n t o t h e t r e n d l i n e
( r esidues) , t he highest det er m inat ion coefficient and
Occam ’s r azor, w h ich d et er m in es t h e ch oice of t h e
sim plest m odel t hat answ er s t he quest ion( 15- 16). Aft er
d ef i n i n g t h e m o d el , g r ap h s w er e p l o t t ed w i t h t h e
or ig in al d at a, t h e t r en d lin e, t h e eq u at ion an d t h e
select ed R2 for each diagnosis. The obj ect iv e of t he
t im e ser ies an aly sis w as t o pr odu ce equ at ion s t h at
could for ecast t he pr opor t ion of hospit alized childr en
t hat would develop t he diagnosis over a cert ain period
of t im e. Diagnoses ident ified in m ore t han 80% of t he
childr en dur ing t he fir st assessm ent w er e defined as
h av in g an ear ly st ar t . Ev olu t ion s an d in v olu t ion s of
t h e d i a g n o s e s w e r e b a s e d o n t h e i n c r e a s e a n d
decr ease in t he pr opor t ions of t he diagnoses in each
of t he six assessm ent s.
Th e pr oj ect w as su bm it t ed t o t h e Boar d of
Direct ors of t he inst it ut ion t o obt ain aut horizat ion for
d a t a c o l l e c t i o n , a n d a p p r o v e d b y t h e Et h i c s
Com m it t ee, in com pliance w it h Resolut ion 196/ 96 by
t he Nat ional Healt h Council/ Brazilian Minist ry of Healt h
for r esear ch inv olv ing hum an beings( 17). The per sons
r e sp o n si b l e f o r t h e ch i l d r e n g a v e t h e i r i n f o r m e d
con sen t .
RESULTS AND DI SCUSSI ON
The children’s ages ranged from 9 days unt il
1 1 m on t h s. Mean ag e w as 4 . 7 4 m on t h s ( st an d ar d
deviat ion 3.78 m ont hs) . However, children of up t o 3
m o n t h s o f ag e w er e p r ed o m i n an t ( 4 6 . 7 % ) . As t o
g e n d e r, 6 6 . 7 % o f t h e c h i l d r e n w e r e m a l e , a t a
proport ion of t wo boys for one girl. Most children were
born t hrough norm al birt h ( 59.1% ) , wit h bet ween 38
and 42 w eek s of gest at ional age ( 97.7% ) . We found
no r ecor ds of for ceps deliv er y or post - t er m childr en.
Approxim at ely 68% of t he children obt ained an Apgar
score of nine in t he fift h m inut e. Apgar scores varied
bet ween six and nine. Pat ient s wit h acyanot ic diseases
cor r esponded t o 53.3% of t he t ot al, w it h confidence
int ervals ranging from 37.9% t o 68.3% ; t he frequency
of cy anot ic diseases w as 46. 7% , w it h int er v als fr om
Table 1 - Nur sing diagnoses ident ified in childr en w it h congenit al hear t disease. For t aleza, 2004 s e s o n g a i D g n i s r u N 1 t
s Eval. 2ndEval. 3rdEval. 4thEval. 5thEval. 6thEval.
º
N % Nº % Nº % Nº % Nº % Nº %
e g n a h c x E s a G d e r i a p m I .
1 40 88.9 40 88.9 41 91.1 42 93.3 42 93.3 42 93.3
n r e t t a P g n i h t a e r B e v it c e f f e n I .
2 33 73.3 36 80.0 41 91.1 43 95.6 42 93.3 39 86.7
e c n a r e l o t n I y t i v it c A .
3 33 73.3 36 80.0 38 84.4 38 84.4 40 88.9 40 88.9
n o it c e f n I r o f k s i R .
4 37 82.2 37 82.2 37 82.2 37 82.2 37 82.2 37 82.2
t n e m p o l e v e D d n a h t w o r G d e y a l e D .
5 35 77.8 35 77.8 35 77.8 35 77.8 35 77.8 35 77.8
n o i s u f r e P e u s s i T e v it c e f f e n I .
6 32 71.1 33 73.3 33 73.3 33 73.3 33 73.3 33 73.3
t u p t u O c a i d r a C d e s a e r c e D .
7 28 62.2 29 64.4 29 64.4 30 66.7 29 64.4 29 64.4
e c n a r a e l C y a w r i A e v it c e f f e n I .
8 14 31.1 19 42.2 24 53.3 29 64.4 32 71.1 32 71.1
y t i r g e t n I n i k S d e r i a p m I r o f k s i R .
9 20 44.4 20 44.4 20 44.4 20 44.4 19 42.2 19 42.2
n o it a r i p s A r o f k s i R . 0
1 15 33.3 17 37.8 17 37.8 17 37.8 17 37.8 18 40.0
e m u l o V d i u l F t n e i c if e D . 1
1 10 22.2 10 22.2 10 22.2 10 22.2 9 20.0 9 20.0
h t w o r G e t a n o it r o p o r p s i D r o f k s i R . 2
1 9 20.0 9 20.0 9 20.0 9 20.0 9 20.0 9 20.0
t n e m p o l e v e D d e y a l e D r o f k s i R . 3
1 9 20.0 9 20.0 9 20.0 9 20.0 9 20.0 9 20.0
a i m r e h t r e p y H . 4
1 3 6.7 6 13.3 10 22.2 17 37.8 13 28.9 4 8.9
y t i r g e t n I n i k S d e r i a p m I . 5
1 8 17.8 8 17.8 10 22.2 9 20.0 8 17.8 7 15.6
e c n a b r u t s i D n r e t t a P p e e l S . 6
1 5 11.1 7 15.6 9 20.0 10 22.2 12 26.7 7 15.6
e c n a r e l o t n I y t i v it c A r o f k s i R . 7
1 12 26.7 9 20.0 7 15.6 7 15.6 5 11.1 5 11.1
e n a r b m e M s u o c u M l a r O d e r i a p m I . 8
1 4 8.9 6 13.3 7 15.6 8 17.8 8 17.8 7 15.6
e m u l o V d i u l F t n e i c if e D r o f k s i R . 9
1 1 2.2 1 2.2 1 2.2 1 2.2 1 2.2 1 2.2
a e h r r a i D . 0
2 2 4.4 - - -
-y r u j n I r o f k s i R . 1
2 1 2.2 - - -
-P25 - Percent ile 25; P50 - Percent ile 50; P75 - Percent ile 75
I n t he t ot al of 270 assessm ent s, we found 21
dif f er en t n u r sin g diagn oses f or t h e 4 5 par t icipan t s.
Six of t hese were above t he 75t h percent ile: I m paired
gas ex change ( 91.5% ) , I neffect iv e br eat hing pat t er n
( 8 6 . 7 % ) , Act i v i t y i n t o l e r a n ce ( 8 3 . 3 % ) , Ri sk f o r
infect ion ( 82. 2% ) , Delay ed gr ow t h and dev elopm ent
( 77.8% ) and I neffect ive t issue perfusion ( 73.0% ) . Five
nursing diagnoses appeared bet ween t he 50t h and t he
7 5t h per cen t ile: Decr eased car diac ou t pu t ( 6 4 . 4 % ) ,
I n e f f e c t i v e a i r w a y c l e a r a n c e ( 5 5 . 6 % ) , Ri s k f o r
im pair ed sk in in t egr it y ( 4 3 . 7 % ) , Risk f or aspir at ion
( 3 7 . 4 % ) an d Def icien t f lu id v olu m e ( 2 1 . 5 % ) ( Table
1 ) .
S o m e n u r s i n g d i a g n o s e s w e r e c o n s t a n t
a c r o s s t h e s i x a s s e s s m e n t s : Ri s k f o r i n f e c t i o n ,
D e l a y e d g r o w t h a n d d e v e l o p m e n t , Ri s k f o r
disproport ionat e growt h, Risk for delayed developm ent
an d r i sk f o r d ef i ci en t f l u i d v o l u m e. Ot h er n u r si n g
d i a g n o s e s i n c r e a s i n g l y a p p e a r e d , s p e c i f i c a l l y :
I m pair ed gas ex change, I neffect iv e t issue per fusion,
Act iv it y int oler ance, I neffect iv e air w ay clear ance and
Risk for aspirat ion. On t he ot her hand, som e diagnoses
g r ad u ally d ecr eased : I n ef f ect iv e b r eat h in g p at t er n ,
Hy per t her m ia, I m pair ed sk in int egr it y, Sleep pat t er n
dist ur bance and Risk for act iv it y int oler ance.
Som e h u m an r esp on ses w er e act u ally an d
pot en t ially iden t ified in t h e ch ildr en w it h con gen it al
heart disease: Delayed growt h and developm ent , Risk
f or d i sp r op or t i on at e g r ow t h , an d Ri sk f or d el ay ed
developm ent , Act ivit y int olerance and risk for act ivit y
i n t o l e r a n ce , I m p a i r e d sk i n i n t e g r i t y a n d Ri sk f o r
i m p ai r ed sk i n i n t eg r i t y. Th e n u r si n g d i ag n o ses o f
Diar r h ea an d Risk f or in j u r y on ly ap p ear ed in on e
sin gle assessm en t . I t sh ou ld be h igh ligh t ed t h at all
par t icipant s pr esent ed Act ivit y int oler ance or Risk for
a ct i v i t y i n t o l e r a n ce . Th i s i s d u e t o t h e d i f f e r e n t
h em od y n am ic an d r esp ir at or y alt er at ion s t h at m ay
b e o r a r e p r o d u ce d w h e n m i n i m a l a ct i v i t i e s l i k e
sucking at t he m ot her’s breast are accom plished. Older
infant s can also pr esent char act er ist ics like incr eased
r e s p i r a t o r y d i s c o m f o r t a n d a l t e r a t i o n s i n h e a r t
fr equencies w hile cr y ing, ev acuat ing and play ing.
I n m o st ca se s, t h e o ccu r r e n ce l e v e l s o f
nur sing diagnoses pr esent ed slight changes, t ending
t o w a r d s st a b i l i z a t i o n . D i a g n o se s a b o v e t h e 7 5t h
percent ile appeared in t he early hospit alizat ion phase
and t ended t o st abilize already during t his period. Three
o f t h ese ev i d en ced g r eat er v ar i at i o n s: I n ef f ect i v e
breat hing pat t ern, Act ivit y int olerance and I neffect ive
air w ay clear an ce. Diag n oses b et w een t h e 5 0t h an d
7 5t h p e r ce n t i l e p r e se n t e d l o w e r p r o p o r t i o n s a n d
g en er ally ap p ear ed af t er an d as a con seq u en ce of
t h e f i r st d i a g n o se s o r co l l a b o r a t i v e p r o b l e m s. I n
general, diagnoses bet ween t he 25t h and 50t h percent ile
occurred at a lat er st age, as com plicat ions or possible
co m p l i ca t i o n s o f o t h er d i a g n o ses o r co l l a b o r a t i v e
problem s, and present ed great changes in occurrence
Nex t , w e select ed t h ose n u r sin g d iag n oses
w it h t h e gr eat est v ar iat ion s in occu r r en ce lev els t o
con st r u ct m at h em at ical m odels t h at w ou ld allow u s
t o pr edict w hat pr opor t ion of childr en w it h congenit al
hear t disease w ould dev elop t hese diagnoses dur ing
a t im e int er v al. For t he ot her nur sing diagnoses w it h
a m or e st able pict ur e, ot her par am et er s can be used,
s u c h a s c o n f i d e n c e i n t e r v a l s . T h e s e p r o v i d e
p r o p o r t i o n i n t e r v a l s f o r t h e o ccu r r e n ce o f t h e se
p h en o m en a .
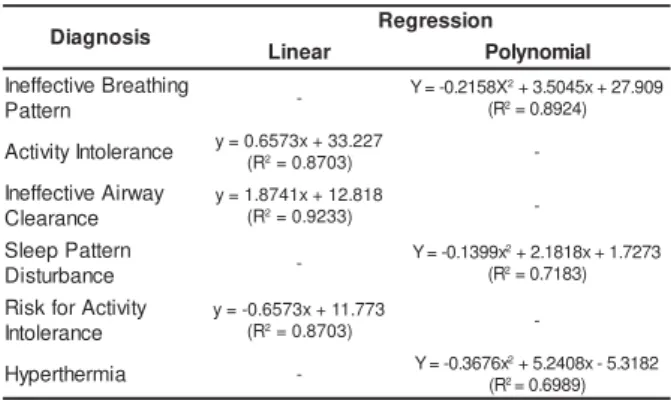
Ta b l e 2 - Eq u a t i o n s t o c a l c u l a t e t r e n d s i n t h e
pr opor t ion of ch ildr en w it h con gen it al h ear t disease
t h at w ill d ev elop cer t ain n u r sin g d iag n oses ov er a
specific per iod of t im e. For t aleza, 2004
s i s o n g a i
D Regression r
a e n i
L Polynomial
g n i h t a e r B e v it c e f f e n I n r e t t a P -X 8 5 1 2 . 0 -=
Y 2+3.5045x+27.909 R
(2=0.8924)
e c n a r e l o t n I y t i v it c
A y=0(R.625=730x.8+70333).227
-y a w r i A e v it c e f f e n I e c n a r a e l C 8 1 8 . 2 1 + x 1 4 7 8 . 1 = y R
( 2=0.9233)
-n r e t t a P p e e l S e c n a b r u t s i D -x 9 9 3 1 . 0 -=
Y 2+2.1818x+1.7273 R
(2=0.7183)
y t i v it c A r o f k s i R e c n a r e l o t n I 3 7 7 . 1 1 + x 3 7 5 6 . 0 -= y R
( 2=0.8703)
-a i m r e h t r e p y
H - Y=-0.3676x
2+5.2408x-5.3182
R ( 2=0.6989)
We con st r u ct ed f iv e param et r ical m odels in
t h e t i m e d o m a i n , w i t h a v i e w t o f o r e ca st i n g t h e
o c c u r r e n c e o f t h e f o l l o w i n g n u r s i n g d i a g n o s e s :
I n ef f ect iv e Br eat h in g Pat t er n , Act iv it y I n t oler an ce,
I n e f f e c t i v e A i r w a y Cl e a r a n c e , S l e e p Pa t t e r n
D i s t u r b a n c e , Ri s k f o r A c t i v i t y I n t o l e r a n c e a n d
Hy p er t h er m ia.
As m ent ioned, we analyzed t he m at hem at ical
eq u at ion s an d select ed t h e m ost ad eq u at e m od els
according t o t he lowest num ber of residues, t he highest
d e t e r m i n a t i o n co e f f i ci e n t a n d Occa m ’s r a zo r. Al l
m o d e l s d e m o n s t r a t e d a s t r o n g d e t e r m i n a t i o n
coefficient for Act iv it y int oler ance, I neffect iv e air w ay
clearance and Risk for act iv it y int olerance. How ev er,
t he linear m odel evidenced a sm all dispersion bet ween
d at a an d t h e t r en d l i n e an d r ev eal ed t o b e easi l y
applicable. Thus, it was considered t he m ost adequat e
m o d e l f o r p r o j e c t i n g t h e d i a g n o s e s . I n e f f e c t i v e
breat hing pat t ern was t he only frequent diagnosis for
w h ich t h e secon d or der poly n om ial m odel r ev ealed
bet t er adj ust m ent t o t he t r endline ( Table 2) .
Alt hough t he polynom ial m odels were select ed
a s t h e m o st a d e q u a t e m o d e l s f o r Sl e e p p a t t e r n
dist ur bance and Hy per t her m ia, t hey pr esent ed w eak
det er m inat ion coefficient s. This r ev eals t he ex ist ence of ot her v ar iables besides t im e in t he occur r ence of t h ese diagn oses.
&C[U 0Q +$2 #+ .KPGCT+# 2QN[PQOKCN24+Figur e 1 - Tem por al analy sis of I neffect ive br eat hing pat t er n ( I BP) and Act iv it y I nt oler ance ( AI ) diagnoses w it h t r endline. For t aleza, 2004
&C[U 0Q +#% &52 .KPGCT+#% 2QN[PQOKCN&52
Fig u r e 2 - Tem p or al an aly sis of I n ef f ect iv e Air w ay Clearance ( I AC) and Sleep Pat t ern Dist urbance ( DSP) diagnoses w it h t r endline. For t aleza, 2004
&C[U 0Q 4#+ *26 .KPGCT4#+ 2QNKPQOKCN*26
Fi g u r e 3 - Te m p o r a l a n a l y si s o f Ri sk f o r Act i v i t y I nt oler ance ( RAI ) and Hy per t her m ia ( HPT) diagnoses
Th e n u r s i n g d i a g n o s e s a b o v e t h e 7 5 t h
per cent ile indicat ed bet t er adj ust m ent bet w een dat a
and t he linear and second order polynom ial t rendline.
The influence of t im e on children who developed t his
diagnoses was 89% for I neffect ive breat hing pat t ern,
93% for Act iv it y int oler ance and 96% for I neffect iv e
air w ay clear ance ( Figur es 1 t o 3) .
Th e t e m p o r a l c u r v e s o f t h e d i a g n o s i s
pr opor t ions r ev eal differ ences t hat , alt hough subt le,
m ust be t aken int o account . The diagnosis of I m paired
g as ex ch an g e ap p ear s ear ly, w it h h ig h p r op or t ion s
and lit t le variat ion over t im e. As opposed t o I neffect ive
br eat hing pat t er n, w hich also appear s ear ly but w it h
l o w e r p r o p o r t i o n s a n d a c u r v i l i n e a r t r e n d , f i r s t
in cr easin g an d t h en d ecr easin g , d at a in d icat e t h at
I neffect ive breat hing pat t ern can be influenced by t he
diagn oses of I m pair ed gas ex ch an ge. How ev er, t h is
is an obscur e r elat ion and ot her v ar iables t han t im e
need t o be analy zed t o confir m t his hy pot hesis.
Act ivit y int olerance w as ident ified as anot her
v er y f r eq u en t d iag n osis in ch ild r en w it h con g en it al
heart disease. This diagnosis also appears early, wit h
l o w e r p r o p o r t i o n s a n d a c u r v i l i n e a r t r e n d , f i r s t
incr easing and t hen st abilizing, indicat ing a possible
i n f l u e n ce o f I m p a i r e d g a s Ex ch a n g e o n Act i v i t y
in t oler an ce.
Th e a d j u s t m e n t o f t h e s e c o n d o r d e r
poly nom ial m odel for Sleep pat t er n dist ur bance and
Hy per t her m ia st ill r ev ealed gr eat disper sion bet w een
dat a and t he t r endline. Besides t im e, appr ox im at ely
3 0 % of ot her v ar iables det er m ine t he pr opor t ion of
childr en w ho w ill m anifest t hese diagnoses.
The lat t er t wo diagnoses present ed a variat ion
wit h a clearly curvilinear t rend, t hat is, t heir proport ions
f i r s t i n c r e a s e d a n d s o o n a f t e r w a r d s d e c r e a s e d ,
form ing a curved t rendline, which j ust ified t he choice
of a m or e com p lex eq u at ion . Diag n oses t h at w er e
not included in t his part of our analysis eit her present ed
a con st an t pr opor t ion or a lin ear pat t er n w it h v er y
slight variat ion. Anot her point t hat m ust be considered
in m ore specific st udies is t he det erm inat ion of fact ors
t hat cont ribut e t o t he est ablishm ent of diagnoses like
Hy per t h er m ia an d Sleep pat t er n dist u r ban ce. Wh en
considering only t he t im e variable, t he adj ust m ent of
t he m odels proposed here for t hese diagnoses rem ains
m od est .
CONCLUSI ONS
S i x n u r s i n g d i a g n o s e s r e v e a l e d g r e a t e r
v ar iat ion ov er t im e: I n ef f ect iv e b r eat h in g p at t er n ,
Act i v i t y i n t o l er an ce, I n ef f ect i v e ai r w ay cl ear an ce,
Hypert herm ia, Sleep pat t ern dist urbance and Risk for
act i v i t y i n t o l er an ce. Fi v e p ar am et r i c m o d el s w er e
co n st r u ct e d i n t h e t i m e d o m a i n , w i t h a v i e w t o
pr edict in g t h e occu r r en ce of t h e n u r sin g diagn oses.
The m ost adequat e m at hem at ical m odels followed t he
st r u ct u r e o f l i n e a r a n d se co n d o r d e r p o l y n o m i a l
eq u at ion s. Th e ad j u st m en t of t h ese eq u at ion s f or
D i s t u r b e d s l e e p p a t t e r n a n d H y p e r t h e r m i a s t i l l
r e v e a l e d g r e a t d i sp e r si o n b e t w e e n d a t a a n d t h e
t r en d lin e. Th is in d icat es t h at , b esid es t im e, ot h er
v ar iables det er m in e t h e pr opor t ion of ch ildr en w h o
w ill m anifest t hese diagnoses.
Al t h o u g h w e h av e co n si d er ed 7 5 % o f t h e
m ean hospit alizat ion t im e for children wit h congenit al
hear t disease, t he dat a analy zed by t he t im e ser ies
m ust be weighed in t erm s of forecast ing t he behavior
o f n u r s i n g d i a g n o s e s f o r c h i l d r e n w h o r e m a i n
hospit alized for a longer per iod.
We b e l i e v e t h a t k n o w l e d g e a b o u t t h e
t em poral evolut ion of children’s responses cont ribut es
t o n u r s i n g i n t e r v e n t i o n s g u i d e d b y d i a g n o s t i c
d e c i s i o n s , w h i c h f a c i l i t a t e s t h e c h o i c e o f m o r e
ad eq u at e act ion s an d allow s f or b et t er p r og n oses.
Nu r sin g act ion s sh ou ld f ocu s on h u m an r esp on ses
relat ed t o hem odynam ic alt erat ions t hat appear at an
early st age and wit h high proport ions, requiring great er
at t ent ion by t he nur sing t eam . These diagnoses also
suggest t hat t he child’s healt h st at e is m or e sev er e.
The im por t ance of nur ses ver ifying vit al signs should
also be em ph asized, as Hy per t h er m ia display s h igh
pr opor t ions aft er six day s of hospit alizat ion.
REFERENCES
1 . Ber n st ein D. O sist em a car diov ascu lar. I n : Beh r m an RE,
Kliegm an RM, Jenson HB. Trat ado de pediat ria. Rio de Janeiro
( RJ) : Guanabar a Koogan; 2 0 0 2 . p. 1 3 1 8 - 4 3 3 .
2 . Am a r a l F, Gr a n zo t t i JA, Ma n so PH, Co n t i LS. Qu a n d o
s u s p e i t a r d e c a r d i o p a t i a c o n g ê n i t a n o r e c é m - n a s c i d o .
Med icin a 2 0 0 2 set em b r o; 3 5 ( 2 ) : 1 9 2 - 7 .
3 . S i l v a V M, Lo p e s MV O, A r a u j o TL. A s o c i a c i ó n e n t r e
d i a g n ó s t i c o s d e e n f e r m e r ía e n n i ñ o s c o n c a r d i o p a t ía s
c o n g é n i t a s . En f Ca r d i o l 2 0 0 4 m a i o d e z e m b r o ; 1 1 ( 3 2
-3 -3 ) : -3 -3 - 7 .
4 . Ru i z RG. La ct a n t e m e n o r p o st o p e r a d o d e co r r e cci ó n
t ot al d e con ex ión an óm ala t ot al d e v en as p u lm on ar es. Rev
Mex En f er m Car d iol 2 0 0 3 ou t u b r o d ezem b r o; 1 1 ( 3 ) : 1 0 7
5 . Gu e r r i e r o A LS, A l m e i d a FA , Gu i m a r ã e s H CQ CP.
D i a g n ó st i co s d e e n f e r m a g e m i n f a n t i l n o p r i m e i r o p ó
s-oper at ór io de cir ur gia car díaca. Act a Paul Enfer m agem 2003
j an eir o- m ar ço; 1 6 ( 1 ) : 1 4 - 2 1 .
6 . S i l v a V M , Lo p e s M V O , A r a u j o TL. D i a g n ó s t i c o s d e
e n f e r m e r ía y p r o b l e m a s c o l a b o r a d o r e s e n n i ñ o s c o n
cardiopat ías congénit as. Rev Mex Enferm Cardiol 2004 m
aio-ag ost o; 1 2 ( 2 ) : 5 0 - 5 .
7 . Ch en CW, Li CY, Wan g JK. Gr ow t h an d d ev elop m en t of
ch ild r en w it h con g en it al h ear t d isease. J Ad v Nu r s 2 0 0 4 ;
4 7 ( 3 ) : 2 6 0 - 9 .
8. Lopes MVO, Silva VM, Arauj o TL. Desenvolvim ent o
lógico-m at elógico-m át ico do soft ware ND. Rev Lat ino- alógico-m Enferlógico-m agelógico-m 2004
j an eir o- f ev er eir o; 1 2 ( 1 ) : 9 2 - 1 0 0 .
9 . Lee T. Nu r sin g diagn oses: f act or s af f ect in g t h eir u se in
char t ing st andar dized car e plans. J Clin Nur s 2005; 14:
640-7 .
10. Hulley SB, Cum m ings SR, Brow ner WS, Grady D, Hearst
N, New m an TB. Delineando a pesquisa clínica: um a abordagem
epidem iológica. Por t o Alegr e ( RS) : Ar t m ed; 2 0 0 3 .
1 1 . Lobion do- Wood G, Haber J. Pesqu isa em en fer m agem :
m ét odos, av aliação cr ít ica e ut ilização. Rio de Janeir o ( RJ) :
Gu an abar a Koogan ; 2 0 0 1 .
12. Jekel JF, Elm ore JG, Kat z DL. Epidem iologia, bioest at íst ica
e m edicina pr ev ent iv a. Por t o Alegr e ( RS) : Ar t m ed; 2002.
13. Nor t h Am er ican Nur sing Diagnosis Associat ion ( Nanda) .
Diag n óst icos d e en f er m ag em . Por t o Aleg r e ( RS) : Ar t m ed ;
2 0 0 2 .
1 4 . Gor don M. Nu r sin g diagn osis: pr ocess an d applicat ion .
St . Lou is: Mosby ; 1 9 9 4 .
15. Levine DM, Berenson ML, St ephan D. Previsão com séries
t em por ais par a dados anuais. I n: Lev ine DM, Ber enson ML,
St eph an D. Est at íst ica: t eor ia e aplicações. Rio de Jan eir o
( RJ) : LTC; 2 0 0 0 . p. 6 2 9 - 7 8 .
1 6 . Mor et t in PA, Toloi CMC. An álise d e sér ies t em p or ais.
São Paulo ( SP) : Edgar d Blücher ; 2004.
17. Conselho Nacional de Saúde ( BR) . Resolução no 196/ 96.
Decr et o no 93. 933 de j aneir o de 1987. Est abelece cr it ér ios
sob r e p esq u isa en v olv en d o ser es h u m an os. Bioét ica 1 9 9 6
j u lh o; 4 ( 2 ) : 1 5 - 2 5 .