SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Comparative
evaluation
of
the
results
of
three
techniques
in
the
reconstruction
of
the
anterior
cruciate
ligament,
with
a
minimum
follow-up
of
two
years
夽
Ricardo
de
Paula
Leite
Cury,
Jan
Willem
Cerf
Sprey,
André
Luiz
Lima
Bragatto,
Marcelo
Valentim
Mansano,
Herman
Fabian
Moscovici,
Luiz
Gabriel
Betoni
Guglielmetti
∗FaculdadedeCiênciasMédicasdaSantaCasadeMisericórdiadeSãoPaulo,DepartamentodeOrtopediaeTraumatologia,Grupode CirurgiadeJoelho,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received23December2015 Accepted12April2016 Availableonline10May2017
Keywords:
Anteriorcruciateligament/injuries Anteriorcruciateligament reconstruction
Knee
Orthopedicprocedures
a
b
s
t
r
a
c
t
Objective:Tocomparetheclinicalresultsofthereconstructionoftheanteriorcruciate liga-mentbytranstibial,transportal,andoutside-intechniques.
Methods:Thiswasaretrospectivestudyon90patients(ACLreconstructionwithautologous flexortendons)operatedbetweenAugust2009andJune2012,bythemedialtransportal(30), transtibial(30),and“outside-in”(30)techniques.Thefollowingparameterswereassessed: objective andsubjectiveIKDC,Lysholm, KT1000,Lachmantest,Pivot-Shiftandanterior drawertest.
Results:Onphysicalexamination,theLachmantestandPivot-Shiftindicatedaslight superi-orityoftheoutside-intechnique,butwithoutstatisticalsignificance(p=0.132andp=0.186 respectively).Theanteriordrawer,KT1000,subjectiveIKDC,Lysholm,andobjectiveIKDC testsshowedsimilarresultsinthegroupsstudied.Ahighernumberofcomplicationswere observedinthemedialtransportaltechnique(p=0.033).
Conclusion: There were no statistically significant differences in the clinical results of patientsundergoingreconstructionoftheanteriorcruciateligamentbytranstibial,medial transportal,andoutside-intechniques.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheFaculdadedeCiênciasMédicasdaSantaCasadeMisericórdiadeSãoPaulo,DepartamentodeOrtopediae Traumatologia,GrupodeCirurgiadeJoelho,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.G.Guglielmetti).
http://dx.doi.org/10.1016/j.rboe.2017.05.003
Avaliac¸ão
comparativa
dos
resultados
de
três
técnicas
na
reconstruc¸ão
do
ligamento
cruzado
anterior
com
seguimento
mínimo
de
dois
anos
Palavras-chave: Ligamentocruzado anterior/lesões
Reconstruc¸ãodoligamento cruzadoanterior
Joelho
Procedimentosortopédicos
r
e
s
u
m
o
Objetivo: Compararosresultadosclínicosobjetivosesubjetivosdareconstruc¸ãodo liga-mentocruzadoanterior(LCA)pelastécnicastranstibial,transportale“deforaparadentro”. Métodos:Estudoretrospectivode90pacientesoperadosentreagostode2009ejunhode2012, parareconstruc¸ãodoLCApelastécnicastransportalmedial(30),transtibial(30)e“defora paradentro”(30).OspacientesforamavaliadospormeiodoInternationalKneeDocumentation Committee(IKDC)objetivoesubjetivo,escoreLysholmetestesKT1000,deLachman, Pivot-Shiftegavetaanterior.
Resultados: Emrelac¸ãoaoexamefísico,nostestesdeLachmanePivot-Shift encontrou-seumadiscretasuperioridadedatécnica“deforaparadentro”,porémsemsignificância estatística(p=0,132ep=0,186respectivamente).Gavetaanterior,KT1000,IKDCsubjetivo, LysholmeIKDCobjetivoapresentaramresultadossemelhantesnosgruposavaliados.Um maiornúmerodecomplicac¸õesfoirelatadonatécnicatransportal(p=0,033).
Conclusão: Resultados clínicos objetivos e subjetivos sem significância estatística na comparac¸ãodastrêstécnicasdereconstruc¸ãodoLCA.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Reconstructionoftheanteriorcruciateligament(ACL)isone of the most common orthopedic surgeries. The results of thisprocedurehavebeenwelldocumentedinseveralstudies asgood-to-excellentin85%–95%ofpatients.1 Nevertheless, someissuesregardingtheplacementoftunnelscontinueto bediscussedandstudied.2
Thefemoral tunnelcan be made witha guide through thetibialtunnel, orapoint closertotheorigin oftheACL could be reached, which is therefore more similar to the originalanatomy(“outside-in”orthroughthemedialportal). Inthe last twodecades,the mostusedmethod worldwide wasthetranstibial.3Anatomicalstudieshaveshownthatthe positioning ofthe tunnelthrough this technique isnot at the centerofthe ACL origin2,4;other biomechanical2,5 and clinical6,7 studies showadvantages regardingachieved sta-bility with a more anatomical positioning of the femoral tunnel.
Therearesomeadvantagestoeachtechnique.Amongthe advantagesofthetranstibialtechnique,itcanbementioned thatnolateralincisionisrequiredinthedistalthigh,an iso-metricpositionisobtained,andthefemoraltunnelisinthe sameorientationasthe tibialtunnel. Thetransportal tech-niqueachievesananatomical femoraltunnel, independent tunnels,non-divergenceintheplacementofthefemoral inter-ferencescrew,andbetterrotationalstability.Theadvantages oftheoutside-intechniqueincludetheanatomical position-ingofthefemoraltunnel,betterrotationalstability, norisk ofposteriorwallrupture,andlessdivergenceofthetunnels whencomparedthetransportaltechnique.8
Thisstudyaimedtocomparetheobjectiveandsubjective clinical resultsoftheACL reconstructionby thetranstibial technique and by the transportal and outside-in anatomi-caltechniqueswiththeuseofautologousflexortendonsas
agraft.Itwashypothesizedthattheanatomicaltechniques wouldgeneratebetterresultsintheevaluatedcriteria.
Patients
and
methods
FromAugust2009toJune2012,170patients(knees)underwent ACLreconstructionbythesamesurgeon.Ofthese,119metthe inclusioncriteriaofthestudy:unilateralACLinjury;skeletally mature;noprevioussurgeriesontheaffectedside(exceptfor arthroscopicmeniscectomy);absenceofdiffusedegenerative alterations(arthrosis);absenceofassociatedligamentinjuries (exceptmedialcollateralligamentgradesIandII);andabsence ofmorbidobesity.ACL re-ruptureatanypointinthe study wasanexclusioncriterion,becausetheobjectivewasto com-parethestabilityofthekneeswithintactACL.Re-ruptures weredefinedasnewkneesprainassociatedwithclinical insta-bility.Ofthe119patients,45wereunderwentthetranstibial technique(between2009and2010),35transportal(between 2010and2011),and39outside-in(between2011and2012). FivepatientswereexcludedduetoACLre-rupture,twofrom thetranstibialgroup,twofromthetransportalgroup,andone fromtheoutside-ingroup.
Patientswereretrospectivelyselectedandrandomlycalled up for clinical evaluation: all patients who had undergone each techniquewerelisted;then,asequenceofpatientsto be contactedwas elaborated, and bydrawing lots patients werecalleduntil30memberswereallottedintoeachgroup:I –transtibial;II–transportal;andIII–outside-intechnique.
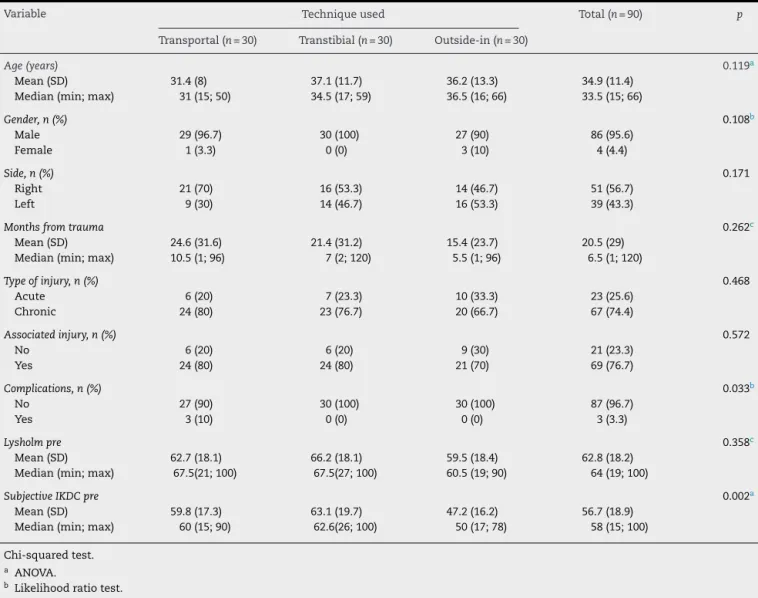
Table1–Descriptionofpersonalcharacteristicsanddiagnosticscalesbeforesurgeryaccordingtothereconstruction techniqueandresultofstatisticaltests.
Variable Techniqueused Total(n=90) p
Transportal(n=30) Transtibial(n=30) Outside-in(n=30)
Age(years) 0.119a
Mean(SD) 31.4(8) 37.1(11.7) 36.2(13.3) 34.9(11.4)
Median(min;max) 31(15;50) 34.5(17;59) 36.5(16;66) 33.5(15;66)
Gender,n(%) 0.108b
Male 29(96.7) 30(100) 27(90) 86(95.6)
Female 1(3.3) 0(0) 3(10) 4(4.4)
Side,n(%) 0.171
Right 21(70) 16(53.3) 14(46.7) 51(56.7)
Left 9(30) 14(46.7) 16(53.3) 39(43.3)
Monthsfromtrauma 0.262c
Mean(SD) 24.6(31.6) 21.4(31.2) 15.4(23.7) 20.5(29) Median(min;max) 10.5(1;96) 7(2;120) 5.5(1;96) 6.5(1;120)
Typeofinjury,n(%) 0.468
Acute 6(20) 7(23.3) 10(33.3) 23(25.6)
Chronic 24(80) 23(76.7) 20(66.7) 67(74.4)
Associatedinjury,n(%) 0.572
No 6(20) 6(20) 9(30) 21(23.3)
Yes 24(80) 24(80) 21(70) 69(76.7)
Complications,n(%) 0.033b
No 27(90) 30(100) 30(100) 87(96.7)
Yes 3(10) 0(0) 0(0) 3(3.3)
Lysholmpre 0.358c
Mean(SD) 62.7(18.1) 66.2(18.1) 59.5(18.4) 62.8(18.2) Median(min;max) 67.5(21;100) 67.5(27;100) 60.5(19;90) 64(19;100)
SubjectiveIKDCpre 0.002a
Mean(SD) 59.8(17.3) 63.1(19.7) 47.2(16.2) 56.7(18.9) Median(min;max) 60(15;90) 62.6(26;100) 50(17;78) 58(15;100)
Chi-squaredtest.
a ANOVA.
b Likelihoodratiotest. c Kruskal–Wallistest.
same surgeon, who also performed all the surgeries. The postoperativeevaluationwasconductedbyphysicianswho werenotpresentatthetimeofsurgery,internsoftheknee surgery group. TheKT1000TM assessment was not applied preoperativelyduetooperationalissues.
Atotalof90patientswerereassessed,86malesandfour females.Therewereatotalof51rightand39leftknees.The meanagewas34.9years.Allofthe90patientspracticedsome physicalactivity beforethe injury.ThesubjectiveIKDCand thepreoperativemeanLysholmscoreswere56.70(14.9–100) and 62.80(15–100), respectively. Only25.6%ofthe patients presentedacuteinjuries(lessthanthreemonths);74.4%had chronic injuries(more than three monthsof trauma). The patients were separated into three groups, in relation to thesurgicaltechnique:transtibialgroup,trans-medialportal group,andoutside-ingroup.Table1showsthatpreoperative personaland clinicalcharacteristics didnotdiffer between groups(p>0.05); onlythe subjectiveIKDC showeda statis-ticallysignificant mean difference betweenthe techniques (p=0.002).Patientsintheoutside-ingrouphadalowermean subjectiveIKDCthanthepatientsintheothergroups. There-fore,thegroupswerepreoperativelyhomogenousingeneral.
Regardingthesurgicaltechnique,arthroscopy,treatmentof possiblemeniscalandchondrallesions,andACL reconstruc-tion wereperformed, withfixationofasemitendinousand gracileflexortendongraft(harvestedbythesurgeonhimself, alwaysusingthesametechnique).
In thetranstibial technique,the tibialtunnelwas made withthekneeinextensionandusinganextensionguide(65 Howell Guide®;BiometSportsMedicineInc.,Warsaw,Ind.). Subsequently, a conventional transtibial guide (aimer) was placed in the posterior margin ofthe intercondyle. Before passingtheguidewire(Kirschner2.4),theaimerwasrotated distallytoreachamorehorizontalposition.Atthatmoment, thefemoraltunnelwasdrilled;thegraftwasthenpassedand fixatedwithanEndobutton®(Smith&Nephew,Andover,MA, UnitedStates)inthefemurandwithametallicinterference screwinthetibia.
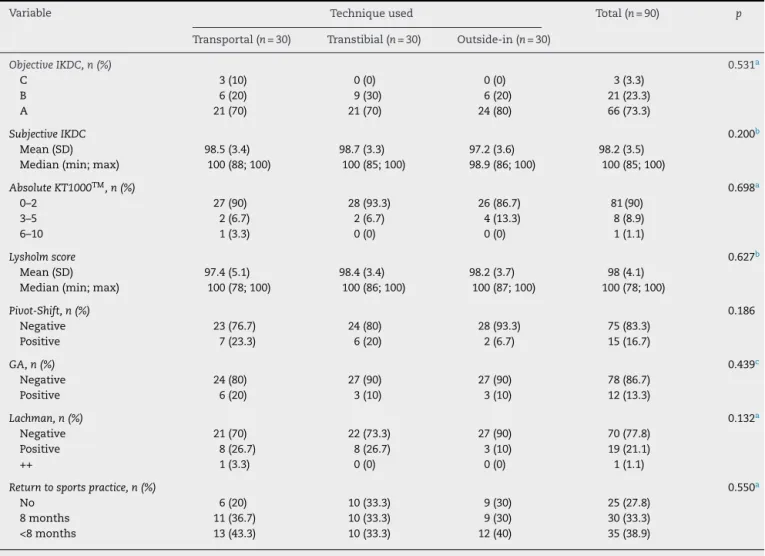
Table2–Descriptionofthepostoperativediagnosticscalesaccordingtoreconstructiontechniqueandresultofthe statisticaltests.
Variable Techniqueused Total(n=90) p
Transportal(n=30) Transtibial(n=30) Outside-in(n=30)
ObjectiveIKDC,n(%) 0.531a
C 3(10) 0(0) 0(0) 3(3.3)
B 6(20) 9(30) 6(20) 21(23.3)
A 21(70) 21(70) 24(80) 66(73.3)
SubjectiveIKDC 0.200b
Mean(SD) 98.5(3.4) 98.7(3.3) 97.2(3.6) 98.2(3.5)
Median(min;max) 100(88;100) 100(85;100) 98.9(86;100) 100(85;100)
AbsoluteKT1000TM,n(%) 0.698a
0–2 27(90) 28(93.3) 26(86.7) 81(90)
3–5 2(6.7) 2(6.7) 4(13.3) 8(8.9)
6–10 1(3.3) 0(0) 0(0) 1(1.1)
Lysholmscore 0.627b
Mean(SD) 97.4(5.1) 98.4(3.4) 98.2(3.7) 98(4.1)
Median(min;max) 100(78;100) 100(86;100) 100(87;100) 100(78;100)
Pivot-Shift,n(%) 0.186
Negative 23(76.7) 24(80) 28(93.3) 75(83.3)
Positive 7(23.3) 6(20) 2(6.7) 15(16.7)
GA,n(%) 0.439c
Negative 24(80) 27(90) 27(90) 78(86.7)
Positive 6(20) 3(10) 3(10) 12(13.3)
Lachman,n(%) 0.132a
Negative 21(70) 22(73.3) 27(90) 70(77.8)
Positive 8(26.7) 8(26.7) 3(10) 19(21.1)
++ 1(3.3) 0(0) 0(0) 1(1.1)
Returntosportspractice,n(%) 0.550a
No 6(20) 10(33.3) 9(30) 25(27.8)
8months 11(36.7) 10(33.3) 9(30) 30(33.3)
<8months 13(43.3) 10(33.3) 12(40) 35(38.9)
Chi-squaredtest.
a Kruskal–Wallistest. b ANOVA.
c Likelihoodratiotest.
positioning) wasmarked through the conventional antero-medial portal. The guidewire (Kirschner 2.4) was inserted and positioned at the previously marked point; the knee was flexed between 120 and 130 degrees, and finally the guidewirewasadvanceduntilitpassedthelateralcortexof thefemur.Subsequently,thefemoraltunnelwasmadewith therespectivedrill.Thefemoralfixationwasmadeusingan Endobutton® (Smith&Nephew,Andover,MA,UnitedStates), andthetibialfixationwasmadewithametallicinterference screw.
Inthe outside-intechnique, thetibial tunnelwasmade with the knee flexed at 90◦ and the tibial guide at 55◦. Then, the femoral tunnel was made, with an anatomical femoral guide, which was introduced through the antero-medialarthroscopic portalandpositionedanatomically.An incisionofapproximately1cmwasmadeoverthelateral epi-condyle; the fascia lata was perforated to reach the bone, allowingtheoutside-inguidewireinsertion,followedbythe correspondingdrillbit.Thefixationwasmadewithametallic interferencescrew,fromtheoutsidein,intothefemurandthe tibia.
All groups underwent the same rehabilitation protocol, using crutchesfortwoweekswithoutpostoperative immo-bilization.Patientswereauthorizedtoperformopenkinetic chainquadricepsexercisesafterthe eighthweek,runafter 16weeks,andreturntosportsaftersixmonths,aftera pro-prioceptive assessment and strength tests applied by the physiotherapist.
wasusedastheprimaryoutcomecriterion.Inordertodetect aminimumdifferenceof20%intheincidenceofCorD (post-operativeobjective IKDC)amongthegroups, withanalpha errorof5%andapowerof80%,30patientsineachgroupwere needed.
Thisstudywasapprovedbytheresearchethicscommittee oftheinstitution.
Results
Theassessmenttwoyearsaftersurgerywasperformedwith physicalexamination,KT1000TM arthrometer, objectiveand subjectiveIKDCscore,Lysholmscore,and timetoreturnto sport.Table2showstheobjectiveandsubjectivepostoperative results.
Regarding the objective evaluation, very similar results wereobtainedwhencomparingthethreegroups,for objec-tiveIKDC,KT1000TM,andanteriordrawertest.IntheLachman scoreandPivot-Shifttest,betterresultswereobservedinthe outside-ingroup,butwithoutstatisticalsignificance(p=0.132 andp=0.186;chi-squaredtestandKruskal–Wallistest, respec-tively).Regardingthesubjectiveevaluation,theLysholmand subjectiveIKDCscoresshowedsimilarresults(p=0.627and p=0.200,respectively;ANOVA).
Regarding returnto sports practice,27% ofthe patients didnotresume,33.3%returnedaftereightmonths,and38.9% beforeeightmonths.Whencomparingreturntosportsamong the three groups, similar results were observed (p=0.550, Kruskal–Wallistest).
Duringpatientenrollment,fivere-ruptureswereobserved, twointhe transtibial group, twointhe medialtransportal group,andoneinoutside-inthegroup.Whencomparingthe occurrenceofrupture betweenthegroups, thesefivecases were included, which led to a total of 32 patients in the transtibialgroup,32inthemedialtransportalgroup,and31 intheoutside-ingroup.Nostatisticallysignificantdifference wasobserved(chi-squaredtest,p=0.8).
Discussion
Recent studies have shown a trend toward better results whenusingtheanatomicaltechnique,inwhichthefemoral tunnelis placedin the center ofthe original ACL.7,13 Sev-eral biomechanical studies in cadavers2,5,13,14 and clinical studies in humans6,7 comparing the transtibial technique withanatomicaltechniques(medialtransportal or outside-in)demonstrated superiorresults(objectiveand subjective) inanatomicaltechniques,especiallyregardingrotational sta-bility. Nonetheless, there is no evidence of a long-term superiority, nor thatone techniquepresents fewer compli-cations, such as new rupture or evolution ofarthrosis. In somestudiesdemonstratingthesuperiorityofonetechnique overanotherthephysicalexaminationofthekneewas per-formedwithout theactionofthemuscles (suchascadaver knees or anesthetizedpatient) 2,5,15,16 and used subjective questionnaires.7,17
In spite all these considerations, in 2015 Robin et al.8 publishedasystematicreviewoftheadvantagesand disad-vantagesofthetranstibial,medialtransportal,andoutside-in
techniques.Despitethedifferencesbetweenthem,8,18 these authors concludedthat thereisnogold standardfor mak-ing thefemoraltunnel, whichleadstoquestionsabout the standardizationofthefemoraltunnelinthevariousstudies alreadymentioned.
When analyzingthephysicalexamination,nostatistical differencewasobservedintheanteriordrawerandLachman tests,asexpected,sincestabilityinthecoronalplaneis main-tainedinalltechniques.InthePivot-Shifttest,whichanalyzes therotationalstability,theanatomicaltechniqueisexpected toshowanadvantage.19–23 Inthepresentstudy,therewere fewer casesofPivot-Shiftpositivity inthe outside-in tech-nique, without statistical significance.However,these data shouldbecarefullyanalyzed,becausewithalargersample, perhaps some statistical difference would be observed, or it couldsimplyconfirmthattherereallyare nodifferences betweenthetechniques.Therefore,morestudiesand espe-ciallylargersamplesareneededformorepreciseconclusions. This study aimed to compare patients with different femoraltunnelpositioningandwithintactgraft.Nonetheless, itisimportanttocommentonre-rupture,sinceRahr-Wagner etal.24recentlypublishedaretrospectivestudy demonstrat-ing morere-ruptures in knees that underwent the medial transportaltechniquewhencomparedwithtranstibial tech-nique.ItisworthrememberingthatthestudybyRahr-Wagner et al.24 wasbased ondatafrom theDanishregistry, there-foreincludingpatientsoperatedbyseveralsurgeonsinseveral hospitals,whichgeneratesprobablebiases.Inaddition,other prospectivestudiescomparingthesetwotechniquesdidnot observe morere-ruptures inthe anatomical technique.25,26 Whenenrollingpatientsforthepresentstudy,twore-ruptures were observed in the transtibial group, two in the medial transportalgroup,andoneintheoutside-ingroup,withno statisticalsignificance.
Thisstudyhaslimitations,suchasthesmallsamplesize, since similar results are expected in the outcome criteria usedtoevaluatereconstructionsoftheanteriorcruciate liga-ment,whichrequiressampleswithalargenumberofpatients; the impossibility ofblinding the examiners in the evalua-tions,sincethescarsofeachtechniquearedifferent;thefact thattheKT1000TMwasnotappliedpreoperativelyprevented postoperative comparison;and thefact thatthe intra- and interobserver agreementswerenotassessed,which impov-erishestheevaluationofthephysicalexamination.
Conclusion
Nostatisticallysignificantdifferenceswerefoundinobjective andsubjectiveclinicalresultswhencomparingpatients sub-mittedtoACLreconstructionbytranstibial,transportal,and outside-intechniques.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. EmondCE,WoelberEB,KurdSK,CiccottiMG,CohenSB.A
comparisonoftheresultsofanteriorcruciateligament
reconstructionusingbioabsorbableversusmetalinterference
screwsameta-analysis.JBoneJointSurgAm.
2011;93(6):572–80.
2. SteinerME,BattagliaTC,HemingJF,RangJD,FestaA,BariaM.
Independentdrillingoutperformsconventionaltranstibial
drillinginanteriorcruciateligamentreconstruction.AmJ
SportsMed.2009;37(10):1912–9.
3. SteinerM.Anatomicsingle-bundleACLreconstruction.
SportsMedArthrosc.2009;17(4):247–51.
4. HemingJF,RandJ,SteinerME.Anatomicallimitationsof
transtibialdrillinginanteriorcruciateligament
reconstruction.AmJSportsMed.2007;35(10):1708–15.
5. BediA,MusahlV,SteuberV,KendoffD,ChoiD,AllenAA,
etal.Transtibialversusanteromedialportalreamingin
anteriorcruciateligamentreconstructionananatomicand
biomechanicalevaluationofsurgicaltechnique.Arthroscopy.
2011;27(3):380–90.
6. Alentorn-GeliE,SamitierG,AlvarezP,SteinbacherG,CugatR.
Anteromedialportalversustranstibialdrillingtechniquesin
ACLreconstructionablindedcross-sectionalstudyattwo-to
five-yearfollow-up.IntOrthop.2010;34(5):747–54.
7. HusseinM,vanEckCF,CretnikA,DinevskiD,FuFH.
Prospectiverandomizedclinicalevaluationofconventional
single-bundle,anatomicsingle-bundle,andanatomic
double-bundleanteriorcruciateligamentreconstruction:281
caseswith3-to5-yearfollow-up.AmJSportsMed.
2012;40(3):512–20.
8. RobinBN,JaniSS,MarvilSC,ReidJB,SchillhammerCK,
LubowitzJH.Advantagesanddisadvantagesoftranstibial,
anteromedialportal,andoutside-infemoraltunneldrillingin
single-bundleanteriorcruciateligamentreconstruction:a
systematicreview.Arthroscopy.2015;31(7):1412–7.
9. AndersonAF,IrrgangJJ,KocherMS,MannBJ,HarrastJJ,
InternationalKneeDocumentationCommittee.The
InternationalKneeDocumentationCommitteeSubjective
KneeEvaluationForm:normativedata.AmJSportsMed.
2006;34(1):128–35.
10.LysholmJ,GillquistJ.Evaluationofkneeligamentsurgery
resultswithspecialemphasisonuseofascoringscale.AmJ
SportsMed.1982;10(3):150–4.
11.KirkwoodBR,SterneJA.Essentialmedicalstatistics.2nded.
Massachusetts,USA:BlackwellScience;2006.
12.NeterJ.Appliedlinearstatisticalmodels.Chicago:Irwin;1996.
13.SteinerME,BattagliaTC,HemingJF,RandJD,FestaA,BariaM.
Independentdrillingoutperformsconventionaltranstibial
drillinginanteriorcruciateligamentreconstruction.AmJ
SportsMed.2009;37(10):1912–9.
14.SimJA,GadikotaHR,LiJS,LiG,GillTJ.Biomechanical
evaluationofkneejointlaxitiesandgraftforcesafteranterior
cruciateligamentreconstructionbyanteromedialportal,
outside-in,andtranstibialtechinques.AmJSportsMed.
2011;39(12):2604–11.
15.MusahlV,PlakseychukA,VanScyocA,SasakiT,DebskiRE,
McMahonPJ,etal.Varyingfemoraltunnelsbetweenthe
anatomicalfootprintandisometricpositions:effecton
kinematicsoftheanteriorcruciateligament-reconstructed
knee.AmJSportsMed.2005;33(5):712–8.
16.BrophyRH,PearleAD.Single-bundleanteriorcruciate
ligamentreconstruction:acomparisonofconventional,
central,andhorizontalsingle-bundlevirtualgraftpositions.
AmJSportsMed.2009;37(7):1317–23.
17.JepsenCF,Lundberg-JensenAK,FaunoeP.Doesthepositionof
thefemoraltunnelaffectthelaxityorclinicaloutcomeofthe
anteriorcruciateligament-reconstructedknee?Aclinical,
prospective,randomized,double-blindstudy.Arthroscopy.
2007;23(12):1326–33.
18.OsakiK,OkazakiK,MatsubaraH,KuwashimaU,MurakamiK,
IwamotoY.Asymmetryinfemoraltunnelsocketlength
duringanteriorcruciateligamentreconstructionwith
transportal,outside-in,andmodifiedtranstibialtechniques.
Arthroscopy.2015;31(12):2365–70.
19.LiuA,SunM,MaC,ChenY,XueX,GuoP,etal.Clinical
outcomesoftranstibialversusanteromedialdrilling
techniquestopreparethefemoraltunnelduringanterior
cruciateligamentreconstruction.KneeSurgSports
TraumatolArthrosc.2015.Jun16[Epubaheadofprint].
PubMedPMID:26077285.
20.WooSL,KanamoriA,ZeminskiJ,YagiM,PapageorgiouC,Fu
FH.Theeffectivenessofreconstructionoftheanterior
cruciateligamentwithhamstringsandpatellartendon.A
cadavericstudycomparinganteriortibialandrotational
loads.JBoneJointSurgAm.2002;84(6):907–14.
21.LohJC,FukudaY,TsudaE,SteadmanRJ,FuFH,WooSL.Knee
stabilityandgraftfunctionfollowinganteriorcruciate
ligamentreconstruction:comparisonbetween11o’clockand
10o’clockfemoraltunnelplacement.Arthroscopy.
2003;19(3):297–304.
22.KimMK,LeeBC,ParkJH.Anatomicsinglebundleanterior
cruciateligamentreconstructionbythetwoanteromedial
portalmethod:thecomparisonoftransportalandtranstibial
techniques.KneeSurgRelatRes.2011;23(4):213–9.
23.MulcaheyMK,DavidTS,EpsteinDM,AlaiaMJ,Montgomery
KD.Transtibialversusanteromedialportalanteriorcruciate
ligamentreconstructionusingsoft-tissuegraftand
expandablefixation.Arthroscopy.2015;31(12):2365–70.
24.Rahr-WagnerL,ThillemannTM,PedersenAB,LindMC.
Increasedriskofrevisionafteranteromedialcomparedwith
transtibialdrillingofthefemoraltunnelduringprimary
anteriorcruciateligamentreconstruction:resultsfromthe
danishkneeligamentreconstructionregister.Arthroscopy.
2013;29(1):98–105.
25.DuffeeA,MagnussenRA,PedrozaAD,FlaniganDC,MOON
Group,KaedingCC.TranstibialACLfemoraltunnel
preparationincreasesoddsofrepeatipsilateralkneesurgery.
JBoneJointSurgAm.2013;95(22):2035–42.
26.FranceschiF,PapaliaR,RizzelloG,BuonoAD,MAffulliN,
DenaroV.Anteromedialportalversustranstibialdrilling
techniquesinanteriorcruciateligamentreconstructionany
clinicalrelevance?Aretrospectivecomparativestudy.