w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
Report
Retroperitoneal
abscess
after
transanal
minimally
invasive
surgery:
case
report
and
review
of
literature
夽
Aaron
Raney
b,
Shankar
Raman
a,∗aMercySurgicalAffiliates,DesMoines,UnitedStates bDesMoinesUniversity,DesMoines,UnitedStates
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2April2017
Accepted19June2017
Availableonline8August2017
Keywords:
Colorectalsurgery
Transanalminimallyinvasive
surgery(TAMIS)
Retroperitonealabscess
Naturalorificetransluminal
endoscopicsurgery(NOTES)
Single-sitelaparoscopicsurgery
(SILS)
Surgicaloncology
a
b
s
t
r
a
c
t
Abscessesareararecomplicationoftransanalminimallyinvasivesurgeryandtransanal
endoscopicmicrosurgery.Reportedcaseshavebeenintherectalandpre-sacralareasand
havebeenmanagedwitheitherantibioticsaloneorinconjunctionwithlaparotomyand
divertingcolostomy.WereportacaseofalargeretroperitonealabscessfollowingaTransanal
minimallyinvasivesurgeryfullthicknessrectalpolypexcision.Thepatientwassuccessfully
managedconservativelywithantibioticsandapercutaneousdrain.Retroperitoneal
infec-tionshouldbeincludedinadifferentialdiagnosisfollowingaTransanalminimallyinvasive
surgeryprocedureasthepresentationcanbeinsidiousandtimelyinterventionisneeded
topreventfurthermorbidity.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This
isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Abscesso
retroperitoneal
após
cirurgia
de
ressecc¸ão
transanal
minimamente
invasiva:
relato
de
caso
clínico
e
revisão
a
literatura
médica
Palavras-chave:
Cirurgiacolorretal
Cirurgiaderessecc¸ãotransanal
minimamenteinvasiva(TAMIS)
Abscessoretroperitoneal
r
e
s
u
m
o
Osabscessossãoumacomplicac¸ãoraradacirurgiaderessecc¸ãotransanalminimamente
invasiva(TAMIS)edamicrocirurgiaendoscópicatransanal(TEMS).Oscasosnotificados
foramnasáreasrectalepré-sacraleforamadministradoscomantibióticosisoladamente
ouemconjuntocomlaparotomiaedesviodecolostomia.Relatamosumcasodegrande
abscesso retroperitoneal após uma excisão de pólipo retal de espessura total TAMIS.
夽
PaperdevelopedatMercyMedicalCenter,DepartmentofSurgery,DesMoines,UnitedStates.
∗ Correspondingauthor.
E-mail:[email protected](S.Raman).
http://dx.doi.org/10.1016/j.jcol.2017.06.007
2237-9363/©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC
Cirurgiaendoscópica
transluminaldeorifícionatural
(NOTES)
Cirurgialaparoscópicadeúnico
local(SILS)
Oncologiacirúrgica
Opacientefoitratadocomsucessocomaadministrac¸ãodeantibióticosedrenagem
per-cutânea.Paraprevenirmaismorbidadeénecessáriaincluirainfecc¸ãoretroperitonealno
diagnosticodiferencialapósumprocedimentoTAMISondeaapresentac¸ãopodeser
insid-iosaeaintervenc¸ãoatempada.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este
´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Introduction
Transanalminimally invasive surgery(TAMIS) isa recently
developedsurgicalapproachfirstdescribedin2010byAtallah
etal.1Itisaformofnaturalorificetransluminalendoscopic
surgery(NOTES)thatisanalternativetothepreviously
devel-opedtransanalendoscopicmicrosurgery(TEMS)technology.
In contrast to TEMS, TAMIS utilizes ordinary laparoscopic
instruments instead ofTEMSspecific instruments.Though
therehavebeennoextensivecomparativestudies,TAMIS
plat-formhasbeenquicklyadoptedduetodecreasedupfrontcost,
readilyaccessibleinstruments,andfasterlearningcurve.1,2
A single-incision laparoscopic surgery (SILS) port, adapted
for transanal use (SILSTM Port, Covidien, Dublin, Ireland)
oraspecifictransanalplatform (GelPOINT©PathTransanal
AccessPlatform, AppliedMedical,Rancho SantaMargarita,
CA,USA),isplacedandsecuredintheanus.1Standard
laparo-scopic instruments are then placed through this port and
allowforconventionallaparoscopicdissection.2
Pneumorec-tumallowsforadequatevisualizationandtheshorterTAMIS
platform providesadvantageous workingangleswithinthe
rectumaswellascircumferentialdissectionwithoutpatient
re-positioning.2,3Furthermore,thesoftplatformhasthe
the-oreticaladvantageofbetterfunctionaloutcomesduetoless
tractionontheanalwall.2
TAMIS has proven to be an effective platform for R0
localresectionofbenignneoplasiaandearlyrectalcancer.2
Reported procedure specific complications have been
pri-marilybleeding,peritonealentry,andrectalabscess.3–5 The
true incidenceof post-TAMIS abscesses isnot well known
andtherehasnotbeenalargeretroperitonealabscess
doc-umented. Wereporta caseofan extensiveretroperitoneal
abscess formation following a TAMIS procedure without
peritoneal entry. This was managed nonoperatively with
antibiotics,andpercutaneousdrainage.
Case
presentation
A62-yearoldmale,withahistoryofcolonicpolyps,
under-wentacolonoscopywherehewasnotedtohavealargerectal
polyplocatedintheleftposterolateralposition,startingjust
abovethelevelofthedentatelineandmeasuring4cm×3cm,
extendingcraniallytojust abovethe level oftheanorectal
ring (Fig. 1). His medical history was significant for
well-controlleddiabetesmellitustypeII,(HemoglobinA1c–5.7%),
hypertension, and nephrolithiasis. On digital rectal exam,
this felt as a soft fleshy polyp located about 3–4cm from
theanal verge.Pre-operativebiopsiesshowed tubulovillous
adenoma and MRI and endorectal ultrasound indicated
possibleT2N0lesion.Inview ofthese findings,the patient
underwentTAMISwithfullthicknessexcisionofthepolyp.He
receivedpreoperativemechanicalbowelprepwithPEG-3350
(Braintree Laboratories Inc, Braintree, MA, USA) without
oralantibiotics.1gofErtapenemwasgivenIVasantibiotic
prophylaxis,15minbeforestartoftheprocedure.Thepatient
wasplacedintheleftlateralpositionandpneumorectumwas
established up to 15mmHg using CO2 insufflator (Stryker,
Kalamazoo,MI,USA).Thewoundwasclosedwith2-0V-LocTM
wound closure device (Covidien, Dublin, Ireland) on both
theanteriorandposterioraspects,leavingthecentralmost
portionopentoavoidexcessivetension.Operatingtimewas
94min and the procedure was uneventful. There was no
intraoperativecontaminationoftheoperativesite.Therewas
no entry into theperitoneal cavityasthis was alow-lying
lesion.Finalpathologicresultsshowedatubulovillous
ade-noma 3.7cm×3.2cm in dimension with focal high-grade
dysplasia and negative margins. Thepatient tolerated the
procedurewellandwasdischargedonthefirstpost-operative
day.
Onpostoperativedayfive,hepresentedtotheemergency
roomwithworseningleftlowerquadrantabdominalpain
radi-atingtohisback.Hehadnorectalpain.Anon-contrastCT
scan ofhisabdomen and pelvis,performed dueto history
ofnephrolithiasis,showedinflammatorystrandingaswellas
extraluminalairinthepelvisandleftlowerquadrantwithout
anyfocallydrainablefluidcollections.Thepatientwasafebrile
and hemodynamically stablewithout leukocytosisor lactic
acidosis. Bowelrest and empiricantibiotics were initiated.
Bloodcultureswerenegative.Thepatient’spainimprovedand
hiswhitecountremainednormal.However,hedeveloped
low-gradefevers.Therefore,aCTscanwithcontrastwasrepeated
48hafterre-admission(post-operativedayseven).It
demon-strated increasedemphysematouscollections. Extraluminal
gaswaslocatedadjacenttothemedialaspectofthe
descen-dingcolon.Additionalgaswasseenintheretroperitoneum,
anterior to the left psoas muscle and extending caudally
and mediallyinto thepre-sacralregionandadjacenttothe
rectum ontheleft.There wasnofreeperitonealair. There
was alsonewfluid associatedwiththe airadjacent to the
psoas withthegreatestcollectionmeasuring10cm×4.1cm
transaxiallyand9cmcraniocaudally(Fig.2).Dueto
progres-sion of infectious process, antibiotics were escalated. The
retroperitonealfluidcollectionwasdrainedbyCT-guided
per-cutaneousplacementof12-Frenchpigtailanteriortotheleft
psoasandreturnedairandcloudyfluid.Drainculturesgrew
moderate growth of Escherichia coli and Pseudomonas
aeru-ginosa, light growth ofBacteroides thetaiotaomicron, and rare
A
B
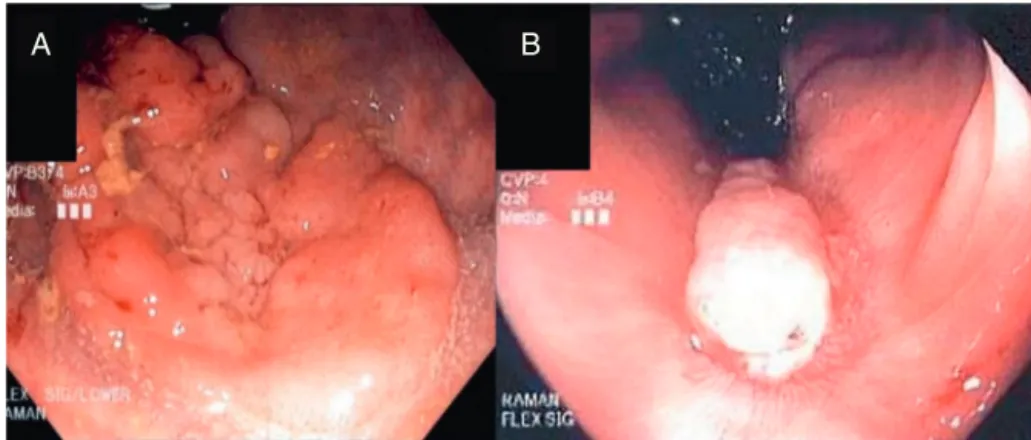
Fig.1–Pre-operativeflexiblesigmoidoscopyshowingleftposterolateral4cm×3cmpolyp(A)andfollow-upflexible
sigmoidoscopyfivemonthspost-operativelydemonstratinghealedposteriorrectalmucosa(B).
B
A
120mm
160mm
Fig.2–CTscanonpost-operativedaysevendemonstratingcommunicationoftherectaldefectwiththeperi-rectalaspectof theabscess(A)andextentofleftretroperitonealemphysemaandabscess(B).
A
B
Lossy P
Lossy
P
120mm
120mm
Fig.3–CTscan15days(post-operativeday22)afterCTguidedpercutaneousdrainplacementdemonstratingresolved peri-rectal(A)andretroperitonealabscesses(B).
levofloxacinandmetronidazoleinresponsetocultures.The
patientimprovedclinicallyasdrainoutputslowed.He
devel-opedpersistenturinaryretentionthatrequireddischargewith
Foleycatheter.Dietwasadvanced andthepatientwas
dis-chargedfivedaysafterdrainplacement.Follow-updrainstudy
fivedayslatershowedsignificantimprovementof
communi-catingretroperitoneal,presacral,andperirectalabscessareas
withtheperirectalabscessdrainingviatheportionofrectum
operativelyleftopen(Fig.3).Thedrainwasremoved15days
afterplacementwithminimalongoingoutputandthepatient
madeacompleterecovery.
Flexible sigmoidoscopy five months afterthe procedure
showed that rectal mucosahad healed completely (Fig. 1).
An inflammatory polyp was seen and biopsied at the site
of previous TAMIS full-thickness excision, pathology
con-firmed benign etiology. At the time of writing, 16 months
afterTAMIS, patient isdoingwell without any evidenceof
Table1–LiteraturereviewofabscesslocationsfollowingTAMISandTAMISrelatedproceduresandmanagementof
abscesscomplications.
Authors Date Procedure Abscesslocation(incidence) Management
Gilletal.4 2015 TAMIS Rectalabscess(1of32,
3%)
DivertingHartmann procedure
Bignelletal.10 2010 TEMS Pre-sacralabscess(7of
262,3%)
Twomanaged
conservativelywith antibioticsalone.Five requireddiverting stomaduetolackof resolutiononantibiotics alone.
Bretagnoletal.11 2007 TEMS Pre-sacralabscess(1of
200,0.5%)
Intra-abdominal abscess(3of200,1.5%)
Laparotomyfor drainageandtemporary colostomy.
Twopatientsrequired laparotomyand drainage,onemanaged conservativelywith antibioticsandnothing bymouth.
TAMIS,transanalminimallyinvasivesurgery;TEMS,transanalendoscopicmicrosurgery.
Discussion
Retroperitonealabscessesarearareclinicaloccurrenceand
often are insidiousin nature. For these reasons, they can
be difficult to diagnose, leading to treatment delay.6 The
mostfrequentpresentationisacombination offever,
lum-barorabdominalpain,andalumbarmass,thoughtheycan
also present with nonspecific symptoms such as malaise,
abdominaldiscomfort,andweightloss.6,7 Laboratory
evalu-ationusuallyshowsleukocytosisaswellasthepotentialfor
anemia, pyuria,and elevated creatinine.6 Diagnosiscan be
madebyultrasoundorCT.Retroperitonealabscessesariseby
invasionfromadjacentstructuresincludingrenalinfections,
lumbarosteomyelitis, pancreatitis, colon carcinoma,
diver-ticulitis,Crohn’sdisease,andappendicitis.7Microorganisms
isolatedfrom theseabscesses mostoftengrowgram
nega-tivebacilli.6Onceanabscessisidentified,earlytreatmentby
drainageandintravenousantibioticsisneeded.
Ourpatientpresentedwithoutleukocytosis,lactic
acido-sisorsignificantfever.Hispredominantsymptomwasback
andflankpain.Thisfurtherhighlightstheinsidious
presenta-tionofretroperitonealabscesses.Whileourpatientdidhave
ahistoryofrenalcalculiandaCTscanshowingaleft
non-obstructingrenal calculus, the retroperitoneal abscesswas
duetofullthicknessexcisionofrectalpolyp.Cultureresults
andabscesstrackingfromthesurgicalsitesupportthis
con-clusion.
FollowingtheadventoftheTAMIStechnologytherehave
beenvariousdocumentedcasesofabscesscomplications
fol-lowingtheTAMISprocedure.These abscesseshavebeen in
eithertheperi-rectal,pre-sacralorpelvicareas(Table1).This
caseisuniqueinthatpatientdevelopedalargepre-sacraland
peri-rectalabscessthatextendedalongleftpsoasmusclein
theretroperitoneumtotheleveloftheleftcolon.This
prob-ablyoccurredduetointraoperativeseedingofbacteriaaided
bydissectionintotheretroperitoneumfrom carbondioxide
insufflation.
Extension of infection from the anal region into the
retroperitoneumhasbeenwelldocumented.Themostsimilar
comparison is that ofa case study of retroperitoneal
sep-sis followinga stapled transanalrectal resection (STARR).8
However,whiletheSTARRproceduredoesinvolvefull
thick-ness rectal wall resection, the use ofa stapler, closure of
the full-thicknessdefectand thenon-endoscopicnatureof
the procedure makeit fardifferent from theTAMIS
proce-dure.Althoughrare,retroperitonealsepsisorabscesscanalso
originatefromanorectalinfectionsthatinvadebeyond
pubo-rectalisandruptureintooneofthesupralevatorspaces.7,9In
alargeseriesof262patientswhounderwentTEMS,presence
oftherectallesionlessthan2cmfromthedentatelinewas
associatedwithhigherincidenceofpelvicsepsis.Pelvicsepsis
developedin4/62patientswithlow-lyinglesionsascompared
to1/200 patientswithhigh lyinglesions(p<0.02).
Interest-ingly,therewasnostatisticalassociationbetweenclosureof
thedefectandincidenceofpelvicsepsis.Also,mostpatients
withpelvicsepsisweremanagedwithdivertingcolostomy.10
Asinterventionalradiology (IR)technologyand skillhas
advanced, it has replaced the need for surgical drainage
in all but the mostcomplex cases. Percutaneous drainage
mustbecarefullyplannedtoavoidcriticalanatomy.
Gener-ally,retroperitoneal abscessmanagementstrategiesinclude
conservativetreatmentwithantibioticsalone,interventional
radiologyguidedpercutaneousdrains,versustraditional
sur-gicalexplorationanddrainplacement.6,8Withinthecontext
ofpost-operativebowelanastomosisorwallclosure,theneed
forprotectivecolostomyshouldbeevaluatedandconsidered.
Furthermore,theneedforrectalresectionmaybenecessitated
ifthedegreeofinfectionissufficientlyinjurious.
Small retroperitonealabscesses(lessthan 3cmin
diam-eter)inahemodynamicallystablepatientmaybeeffectively
However,largerabscessesorun-resolvingsmallerabscesses
mustbedrainedeitherbypercutaneousdrainplacementor
bysurgicalexploration anddrainage. Surgeryoffersseveral
advantages over IR drainage including the ability to fully
explore the anatomy and extent of the infection as well
asthe abilitytoremove fistulous tracts.6 However, surgery
does carry more significant risks, delays, and morbidity.
Resolutionand recurrenceare similarbetweenthesurgical
andIRapproaches.6
Previous rectal and pre-sacral abscess complications of
TAMIS and TEMS for local excisions have been managed
withantibioticsaloneorincombinationwithlaparotomyand
divertingcolostomy (Table 1). Our patient’s large
retroperi-tonealabscesswasmanaged withpercutaneousCT guided
drain placement and antibiotics. Wewere able to avoid a
colostomy or loop ileostomy in spite of the presence of
extensiveretroperitoneal inflammationand abscess
forma-tionextendingfromthelowrectumuptotheleftpsoas as
the patient did not have sepsis or generalized peritonitis.
Ourpracticehasbeentomanagecomplicated diverticulitis
withabscessformationwithCTguideddrainage,duetothe
availabilityofskilledinterventionalradiologists.Weapplied
thoseprinciples tomanagethe current patient, controlling
the infectious process with percutaneous drainage. If this
wasinfeasibleor unsuccessful,surgicalinterventionwould
beindicated.Whetherleaving thesite ofTAMIS open
con-tributed to the postoperative retroperitoneal infection and
abscessformationisarbitraryastheliteraturedoesnotshow
closurepreventscomplicationsorleavingthesiteopencauses
complications.Closureisessentialtopreventintraperitoneal
contaminationwhentheperitonealcavityisentered.When
thereisnoentryintotheperitonealcavity,closingthedefect
hasnoobviousadvantages.Inalargemulticenter
retrospec-tivestudyof75patientsundergoingTAMIS,thedefectwasnot
closedin35patients.Therewasnosignificantdifferencein
incidenceofcomplicationsbetweenthetwogroups.12
Inter-estingly,in anotherstudy ofpatientsundergoing transanal
excisionandTAMIS,ahighernumberofpostoperative
compli-cationsofallgradeswerenotedinpatientswherethedefect
wasclosed.13
Conclusion
Ourcasereportdemonstratesacomplicationthatisunique
tofull-thicknessexcisionofrectallesions.FollowingTAMIS,
patientscan present withsymptomsthat are distant from
the site of surgery. Retroperitoneal infection should be
consideredinthedifferentialdiagnosis.Timelyintervention
isofparamountimportanceinpreventingfurthermorbidity
frominfection.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.AtallahS,AlbertM,LarachS.Transanalminimallyinvasive
surgery:agiantleapforward.SurgEndosc.2010;24:2200–5.
2.QuaresimaS,BallaA,FranceschilliL,LaTorreM,IafrateC,
ShalabyM,etal.Transanalminimallyinvasivesurgeryfor
rectallesions.JSocLaparoendoscSurg.2016;20,e2016.00032.
3.Martin-PerezB,Andrade-RibeiroG,HunterL,AtallahS.A
systematicreviewoftransanalminimallyinvasivesurgery
(TAMIS)from2010to2013.TechColoproctol.2014;18:775–88.
4.GillS,StetlerJ,PatelA,ShafferV,SrinivasanJ,StaleyC,etal.
Transanalminimallyinvasivesurgery(TAMIS):standardizing
areproducibleprocedure.JGastrointestSurg.2015;19:1528–36.
5.KellerD,TahilramaniR,Flores-GonzalezJ,MahmoodA,Haas
E.Transanalminimallyinvasivesurgery:reviewofindications
andoutcomesfrom75consecutivepatients.JAmCollSurg.
2016;222:814–22.
6.ManjónC,SánchezA,PiedraLaraJ,SilvaV,BetriuG,Pe ˜nalver
C,etal.Retroperitonealabscesses–analysisofaseriesof66
cases.ScandJUrolNephrol.2003;37:139–44.
7.OkudaK,OshimaY,SaitoK,UesakaT,TerasakiY,KasaiH,
etal.Midlineextraperitonealapproachforbilateral
widespreadretroperitonealabscessoriginatingfrom
anorectalinfection.IntJSurgCaseRep.2016;19:4–7.
8.StolfiV,MicossiC,SileriP,VenzaM,GaspariA.
Retroperitonealsepsiswithmediastinalandsubcutaneous
emphysemacomplicatingstapledtransanalrectalresection
(STARR).TechColoproctol.2009;13:69–71.
9.ZaveriJ,NathaniR,MathureA.Ano-rectalabscesswith
retro-peritonealspread(acasereport).JPostgradMed.
1987;33:97–8.
10.BignellM,RamwellA,EvansJ,DasturN,SimsonJ.
Complicationsoftransanalendoscopicmicrosurgery(TEMS):
aprospectiveaudit.ColorectalDis.2010;12:99–103.
11.BretagnolF,MerrieA,GeorgeB,WarrenBF,MortensenNJ.
Localexcisionofrectaltumoursbytransanalendoscopic
microsurgery.BrJSurg.2007;94:627–33.
12.HahnloserD,CanteroR,SalgadoG,DindoD,RegaD,DelrioP.
Transanalminimalinvasivesurgeryforrectallesions:should
thedefectbeclosed?ColorectalDis.2015;17:397–402.
13.NouraS,OhueM,MiyoshiN,YasuiM.Significanceofdefect
closurefollowingtransanallocalfull-thicknessexcisionof