REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologia www.sba.com.brSCIENTIFIC
ARTICLE
Analgesia
Nociception
Index
for
perioperative
analgesia
monitoring
in
spinal
surgery
Guldem
Turan
a,∗,
Arzu
Yıldırım
Ar
a,
Yıldız
Yigit
Kuplay
a,
Oznur
Demiroluk
a,
Mustafa
Gazi
a,
Nur
Akgun
a,
Erhan
Celikoglu
baFatihSultanMehmetTeachingandResearchHospital,AnesthesiologyandIntensiveCareUnit,Istanbul,Turkey bFatihSultanMehmetTeachingandResearchHospital,DepartmentofNeurosurgery,Istanbul,Turkey
Received29January2016;accepted26July2016 Availableonline18August2016
KEYWORDS
AnalgesiaNociceptive
Index; Sevoflurane; TIVA;
Spinalsurgery
Abstract
Backgroundandobjectives: TheAnalgesiaNociceptionIndexisanindexusedtomeasurethe levelsofpain,sympatheticsystemactivityandheartratevariabilityduringgeneral anesthe-sia.In ourstudy,AnalgesiaNociceptionIndexmonitoringintwogroups whohadundergone spinal stabilizationsurgery andwere administered propofol---remifentanil (TotalIntravenous Anesthesia)andsevoflurane---remifentanylanesthesiawascomparedregardingitssignificance forpredictionofpostoperativeearlypain.
Methods:BIS and Analgesia Nociception Index monitoring were conducted in the patients togetherwithstandardmonitoring.Duringinduction,fentanyl2g.kg−1,propofol2.5mg.kg−1
and rocuronium 0.6mg.kg−1 were administered. During maintenance, 1.0 MAC
sevoflu-rane+remifentanil0.05---0.3g.kg−1.min−1andpropofol50---150g.kg−1.min−1+remifentanil
0.05---0.3g.kg−1.min−1wereadministeredinGroupSandGroupT,respectively.Hemodynamic
parameters,BISandAnalgesiaNociceptionIndexvalueswererecordedduringsurgeryand30min postoperatively.Postoperativevisualanalogscale(VAS)valuesat30minuteswererecorded.
Results:WhilenodifferencewasfoundbetweenmeanAnalgesiaNociceptionIndexatalltimes ofmeasurementinbothgroups,AnalgesiaNociceptionIndexmeasurementsafteradministration ofperioperativeanalgesicdrugwererecordedtobesignificantlyhighercomparedtobaseline valuesinbothgroups.Therewas correlationbetweenmeanvaluesofAnalgesiaNociception IndexandVASafteranesthesia.
Conclusion:AnalgesiaNociceptionIndexisavaluableparameterformonitoringofperioperative andpostoperativeanalgesia.Inspinesurgery,similaranalgesiacanbeprovidedinbothTotal IntravenousAnesthesiawithremifentanilandsevofluraneadministration.AnalgesiaNociception Indexisefficientforpredictionoftheneedforanalgesiaduringtheearlypostoperativeperiod, andthereforeistheprovisionofpatientcomfort.
©2016SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](G.Turan). http://dx.doi.org/10.1016/j.bjane.2016.07.010
PALAVRAS-CHAVE
Índicede
analgesia/nocicepc¸ão;
Sevoflurano; TIVA;
Cirurgiadecoluna
vertebral
Índicedeanalgesia/nocicepc¸ãoparamonitorizac¸ãodaanalgesiaperioperatória nacirurgiadacolunavertebral
Resumo
Justificativaeobjetivos: OÍndicedeanalgesia/nocicepc¸ão(ANI)éusadoparamedirosníveis de dor, aatividade do sistema simpáticoe a variabilidadeda frequência cardíaca durante a anestesia geral. Em nosso estudo,a monitorac¸ão doANI em doisgrupos que foram sub-metidos à cirurgia de estabilizac¸ão dacoluna vertebral e receberam propofol-remifentanil (TotalIntravenousAnesthesia-TIVA)esevoflurano-remifentanilforamcomparadospara iden-tificarsuaimportâncianaprevisãoprecocededornopós-operatório.
Métodos: Os pacientes foram monitorados com o uso de BIS e ANI juntamente com a monitorac¸ão padrão. Durante a induc¸ão, fentanil (2g.kg−1), propofol (2,5mg.kg−1) e
rocurônio (0,6mg.kg−1) foram administrados. Durante a manutenc¸ão, 1 CAM de
sevoflu-rano+remifentanil(0,05---0,3g.kg−1.min−1)epropofol(50---150g.kg−1.min−1)+remifentanil
(0,05---0,3g.kg−1.min−1)foramadministradosaosgruposSeT,respectivamente.Parâmetros
hemodinâmicos,valoresdeBISeANIforamregistradosduranteacirurgiaeaos30minutosde pós-operatório.OsvaloresVisualAnalogueScale(VAS)aos30minutosdepós-operatórioforam registrados.
Resultados: Enquantonãoobservamosdiferenc¸aentreasmédiasdoANIemtodosostempos demensurac¸ãodeambososgrupos,asmensurac¸õesdoANIapósaadministrac¸ãodoanalgésico noperioperatórioforamsignificativamentemaioresqueosvaloresbasaisdeambososgrupos. Houvecorrelac¸ãoentreasmédiasdosvaloresdeANIeVASapósaanestesia.
Conclusão:ANI éumparâmetroimportantepara omonitorizac¸ãodeanalgesianosperíodos perioperatórioepós-operatório.Nacirurgiadacolunavertebral,analgesiasemelhantepodeser obtidacomanestesiaintravenosatotalcomremifentanilecomaadministrac¸ãodesevoflurano. OANI éeficiente para preveranecessidadede analgesiaduranteoperíodo pós-operatório imediatoe,portanto,paraproporcionarconfortoaopaciente.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Spinalstabilizationsurgeryisatop-levelsurgeryforcausing painful stimuli. Perception of pain by the patient dur-ingmonitoring of anesthesiacan beobserved aselevated arterial blood pressure and/or heart rate. The analgesia nociceptionindexiscalculatedbymeasurementofchangein thenociception---antinociceptionbalancereflectingtoheart rate simultaneously.1,2 Apatient without pain willhave a
dominantparasympathetictone.Normally,Analgesia Noci-ceptionIndex(ANI) valueranges from0to100,but when parasympathetic activity is dominant,then ANI shows the valuesover50 ormore.When thepainisperceived, sym-pathetic system will be dominant and the ANI value will fallbelow 50.Undergeneral anesthesia,the ANIrangeof 50---70showstheadequatelevelofanalgesia.Inaconscious patient,while highervaluesareindicativeofanalgesia,in lowerlevels,psychologicalstressfactormaycomeintoplay andANImayloseitsreliability.3,4
SinceANIyieldscontinuousandasinglenumericalvalue, it can be a valuable parameter during the monitoring of the level of analgesia. Additionally, it mayplay a rolein prediction of thelevel of postoperative early pain. Thus, patientcomfortcanbeprovidedbyenablingtoadminister additionalanalgesicdrugattheendofthesurgery.
In ourstudy,we ensuredANImonitoringduring surgery andduringtheearlypostoperativeperiodinthefollowing
twogroupsofpatientswhohadundergonespinal stabiliza-tionsurgery, which wasa painful surgery: the first group wasadministeredTotalIntravenousAnesthesia (TIVA)with propofolandremifentanylandthesecondgroupwas admin-isteredsevoflurane---remifentanylanesthesia.Theaimofthe study wasto investigate ifthere wasa difference or not betweenthetwoanesthesiamethodsregardingpredictionof perioperativeanalgesialevelandthelevelofpostoperative earlypain.
Materials
and
methods
Approvalwasobtainedfromthehospital’sethicscommittee (FSMEAHKAEKno2015/59)andinformedcontentsfromeach patientforthestudy.
premedicationwererandomlydividedintotwoequal-sized groupspreoperativelybyusingsimplecomputerprogram.
The patient was placed on the operating table and a venous accesswasestablished throughthe dorsumof the hand.Afteradministrationoflocalanestheticagent,Allen testwasperformedandtheninvasivearterialbloodpressure wasperformedwitharterialcannulationpreferablythrough rightradialartery.Heartrateandperipheraloxygen satu-rationmonitorizationwereperformed(Mindray,China).BIS monitorization(Covidien,Dublin,Ireland)wasperformedby using4electrodessuitablyplacedonthepatient’sforehead. TwoprobesofANImonitor(MetroDoloris,Lille,France)were suitablyplaced.Accordingtorecommendationofthe man-ufacturer, the front facing electrode of ANI probes was plannedtobeplacedonthemiddleofthesternumasthe firstchoice. Sincethepatients wouldbeinproneposition duetocertaincharacteristicsofthesurgery,theprobewas placed behind the middle of the sternum as the second choice,andthemeasurementwasobtained.ThesecondANI probewasplacedontheregioncorrespondingtothe8---9th ribatthelevelofthemidaxillaryline.
ANIpointswereconsideredasthefollowing:0---30severe pain,30---50moderatepain,50---70comfortableand70---100 nopain,andnoneedofanyanalgesic.
After basal measurements, during induction, fen-tanyl 2g.kg−1, propofol 2.5mg.kg−1 and rocuronium
0.6mg.kg−1 were administered in both groups. During maintenance,accordingtoBISvaluesbetween 40and60, 1.0MACsevoflurane+remifentanyl0.05---0.3g.kg−1.min−1
and propofol 50---150g.kg−1.min−1+remifentanyl
0.05---0.3g.kg−1.min−1 were administered in Group S and
Group T. Measurements were recorded as the following: after induction, intubation, surgical incision, at 5---10min intervals perioperatively, at the end of anesthesia, after extubationandatthepostoperative5th,15thand30th min-utes. Foranalgesic purpose, paracetamol1g.100mL−1 (IV infusion),diclofenacsodium20mg(IV)andtramadol100mg (IVinfusion)wereadministeredinallofthepatients approx-imately30minbeforetheendofsurgery.Fiveminutesafter theendof10mininfusionofanalgesicdrugs,measurements wereseparately recordedasmeasurements at theend of analgesic drug.Postoperative 5,15 and30min VAS values wererecordedonascorebetween0and10(0:nopain,1---3: mild pain,4---7: moderate pain, 8---9: severe painand 10: veryseverepain).Atropineandephedrineadministrations, whichmightinfluenceheartratevariability,wererecorded.
Statisticalevaluations
Whenweconsidered=26andSD=16attheendofpower analysisperformedbyusingpowerandsample-sizeprogram, samplesize wasdeterminedtobeminimumn:9for each groupdetectedforPower=0.80and˛=0.05.
During the evaluation of the data obtained from the study,IBMSPSSStatistics22.0programwasusedforthe sta-tisticalanalysis. Duringtheassessment ofthe studydata, conformity of the parameters to the normal distribution wasassessedby theKolmogorov---Smirnovtest. Duringthe evaluationofthestudydata,regardingthecomparisonsof descriptivestatistical methods(Mean, Standarddeviation) aswellasquantitativedata,Studentttestwasusedforthe
ANI values for perioperative and postoperative period 120
100 80 60 40 20 0
Group S Group T
Basal
After induction
After entubation After incision51
5th min 10h min 15th min 20th min 30th min 40th min 50th min 60th min 70th min 80th min 90th min
100th min 110th min 130th min 140th min 150th min
End of anesthesia
After e
xtubation
postop 5th min
postop 15th min postop 30th min
Figure 1 ANI values for perioperative and postoperative period.
intergroupcomparisonsofparameterswithnormal distribu-tionandMannWhitneyUtestwasusedfor theintergroup comparisons of parameters without normal distribution. PairedSamplest-testwasusedforthein-groupcomparisons of parameters with normal distribution. Wilcoxon Signed Rankstestwasusedforthein-groupcomparisonsof param-eterswithoutnormaldistribution.Duringtheevaluationof correlationbetweentheparametersconformingtoanormal distribution, Pearson’s correlation analysis wasused. Chi-squaretestwasusedfortheevaluationofqualitativedata. Significancewasevaluatedatalevelofp<0.05.
Results
Therewasnodifferencebetweendemographic characteris-ticsanddurationsofanesthesiaandsurgeryofthepatients (Table1).
Whilethere was nodifference hemodynamicallyat all themeasurementtimesinmeanarterialpressuresbetween groups,heartratemeasurementsattheperioperative20th and30thminutewerefoundtobehigherinTIVAgroup com-paredtosevofluranegroup(p=0.038,p=0.031).
There was no difference between the two groups regarding meanANI valuesatall themeasurement times. WhilemeanANIvaluesatallthemeasurementsafter intu-bationwerebelow50inbothgroups(GroupT44.3±10.9, GroupS39±11.2),ANIvaluewasmeasuredtobe43.7±9.2 in GroupS afterincision(inGroup P51.33±16.14). Mean valuesof ANImeasurementsperformed at the5thminute after incision were found to be below 50 in both groups (Group T 44.7±8.7, Group S 48.8±14). Mean ANI values atalltheothermeasurementtimeswereabove50ormore. MeanANIvaluesmeasuredafteradministrationof perioper-ativeanalgesicdrugwererecordedattheideallevelsinboth groups(GroupT67.6±13.1,GroupS68.1±18.3)(Fig.1).
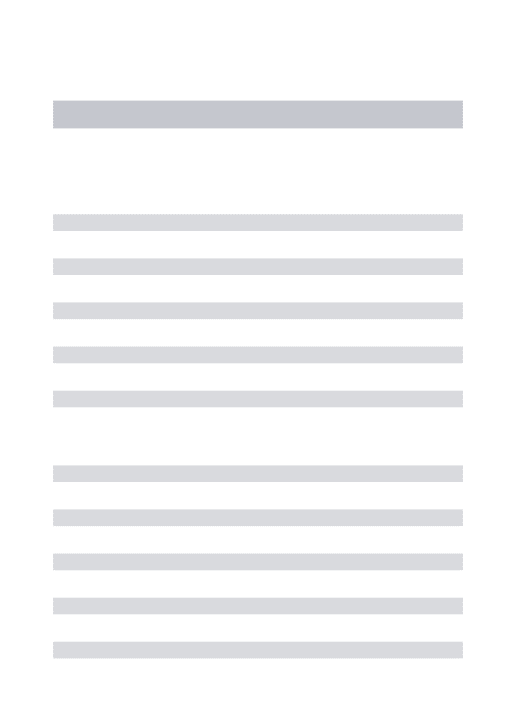
Therewasnodifferencebetweengroupsregardingmean postoperative VAS values. There wascorrelation between mean ANI valuesand VASvalues at the endof anesthesia (Table2).
Therewasnodifferencebetweengroupsregardingmean BISvalues.
Table1 Demographiccharacteristicsanddurationsofanesthesiaandsurgery.
GroupS GroupT p
Mean±SD Mean±SD
Age(years) 56.27±8.3 54.27±9.81 0.552
Bodymassindex(kg.m−2) 28.0±3.76 28.8±5.47 0.644
Durationofanesthesia(min) 183.4±54.67 180.93±52.75 0.930
Durationofsurgery(min) 159.27±53.2 155.87±57.29 0.898
Studentt-test.
Table2 VisualanalogscorevaluesaccordingtoANI.
Visualanalogscore AnalgesiaNociceptionIndex p
Medium(30---50) Normal(50---70) Nopain,noneedofanyanalgesic(70---100)
n(%) n(%) n(%)
Afterextubation 0.066
Nopain(0) 1(33.3) 12(92.3) 9(64.3)
Moderate(4---7) 2(66.7) 1(7.7) 5(35.7)
VAS5thmin 0.109
Nopain(0) 0(0) 10(76.9) 7(50)
Mild(1---3) 3(100) 3(23.1) 6(42.9)
Moderate(4---7) 0(0) 0(0) 1(7.1)
VAS15thmin 0.259
Nopain(0) 0(0) 7(53.8) 5(35.7)
Mild(1---3) 2(66.7) 6(46.2) 7(50)
Moderate(4---7) 1(33.3) 0(0) 2(14.3)
VAS30thmin 0.522
Nopain(0) 0(0) 6(46.2) 4(38.6)
Mild(1---3) 2(66.7) 6(46.2) 8(57.1)
Moderate(4---7) 1(33.3) 1(7.7) 2(14.3)
Ki-Karetest.
Discussion
Sinceanalgesia nociception indexyieldscontinuous and a
singlenumericalvalueespeciallyinthemostpainfulsurgical
procedures,itcanbeavaluableparameterduring
monitor-ingoflevelofanalgesia.Additionally,itmayplayarolein
prediction of thelevel of postoperative early pain. Thus,
patientcomfortcanbeprovidedbyenablingtoadminister
additionalanalgesicdrugattheendofthesurgery.
Jeanne et al.5 performed ANI monitoring in 15 adult
patientswhohadundergonelaparoscopicappendectomyor cholecystectomy. In the study, propofol and remifentanyl infusion was used during maintenance of anesthesia, and while higher ANI values (88or more)were observed with anesthesia induction, ANI values decreased to60---50 lev-elswithinitiationof surgery. Aftercompletionofsurgery, anANIvalueof90wasobserved.TheauthorsfoundANIto be more sensitive than heart rate variability and systolic arterialbloodpressureasanindicatorofpain.
In thirty patients administered sevoflurane anesthesia, Ledowskietal.6observedadecreaseinANIvaluewith
intu-bationandafterskinincisionandan increaseinANIvalue withadministrationof fentanyl.Also,in ourstudy,similar
tosevofluranegroup,adecreasewasobservedinANIvalue withskinincision.
Szentaletal.7divided120patientswhohadundergone
laparoscopic cholecystectomy into two equal groups and performed analgesiaprotocol withANI monitoring.At the end of their study evaluating the postoperative VAS and morphinerequirement,theyreportedthatANI monitoring didnotprovideanadvantageinpredictionofpostoperative pain.
Jeanneetal.8monitoredtheANIvaluesinthepatients
whohad undergonetotal kneereplacementwithpropofol anesthesiaandreportedthatalthough thedatawere reli-ablein the patients under general anesthesiathey might notbereliableinawakenedpatients.
Logieretal.9reportedthatanincreasecouldbeobserved
inheartratevariabilityandsystemicarterialbloodpressure duetotourniquetpaininthepatientsusedlong-term tourni-quetbutthisincreasecouldoccurduetootherreasons.They statedthatuseofANImonitoringcouldbeefficientinorder tomakethisdiscrimination.
Bosellietal.10 investigatedthecorrelationbetweenANI
ANI<50 value and VAS>3. The authors reported that ANI value immediately before extubation was basedon many differentfactorsotherthanpaincommonlyencounteredin the Post-Anesthesia Care Unit (PACU) that was known to affectsympatheticactivity,suchasstressandanxiety,and thereforemightinfluenceANIvalueinawakenedpatients. TheyreportedthatANIvaluesmightbeaffecteddepending onwhethertheanestheticmethodselectedwasinhalation or TIVAand inhalation anesthetics might result in amore markedreductioninheartratevariability.
Againthesameinvestigatorsstatedthatthelimitations oftheirstudy wasthe useofatropineand neostigmineto preventresidualparalysis afterreversal of neuromuscular blockadein case use of cisatracurium andatropine might affectheartratevariability.Inourstudy,wealso adminis-teredatropineandneostigminetopreventresidualparalysis afterreversalofneuromuscularblockade.Consideringthat standardproceduresareappliedinallofthepatientsandthe drugscounterbalancetheirinfluencesonheartrate variabil-ity,wethinkthatroutineprocedureswillnotcauseproblem. However,itcanberecommendedtomonitorsafereversal byperformingroutineTOFmonitorizationand/ortoprefer sugammadextoprovidemoreidealconditions.Besidesthat, sinceANIvaluesarecomparedwithpostoperativeVAS val-uesattheendofanesthesiainourstudy,theinfluenceof atropine/neostigmineadministeredis not observedat the measurements.
The investigators of the aforementioned study stated thattheinfluenceofshort-actingremifentanyl,usedalsoin ourstudyonheartratevariability,mightbedifferentthan long-actingfentanylorsulfentanylandmayactasanother limitationoftheirstudy.Althoughlong-actingopioidscanbe preferred,wethinkthattheirinfluencesonrecoveryfrom anesthesiashouldalsobeconsidered.
In the study performed in 120 patients by Ledowski etal.,11theauthorsevaluatedthecorrelationbetweenANI
valuesand VAS values in the postoperative care unit and observedacorrelationbetweenANIvaluesandseverepain in limited number of patients. As it was interpreted by Borellietal.,10thismightresultfromotherfactors
influenc-ingANIvaluesinthepostoperativecareunit.Therefore,we usedANIvalueattheendofanesthesiaasabaseinourstudy. Gruenewald et al.12,13 published two different
stud-ies on this subject. The authors compared ANI value and Surgical Pleth Index (SPI) for the measurement of nociception---antinociceptionbalanceinboth oftheir stud-ies.The Surgical Pleth Index(SPI)is avalue derived from measurementperformedwithfingerphotoplethysmographic signal.Twenty-fivepatientswereincludedinboththe stud-ies;BISvaluewasmonitoredtobebetween30and60,and whiletheauthorsusedsevofluraneandremifentanylinone of their studies, they used propofol and remifentanyl in anotherstudy.Theyreportedthatboth ofthemethods in bothoftheirstudiesperformedwithbothoftheanesthesia methodswerefoundtobesignificantasindicatorof anal-gesiaandtheyemphasizedthatitwasnecessarytoperform studieswithANIindifferentpatientgroupswithlarge num-berofpatients.Additionally,theystatedthatlargernumber of femalepatients in their study performed with sevoflu-ranemightaffectthestudyresultsduetohigherincidence ofchronicdiseases involvingtheregulation mechanismsof autonomicnervoussysteminmalegender.
Bollag et al.14 performed a study in 20 patients who
hadundergonehysterectomytodemonstratethe sympath-omimeticandalsoanalgesiceffectofketamineonANI mea-surements.Theyadministeredketamineasasinglei.v.bolus ofdose of0.5g.kg−15minafterintubationandreported
thatANIvaluesdidnotchangetowardanalgesiawith admin-istrationofketamine.Here,thesympathomimeticeffectsof ketaminemightaffectANImeasurements.
Sabourdinetal.15 administereddesfluraneand
remifen-tanylin12pediatricpatientswithmeanageof8yearsand emphasizedthatANImeasurementsweremoresensitiveas anindicatorofperioperativepainanditisnecessaryto per-formstudieswithlargenumberofpatientsinthepediatric patientgroup.
When the limitations of our study are investigated, this can be explained as administration of atropine and neostigminetopreventresidualparalysisafterreversal of neuromuscularblockaderegardinginfluencingtheheartrate variability.Forthispurpose,administrationofsugammadex can be recommended. However, since we compared ANI values with postoperative VAS value at the end of anes-thesia in our study, we did not observe the influence of atropine/neostigmine administered at the measurements. Also,administrationofperioperative drugsinfluencingthe heartratevariabilitysuchasatropineandephedrinemight influence ANI values. We found no difference between ourgroupsregardingperioperativeatropineadministration. Therefore we predicted that the mean values were not affected.However,duringevaluationofANIvalues,wethink thatthe effectsofadministrationofdrugs influencingthe heartratevariabilityshouldbecertainlyconsidered.
The second limitation of ourstudy was notbeing able toplacethefrontfaceoftheelectrodeoftheANI probes on themiddle of the sternum in the surgeriesperformed intheproneposition.Sincesurgerypositionofourpatient groupwasproneposition,weplacedthefrontfaceofthe electrode of the ANI probes on the back region of the patientaccordingtorecommendationofthemanufacturer underthenecessaryconditions.Therefore,weencountered notechnicalproblemassociatedwithmeasurement inour patients.Additionally,wedevelopedasolutionbycovering the surface of electrode withtransparent surgical drapes topreventthedetachmentofANIelectrodesfromtheskin asaresultbygettingwetwiththesterilizationsolutionand thereforenotbeingabletoperformthemeasurementaswe experiencedinourpreviousstudyofpatientsduringclinical practice.
Inconclusion,underthecondition thatconsidering the factorswhichmayinfluencethemeasurementof perioper-ativeandpostoperativemonitoringofanalgesia(superficial anesthesia,drugadministrationinfluencingheartrate vari-ability, etc.), ANI is a valuable parameter. In spinal stabilizationsurgeries,similaranalgesiacanbeprovidedin bothTIVAwithremifentanylandsevofluraneadministration. ANIisefficientforpredictionoftheneedforanalgesia dur-ingtheearly postoperativeperiodandtherefore provision ofpatientcomfort.
Conflicts
of
interest
References
1.LogierR,JeanneM,DeJonckheereJ, etal.PhysioDoloris:a monitoringdevice for analgesia/nociception balance evalua-tionusing heartratevariability analysis.ConfProc IEEEEng MedBiolSoc. 2010;2010:1194---7, http://dx.doi.org/10.1109/ IEMBS.2010.5625971.
2.DeJonckheereJ,DelecroixM,JeanneM,etal.Automated anal-gesicdrugsdeliveryguidedbyvagaltoneevaluation:interestof theAnalgesiaNociceptionIndex(ANI).ConfProcIEEEEngMed BiolSoc.2013:1952---5.
3.DeJonckheereJ,RommelD,NandrinoJL,etal.Heartrate vari-abilityanalysisasan indexof emotionregulationprocesses: interestoftheAnalgesiaNociceptionIndex(ANI).ConfProcIEEE EngMedBiolSoc.2012:3432---5.
4.JeanneM,LogierR,DeJonckheereJ,etal.Heartrate variabil-ityduringtotalintravenousanesthesia:effectsofnociception andanalgesia.AutonNeurosci.2009;147:91---6.
5.Jeanne M, Clément C, De Jonckheere J, et al. Variations ofthe analgesianociception index duringgeneral anaesthe-siafor laparoscopicabdominalsurgery.JClinMonitComput. 2012;26:289---94.
6.Ledowski T, Averhoff L, Tiong WS, et al. Analgesia Noci-ceptionIndex (ANI) to predictintraoperativehaemodynamic changes: results of a pilot investigation. Acta Anaesthesiol Scand.2014;58:74---9.
7.SzentalJA, WebbA,Weeraratne C,etal. Postoperativepain afterlaparoscopic cholecystectomy is not reduced by intra-operative analgesia guided by analgesia nociception index (ANI®) monitoring: arandomizedclinicaltrial.Br JAnaesth.
2015;114:640---5.
8.JeanneM,DelecroixM,DeJonckheere J,etal.Variationsof theanalgesianociceptionindexduringpropofolanesthesiafor totalkneereplacement.ClinJPain.2014;30:1084---8.
9.LogierR,DeJonckheereJ,DelecroixM,etal.Heartrate vari-abilityanalysisfor arterial hypertensionetiological diagnosis duringsurgicalproceduresundertourniquet.ConfProcIEEEEng MedBiol Soc. 2011;2011:3776---9,http://dx.doi.org/10.1109/ IEMBS.2011.6090645.
10.Boselli E, Bouvet L, Begou G, et al. Prediction of imme-diate postoperative pain using the analgesia/nociception index: a prospective observational study. Br J Anaesth. 2014;112:715---21.
11.LedowskiT,TiongWS,LeeC,etal.Analgesianociceptionindex: evaluationasanewparameterforacutepostoperativepain.Br JAnaesth.2013;111:627---9.
12.Gruenewald M, Ilies C, Herz J, et al. Influence of noci-ception stimulation on analgesia nociception index (ANI) during propofol---remifentanyl anaesthesia. Br J Anaesth. 2013;110:1024---30.
13.Gruenewald M, Ilies C, Herz J, et al. Measurement of the nociceptivebalancebyanalgesianociception index(ani)and surgical pleth index (spi) during sevoflurane---remifentanyl anaesthesia.MinervaAnestesiol.2015;81:480---9.
14.BollagL,OrtnerCM,JelacicS,etal.Theeffectsoflow-dose ketamineontheanalgesianociception index(ANI)measured withthenovelPhysioDolorisTManalgesiamonitor:apilotstudy.
JClinMonitComput.2015;29:291---5.