REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
CLINICAL
INFORMATION
Cardiac
tamponade:
a
rare
complication
of
central
venous
catheter
---
a
clinical
case
report
Ana
Catarina
Azevedo
a,
Isabel
Flor
de
Lima
a,∗,
Vânia
Brito
a,
Maria
João
Centeno
a,
Antero
Fernandes
baHospitalGarciadeOrta,EPE,Almada,Portugal
bHospitalGarciadeOrta,UnidadedeCuidadosIntensivos,EPE,Almada,Portugal
Received21June2014;accepted15April2015
Availableonline18September2016
KEYWORDS
Cardiactamponade; Centralvenous catheter; Iatrogenesis
Abstract Theextensiveuseofcentralvenouscatheters(CVC)inahospitalenvironmentleads toincreasediatrogeniccomplications,asmorecathetersareusedenclosedanditsmaintenance isprolonged.Severalcomplicationsareknowntoberelatedtocentralvenouscatheter,ofwhich theuncommoncardiactamponade(CT),hardlyrecognizedandassociatedwithhighmortality. Wepresentaclinicalcase,with favorableoutcome,ofapatientwho developedaCT 17 daysafterCVCplacement,andtrytoreflectonthemeasuresthatcanbetakentoreduceits incidence,aswellasthetherapeuticapproachestopracticeinthepresenceofasuspectedCT. ©2016SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Tamponamento cardíaco; Catetervenoso central; Iatrogenia
Tamponamentocardíaco:umacomplicac¸ãoraradacateterizac¸ãovenosacentral ---relatodeumcasoclínico
Resumo Ovasto usodos cateteres venosos centrais(CVC) em meio hospitalarincita a um aumentodaiatrogenia,umavezquesãocolocadosmaiscatetereseasuamanutenc¸ãoémais prolongada.Sãoconhecidasascomplicac¸õesrelacionadascomacateterizac¸ãovenosacentral, umadasquais otamponamentocardíaco (TC),raro,dificilmentereconhecidoeassociadoa grandemortalidade.
∗Correspondingauthor.
E-mail:[email protected](I.FlordeLima).
https://doi.org/10.1016/j.bjane.2015.04.005
Osautoresapresentamumcasoclínico,comdesfechofavorável,deumadoenteque desen-volveu um TC 17 diasapós a colocac¸ão de um CVCe procuram refletir sobre as medidas que podem seradotadas para reduzir asuaincidência, bemcomo asatitudes terapêuticas nasuspeitadeTC.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Centralvenouscatheter(CVC)iswidelyusedinhospitalsfor central monitoring; placement of temporary pacemakers; administrationof fluids, blood products, parenteral nutri-tionordrugs(antibiotics,vasopressors,chemotherapy,and others). This extensive use of CVC prompts an increase iniatrogenicconditionsassociatedwiththistechnique,as morecatheterarebeingplacedandkeptlonger.1,2
Complications of central venous catheterization are
known and cardiac tamponade (CT) is a rare and hardly
recognizedcomplication associatedwithhigh mortality.3,4
Basedprimarilyoncasereports,itsincidencerangesfrom
0.0001% to1.4% and itsassociated mortality from65% to
100%in adults;in children,theincidenceis higher(1---3%)
andmortalityislower(30---50%).5,6
ThesignsandsymptomsofCT,inadditiontobeing
unspe-cific, may arise within few minutes after CVC insertion
or upto five months after placement,3,5,7 which explains
the missedor latediagnosis and the fate of many of the
describedcases.
Wepresentacasewithafavorableoutcomeinapatient
whodevelopedaCT17daysafterCVCplacementintheright
internaljugularvein.
Inthisarticle, wewilldiscussthefactorsthatincrease
the risk of this complication, the measures that can be
adoptedinourprotocolstoreducetheincidence,andthe
therapeuticapproachestousewhenfacedwithasuspected
CT.
Clinical
case
Female patient, 26 years old, 150cm tall, 55kg, ASA IV,
admittedforelectiveleftnephrectomydueto
pyonephro-sis refractory to antibiotic therapy. The patient relevant
clinicalhistoryincludedpolymalformativesyndrome
(hydro-cephalus, spina bifida, interventricular communication,
vesicoureteral reflux, neurogenic bladder, dysfunctional
colon, and imperforate anus), with various surgical
repair interventions, epilepsy, and chronic renal failure
on hemodialysis (renal transplantation in 2001).
Labora-tory tests showed hemoglobin --- 102g.L−1; hematocrit
---0.311L.L−1; platelets ---193×109.L−1; prothrombinrate
---60%; aPTT--- 45.4s; INR --- 1.45;creatinine --- 9.8mg.dL−1.
Electrocardiogram (ECG) showedsinus tachycardia with a
frequencyof106beatsperminute.
Thepatienthadnoperipheralvenousaccess,reasonwhy
aCVCwasplacedbeforetheinductionofgeneralanesthesia.
Therightinternaljugularveinwaspuncturedatfirstattempt
by an experienced anesthesiologist. A 3-lumen catheter,
15cmlong(Certofix®Trio;B|BRAUN)wasinsertedusingthe
Seldingertechnique,withoutanychangesinECG.The
cor-rectinsertionintothevenoussystemwasconfirmedby
ultra-soundvisualizationof the needle,guidewireand catheter
and free aspiration of dark red blood through the three
lumens. During surgery, the patient required vasopressor
supportwithnorepinephrine,bloodtransfusions(twounits
offreshfrozenplasmaandsevenunitsofcryoprecipitate),
inadditiontofluidmaintenance/bloodlossreplacement,an
estimated1000mLofinfusedfluidsthroughtheCVC.
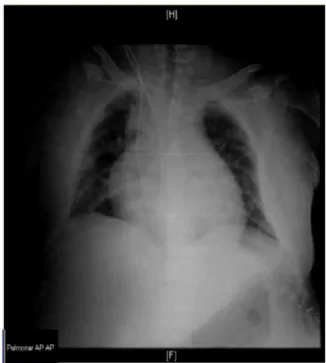
AchestX-raywasperformedatthePost-AnesthesiaCare
Unit(PACU)immediatelyaftersurgery(Fig.1),with
intrac-ardiacviewofthecathetertip.Duetothepoor technical
conditionsofradiography,thefindingwasneglectedandthe
catheterwasnotexternalized.
Thepatientreturnedtotheoperatingroomsevendays
laterduetoaretroperitoneal hematoma,inthe
nephrec-tomybed,withoutactivebleedingfocus.Duringsurgery,the
patientrequired vasopressorsupport withnorepinephrine
and,throughthesameCVC,twounitsofpackedredblood
cells and isosmolar fluid were infused, with a volume of
1200mL,uneventfully.
Figure 1 Postoperative chest X-ray performed after CVC
Figure2 ChestX-rayperformed14daysafterCVCplacement
(onsetofsymptoms).
During hospitalization, 14 days after CVC placement,
the patient developed dyspnea and precordial pain, and
another chest X-ray was performed (Fig. 2), again
with-out appraisingthe tip of the CVC positioning. At day 16,
the patient presented with hemodynamic instability with
significant worsening on the 17th day and progression to
cardiopulmonaryarrest(CPA)withasystole,withreturnof
spontaneouscirculation10minafterthestartofadvanced
lifesupport(ALS).
Immediately after transfer to the Intensive Care Unit
(ICU),shehadanewepisodeofbradycardiawith
progres-siontoasystole, withpulserecoveryafterfiveminutesof
ALS.Subsequently,atransthoracicechocardiogramshowed
CTandtheCVCtipintothepericardialspace.Wecontacted
thecardiologydepartment,andpericardiocentesiswas
per-formed,withimmediateoutputof400mLofhematicliquid,
resultingin improved hemodynamics.Pericardialdrainage
wasperformed withoutputof750mLofhematicliquidin
24h.ThejugularCVCwasremovedafteranewchestX-ray,
whichconfirmedtheintracardiacplacementofthecatheter
tip(Fig.3).
ThepatientwasdischargedfromtheICUtwodayslater,
hemodynamically stable, withspontaneous breathing and
withoutsequelae.
Discussion
A study8 based on 6440 medicalrecords of complications
associatedwithmedicalpractice,performedbetween1979
and 2000, reveals that 110 (1.7%) of such complications
wererelatedtoCVCplacementandthatof16registeredCT,
13wereassociatedwithprolongeduseofcatheters,witha
highmortalityrate(81%)comparedtoothercomplications.
Infact,CTcausedbycentralvenouscatheterizationisa
well-documentedentity,withclinicalcasesreportedsince
1958.5 However, its variable incidence in the literature
Figure3 ChestX-rayperformed17daysafterCVCplacement
(afterpericardiocentesis).
remains low because CT cases are not recognized or not
disclosed.5
Therearedifferentmechanismsinvolvedinpost-CVCCT:
directtraumaatthetimeofinsertion,cathetermigration,
andmechanicalandchemicalerosion.1,5
Upon insertion, the guidewire (despite its flexible
J-tip), introducer or catheter may cause a detachment of
the superior vena cava (SVC) wall at the atrium
junc-tion (SVC intrapericardial portion) or perforation of the
heartchambersandfrequentlycausingacutesymptoms.1,6,9
Noteworthily,thecomplicationsdirectlyresultingfromCVC
insertion are closely related to the physician’s
experi-ence.Inexperiencedphysicianshavefailurerateswiththe
techniqueandcomplicationsthataretwicethoseof
expe-riencedphysicians.1CVCmaterial(polyethylene,siliconeor
polyurethane)alsohasinfluenceonCTorigin.Themorestiff
andlessflexibleitis,thegreatertheriskofperforation.2
CVC repeated contact with the endocardium leads to
thrombusformationandCVCadherencetothemyocardium,
myocardialwallerosion,necrosis,andperforationuptothe
pericardial space, causing CTafter several days.2,9
Perfo-rationismorelikelytooccurifthecathetertipislocated
intheheart,incontactwiththewall,becausethecutting
edgemovesincorrespondence withtherespiratory
move-mentsandcardiaccontractility.2The angleformed bythe
catheter tip and the vessel or heart wall is also a major
riskfactor.Themoreperpendiculartheangleis(>40◦),the
greater the possibilityof erosionandnecrosis perforation
ofthevesselintimaorheartwall,2,5whichismoreevident
when CVCis placedvia subclavianor leftinternal jugular
veinduetoitsmoretortuouspath.5
Chemical erosionhappens whenhyperosmolar fluids in
contactwiththeendocardiumleadtoerosionandosmotic
injuryperforation,withtransmuraldiffusionoffluids
lead-ing to pericardial effusion.2,9 From the momentin which
thereis hypertonic fluid present inthe pericardial space,
The mostcommonsites of perforationareright atrium
(RA)and right ventricle(RV)in 80% ofcases, followedby
theSVC.5There isalso reportsof leftatrial(LA),SVC/RA
junction,andleftsubclavianveinperforations.9
CTmaynotalwaysbeprevented, butcertainmeasures
canreduceitsincidenceandmortality.Ourconductduring
central venous catheterization can be changed and some
precautionscanbetaken.
Acatheterwiththeshortestlengthpossible,appropriate
totheclinical situation,should beselected.1,10 According
totheliterature,catheterswith15---16cmsignificantly
min-imizeCVCintracardiacplacementviasubclavianorjugular
vein.1,11
Whenever possible and available, realtime ultrasound
should beused toguide theinsertion of CVC via internal
jugularvein,inordertoimprovethesuccessrateandreduce
the incidence of complications.10,12,13 Regarding catheter
placementvia subclavianorfemoral vein,theevidenceis
ambiguous to recommend its routine use.10,13 The use of
ultrasoundhasbeen suggestedforvein andlocalanatomy
screeningpriortopuncture(staticultrasound),particularly
inhighriskpatients.13
At thetimeofpuncture,theblood coloror absenceof
pulsatileflowshouldnotprecludethelaterconfirmationof
theCVClocation.10
The catheter tip position may be confirmed by three
methods:chestX-ray,fluoroscopy,andendocavitaryECG.10
ThemajoradvantageoffluoroscopyandendocavitaryECGis
thepossibilitytoconfirmtheinitialpositionofthecatheter
tip on the bedside monitor. The literature reports that
placing a CVC without a fluoroscopic or continuous ECG
monitoring of the catheter tip results in at least 15% of
erroneouslypositionedcatheters.14Intheoperatingtheater
ofourhospital,the protocolrequires achest X-rayin the
immediatepostoperativeperiod.
Itisalsoimportanttocheckthebloodbackflowthrough
theCVClumensand,particularly,aspiratetheblood from
the distal lumen15 toconfirm its position in the vascular
system,3,9,16 andperformitregularlyandaseptically
when-ever the catheter is used.Noteworthily, thedistal lumen
shouldnotbeusedtoinfusehyperosmolarsolutions.5,6
The movement ofarms,head, neck,andtrunk
exacer-bated by the large anatomicvariations in the VCS length
maycausethecathetermigration,1,5,15soitmustbesecurely
fixedtotheskin.
Several anatomical landmarks have traditionally been
usedtoassesstheproperfinalpositionofthecathetertip
usingradiologicalcontrol.1,5,9,17---21However,althoughthere
isnoconsensusonitspositionintheSVC, itsintracardiac
locationshouldcertainlybeavoidedbecauseitisassociated
withhighermortality.11
Regarding diagnosis, 36% of the CT secondary to CVC
placement occur within the first 24h,1,3,7 which suggests
thattheperforationoccurred atthetimeofinsertionand
notbymigrationorerosion,and82%occurinthefirstweek
afterCVCplacement.1,3,7
The symptoms include chest or epigastrium pain or
discomfort, nausea, dyspnea, tachycardia, engorgement
of neck veins, paradoxical pulse, hypotension, low ECG
voltage, and increased cardiac silhouette.3 The classic
Beck’striad(hypotension,muffledheartsounds,andjugular
engorgement)isnotpresentinover29%ofcases,anddeath
fromcardiovascularcollapsemaybesuddenwith‘‘vague’’
signs/symptoms.1,5
InanypatientwithCVC,presentingwithchestpainand
anyoftheabovementionedsymptoms,aCTshouldbe
sus-pecteduntilprovenotherwise.3,9Atthisstage,anECGmay
notshowchanges;achestX-raywillshowchangesonlyifa
significantamountoffluidisaccumulatedinthepericardial
space;anechocardiogramthat,althoughadiagnostictest,
isnotalwayspromptlyavailable;oranyothertestthathelps
thediagnosismustbedismissedtoavoidtreatmentdelay.3,5
AsuccessfulCTapproachdependsonearlydiagnosisand
prompt and proper treatment. So, if the probable
diag-nosis of CT is admitted, the catheter infusion should be
immediatelystopped,3,5,9,16 theinfusioncontainermustbe
lowered below the level of the patient’s heart, and any
pericardialcontentmustbecarefullyaspiratedthroughthe
catheter.3,5,9 Note that thebackflow ofblood throughthe
CVCdoesnotexcludethe CTdiagnosis,particularlyifthe
CVCtipisalreadyinthepericardialspace.1CVCshouldbe
carefullyremoved3,5,9andanechocardiographyperformed.7
IfCPAisimminent,emergencypericardiocentesisshouldbe
performed5,9and,asalastresort,thoracotomy.3,5,9
In this clinical case, the catheter selection was
ade-quate(15cmflexiblepolyurethanecatheter);theprocedure
wasultrasound-guidedmonitoredwithECG,withoutcausing
arrhythmiabytheguidewire;andthebackflowofbloodwas
observedthroughthe threelumensofthecatheter,which
confirmed CVC position in the vascular system. However,
thechestX-rayperformedintheimmediatepostoperative
periodshowedthecathetertipwithintheheart,butasit
wasan anteroposteriorincidenceandtechnicalconditions
were bad, the findingwas underestimated. The catheter
permanencefor17daysinananomalousposition(possiblyin
RA),inapatientwithpolymalformativesyndromeand
sev-eralprevioussurgeries,resultedintheCTbyanincreasing
mechanicalerosionmechanism and migrationtothe
peri-cardialspace. Although the causes ofpericardial disease,
andconsequently CT,arevery diverse,22 inthis case
see-ing the catheter tip in the pericardial space defined the
etiologic diagnosis of CT. There were no objective
clini-cal,analyticalor imagingcriteriatosupportother causes
ofsubacuteCT,especiallycomplicationsfrommedical
con-ditions, such as infectious pericarditis, acute myocardial
infarction(Dressler’s syndrome), congestiveheart failure,
uremia,inflammatoryboweldisease,hypothyroidism,
con-nective tissue disease, metastases, or drug side effects
(procainamide, isoniazid, hydralazine, minoxidil,
pheny-toin,anticoagulants,methysergide).23
Interestingly,amulticenterUSstudy11 ofintensivecare
units found intracardiac placement of CVC tip in 47% of
patientsandthattheCVCpositionwasnotcorrectedafter
thechestX-ray.Thesenumbersandourreportedcasealert
usfor a careful consideration of the control X-rays after
CVCplacement,inordertodetectanomalouspositionsand
effectivelycorrectitaftervisualization.
However, we consider that the importance of the
cathetertipexactpositioninthechestradiographyis
over-estimated in the literature, because no position will be
realisticinanteroposteriorradiographsandevenifpatients
areimmobile,thephysiological movementsofthecardiac
andrespiratorycyclemaychangethecathetertipposition
In fact, there is no evidence in the literature that
radiography can prevent late complications such as CT.9
Moreover, we advocate that the CVC position should be
confirmed by radiography and should be reviewed
when-everchestX-raysareperformedfor otherreasons,mainly
to prevent intracardiac placement and hidden catheter
migration.
Conclusion
The selection of moreflexible andshort cathetersshould
be an option. Real-time ultrasound reduces the number
of complications associated with the technique, but it
does not allow the catheter tip view or prevent late
complications. Fluoroscopy and endocardialECG, if
avail-able, are effective methods to identify the catheter tip
initialpositionat thebedside,butshouldnotdismiss
con-trolradiographs.Radiologicconfirmationofthecathetertip
position is an important measure toprevent intracardiac
placement,but itdoes notguaranteethatvesselor heart
wall erosionor migration occur, so its position shouldbe
reviewed whenever chest X-rays are performed for other
reasons.The backflow of blood throughlumensshouldbe
checkedwheneverfluidsor drugs areinfusedthroughthe
catheter.
CTshould beconsidered in allpatients withCVC,
pre-senting withdeterioration in their clinical condition. The
keytotherapeuticsuccess dependsonearlyclinical
suspi-cion,and echocardiography is a surplus in confirming the
diagnosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.FernándezCG,BorregánJCR,RicoRF,et al.Tamponamiento cardíaco trascambio de catéter venoso central, sobre guía, paranutriciónparenteraltotal.Lopodemosevitar?NutrHosp. 2013;18:46---50.
2.KimMH,LeeD,KimMC.Bilateralhydrothoraxandcardiac tam-ponade afterright subclavianvein catheterization.Korean J Anesthesiol.2010;59:S211---7.
3.Karnauchow PN. Cardiac tampon de from central venous catheterization.CMAJ.1986;135.
4.Figuerola M, Tomás MT, Armengol J, et al. Pericardial tam-ponadeandcoronarysinusthrombosisassociatedwithcentral venouscatheterization.Chest.1992;101:1154---5.
5.BoothSA,NortonB,MulveyDA.Centralvenouscatheterization andfatalcardiactamponade.BJA.2001;87:298---302.
6.SilveiraL.Tamponamentocardíacoporcateterismovenoso cen-tral.RevPortuguesaCirurgia.2009;9:55---8.
7.Greenspoon JS, Masaki DI, Kurz CR. Cardiac tamponade in pregancy during central hyperalimentation. Obstet Gynecol. 1989;73:465.
8.DominoKB,BowdleTA,PosnerKL,etal.Injuriesandliability relatedtocentralvascularcatheters:aclosedclaimsanalysis. Anesthesiology.2004;100:1411---8.
9.Askegard-GiesmannJR,CanianoDA,KenneyBD.Rarebut seri-ouscomplicationsofcentrallineinsertion.SeminPediatrSurg. 2009;18:73---83.
10.PracticeGuidelinesforcentralvenousaccess:areportbythe American Society of Anesthesiologists task force on central venousaccess.Anesthesiology.2012;116.
11.McGeeWT,AckermanBL,RoubenLR,etal.Malpositionof cen-tralvenouscatheters:aprospective,randomized,multicenter trial.CritCareMed.1993;21:1118---23.
12.Guidanceontheuseofultrasoundlocatingdevicesforplacing centralvenouscatheters:recommendationsofNational Insti-tute for Clinical Excellence. Technology Appraisal Guidance No.49.Reviewin2005.
13.Guidelines for performing ultrasound guided vascular can-nulation: recommendations of the American Society of Echocardiographyand theSocietyofCardiovascular Anesthe-siologists.JAmSocEchocardiogr.2001;24:1291---318.
14.RaymondosK,PanningB.Howtoavoidfatalcomplicationsafter centralvenouscatheterization.BJA.2002;88:147---54.
15.YavascaogluB, YilmazlarA, KorfaliG,et al.Pericardial tam-ponade as a delayed lethal complication of central venous catheterization.EJA.2001;18:487---9.
16.Suddleson EA. Cardiac tamponade: a complication of cen-tral venous hyperalimentation. J Parenter Enteral Nutr. 1986;10:528.
17.GreenallMJ,BlewittRW,McMahonMJ.Cardiactamponadeand centralvenouscatheters.BrMedJ.1975;2:595---7.
18.RutherfordJS,MerryAF,OccleshawCJ.Depthofcentralvenous catheterization:anauditofpracticeinacardiacsurgicalunit. AnaesthIntensiveCare.1994;22:267---71.
19.Schuster M, Nave H, Piepenbrock S, et al. The carina as a landmarkincentralvenouscatheterplacement.BrJAnaesth. 2000;85:192---4.
20.AlbrechtK,NaveH,BreitmeierD,etal.Appliedanatomyofthe superiorvenacava---thecarinaasalandmarktoguidecentral venouscatheterplacement.BrJAnaesth.2004;92:75---7.
21.UchidaY,SakamotoM,TakahashiH,etal.Optimalpredictionof thecentralvenouscatheterinsertiondepthonaroutinechest X-ray.Nutrition.2011;27:557---60.
22.Spodick DH. Acute cardiac tamponade. N Engl J Med. 2003;349:684---90.