w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Intra-articular
injection
with
triamcinolone
hexacetonide
in
patients
with
rheumatoid
arthritis:
prospective
assessment
of
goniometry
and
joint
inflammation
parameters
Rita
Nely
Vilar
Furtado
∗,
Flávia
Soares
Machado,
Karine
Rodrigues
da
Luz,
Marla
Francisca
dos
Santos,
Monique
Sayuri
Konai,
Roberta
Vilela
Lopes,
Jamil
Natour
UniversidadeFederaldeSãoPaulo,DisciplinadeReumatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received7December2015 Accepted1June2016
Availableonline6September2016
Keywords:
Rheumatoidarthritis Intra-articularinjections Triamcinolone
Improvement
a
b
s
t
r
a
c
t
Objectives: Toevaluatelocaljointvariablesafterintra-articularinjectionwithtriamcinolone hexacetonideinrheumatoidarthritispatients.
Methods:We blindly and prospectively (baseline, 1, 4, 12 and 24 weeks) evaluated metacarpophalangeal,wrist,elbow,shoulder,kneeandanklejointsaftertriamcinolone hex-acetonideintra-articularinjectionbythefollowingoutcomemeasures:visualanaloguescale 0–10cm(VAS)forrestpain(VASR);VASformovementpain(VASM);VASforjointswelling (VASSw);flexion(FlexG)andextension(ExtG).
Results:289patients(635joints)werestudied.VASSw(p<0.001)andVASR(0.001<p<0.016) improvedfromT0toT4,T12andT24foralljoints.VASMimprovedfromT0toT4(p<0.021) foralljoints;T0toT12(p<0.023)forMCFandknee;T0toT24(p<0.019)onlyforMCFand knee.FlexGimprovedfromT0toT4(p<0.001)foralljoints;T0toT12(p<0.001)andT0to T24(p<0.02)onlyforMCFandknee.ExtGimprovedfromT0toT4(p<0.001)foralljoints exceptforelbow;T0toT12(p=0.003)forwrist,metacarpophalangealandknee;andT0to T24(p=0.014)forMCFandknee.
Conclusion: VASSwrespondedbetteratshortandmediumtermafterIAIwithtriamcinolone hexacetonideinoursampleofRApatients.
©2016PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](R.N.Furtado).
http://dx.doi.org/10.1016/j.rbre.2016.08.001
Injec¸ão
intra-articular
de
hexacetonido
de
triancinolona
em
pacientes
com
artrite
reumatoide:
avaliac¸ão
prospectiva
da
goniometria
e
parâmetros
de
inflamac¸ão
articular
Palavras-chave:
Artritereumatoide Injec¸õesintra-articulares Triamcinolona
Melhoria
r
e
s
u
m
o
Objetivos: Avaliarvariáveisarticulareslocaisapósainfiltrac¸ãointra-articular(IIA)de hex-acetonidodetriancinolona(HT)empacientescomartritereumatoide(AR).
Métodos: Foramavaliadas,demodocegoeprospectivo(nostemposinicial,1,4,12e24 sem-anas),asarticulac¸õesmetacarpofalângica(MCF),punho,cotovelo,ombro,joelhoetornozelo apósaIIAdeHTutilizando-sedasseguintesmedidasdedesfecho:escalavisualanalógica (EVA)de0a10cmparadoremrepouso(EVAr);EVAparadoraomovimento(EVAm);EVA paraedemaarticular(EVAe);flexão(FlexG)eextensão(ExtG).
Resultados: Estudaram-se 289pacientes(635 articulac¸ões). A EVAe (p<0,001)e a EVAr (0,001<p<0,016)melhoraramdeT0aT4,T12eT24emtodasasarticulac¸ões.AEVAm mel-horoudeT0-T4(p<0,021)emtodasasarticulac¸ões;T0-T12(p<0,023)naMCFenojoelho; T0-T24(p<0,019)apenasnaMCFenojoelho.AFlexGmelhoroudeT0-T4(p<0,001)emtodas asarticulac¸ões;T0-T12(p<0,001)eT0-T24(p<0,02)apenasnaMCFenojoelho.AExtG mel-horoudeT0-T4(p<0,001)emtodasasarticulac¸ões,excetonocotovelo;T0-T12(p=0,003) nopunho,naMCFenojoelho;eT0-T24(p=0,014)naMCFenojoelho.
Conclusão: AEVAerespondeumelhoremcurtoemédioprazosapósaIIAdeHTnessa amostradepacientescomAR.
©2016PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Intra-articular injection (IAI) with corticosteroids (CEs) has beenaverycommonpracticeamongrheumatologistssince 1951.1Itisusuallyusedwhenmonoorpauci-articular
synovi-tispersists.2
Thereare severalCEsusedinclinicalpractice.However, overthe decades,ithasbeen observedinpharmacokinetic studies that the CE with more microcrystalline properties remainslongerinthejoint.3
Thus,since1961triamcinoloneestershavebeenusedinIAI forthetreatmentofrefractorysynovitis.2Triamcinolone
hex-acetonide(TH)isthefluorinatedCEwiththelowestsolubility and mostatrophying propertiesamongthe CEs.3 However,
it islessutilized incomparisonwithother less atrophying CEs.4–6AlthoughIAIiswidelyusedinclinicalpracticeamong
rheumatologists, little isknown about predictors and local variables(pain,swellingandgoniometry)ofbestresponseto IAI.
Theaimofthisstudywastoassesstheresponseof vari-ablessuchasjointpain,swellingandgoniometryafterIAIwith THinshortandmediumtermsinrheumatoidarthritis(RA) patients.
Materials
and
methods
Aprospectivestudywasconductedinacohortof289adultRA patients7withrefractorysynovitiswhoreceivedTHIAI.
PatientswererecruitedfromoutpatientRAclinicfromthe RheumatologyDivision ofthe Universidade Federal deSao Paulo,SaoPaulo,Brazil.TheEthicsCommitteeofthis insti-tutionapprovedthisstudy.
Inclusion criteria were: RA diagnosis according to the American College of Rheumatology (ACR)7; age between
18 and 65 years; refractory synovitis (persistent pain and swelling) in at least one of the following joints: metacar-pophalangeal (MCP), wrist, elbow, shoulder, knee or ankle; functional class II or III8; stable dose of DMARD for the
pastthreemonths;andstabledoseofCEinthelastmonth. Patients were excluded if there wasany suspicion oflocal or systemicinfection;severeclottingdisorder;receivedany IAIinthepast3monthsbeforethestudy,orwereclinically decompensated from diseases suchasdiabetesmellitus or hypertension.Allpatientshaveread,understoodandagreed tosigntheinformedconsentform.
Intervention
IAIwithTHwasblindlyperformedafterrigorousantisepsis withtopicalpovidone-iodine.Weusedsterileanddisposable materialsinallIAIs.Theprocedurewasperformedonasingle occasion (T0–baseline)bythesame rheumatologistwith20 yearsofexperienceininterventionalrheumatology.
The doses of TH used varied according to each joint: shoulder,80mg(4mL);elbow40mgto60mg(2–3mL);wrist, 30–40mg (1.5–2mL); MCP joint, 10–20mg (0.5–1mL); knee, 40–80mg (2–4mL), ankle, 40–60mg (2–3mL).9 The patients
underwentmono,pauci(upto3joints)orpoly(4–8joints)IAI accordingtothenumberofjointswithrefractorysynovitisat thetimeofenrollment.
Assessment
Theassessmenttimeswere:T0(baseline),T1(1week),T4 (4weeks),T12(12weeks)andT24(24weeks)aftertheIAI.
Thefollowingassessmentinstrumentswereusedateach timeofassessment:VAS(visualanaloguescale,0–10cm)for jointpain atrest (VASR),VAS forjoint pain duringmotion (VASM),VASforjointswelling(VASSw);goniometryfor flex-ion(FlexG) and extension(ExtG) forall joints studied. The shoulderwasnotassessedforextension.
Statisticalanalysis
The continuous variables were described in mean and standarddeviation(SD)andthecategoricalvariablesin fre-quenciesandpercentages.
Comparisonofthesepercentageswithcontinuousbaseline variables was made using Kruskal–Wallis test, while com-parison withbaselinecategoricalvariables was doneusing Chi-squareorFisher’sExacttest.Thesetestswereusedonly for same baseline demographic variables and not used in thecomparisonoftherepeatedvariables.Fortheassessment oftimesofthemostimportantcontinuousvariables ofthe presentstudy,e.g.VASR,VASM,VASSw,FlexGandExtG,we usedANOVAwithrepeatedmeasures.Allstatisticalanalyses forthesevariables assessedattimepointswerecarriedout usingANOVAtestwithrepeatedmeasures.
p values were considered statistically significant under 0.05.
Results
Two hundred and eighty-nine RA patients were studied prospectively,withameanageof47.6years(±10.8);mean dis-easedurationof10.98years(±8.4);48.5%ofthesamplewas Caucasianandthewomentomenratiowas12:1.Sixhundred andthirty-fivejointswereincludedandstudiedbetweenT0 andT4,and313jointsuntilT24.AlljointsassesseduntilT4, werealsoevaluatedatT1,andallthoseassessedatT24were alsoevaluatedatT12.
Wefoundnosignificantdifferencesintheproportionofleft andrightsidesinthejointsstudied(p=0.302,Chi-squaretest). Also,wefoundnosignificantdifferencesinagedistribution amongthedifferentjoints(p=0.064,Kruskal–Wallistest).
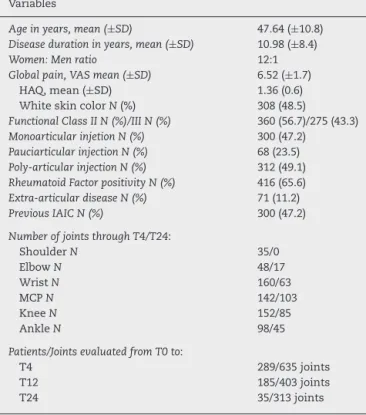
Themoststudiedjointsatinclusionwerewrists(160)and theleaststudiedwereshoulders(35).Ontheotherhand,the jointsmostassessedatT24wereMCPjoints(103).The vari-ablesstudied atT0;the distributionofmono and paucior poly-IAIandthenumberofassessedjointsuntilT4andT24 areshowninTable1.
Tables 2–6 show the results of statistical analysis for responsetoIAIwithTHforeachvariable,VASR,VASM,VASSw, FlexGandExtG.Statisticalanalysiswasperformedcomparing thetimeofassessmentwithT0(baseline)foreachvariable.
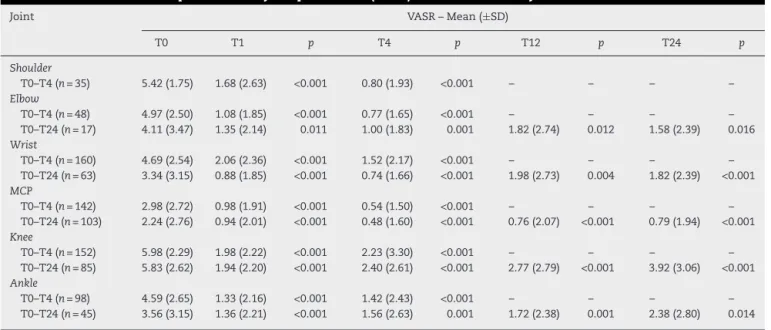
VASRshowedaverygoodresponsetoIAIwithTHanda statisticallysignificantimprovementfromT0toT4(p<0.001); T0toT12(p<0.012);andT0toT24(p<0.016)foralljoints stud-ied.TheimprovementoftheelbowfromT0toT12,andelbow andanklefrom T0toT24werethose rateswiththelowest statisticalsignificance.ThisanalysisisshowninTable2.
Table1–Demographic,relatedtodiseaseandrelatedto injectiondataofthebaselinesample.
Variables
Ageinyears,mean(±SD) 47.64(±10.8) Diseasedurationinyears,mean(±SD) 10.98(±8.4)
Women:Menratio 12:1
Globalpain,VASmean(±SD) 6.52(±1.7)
HAQ,mean(±SD) 1.36(0.6)
WhiteskincolorN(%) 308(48.5)
FunctionalClassIIN(%)/IIIN(%) 360(56.7)/275(43.3) MonoarticularinjetionN(%) 300(47.2)
PauciarticularinjectionN(%) 68(23.5) Poly-articularinjectionN(%) 312(49.1) RheumatoidFactorpositivityN(%) 416(65.6) Extra-articulardiseaseN(%) 71(11.2) PreviousIAICN(%) 300(47.2)
NumberofjointsthroughT4/T24:
ShoulderN 35/0
ElbowN 48/17
WristN 160/63
MCPN 142/103
KneeN 152/85
AnkleN 98/45
Patients/JointsevaluatedfromT0to:
T4 289/635joints
T12 185/403joints
T24 35/313joints
HAQ,HealthAssessmentQuestionnaire;N(%),frequency (percent-age);SD,standarddeviation; IAIC,intra-articularinjection with corticosteroid;MCP, metacarpophalangeal;VAS, visualanalogue scale.
VASMpresentedtheworstevolutioncomparedtoVASRin thesamejoints.VASMshowedimprovementfromT0toT4 (p<0.001)foralljointsstudied;fromT0toT12(p<0.023)for thewrist,MCPandknee;andfromT0toT24(p<0.019)only forMCPandknee.TheelbowwastheonlyjointwhichVASM didnotimproveaftertheIAIwithTHfromT0toT24.Theankle didnotimprovefromT0toT12,andtheankleandthewrist showednoimprovementfromT0toT24(Table3).
VASSwshowedthebestperformanceforalljoints,atall assessmenttimes,asseeninTable4.Thisvariableimproved statisticallyfromT0toT4(p<0.001);T0toT12(p<0.001);and T0toT24(p<0.001)foralljoints,withthehigheststatistical significance(p<0.001)(Table4).
JointgoniometryrespondedworsttoIAIwithTHcompared totheothervariables.FlexGimprovedfromT0toT4(p<0.001) forallthejoints.However,this improvementoccurredonly forMCFandkneefromT0toT12(p<0.001)andfromT0toT24 (p<0.011).Inotherwords,inthemediumterm,this improve-mentwasnotsustained.ThesedataareseeninTable5.
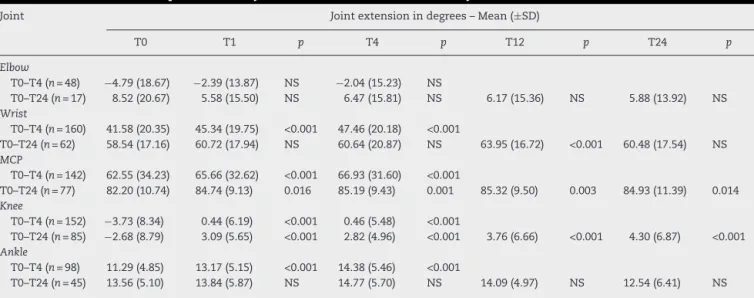
ExtGalsorespondedworsttotheIAIwithTHcomparedto painandjointswelling.ExtGimprovedfromT0toT4(p<0.001) foralljointsexceptfortheelbow;fromT0toT12(p<0.003)for thewrist,MCPandknee;andfromT0toT24(p<0.014)forMCP andknee(Table6).
Discussion
Table2–Assessmentofimprovementinjointpainatrest(VASR)overtimeforeachjointstudied.
Joint VASR–Mean(±SD)
T0 T1 p T4 p T12 p T24 p
Shoulder
T0–T4(n=35) 5.42(1.75) 1.68(2.63) <0.001 0.80(1.93) <0.001 – – – –
Elbow
T0–T4(n=48) 4.97(2.50) 1.08(1.85) <0.001 0.77(1.65) <0.001 – – – –
T0–T24(n=17) 4.11(3.47) 1.35(2.14) 0.011 1.00(1.83) 0.001 1.82(2.74) 0.012 1.58(2.39) 0.016 Wrist
T0–T4(n=160) 4.69(2.54) 2.06(2.36) <0.001 1.52(2.17) <0.001 – – – –
T0–T24(n=63) 3.34(3.15) 0.88(1.85) <0.001 0.74(1.66) <0.001 1.98(2.73) 0.004 1.82(2.39) <0.001 MCP
T0–T4(n=142) 2.98(2.72) 0.98(1.91) <0.001 0.54(1.50) <0.001 – – – –
T0–T24(n=103) 2.24(2.76) 0.94(2.01) <0.001 0.48(1.60) <0.001 0.76(2.07) <0.001 0.79(1.94) <0.001 Knee
T0–T4(n=152) 5.98(2.29) 1.98(2.22) <0.001 2.23(3.30) <0.001 – – – –
T0–T24(n=85) 5.83(2.62) 1.94(2.20) <0.001 2.40(2.61) <0.001 2.77(2.79) <0.001 3.92(3.06) <0.001 Ankle
T0–T4(n=98) 4.59(2.65) 1.33(2.16) <0.001 1.42(2.43) <0.001 – – – –
T0–T24(n=45) 3.56(3.15) 1.36(2.21) <0.001 1.56(2.63) 0.001 1.72(2.38) 0.001 2.38(2.80) 0.014
VASR,visualanaloguescale0–10cmforrestpain;SD,standarddeviation;MCP,metacarpophalangealjoint. Statisticaltest:ANOVAforrepeatedmeasures.
slowest joint clearance and the most potent in producing synovial atrophy.However, it is alsothe most potential to causedamageif injectedinto extra-articulartissue.3 Ithas
beenprovenitssuperiorityoverotherintraarticularCEused inRAandinosteoarthritis(OA)patients.Itsusehasbeen con-sideredsuperiortotheuseofsystemicCEwhenusedinmono orpolyIAIinRApatients.10,11
Althoughitisaprocedurewidelyusedbyrheumatologists, therearefewprospectivestudiescomparingtheeffectiveness ofIAIwithotherinterventions,orevenwiththesystemicuse ofotherCE.10,11
Byconductingthisstudy,weintendedtoidentifythejoint variableswhichbestrespondedtoIAIwithTHinthejoints
weconsidered relevantinRApatients, using“blinded”and prospectiveassessmentsatshortandmid-term.
ItwasobservedthatVASRimprovedfromT0toT4,T0to T12andT0toT24forallinjectedjoints.Weexpectedtherest paintobeavariablewellresponsivetotheIAI.Surprisingly, VASMimproved statisticallyforall jointsonlyinthe short term(T0–T4).Inthelongterm,thisvariableimproved statisti-cally,foronlyMCPsandknees.Thedifferenceinpainresponse betweenVASRandVASMmaybeduetoseveralfactors.Painon movementmaybeamoredifficultvariabletotreatbecauseof thestressresultingfromthemovementoftheinflamedjoint. Joint goniometry variables (FlexG and ExtG) responded welltoIAIwithTHonlyintheshortterm,wherestatistical
Table3–Assessmentofimprovementinjointpaininmotion(VASM)overtimeforeachjointstudied.
Joint VASM–Mean(±SD)
T0 T1 p T4 p T12 p T24 p
Shoulder
T0–T4(n=35) 7.11(1.62) 4.74(2.47) <0.001 3.31(2.71) <0.001 – – – –
Elbow
T0–T4(n=48) 5.70(3.29) 2.66(2.83) <0.001 1.93(2.60) <0.001 – – – –
T0–T24(n=17) 2.05(2.53) 0.88(1.96) NS 0.58(1.66) NS 0.29(1.21) NS 0.58(1.66) NS Wrist
T0–T4(n=160) 4.76(3.11) 2.69(2.67) <0.001 2.28(2.57) <0.001 – – – –
T0–T24(n=63) 1.74(2.40) 0.55(1.58) <0.001 0.79(1.84) 0.021 0.82(1.83) 0.023 1.66(2.37) NS MCP
T0–T4(n=142) 2.93(3.18) 1.38(2.19) <0.001 1.02(2.01) <0.001 – – – –
T0–T24(n=103) 1.50(2.30) 0.63(1.66) 0.012 0.33(1.26) <0.001 0.38(1.34) <0.001 0.67(1.72) 0.019 Knee
T0–T4(n=152) 6.16(2.37) 2.40(2.37) <0.001 2.11(2.39) <0.001 – – – –
T0–T24(n=85) 5.52(2.69) 1.81(2.22) <0.001 1.91(2.49) <0.001 2.56(2.66) <0.001 3.51(3.18) <0.001 Ankle
T0–T4(n=98) 5.30(3.28) 2.85(2.91) <0.001 2.80(3.05) <0.001 – – – –
T0–T24(n=45) 2.44(2.52) 0.77(1.83) 0.003 0.88(1.93) 0.002 1.66(2.38) NS 2.22(2.51) NS
Table4–Assessmentofimprovementinjointswelling(VASSw)overtimeforeachjointstudied.
Joint VASSw–Mean(±SD)
T0 T1 p T4 p T12 p T24 p
Shoulder
T0–T4(n=35) 3.37(1.64) 1.31(0.99) <0.001 0.62(0.77) <0.001 – – – –
Elbow
T0–T4(n=48) 5.47(1.32) 2.04(1.85) <0.001 1.43(1.72) <0.001 – – – –
T0–T24(n=17) 5.47(2.18) 1.17(2.18) <0.001 1.47(2.34) <0.001 1.47(2.33) <0.001 0.88(1.96) <0.001 Wrist
T0–T4(n=160) 5.27(1.32) 2.83(2.08) <0.001 2.23(2.09) <0.001 – – – –
T0–T24(n=63) 5.27(1.32) 2.46(2.51) <0.001 1.98(2.46) <0.001 3.33(2.37) <0.001 3.57(2.27) <0.001 MCP
T0–T4(n=142) 5.07(0.84) 2.05(2.23) <0.001 1.25(1.92) <0.001 – – – –
T0–T24(n=103) 5.07(0.84) 1.99(2.45) <0.001 1.21(2.15) <0.001 1.85(2.41) <0.001 1.99(2.45) <0.001 Knee
T0–T4(n=152) 4.58(1.68) 1.93(1.81) <0.001 1.30(1.54) <0.001 – – – –
T0–T24(n=85) 4.17(1.66) 1.48(1.91) <0.001 1.05(1.57) <0.001 1.17(1.64) <0.001 1.50(1.78) <0.001 Ankle
T0–T4(n=98) 5.56(1.45) 2.71(2.12) <0.001 2.31(2.09) <0.001 – – – –
T0–T24(n=45) 5.47(1.32) 2.11(2.49) <0.001 1.88(2.45) <0.001 2.66(2.52) <0.001 2.77(2.51) <0.001
VASSw,visualanaloguescale0–10cmforjointswelling;SD,standarddeviation;MCP,metacarpophalangealjoint. Statisticaltest:ANOVAforrepeatedmeasures.
responsestoalljointsstudiedwereobserved.However,inthe mediumterm,the responseswere statisticallymorefragile and ina fewernumber ofjoints. Thisfinding may bedue tothe fact that our samplewas composed byRApatients withameanlengthtimeofdiseaseofalmost11years.The highprevalenceoflongstandingRAprobablyrepresenteda crucialfactor for the goniometryoutcomes. Long standing patientslikethesemaypresentseverestructuraldamageand secondary osteoarthritis and this may haveinfluenced the responseofgoniometryvariablesFlexGandExtGaswellas VASM.
VASSwwasthevariablewiththebestresponsetoIAIwith THatallassessmenttimesforalljoints,andwithbest sta-tisticalsignificance.Weobservedastatisticalimprovement fromT0atT4,T12andT24weeksforalljoints,alwayswith ap<0.001.Thisreinforcesthehypothesisoftheatrophying propertiesofTH,possiblycausingadecreaseinVASSw,ajoint parametermoreobjectivethanthepain.
Intheliterature,wefoundthattheIAIresponseduration mayvaryaccordingtothediseaseinquestion.Itisobserved in meta-analyses and systematic reviews that the typical response duration toIAI in OA patients is (typically)from
Table5–Assessmentofimprovementinjointflexionovertimeforeachjointstudied.
Joint Jointflexionindegrees–Mean(±SD)
T0 T1 p T4 p T12 p T24 p
Shoulder
T0–T4(n=35) 137.42(32.50) 148.25(31.85) <0.001 156.14(32.99) <0.001 – – – – Elbow
T0–T4(n=48) 124.72(12.20) 132.08(10.14) <0.001 133.16(8.45) <0.001 – – – – T0–T24(n=17) 126.17(10.82) 130.58(11.97) NS 127.35(6.40) NS 126.47(10.27) NS 128.52(7.01) NS Wrist
T0–T4(n=160) 42.46(18.70) 45.57(21.10) 0.005 47.73(19.16) <0.001 – – – –
T0–T24(n=63) 45.87(22.31) 47.22(24.86) NS 48.73(21.53) NS 48.53(22.66) NS 46.50(20.62) NS MCP
T0–T4(n=142) 76.72(18.63) 83.57(10.65) <0.001 85.03(9.40) <0.001 – – – – T0–T24(n=103) 82.28(10.65) 84.56(9.26) 0.007 85.09(9.54) <0.001 85.19(9.94) <0.001 84.51(11.42) 0.011 Knee
T0–T4(n=152) 116.01(15.07) 121.25(15.59) <0.001 123.49(17.26) <0.001 – – – – T0–T24(n=85) 115.94(13.82) 120.14(17.36) 0.009 122.17(14.22) <0.001 121.29(13.02) <0.001 120.14(14.26) 0.002 Ankle
T0–T4(n=98) 28.59(13.91) 32.34(13.26) <0.001 32.85(14.51) <0.001 – – – – T0–T24(n=45) 33.11(16.42) 34.22(16.05) NS 31.77(16.99) NS 33.22(17.22) NS 32.00(16.69) NS
Table6–Assessmentofimprovementinjointextensionovertimeforeachjointstudied.
Joint Jointextensionindegrees–Mean(±SD)
T0 T1 p T4 p T12 p T24 p
Elbow
T0–T4(n=48) −4.79(18.67) −2.39(13.87) NS −2.04(15.23) NS
T0–T24(n=17) 8.52(20.67) 5.58(15.50) NS 6.47(15.81) NS 6.17(15.36) NS 5.88(13.92) NS Wrist
T0–T4(n=160) 41.58(20.35) 45.34(19.75) <0.001 47.46(20.18) <0.001
T0–T24(n=62) 58.54(17.16) 60.72(17.94) NS 60.64(20.87) NS 63.95(16.72) <0.001 60.48(17.54) NS MCP
T0–T4(n=142) 62.55(34.23) 65.66(32.62) <0.001 66.93(31.60) <0.001
T0–T24(n=77) 82.20(10.74) 84.74(9.13) 0.016 85.19(9.43) 0.001 85.32(9.50) 0.003 84.93(11.39) 0.014 Knee
T0–T4(n=152) −3.73(8.34) 0.44(6.19) <0.001 0.46(5.48) <0.001
T0–T24(n=85) −2.68(8.79) 3.09(5.65) <0.001 2.82(4.96) <0.001 3.76(6.66) <0.001 4.30(6.87) <0.001 Ankle
T0–T4(n=98) 11.29(4.85) 13.17(5.15) <0.001 14.38(5.46) <0.001
T0–T24(n=45) 13.56(5.10) 13.84(5.87) NS 14.77(5.70) NS 14.09(4.97) NS 12.54(6.41) NS
SD,standarddeviation;NS,nostatisticaldifference;MCP,metacarpophalangealjoint. Statisticaltest:ANOVAforrepeatedmeasures.
onlyonetotwoweeks,reportedamaximumof4weeks.12–14
Theseresultsarequitedifferentfromours,whichshowed sus-tainedresponse(improvement)toIAIwithTHforatleastfour weeksforall variables inall assessed joints.On assessing the VASs, most of the joints showed sustained response up to 12 weeks. For MCPs and knee joints, we observed sustained response until T24, notonly for the three VASs variables, but also for the joint goniometry of flexion and extension.
As regards juvenile idiopathic arthritis (JIA), systematic reviewshaveshown aresponsetothe CEIAIwitha maxi-mumdurationof1yearand3monthsto1yearand8months, dependingon thestudy.Inthese studies,thepredictors of increasedresponsetoIAIwere“currentuseofmethotrexate”, “kneeinjected”,“useofTHforIAI”and“currentuseofCEat thetimeofIAI”.15–18Inourstudy,kneealsoshowedan
excel-lentresponse.Butourfollow-uptimeofpatientswasmuch shorter,only24weeks.
Thejointsthatshowedstatistical improvementafterIAI withTHforallvariablesandtimespointsstudiedinourstudy weretheMCPsandknees.Thisfindingmaybedue,among other causes,to the excellent accuracyofthe IAI inthose joints,asdeterminedbyLopesetal.19Theseauthorsfoundan
accuracyof100%and97%forIAIswithTHperformedblindly andrespectivelyforkneesandMCPs.
Wecan pointsomelimitations ofthe presentstudy.We canmentiontheintragroupanalysis;thenon-homogeneous distributionofthe kinds ofinjectedjoints (particularlythe low number of shoulders) and follow-up time; the lack of a functional assessment (ex: HAQ) atthe time-points; the lackof long-termfollow-up. The followingare also limita-tionsofthepresentstudy:theabsenceofanalysisbetween pre-injectedandfist-injectedjoints,theabsenceofanalysisof injectionaccuracyandtheabsenceofanalysisofthe correla-tionbetweentheuseofantirheumaticdrugsandthepresence ofarticulardeformitywiththeresponsetoIAI;and,moreover, theabsenceofamoreobjectiveassessmenttool,suchasthe articularultrasound.Theabsenceofanymethodofstatistical
correctionformultiplecomparisonscanalsobeconsidereda limitation.
Moreover,theapplicabilityofourworkisrelevant.Through it,weidentifiedthatjointswelling isthevariablethat best respondstoIAIwithTHinalargecohortofpatients evalu-atedprospectivelyand“blindly”.Thisreinforcestheindication ofTHusetopromotechemicalsynovectomyinRApatients withrefractorysynovitis.Anotherinterestingfinding inour studyistheevidenceofapoorresponseinjointgoniometry inthemediumtermafterIAIwithTH.Therefore,weshould notalwaysexpectsignificantchangesinjointgoniometryafter IAIwithCE,eveninjointsthatimprovedpainandswelling.
ThisstudycorroboratesthestatementofIAIwithTHfor treatmentofrefractorysynovitisinRApatients.Jointswelling wasidentifiedasthevariablewiththebestresponsetothis procedure,andthekneesandMCPsasthejointswiththebest responsetoit.Moreprospectivestudiesarerequiredtodefine othervariablessuchastheoptimaldoseofTHandtheexact durationofresponseafterIAI.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HollanderJL,BrownEMJr,JessarRA,BrownCY.Comparative effectsofCompoundF(17-hydroxycorticosterone)and cortisoneinjectedlocallyintotherheumatoidarthriticjoint. AnnRheumDis.1951;10:473–6.
2.GrayRG,GottliebNL.Intra-articularcorticosteroids.An updatedassessment.ClinOrthopRelatRes.1983:235–63.
4. BainLS,BalchHW,WetherlyJM,YeadonA.Intraarticular triamcinolonehexacetonide:double-blindcomparisonwith methylprednisolone.BrJClinPract.1972;26:559–61.
5. BlythT,HunterJA,StirlingA.Painreliefintherheumatoid kneeaftersteroidinjection.Asingle-blindcomparisonof hydrocortisonesuccinate,andtriamcinoloneacetonideor hexacetonide.BrJRheumatol.1994;33:461–3.
6. ZulianF,MartiniG,GobberD,AgostoC,GiganteC,Zacchello F.Comparisonofintra-articulartriamcinolonehexacetonide andtriamcinoloneacetonideinoligoarticularjuvenile idiopathicarthritis.Rheumatology(Oxford).2003;42: 1254–9.
7. ArnettFC,EdworthySM,BlochDA,McShaneDJ,FriesJF, CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriafortheclassificationofrheumatoid arthritis.ArthritisRheum.1988;31:315–24.
8. HochbergMC,ChangRW,DwoshI,LindseyS,PincusT,Wolfe F.TheAmericanCollegeofRheumatology1991revised criteriafortheclassificationofglobalfunctionalstatusin rheumatoidarthritis.ArthritisRheum.1992;35:498–502.
9. FurtadoRNV,NatourJ.Infiltrac¸õesnoaparelholocomotor, vol.1,1sted.RiodeJaneiro:Artmed;2011.
10.KonaiMS,VilarFurtadoRN,DosSantosMF,NatourJ. Monoarticularcorticosteroidinjectionversussystemic administrationinthetreatmentofrheumatoidarthritis patients:arandomizeddouble-blindcontrolledstudy.Clin ExpRheumat.2009;27:214–21.
11.FurtadoRN,OliveiraLM,NatourJ.Polyarticularcorticosteroid injectionversussystemicadministrationintreatmentof rheumatoidarthritispatients:arandomizedcontrolledstudy. JRheumatol.2005;32:1691–8.
12.ArrollB,Goodyear-SmithF.Corticosteroidinjectionsfor osteoarthritisoftheknee:meta-analysis.BMJ.2004;328:869.
13.GodwinM,DawesM.Intra-articularsteroidinjectionsfor painfulknees.Systematicreviewwithmeta-analysis.Can FamPhysician.2004;50:241–8.
14.HepperCT,HalvorsonJJ,DuncanST,GregoryAJ,DunnWR, SpindlerKP.Theefficacyanddurationofintra-articular corticosteroidinjectionforkneeosteoarthritis:asystematic reviewoflevelIstudies.JAmAcadOrthopSurg.
2009;17:638–46.
15.BreitW,FroschM,MeyerU,HeineckeA,GanserG.A subgroup-specificevaluationoftheefficacyofintraarticular triamcinolonehexacetonideinjuvenilechronicarthritis.J Rheumatol.2000;27:2696–702.
16.MartiP,MolinariL,BoltIB,SegerR,SaurenmannRK.Factors influencingtheefficacyofintra-articularsteroidinjectionsin patientswithjuvenileidiopathicarthritis.EurJPediatr. 2008;167:425–30.
17.BloomBJ,AlarioAJ,MillerLC.Intra-articularcorticosteroid therapyforjuvenileidiopathicarthritis:reportofan experientialcohortandliteraturereview.RheumatolInt. 2011;31:749–56.
18.PapadopoulouC,KostikM,Gonzalez-FernandezMI,BohmM, Nieto-GonzalezJC,PistorioA,etal.Delineatingtheroleof multipleintraarticularcorticosteroidinjectionsinthe managementofjuvenileidiopathicarthritisinthebiologic era.ArthritisCareRes.2013;65:1112–20.
19.LopesRV,FurtadoRN,ParmigianiL,RosenfeldA,Fernandes AR,NatourJ.Accuracyofintra-articularinjectionsin peripheraljointsperformedblindlyinpatientswith