www.jped.com.br
ORIGINAL
ARTICLE
Sensitivity
and
specificity
of
different
measures
of
adiposity
to
distinguish
between
low/high
motor
coordination
夽
Luís
Lopes
a,b,∗,
Rute
Santos
a,c,
Carla
Moreira
a,
Beatriz
Pereira
b,
Vítor
Pires
Lopes
daResearchCentreforPhysicalActivity,HealthandLeisure(CIAFEL),FacultyofSports,UniversidadedoPorto(UP),Porto,
Portugal
bResearchCentreonChildStudies(CIEC),InstituteofEducation,UniversidadedoMinho,Braga,Portugal cInstitutoUniversitáriodaMaia,Maia,Portugal
dResearchCenterinSportsSciences,HealthSciencesandHumanDevelopment(CIDESD),DepartmentofSportsScienceof
InstitutoPolitécnicodeBraganc¸a,Braganc¸a,Portugal
Received12September2013;accepted25April2014 Availableonline7September2014
KEYWORDS
Adiposity;
Motorcoordination; KTK;
Cardiorespiratory fitness;
Children
Abstract
Objective: This study aimedto determinethe abilityof differentmeasures ofadiposity to
discriminatebetweenlow/highmotorcoordinationandtoevaluatetherelationshipbetween differentmeasuresofadiposityandmotorcoordination.
Methods: Thisstudyincluded596elementaryschoolchildrenaged9to12years(218females
---47.1%).Weight,height,andwaistcircumferencewereobjectivelymeasuredbystandardized protocols.Bodyfatpercentagewasestimatedbybioelectricimpedance.Bodymassindexand waist-to-heightratiowerecomputed. Motorcoordinationwasassessedby the Körperkoordi-nationTestfürKinder.Cardiorespiratoryfitnesswaspredictedbyamaximalmultistage20m shuttle-runtestoftheFitnessgramTestBattery.Aquestionnairewasusedtoassessthematernal educationallevel.
Results: The receiver operating characteristic performance of body fat percentage in
femalesand waist circumference inmales presented aslightly better discriminatory accu-racy than body mass index, waist circumference and waist-to-height ratio in predicting low motor coordination. After adjustments, logistic regression analyses showed that body mass index (=2.155; 95%CI: 1.164-3.992; p=0.015 for girls; =3.255; 95% CI: 1.740-6.088;p<0.001formales), waistcircumference (=2.489;95%CI:1.242-4.988;p=0.010 for girls; =3.296; 95%CI:1.784-6.090; p<0.001 for males), body fat percentage (=2.395;
夽
Pleasecitethisarticleas:LopesL,SantosR,MoreiraC,PereiraBL,LopesVP.Sensitivityandspecificityofdifferentmeasuresofadiposity todistinguishbetweenlow/highmotorcoordination.JPediatr(RioJ).2015;91:44---51.
∗Correspondingauthor.
E-mail:[email protected](L.Lopes).
http://dx.doi.org/10.1016/j.jped.2014.05.005
95%CI:1.234-4.646;p=0.010forgirls;=2.603;95%CI:1.462-4.634;p<0.001formales)and waist-to-heightratio(=3.840;95%CI:2.025-7.283;p<0.001 formales)werepositively and significantlyassociatedwithmotorcoordinationinbothsexes,withtheexceptionof waist-to-heightratioingirls(=1.343;95%CI:0.713-2.528;p=0.381).
Conclusion: Bodyfatpercentageandwaistcircumferenceshowedaslightlybetter
discrimina-toryaccuracyinpredictinglowmotorcoordinationforfemalesandformales,respectively. ©2013SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Adiposidade;
Coordenac¸ãomotora; KTK;
Capacidade cardiorrespiratória; Crianc¸as
Sensibilidadeeespecificidadedediferentesmedidasdeadiposidadepara diferenciac¸ãoentrepouca/amplacoordenac¸ãomotora
Resumo
Objetivo: Esteestudo pretende:(i)determinaracapacidadede diferentesmedidasde
adi-posidadeparadiferenciarpouca/amplaCM;e(ii)avaliararelac¸ãoentrediferentesmedidasde adiposidadeecoordenac¸ãomotora.
Método: 596crianc¸asem idadeescolarfundamental,de9a12anos(218meninas---47,1%)
participaramdesteestudo.Opeso,aalturaeacircunferênciadacinturaforammensurados objetivamentepelosprotocolospadronizados.Opercentualdegorduracorporalfoiestimado pela impedância bioelétrica. Foram calculados o índice de massa corporal e a razão cin-tura/estatura.Acoordenac¸ãomotorafoiavaliadapormeiodotestedecoordenac¸ãocorporal paracrianc¸as.Acapacidadecardiorrespiratóriafoipreditaporumtesteshuttle-runmultinível denomáximo20mdaBateriadeTestesFitnessgram.Foiusadoumquestionárioparaavaliaro níveldeescolaridadedasmães.
Resultados: Odesempenhonacurvadecaracterísticadeoperac¸ãodoreceptordopercentual
degorduracorporal,emmeninas,edacircunferênciadacintura,emmeninos,demonstrouuma precisãodiscriminatórialevementemelhorqueoíndicedemassacorporal,acircunferênciada cintura earazãocintura/estaturaem predizerpoucacoordenac¸ãomotora.Apósajustes,as análisesderegressãologísticademonstraramqueoíndicedemassacorporal(=2,155; Inter-valodeConfianc¸a(IC)95%:1,164-3,992;p=0,015parameninas;=3,255;IC95%:1,740-6,088; p<0,001parameninos),acircunferênciadacintura(=2,489;IC95%:1,242-4,988;p=0,010 parameninas;=3,296;IC95%:1,784-6,090;p<0,001parameninos),opercentualdegordura corporal(=2,395;IC95%:1,234-4,646;p=0,010parameninas;=2,603;IC95%:1,462-4,634; p<0,001parameninos)earazãocintura/estatura(=3,840;IC95%:2,025-7,283;p<0,001para meninos)estavampositivaesignificativamenterelacionadosàcoordenac¸ãomotoraemambos ossexos,comexcec¸ãodarazãocintura/estaturaemmeninas(=1,343;IC95%:0,713-2,528; p=0,381).
Conclusão: Opercentual degordura corporale acircunferênciada cinturamostraram uma
precisãodiscriminatórialigeiramentemelhornaprevisãodepoucacoordenac¸ãomotorapara meninasemeninos,respectivamente.
©2013SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Childhood and adolescent obesity has become an impor-tantpublichealthproblem,asitsprevalencehasincreased significantlyoverthepastyearsinseveralcountries.1In Por-tugal,approximatelyone-thirdofchildrenandadolescents areoverweightorobese.2
An appropriatemotor coordination(MC) level is essen-tialforchildren’shealthygrowthanddevelopment,aswell asfor psychosocial skills andwell-being.3,4 Although rudi-mentary forms of movement patterns may naturally be developed, mature forms of motor proficiency are more likely to be achieved with appropriate practice, encour-agement, feedback,and instruction.5 The early childhood
yearsarea keytime for thedevelopment ofthese skills, whichareconsideredthebuildingblocksofmorecomplex movements.6
insixofninestudies,andtheremainingthreedemonstrated norelationship. For example, D’Hondt et al.,11 in a two-yearlongitudinalstudy,investigatedtheshort-termchange inthelevelofgrossMCaccordingtochildren’sweightstatus, andconcludedthatparticipantsinthenormalweightgroup showedmoreprogress thantheiroverweight/obesepeers, whodemonstratedsignificantlypoorerperformances.
There are some sophisticated methods to accurately measure body fat percentage, such as computed axial tomographyor dual-energy X-ray absorptiometric densito-metry;however,itisnotfeasibletoapplysuchtechniques inlargeepidemiologicalstudiesoreveninclinicalsettings becausetheyarecomplex,time-consuming,andexpensive. Therefore, several anthropometric measures, indices and othertechniques(suchasbioelectricimpedance)havebeen usedintheliteratureontheassociationbetweenadiposity andMC,andthemostcommonisthebodymassindex(BMI). Nevertheless,waistcircumferenceandwaist-to-heightratio measuresofcentralobesityhaveyieldedimportantinsight inpediatricpopulations12aswell,andappearstobestronger predictors of cardiovascular risk among children.13 In a recentsystematicreview,Rivilisetal.14concludedthatan adversebodycompositionwasassociatedwithpoormotor proficiencyregardless of themeasure ofadiposity consid-ered.
However,thegapthatremainsintheliteratureisonthe abilityofthedifferentmeasuresofweightstatus/adiposity to predict low MC, namely which is the most accurately non-laboratorymeasure of adipositythat better identifies low/highMC.Therefore,theaimsofthisstudywere(i)to determinetheability(sensibilityandspecificity)of differ-entmeasuresofadiposity:BMI,waistcircumference,body fat percentage, and waist-to-height ratio to discriminate betweenlow/highMC;and(ii)toevaluatetherelationship between BMI, waist circumference, waist-to-height ratio, andfat mass percentageand MC,in asample of children aged9-12years.The studyattempts toanswer two ques-tions:whatis themost accurate(resultfromthebalance betweensensitivityandspecificity)nonlaboratorymeasure ofadipositytodistinguishbetweenhigh/lowMC?AnddoBMI, waist circumference, waist-to-height ratio, and fat mass percentagepredict MC?This study willallow for monitor-ingandcomparing,andwillcontributetotheconstruction ofnewknowledge throughtheexploration ofassociations between these four non-laboratory measures of adiposity andMC.
Methods
Data for the present study derived from the Bracara Study, which aimed to evaluate the relations between MC, physical activity, physical fitness, body composition, academic achievement, and health behaviors among ele-mentaryschoolchildren.TheBracaraStudywasconducted in a middle city located in the north of Portugal during the2009/2010academicyear.Studydesign,sampling,and measuresarereportedelsewhere.15
StudyDesignandSampling
All 21 urban public elementary schools in the city were considered and invited to participate in this study,
correspondingto846childrenenrolledinthefourthgrade. Two schools declined the invitation, corresponding to 90 children;sixschoolscouldnotbeevaluatedintimetotake part in this study, corresponding to 130 children; and 30 children who failed the inclusion criteria (having a men-taland/orphysicaldisabilityorahealthconditionthatdid notallowthemtoparticipateinphysicaleducationclasses) orwhohadmissinginformationonthevariablesofinterest wereexcludedfromthisanalysis.Therefore,thefinal sam-ple included 596 participants (281females ---47.1%) aged 9-12years.
Theschools’directorsandchildren’sparents/guardians receivedverbal andwritten descriptionsof thestudy and signed an informedconsent.The protocol andprocedures employedfollowedtheHelsinkiDeclarationforInvestigation in Human Subjects andwere approved by the Portuguese MinistryofEducationandbytheUniversity’sEthics Commit-tee.
Alldatawascollectedduringregularlyscheduledphysical educationclassesbytwofull-timeassessors,whowere phys-icaleducationteachersandreceivedspecifictraining,and had already participated in previous anthropometry, Kör-perkoordination Testfür Kinder(KTK),and aerobicfitness datacollection.Theywerehelpedbythephysicaleducation teachersoftheschoolsenrolledinthisstudy.Thedatawere collected at the same time and the agreement between thesetwoassessorswastestedinapreviousdatacollection showinggoodresults(datanotpublished).
Measures
Anthropometry
Weight wasmeasured tothe nearest 0.1kgusing a regu-larly calibrated digital scale, model TBF-300 (Tanita, São Paulo,Brazil)withthechildreninlightclothingandwithout shoes. Body fat percentage was estimated by a bioelec-tric impedance digital scale, model TBF-300 (Tanita, São Paulo, Brazil). Height was measured to the nearest mil-limeterinbareorstockingfeetwiththechildrenstanding uprightagainstastadiometer,model220(Seca,SãoPaulo, Brazil).Waistcircumferencemeasurementsweretakenwith anon-elastictapeasdescribedbyLohmanetal.16BMI[body mass (kg)/height (m2)] and waist-to-height ratio [waist (cm)/height(cm)]werecalculated.
MC
ThebodycoordinationtestKTKwasusedtoassessMC.17The KTKbatteryhasfouritems:balance;jumpinglaterally; hop-pingononelegoveranobstacle;andshiftingplatforms.The testswereappliedfollowingtheoriginalprotocolsdescribed elsewhere.15 Forthisstudy,participantsweredividedinto two categories according to their MC quotient: high MC (those with normal, good, or very good MC) and low MC (insufficientMCandMCdisorders).Theterminologyusedin thispaperisinagreementwiththemostrelevantandrecent literatureonthissubject.4,8,15,18---20
CardiorespiratoryFitness
Table1 Participants’characteristics.
All (n=596)
Females (n=281)
Males (n=315)
pa
Age(years) 9.7±0.6 9.7±0.5 9.7±0.6 0.552
BMI(kg/m2) 18.6±3.3 18.6±3.3 18.6±3.3 0.934
Waistcircumference(cm) 66.8±8.6 66.3±8.74 67.2±8.74 0.215 Waist-heightratio 0.48±0.05 0.48±0.06 0.49±0.05 0.149 Bodyfatpercentage(%) 19.7±8.3 21.4±8.9 18.3±7.4 <0.001 Motorcoordination(motorquotient) 85.7±14.4 81.7±14.5 89.3±13.4 <0.001
BMI,bodymassindex(kg/m2).
a Student’st-testtocomparegenderdifferences.
Sociodemographics
Maternaleducationallevelwasassessedbyaquestionnaire distributedtothemothersoftheparticipantsinthisstudy andwasusedasaproxymeasureofsocioeconomicstatusas previously appliedin Portuguese studies. The educational level wascategorizedaccording tothePortuguese Educa-tionLevelin2009:low(mandatoryeducation---nineschool years); medium (secondary education --- 12 school years); andhigh(collegeoruniversitydegree).
Statistical
analysis
Student’st-testforcontinuousvariableswasusedfor com-parisonsbetweengroups.Receiveroperatingcharacteristic (ROC)curveswereusedtoanalyzethepotentialdiagnostic accuracyofthedifferentmeasuresofadiposityto discrim-inate between low and high MC (best trade-off between sensitivity and specificity of different adiposity measures thatbestdifferentiatebetweenhighandlowMC).Thearea under the ROC curve (AUC) represents the ability of the test tocorrectly classifytheparticipants withhigh orlow MC.AUCvaluesrangebetween1(aperfecttest)and0.5(a inadequatetest).
In a preliminary analysis, the variables ‘‘school’’ and ‘‘teacher’’werenotsignificantlycorrelatedwithchildren’s MC,physicalfitness,orbodycomposition,andtherewere nosignificantdifferencesinthemeanvaluesofMC,physical fitness,orbodycompositionbetween schoolsor teachers. Therefore,multilevelanalysiswasnotperformedandthese variableswerenotusedaspotentialconfounders.In Portu-gal,thereisamandatorycurriculumforschools(schooland teacher are not allowed tointroduce different subjects); furthermore, the ‘‘type of the school’’ (i.e. the type of buildingandthespacesavailableforoutdooractivities dur-ingrecess)inthisstudywassimilar.Thosemaybepossible explanationsforthelack ofassociations.Therefore, logis-ticregressionanalyseswereperformedtofurtherstudythe relationship between different measures of adiposity and MC.Adjustmentswereperformedforpotentialconfounders: cardiorespiratoryfitnessandmaternaleducationlevels.In thisanalysis,giventhatthemotorquotientofeach partici-pantwascalculatedbasedonthescoresattainedbyageand gender,nofurtheradjustmentsforagewereperformed.
Data were analyzed using the IBM SPSS Statistics v.19 (SPSS,Inc.IBMCompany,NewYork,USA)andMedCalc sta-tisticalsoftware(MedCalcsoftware,Mariakerke,Belgium). Ap-valueunder0.05denotedstatisticalsignificance.
Results
Descriptivestatisticsfortheage,BMI,waistcircumference, bodyfatpercentage,waist-to-heightratio,andMCare sum-marizedinTable1.FemaleshadsignificantlylowerMCand higherbodyfatpercentagethanmales(p<0.001forboth). 169females(28.4%)and138males(23.1%)wereclassified hashaving lowMC, whereas112 females (18.8%)and 177 males(29.7%)wereclassifiedashavinghighMC.
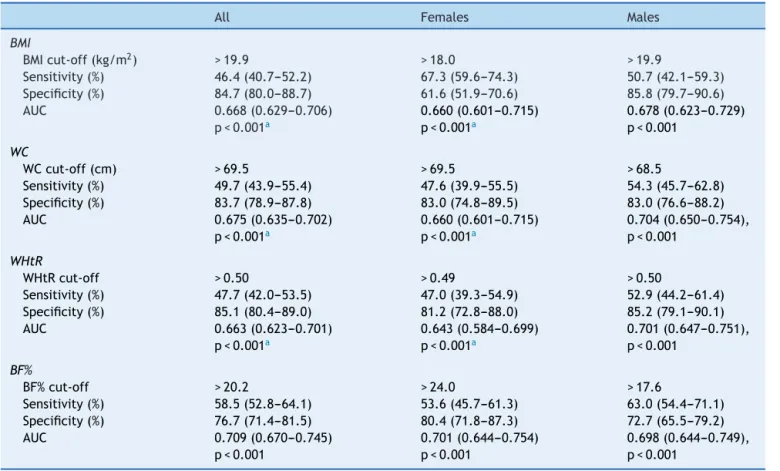
ROCcurveanalysisshowedthatallmeasuresof adipos-ity performed well on average in identifying low MC, as indicated byAUC>0.6. The ROC performanceof body fat percentage showed a slightly better discriminatory accu-racythandidBMI,waistcircumferenceandwaist-to-height ratioin predicting low MCin females. In males, the ROC performanceof waistcircumference showeda better dis-criminatoryaccuracy than BMI, body fat percentage, and waist-to-height ratio in predicting low MC.In males, the ROCperformanceofBMI,waistcircumference,and waist-to-heightratiowereslightlybetterthaninfemales.TheAUC ofBMI,waistcircumference,andwaist-to-heightratiowere significantlydifferent from bodyfat percentage (p<0.05) forthewholesample andfor females.Thefollowingwere observedtobeoptimal cut-offsfor defining lowMC:BMI, 18.0kg/m2and19.9kg/m2;waistcircumference,69.50cm and68.50cm;bodyfatpercentage,24.0%17.60%;and waist-to-heightratio of0.497 and0.50, for females andmales, respectively.(Table2).
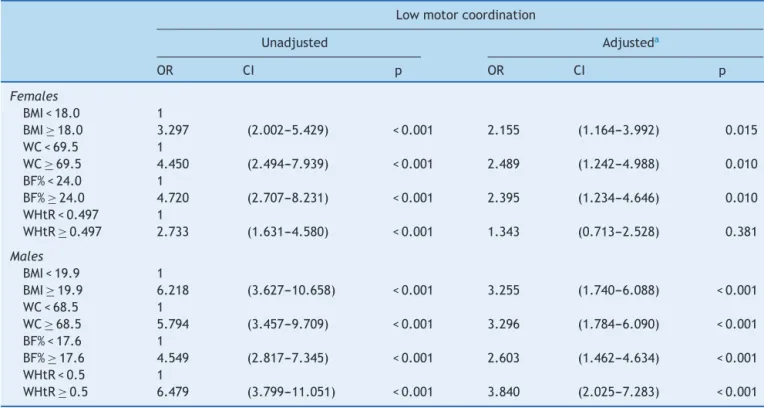
LogisticregressionanalysesshowedthatBMI,waist cir-cumference,bodyfatpercentage,andwaist-to-heightratio werepositivelyandsignificantlyassociatedwithlowMCin bothsexes,withtheexceptionofwaist-to-heightratioafter adjustmentsforfemales(Table3).
Discussion
Table2 Cut-offvalues,sensitivity,andspecificityfortheassociationofdifferentmeasuresofadipositywithmotorcoordination bysex.
All Females Males
BMI
BMIcut-off(kg/m2) >19.9 >18.0 >19.9
Sensitivity(%) 46.4(40.7---52.2) 67.3(59.6---74.3) 50.7(42.1---59.3) Specificity(%) 84.7(80.0---88.7) 61.6(51.9---70.6) 85.8(79.7---90.6) AUC 0.668(0.629---0.706)
p<0.001a
0.660(0.601---0.715) p<0.001a
0.678(0.623---0.729) p<0.001
WC
WCcut-off(cm) >69.5 >69.5 >68.5
Sensitivity(%) 49.7(43.9---55.4) 47.6(39.9---55.5) 54.3(45.7---62.8) Specificity(%) 83.7(78.9---87.8) 83.0(74.8---89.5) 83.0(76.6---88.2)
AUC 0.675(0.635---0.702)
p<0.001a
0.660(0.601---0.715) p<0.001a
0.704(0.650---0.754), p<0.001
WHtR
WHtRcut-off >0.50 >0.49 >0.50
Sensitivity(%) 47.7(42.0---53.5) 47.0(39.3---54.9) 52.9(44.2---61.4) Specificity(%) 85.1(80.4---89.0) 81.2(72.8---88.0) 85.2(79.1---90.1)
AUC 0.663(0.623---0.701)
p<0.001a
0.643(0.584---0.699) p<0.001a
0.701(0.647---0.751), p<0.001
BF%
BF%cut-off >20.2 >24.0 >17.6
Sensitivity(%) 58.5(52.8---64.1) 53.6(45.7---61.3) 63.0(54.4---71.1) Specificity(%) 76.7(71.4---81.5) 80.4(71.8---87.3) 72.7(65.5---79.2)
AUC 0.709(0.670---0.745)
p<0.001
0.701(0.644---0.754) p<0.001
0.698(0.644---0.749), p<0.001
AUC,areaunderthecurve;BMI,bodymassindex(kg/m2);WC,waistcircumference(cm);BF%,bodyfatpercentage;WHtR,waist(cm)
toheight(cm)ratio;95%ConfidenceIntervalsinparentheses.
aAUCsignificantlydifferentfromBF%(p<0.05).
adipositywerenegativelyandsignificantlyassociatedwith MCinbothsexes,withtheexceptionofwaist-to-heightratio forfemales,afteradjustingforcardiorespiratoryfitnessand maternaleducationlevel.
A recent review of the associations between MC and aspects of physical and psychological attributes provides indirectevidencethatMCmaybeanimportantantecedent or consequent mechanism for promoting health-related behaviors, including weight status.10 However, measure-ment issues may potentially play a role in obscuring the relationshipbetweenbodycompositionandMC.14
In the present study, body fat percentage assessed by bioelectric impedance was the measure that best pre-dictedlowMCinfemales.Bodyfatpercentagemeasurement techniques have been developed and validated for chil-dren;however,theyhaverarelybeenusedintheliterature regardingtherelationship betweenadiposity andMC.The existingstudieshavefoundsignificantassociationsbetween body fat percentage and MC, whether using skin folds,9 bioelectric impedance22 or whole body air displacement plethysmography methods.23 Usingbioelectric impedance, Cairneyetal.,22 alsofoundthatchildrenwithpoorMChad greater bodyweightand bodyfat compared totheir nor-malMC peers.Bioelectricimpedance is an appealing tool forassessingbodycompositionduetothefactthatitis sim-ple,painless,non-invasive,andincreasinglycheap,making ithighly suitablefor surveyandclinic use, particularlyin
school-agechildren.24 However,theresultingestimates of fatandfat-freemassareinpooragreementwithmore accu-ratemethods,tendingtobebothbiasedandimprecise.25
BMIisthemostcommonanthropometricmeasureusedin studies relatingtoadiposity statusandMC.10,14 In a cross-sectional study with954 Flemishstratified primaryschool children,D’Hondtetal.,8observedthatlessthan20%ofthe healthy-weightparticipants wasidentified asbeing motor impaired,whilethatproportionincreasedto43.3%andupto 70.8%inchildrenwithoverweightandobesity,respectively. BMIisasuboptimalmarkerofbodyfatbecauseitdoesnot distinguishfatfromleantissueorbone;therefore, classify-ingpeopleasoverweightorobesebasedontheirBMIalone mayleadtosignificantmisclassification.Moreover,BMIisnot asuitablemethodtoassessbodyfatdistribution,26andithas beensuggestedthatBMImaybealesssensitiveindicatorof fatinchildrenandadolescentsthanwaistcircumferenceor waist-to-heightratio.26
Table3 Oddsratiosand95%confidenceintervalsfromlogisticregressionmodelpredictinglowmotorcoordination,forbody massindex,waistcircumference,waist-to-heightratio,andfatmasspercentage,bysex.
Lowmotorcoordination
Unadjusted Adjusteda
OR CI p OR CI p
Females
BMI<18.0 1
BMI≥18.0 3.297 (2.002---5.429) <0.001 2.155 (1.164---3.992) 0.015 WC<69.5 1
WC≥69.5 4.450 (2.494---7.939) <0.001 2.489 (1.242---4.988) 0.010 BF%<24.0 1
BF%≥24.0 4.720 (2.707---8.231) <0.001 2.395 (1.234---4.646) 0.010 WHtR<0.497 1
WHtR≥0.497 2.733 (1.631---4.580) <0.001 1.343 (0.713---2.528) 0.381
Males
BMI<19.9 1
BMI≥19.9 6.218 (3.627---10.658) <0.001 3.255 (1.740---6.088) <0.001 WC<68.5 1
WC≥68.5 5.794 (3.457---9.709) <0.001 3.296 (1.784---6.090) <0.001 BF%<17.6 1
BF%≥17.6 4.549 (2.817---7.345) <0.001 2.603 (1.462---4.634) <0.001 WHtR<0.5 1
WHtR≥0.5 6.479 (3.799---11.051) <0.001 3.840 (2.025---7.283) <0.001
BMI,bodymassindex(kg/m2),WC,waistcircumference(cm);BF%,bodyfatpercentage;WHtR,waist(cm)toheight(cm)ratio;OR,
oddsratio;CI,confidenceintervals.
a Adjustedforcardiorespiratoryfitnessandmothers’educationlevels.
developedforchildrenandadolescentsinsomecountries.29 Abdominalobesity appears toreflectintra-abdominal fat, including visceral adipose tissue,30 and it is known that increasedvisceraladiposetissueisstronglycorrelatedwith cardiovasculardiseaseriskfactors.31 Duringchildhoodand adolescence,abdominal obesity is an important predictor forseveralcardiovasculardiseaseriskfactors.13 Indeed,in across-sectionalstudywith571elementaryschoolstudents, Faughtetal.32 foundanassociationbetweenpoorMCwith increasedbodyfatandlowcardiorespiratoryfitness--- physi-calactivitywasasignificantmediatorforbothrelationships. TheseauthorsconcludedthatpoorMCisrelatedtofactors associatedwithincreasedriskforcoronaryvasculardisease, includingdecreasedcardiorespiratoryfitnessandincreased bodyfatthroughthemediatinginfluenceofphysicalactivity inchildren.
Waist-to-heightratiohasbeenproposedasaconvenient alternative measurement to assess central fatness in children.13 Similartowaistcircumference,waist-to-height ratiohasbeenshowntobestronglycorrelatedwith abdom-inal fat measured using imaging techniques.31 Correcting waist circumference to height may obviate the need for age-, sex-, and ethnic-related reference values,33 while waist circumference requires population-specific cut-off values.34 To the best of the authors’ knowledge, there are nostudies linking waist-to-height ratio and MC; how-ever, the good AUC found in this study may suggest that waist-to-heightratiois agoodmeasurefor predictinglow MC.
Strengthsandlimitations
Thisstudyhassomelimitationsthatneedtoberecognized. The data has been derived from a cross-sectional study; thereforetheresultsdonotindicatecausality.Thepresent sampleisnotrepresentativeofthePortuguesepopulation; therefore,thepresentfindingsarenotgeneralizable.
Overall,thestrengthsofthepresentstudyarethatthe presentfindingsarebasedonobjectivemeasurementsusing reliableandvalidtestinstruments(theKTK);theinclusion ofpotentialconfoundingfactorssuchasmaternaleducation level (usedasa proxy measure of socioeconomicstatus), which is recognized ashaving a powerful and synergistic relationshipwithobesity;35 thepresence of cardiorespira-tory fitness as a potential confounding element, due to its importance of being simultaneously linked to adipos-ity and MC (i.e., inversely associated with adiposity and positivelyrelatedtoMC);9,32 andthenoveltyof thestudy, which aimed to determine the ability of different meas-ures of adiposity to discriminate between low and high MC.
More research on other measures and techniques is neededtofurtherassesstheaccuracyofdifferentmeasures ofadiposityindiscriminatingbetweenlowandhighMC.
bothsexes, withthe exception ofwaist-to-height ratioin femalesafteradjustments.
Funding
Portuguese FCT-MEC (Fundac¸ão para a Ciência e a Tecnologia-MinistériodaEducac¸ãoe Ciência)grant [Doc-toralScholarship/43808/2008].
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The first author was supported by a Portuguese FCT-MEC grant[DoctoralScholarship/43808/2008].
References
1.WangY,LobsteinT.Worldwidetrendsinchildhoodoverweight andobesity.IntJPediatrObes.2006;1:11---25.
2.SardinhaLB,SantosR,ValeS,SilvaAM,FerreiraJP,Raimundo AM, et al. Prevalence of overweight and obesity among Portugueseyouth: a studyina representative sampleof 10-18-year-old children and adolescents. Int J Pediatr Obes. 2011;6:e124---8.
3.PiekJP,BaynamGB,BarrettNC.Therelationshipbetweenfine andgrossmotorability,self-perceptionsandself-worthin chil-drenandadolescents.HumMovSci.2006;25:65---75.
4.HagaM.Physicalfitnessinchildrenwithhighmotorcompetence isdifferentfromthatinchildrenwithlowmotorcompetence. PhysTher.2009;89:1089---97.
5.Gallahue DL, OzmunJC. Understanding motor development: infants, children, adolescents, adults. Boston: McGraw Hill; 2006.
6.ClarkJE,MetcalfeJS.Themountainofmotordevelopment:a metaphor.In:ClarkJE,HumphreyJH,editors.Motor develop-ment:researchandreviews.Reston,VA:NASPEPublications; 2002.p.163---90.
7.OkelyAD,BoothML,CheyT.Relationshipsbetweenbody compo-sition and fundamental movement skills amongchildren and adolescents.ResQExercSport.2004;75:238---47.
8.D’HondtE,DeforcheB,VaeyensR,VandorpeB, Vandendriess-cheJ, Pion J,et al.Grossmotor coordinationin relationto weight statusand age in5- to12-year-old boys and girls:a cross-sectionalstudy.IntJPediatrObes.2011;6:e556---64. 9.Lopes VP, Maia JA, Rodrigues LP, Malina R. Motor
coordina-tion,physicalactivityandfitnessaspredictorsoflongitudinal changeinadiposityduringchildhood.EurJSportSci.2012;12: 384---91.
10.Lubans DR, Morgan PJ, Cliff DP, Barnett LM, Okely AD. Fundamental movement skills in children and adolescents: review of associated health benefits. Sports Med. 2010;40: 1019---35.
11.D’HondtE,DeforcheB,GentierI,DeBourdeaudhuijI,Vaeyens R,PhilippaertsR,etal.Alongitudinalanalysisofgrossmotor coordinationinoverweightandobesechildrenversus normal-weightpeers.IntJObes(Lond).2013;37:61---7.
12.Taylor RW, JonesIE, Williams SM,Goulding A. Evaluationof waistcircumference,waist-to-hipratio,andtheconicityindex asscreeningtoolsforhightrunkfatmass,asmeasuredby dual-energyX-rayabsorptiometry,inchildrenaged3-19y.AmJClin Nutr.2000;72:490---5.
13.SavvaSC,TornaritisM,SavvaME,KouridesY,PanagiA,Silikiotou N, et al. Waist circumference and waist-to-height ratio are betterpredictorsofcardiovasculardiseaseriskfactorsin chil-dren than body massindex. IntJ Obes RelatMetab Disord. 2000;24:1453---8.
14.Rivilis I, Hay J, Cairney J, Klentrou P, Liu J, Faught BE. Physicalactivity and fitness in children with developmental coordination disorder: a systematic review.Res Dev Disabil. 2011;32:894---910.
15.LopesL,SantosR,PereiraB,LopesVP.Associationsbetween sedentarybehaviorand motorcoordination inchildren.AmJ HumBiol.2012;24:746---52.
16.LohmanT,RocheA,MartorellR,editors.Anthropometric stan-dardizationreferencemanual.Champaign,IL:HumanKinetics; 1991.
17.SchilingF.KörperkoordinationTestfürKinder,KTK.BeltzTest Gmbh.Weinheim:1974.
18.Hardy LL, Reinten-Reynolds T, Espinel P, Zask A, Okely AD. Prevalenceandcorrelatesoflowfundamentalmovementskill competencyinchildren.Pediatrics.2012;130:e390---8. 19.WrotniakBH,EpsteinLH,DornJM,JonesKE,KondilisVA.The
relationshipbetweenmotorproficiencyandphysicalactivityin children.Pediatrics.2006;118:e1758---65.
20.InstituteofMedicine.Educatingthestudentbody:taking phys-icalactivityandphysicaleducationtoschool.Washington,DC: TheNationalAcademiesPress;2013.
21.WelkGJ,MeredithMD,editors.Fitnessgram/Activitygram Ref-erenceGuide.Dallas:TheCooperInstitute;2008.
22.CairneyJ,HayJA,FaughtBE,HawesR.Developmental coor-dinationdisorderandoverweightandobesityinchildrenaged 9-14y.IntJObes(Lond).2005;29:369---72.
23.SilmanA,CairneyJ,HayJ,KlentrouP,FaughtBE.Roleof phys-icalactivityandperceivedadequacyonpeakaerobicpowerin childrenwithdevelopmentalcoordination disorder.HumMov Sci.2011;30:672---81.
24.WrightCM,SherriffA,WardSC,McCollJH,ReillyJJ,NessAR. Developmentofbioelectricalimpedance-derivedindicesoffat andfat-freemassforassessmentofnutritionalstatusin child-hood.EurJClinNutr.2008;62:210---7.
25.EisenmannJC,HeelanKA,WelkGJ.Assessingbodycomposition among3-to8-year-oldchildren:anthropometry,BIA,andDXA. ObesRes.2004;12:1633---40.
26.Brambilla P,Bedogni G, Moreno LA, Goran MI, Gutin B, Fox KR,etal.Crossvalidationofanthropometryagainstmagnetic resonanceimagingfortheassessmentofvisceraland subcuta-neousadiposetissueinchildren.IntJObes(Lond).2006;30: 23---30.
27.CairneyJ,HayJ,VeldhuizenS,MissiunaC,MahlbergN,Faught BE.Trajectories of relative weight and waist circumference amongchildrenwithandwithoutdevelopmentalcoordination disorder.CMAJ.2010;182:1167---72.
28.LeeS,BachaF,GungorN,ArslanianSA. Waistcircumference isanindependentpredictorofinsulinresistanceinblackand whiteyouths.JPediatr.2006;148:188---94.
29.Fernández JR, Redden DT, Pietrobelli A, Allison DB. Waist circumference percentiles in nationally representative sam-ples of African-American. European-American, and Mexican-American children and adolescents. J Pediatr. 2004;145: 439---44.
30.ClaseyJL,BouchardC,TeatesCD,RiblettJE,ThornerMO, Hart-man ML, et al. The use of anthropometric and dual-energy X-rayabsorptiometry(DXA)measurestoestimatetotal abdom-inalandabdominalvisceralfatinmenandwomen.ObesRes. 1999;7:256---64.
and correlation with computed axial tomography. Nutrition. 2007;23:36---45.
32.Faught BE, Hay JA, Cairney J, Flouris A. Increased risk for coronary vascular disease in children with develop-mental coordination disorder. J Adolesc Health. 2005;37: 376---80.
33.Ashwell M, Hsieh SD. Six reasons why the waist-to-height ratioisarapidand effectiveglobalindicatorforhealthrisks of obesity and how its use could simplify the international
publichealthmessageonobesity.IntJFoodSciNutr.2005;56: 303---7.
34.World Health Organization, (WHO). Obesity: preventing and managingtheglobal,epidemic.,WHO.,TechnicalReportSeries 894.Geneva:WHO;2000.