www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Incidence
and
endoscopic
characteristics
of
acute
laryngeal
lesions
in
children
undergoing
endotracheal
intubation
夽
Eliandra
da
Silveira
de
Lima
a,∗,
Maíra
Alves
Braga
de
Oliveira
a,
Carolina
Rocha
Barone
a,
Kharina
Mayara
Moreira
Dias
a,
Samanta
Daiana
de
Rossi
a,
Claudia
Schweiger
b,c,
Denise
Manica
b,c,
Larissa
Valency
Enéas
c,
Catia
de
Souza
Saleh
Netto
c,
Gabriel
Kuhl
a,b,
Paulo
Roberto
Antonacci
Carvalho
c,d,
Paulo
Jose
Cauduro
Marostica
c,eaUniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
bHospitaldeClínicasdePortoAlegre(HCPA),DepartamentodeOtorrinolaringologia,PortoAlegre,RS,Brazil
cUniversidadeFederaldoRioGrandedoSul(UFRGS),ProgramadePósGraduac¸ãoemSaúdedaCrianc¸aedoAdolescente,
PortoAlegre,RS,Brazil
dHospitaldeClínicasdePortoAlegre(HCPA),UnidadedeTerapiaIntensivaPediátrica,PortoAlegre,RS,Brazil eHospitaldeClínicasdePortoAlegre(HCPA),UnidadedePneumologiaPediátrica,PortoAlegre,RS,Brazil
Received1July2015;accepted1September2015 Availableonline7January2016
KEYWORDS Intubation; Laryngealdiseases; Laryngoscopy; Artificialrespiration
Abstract
Introduction:Acute laryngeal lesions after intubation appear to be precursors of chronic lesions.
Objective: Todescribetheincidenceandtypeofacutelaryngeallesionsafterextubationina pediatricintensivecareunit(PICU).
Methods:Acohortstudyinvolvingchildrenfrombirthto<5years,submittedtointubationfor morethan24hinthePICUofanuniversityhospital.Inthefirsteighthoursafterextubation, aflexiblefiberopticlaryngoscopy(FFL)wasperformedatthebedside.Thosewithmoderateto severeabnormalitiesunderwentasecondexaminationseventotendayslater.
Results:177patientswereincluded,withamedianageof2.46months.Themeanintubation timewas8.19days.Seventy-three(41.2%)patientshadmoderateorseverealterationsatthe FFL, withtheremainingshowing onlyminoralterationsornormalresults.Duringfollow-up, 16childrenfromthegroupwithmoderatetoseverelesionsdevelopedsubglotticstenosis.One patientfromthenormalFFLgrouphadsubglotticstenosis,resultinginanincidenceof9.6%of chroniclesions.
夽 Pleasecitethisarticleas:deLimaES,deOliveiraMA,BaroneCR,DiasKM,deRossiSD,SchweigerC,etal.Incidenceandendoscopic
characteristicsofacutelaryngeallesionsinchildrenundergoingendotrachealintubation.BrazJOtorhinolaryngol.2016;82:507---11.
∗Correspondingauthor.
E-mail:[email protected](E.S.deLima).
http://dx.doi.org/10.1016/j.bjorl.2015.09.012
1808-8694/©2015Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen
Conclusion:Mostchildreninthestudydevelopedmildacutelaryngeallesionscausedby endo-trachealintubation,whichimprovedinafewdaysafterextubation.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Intubac¸ão;
Doenc¸asdalaringe; Laringoscopia; Respirac¸ãoartificial
Incidênciaecaracterísticasendoscópicasdelesõesagudaslaríngeasemcrianc¸as submetidasàintubac¸ãoendotraqueal
Resumo
Introduc¸ão:Aslesõeslaríngeasagudasapósaintubac¸ãoparecem serprecursorasdaslesões crônicas.
Objetivo:Descreveraincidênciaeotipodelesõeslaríngeasagudasapósextubac¸ãoemUnidade deTerapiaIntensivaPediátrica(UTIP).
Método: Estudodecoorteenvolvendocrianc¸asde0a5anosincompletos,comintubac¸ãopor maisde24horasnaUTIPdeumhospitaluniversitário.Nasprimeiras8horasapósextubac¸ão, umanasofibrolaringoscopiaàbeiradoleitofoirealizada.Aquelescomanormalidades moder-adasagravesforamsubmetidosanovoexameentre7---10diasapós.
Resultados: 177pacientesforamincluídos,comidademedianade2,46meses.Otempomédio deintubac¸ãofoide8,19dias.Setentaetrês(41,2%)pacientesapresentaramalterac¸ões moder-adasougravesàlaringoscopia,orestantemostrandoapenasalterac¸õeslevesouexamenormal. Durante oacompanhamento,16 crianc¸as dogrupo lesõesmoderadaagrave desenvolveram estenose subglótica. Um paciente do grupo laringoscopia normal teve estenose subglótica, somando-seumaincidênciade9,6%delesõescrônicas.
Conclusão:Amaioriadascrianc¸asdoestudodesenvolveulesõeslaríngeasagudasleves decor-rentesdaintubac¸ãoendotraqueal,commelhoraemalgunsdiasapósaextubac¸ão.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Itisestimatedthatoneinthreepatientsadmittedtoa pedi-atric intensive care unit (PICU) will require endotracheal intubationforanaverageoffivedays.1
Theendotrachealtubeexertspressureonthemucosaof theposterior aspect of the larynx; theresulting ischemia seemstobethestartingpointforthedevelopmentof post-intubationacutelaryngeallesions.Thelesionsoccuratthe pointsofgreatestcontactwiththetube:medialsurfaceof the arytenoid cartilage, medial portion of cricoarytenoid joint and vocal process, posterior glottis in the interary-tenoidregion,andsubglottisinvolvingtheinnersurfaceof thecricoidcartilage,usuallytheposteriorportion.2-4
There are several classifications for acute lesions sec-ondary to intubation. According to Lindholm, the lesions canbeclassifiedfromgradesItoIV,dependingonseverity.5
AccordingtoBenjamin,acutelaryngeallesionsaredivided into five groups: early nonspecific alterations, edema, granulation tissue, ulceration, and miscellaneous.3 Fan
et al. classified the findings as normal or mild (interary-tenoidregionulceration,vocalfoldgranuloma),moderate (pseudomembranes,bulky granulomas) and severe lesions (subglotticstenosis, subglotticmembrane,tracheal steno-sis,vocalfoldparalysis).6Coliceetal.classifiedthefindings
asnormal, mild (erythema or mucosal ulceration without
lumen size reduction during inspiration), moderate (ery-thema,ulceration,andmucosaledema,reducinglaryngeal lumen during inspiration) and severe lesions (erythema, ulceration, and mucosal edema reducing laryngeal lumen by morethan50% duringinspiration).7 This lackof
homo-geneityinclassificationsmakesitdifficult tocomparethe studies.
Theincidenceofsubglotticstenosis(SGS)inthePICUof theuniversityhospitalwherethisstudywasperformedwas estimated at 11.3%.8 Due tothe fact that severe chronic
lesionsgenerallyresultfromtheevolutionofacutelesions,9
itisofutmostimportancetoknowtheepidemiologyofthe latter,inordertogeneratedataforthepreventionofsevere laryngeallesions.
Therefore,thisstudyaimedtodescribetheincidenceand typeofacutelaryngeallesionsafterextubationinthePICU.
Methods
history ofendotracheal intubation, presence or historyof tracheotomy,andpatientsconsideredtobecriticallyillby thecareteam.
Inthefirsteighthoursafterextubationaflexible fiberop-ticlaryngoscopy(FFL)wasperformedinthePICUwiththe patientinbedandwithoutsedation.Thefiberoptic laryngo-scopewasintroducedonlytothesupraglotticregion,aiming toobtainimagesofthesupraglottic,glottic,andsubglottic regions.Theglotticlevelwasnotsurpassedinanypatient, to avoid triggering a laryngospasm. The recorded movies wereevaluatedbya researcher(GK)blindedtotheother patients’dataandexperiencedinFFL.
ThedefinitionsusedtoclassifylesionsbyFNLafter extu-bationwere:hyperemia---classifiedasmildwhenaffecting up to one-third of the structure, moderate when affect-ingmore thantwo-thirds, andintensewhen affecting the entire structure; edema --- classified asmild when affect-inguptoone-thirdofthestructure,moderatewhenmore than two-thirds were affected, and intense when affect-ingtheentirestructure;vocal foldbleeding;immobility ---definedastheabsenceofhemilarynxmovement and clas-sifiedaccordingtothelaterality(right,left,andbilateral); ulceration--- discontinuityofthemucosathatoverlays the larynx;andgranulation---emergenceofabnormaltissueof granulomatous appearance. Both ulcerationsand granula-tionswereclassifiedaccordingtolocation:ifintheglottis, asunilateral(whenaffectingonevocal processofthe ary-tenoid), bilateral (whenaffecting both vocal processesof thearytenoid),orinterarytenoid(whenoccupyingthe pos-teriorwallbetweenthevocalprocesses);ifinthesubglottic region, as partial (less than 360◦ of the lumen) or total
(affecting360◦ofthelumen).Furthermore,thepresenceof
obstructive(ifitpreventedthevisualizationoftheglottis) ornon-obstructivelaryngomalaciawasalsodescribed.
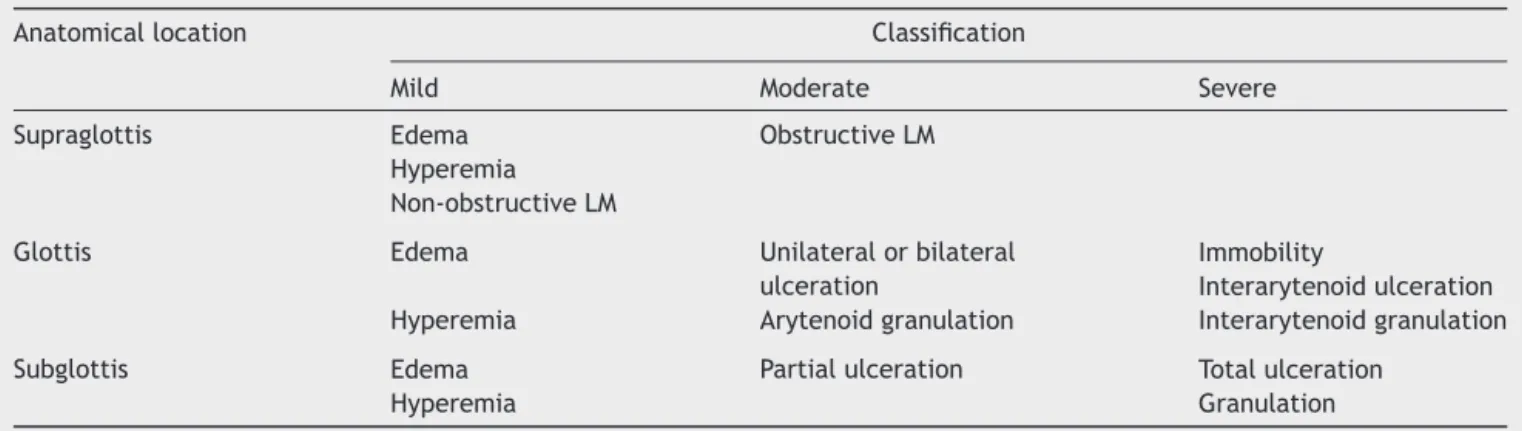
Therefore, the lesions classified as mild alterations included: hyperemia, edema, vocal foldhemorrhage, and non-obstructive laryngomalacia; as moderate: obstructive laryngomalacia, unilateral or bilateral glottal ulceration, arytenoid granulation, and partial subglottic ulceration; andassevere:vocalfoldimmobility,interarytenoid ulcera-tion,interarytenoidgranulation,totalsubglotticulceration, and subglottic granulation (Table 1). Laryngomalacia was includedasacutelaryngeallesionbecause,ifobstructive, it would not allow the visualization of the glottic and
Figure1 Flexible fiberopticlaryngoscopy after extubation: normalsubglottis;mildposteriorglotticedema.
subglotticstructures.Hence,thesepatientswerefollowed as possible cases of acute laryngeal lesion, and their endoscopywasrepeatedbetweensevenandtendaysafter thefirstassessment,asexplainedsubsequently.
DuringtheperiodwhentheyremainedinthePICU,the childrenweremonitoreddailybytheresearchers,collecting datasuchasmobilizationofendotrachealtubebythe assis-tantstaff, numberof reintubations, need for an increase inbasaldoseofsedation,oruseofextradosesofsedation, whicharetheadditionaldosesofsedationinadditiontothat regularlyprescribed.
Patientswithnormalresultsorslightalterations(Fig.1) had a follow up consultation in the Pediatric Laryngol-ogyOutpatient Clinicof the Hospital Otorhinolaryngology Service one month after discharge. Those who remained laryngologicallyasymptomatic(absenceofstridor, laryngi-tis,dysphonia,or swallowingdisorders)were followed by monthlytelephonecontactaftertheoutpatientassessment, uptoatotalof12months.Otherwise,theyunderwent air-wayendoscopyundergeneralanesthesia.
Patients with moderate to severe alterations (Fig. 2) underwentFFLasecondtimebetweensevenandtendays afterextubation.When thatexamination revealednormal
Table1 ClassificationofFFLfindingsasmild,moderate,orsevere,accordingtotheanatomicallocation. Anatomicallocation Classification
Mild Moderate Severe Supraglottis Edema ObstructiveLM
Hyperemia Non-obstructiveLM
Glottis Edema Unilateralorbilateral ulceration
Immobility
Interarytenoidulceration Hyperemia Arytenoidgranulation Interarytenoidgranulation Subglottis Edema Partialulceration Totalulceration
Hyperemia Granulation
Figure2 Flexible fiberoptic laryngoscopyafter extubation: extensiveanteriorsubglotticgranulation.
results,thepatientswerefollowedinthesamewayasthe patients with early findings classified as normal or mild. Whenlesionswereidentifiedinthissecondexamination,the patientswerereferredforairwayendoscopyundergeneral anesthesia.
ThisstudywasapprovedbytheResearchEthics Commit-tee of the hospital under No. 05-266 and the parents or legalguardianssigned an informedconsentprior tostudy enrollment.
Thevariablesareshownasproportionsaccordingtothe assessedcategories.
Results
There were 177 patients included, with a median age of 2.46months, ofwhom 59.9%were males.The most com-monlyusedrouteofintubationwastheorotrachealroute, whereasthenasotrachealintubationwasperformedinonly one patient.An endotracheal tube with cuff wasused in 19.4%ofpatients.Themeanintubationtimewas8.19days. Thecausesofintubationwerebronchiolitis(63.3%), pneu-monia (13.6%), meningitis (5.6%), respiratory dysfunction (5.1%),asthma(2.3%),andotherdiagnoses(10.2%).
The FFL performed immediately after the extubation showed that 104 (58.8%) patients had normal results or onlymildalterations,whereas73(41.2%)patientshad mod-erate or severe alterations in addition to possible minor ones.Overall,themostfrequentlyfoundmildalterationwas edema,ofsupraglotticlocationin138 patients(78%), fol-lowedby posterior glotticedema in 127 patients(72.2%), vocalfoldedemain85patients(48%),andsubglotticedema in48patients(27.8%).Hyperemiawasthesecondmost com-monmild alteration,found in the supraglotticlocationin 122patients(69%),in theposteriorglottisin 106patients (59.8%),andinthesubglotticregionin76patients(43.7%). Otheracutealterationswerenon-obstructive laryngomala-cia(22%)andvocalfoldbleeding(5.1%).
Themostcommonmoderatealterationswerearytenoid granulationin36patients(20.5%)andunilateralorbilateral glottalulceration in 29 patients (16.6%). Other moderate
changeswereobstructivelaryngomalacia(1.7%)andpartial subglotticulceration(1.7%).
Themostfrequentseverealterationwassubglottic gran-ulation, identified in 36 patients (21%). The other severe alterationswerecompletesubglotticulceration(4%), inter-arytenoidgranulation (3.4%),vocalfoldimmobility(1.7%), andinterarytenoidulceration(0.6%).
Itwasnotpossible tovisualize thesubglottic regionin ninepatients,duetothepresenceofglotticgranulationin seven casesanddue toobstructivelaryngomalacia intwo cases. These patients underwent a new assessment after seventotendays.Atthenewassessment,onlyonepatient with glottic granulation developed subglottic stenosis. In thiscase,thepatientunderwentlaryngoscopyunder seda-tion.
Duringthefollow-upafterextubation,16patientsinthe groupwithmoderateor severealterationsdeveloped sub-glotticstenosis. OnlyonepatientwithnormalFFLorwith mild alterationdevelopedsubglottic stenosis,withatotal incidenceofchroniclesionsof9.6%.
Discussion
In the study by Smith et al., with data obtained from a PICUbetweenDecemberof2005andNovemberof2006in patientsfromthepresentlineofresearch,theoverall preva-lenceofalterationsin theFFLinchildrenpost-extubation was92.68%;ofthistotal,51.22%weremildlesions;14.63% wereclassifiedasmoderate,and26.83%assevere.Themost frequent moderate to severe lesions were posterior glot-ticgranulation,subglotticgranulation,andposteriorglottic ulceration.10Attheanalysisperformedinthepresentstudy,
withdatacollectedduringsevenyears,thepercentageof lesionsandthedegreeofseverityweresimilartotheresults obtainedbySmithetal.
IntheprospectivestudybyCordeiroetal.,carriedout in patients fromthe neonatalICU and PICU ofthe Hospi-tal daUniversidade de São Paulo, the overall prevalence ofpost-intubationlaryngeal lesionsin childrenwas89.9%. Ofthistotal,themildlesionsaccountedfor54.8%; moder-atefor24.2%;andsevere, for10.7%.The mostfrequently found moderatelesionwasvocal foldedema,followed by ulceration.The mostfrequentlyfoundsevere lesionswere fibrousnodulesonthevocalfold,followedbysynechias.11
Theinclusionofnewbornsinthestudyandtheuseofanother lesionclassificationmayexplainthedifferentresults com-paredtothisstudy,especiallyfortheseverelesions.
Post-intubationlaryngeal lesionsaremostlytemporary. However,whenpresent,theysignificantlyimpactpatients’ health and quality of life and may prolong hospitaliza-tion. When located in the anteriorportion of the glottis, the main presenting symptom is dysphonia or hoarse cry. The lesionslocated in theposterior glottic andsubglottic regions feature stridorand respiratory dysfunctionas the mainsymptoms.Somelesionssuchasgranulomascanalso causeforeignbodysensation,cough,clearingofthethroat, andlaryngealpain.3,12 Additionally,acutelaryngeallesions
Conclusion
This study shows that most children have acute lesions resultingfromendotrachealintubation, butmostof these lesions are mild and improve within a few days after extubation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.FariasJA,MonteverdeE.Weneedtopredictextubationfailure. JPediatr(RioJ).2006;82:322---4.
2.MartinsRHG,DiasNH,BrazJRC,CastilhoEC.Complicac¸õesdas viasaéreas relacionadas àintubac¸ão endotraqueal.RevBras Otorrinolaringol.2004;70:671---7.
3.BenjaminB.Prolongedintubationinjuriesofthelarynx: endo-scopicdiagnosis,classificationanttreatment.AnnOtolRhinol LaryngolSuppl.1993;160:1---15.
4.BishopMJ.Mechanismsoflaryngotrachealinjuryfollowing pro-longedtrachealintubation.Chest.1989;96:185---6.
5.LindholmCE.Prolongedendotrachealintubation.Acta Anaes-thesiolScandSuppl.1970;33:1---131.
6.Fan LL, Flynn JW, Pathak DR. Risk factors predicting laryn-geal injury in intubated neonates. Crit Care Med. 1983;11: 431---3.
7.ColiceGL,StukelTA,DainB.Laryngealcomplicationsof pro-longedintubation.Chest.1989;96:877---84.
8.ManicaD,SchweigerC,CauduroMarosticaPJ,KuhlG,Antonacci CarvalhoPR.Associationbetweenlengthofintubationand sub-glotticstenosisinchildren.Laryngoscope.2013;123:1049---54.
9.SchweigerC,MarosticaPJ,SmithMM,ManicaD,CarvalhoPR, KuhlG.JLaryngolOtol.2013;127:399---403.
10.Smith MM,KuhlG, CarvalhoPR, MarosticaPJ.Flexible fiber-optic laryngoscopy in the first hours after extubation for the evaluation of laryngeal lesions dueto intubation inthe pediatric intensive care unit.IntJPediatr Otorhinolaryngol. 2007;71:1423---8.
11.Cordeiro AM, Shin SH, Fernandes IC, Bousso A, Troster EJ. Incidência ecaracterísticas endoscópicas de lesões das vias aéreasassociadasàintubac¸ãotraquealemcrianc¸as.RevAssoc MedBras.2004;50:87---92.