HEALTH SERVI CES I N TUBERCULOSI S CONTROL: FAMI LY FOCUS AND
COMMUNI TY ORI ENTATI ON
Sônia Apar ecida da Cr uz Oliv eir a1 Ant onio Ruffino Net t o2 Ter eza Cr ist ina Scat ena Villa3 Silv ia Helena Figueir edo Vendr am ini4 Rubia Laine de Paula Andr ade5 Lúcia Mar ina Scat ena6
Oliveira SAC, Ruffino- Net t o A, Villa TCS, Vendram ini SHF, Andrade RLP, Scat ena LM. Healt h services in t uberculosis cont r ol: fam ily focus and com m unit y or ient at ion. Rev Lat ino- am Enfer m agem 2009 m aio- j unho; 17( 3) : 361- 7.
This st udy aim ed t o assess, according t o pat ient s’ percept ion, t he perform ance of t he Healt h Services responsible for t uberculosis ( TB) cont rol, concerning t he dim ensions fam ily focus and com m unit y orient at ion. A cross- sect ional evaluat ive r esear ch w as car r ied out w it h 108 TB pat ient s. A quest ionnair e developed by St ar field and Macinko w as used, adapt ed for TB care by Villa and Ruffino- Net t o. Result s evidence, in t he first dim ension, t hat healt h pr ofessionals ( HP) ar e concer ned w it h pat ient s’ signs and sy m pt om s; and, at a low er lev el, w it h ot her healt h pr oblem s of r elat iv es, en dan ger in g t h e com pr eh en siv e h ealt h car e. I n t h e secon d dim en sion , HP sh ow lit t le concern with the active search of cases, deficiency in HP training, and low rates of exam ined contacts. Results show the need t o broaden HP’s epidem iological view, as t heir at t ent ion is focused on pat ient s, wit h few prevent ive act ions concerning fam ily/ com m unity. This evidences the need for a closer relationship am ong HP/ patients/ fam ily/ com m unity.
DESCRI PTORS: pr im ar y healt h car e; t uber culosis; healt h ser v ices ev aluat ion
SERVI CI OS DE SALUD PARA CONTROLAR LA TUBERCULOSI S: ENFOQUE EN LA FAMI LI A
Y ORI ENTACI ÓN PARA LA COMUNI DAD
Se evaluó, baj o la per cepción de enfer m os, el desem peño de Ser vicios de Salud r esponsables por cont r olar la t uberculosis ( TB) en las dim ensiones: enfoque en la fam ilia y orient ación para la com unidad. Com o m ét odo, fue ut ilizada la inv est igación ev aluat iv a t r ansv er sal con 108 enfer m os de TB. Se ut ilizó cuest ionar io de St ar field y Macink o, adapt ado par a at ender la TB por Villa y Ruffino- Net t o. Los r esult ados apunt an que, en la pr im er a dim ensión, los profesionales de la salud ( PS) dem uest ran preocupación con señales/ sínt om as de pacient es y, en m enor grado, con ot ros problem as de salud de fam iliares, com prom et iendo el cuidado com plet o. En la segunda dim ensión, los PS m uest ran poca preocupación con la búsqueda act iva de casos, con la deficiencia de capacit ación de PS, y con la baj a t asa de cont act os exam inados. Se concluye que es necesario am pliar la visión epidem iológica de PS, cuya at ención est á focalizada en el enferm o, con pocas acciones prevent ivas sobre fam ilia/ com unidad, lo que m uest r a que es im pr escindible una m ay or apr ox im ación ent r e PS/ enfer m os/ fam iliar es/ com unidad.
DESCRI PTORES: at ención pr im ar ia de salud; t uber culosis; ev aluación de ser v icios de salud
SERVI ÇOS DE SAÚDE NO CONTROLE DA TUBERCULOSE: ENFOQUE NA FAMÍ LI A
E ORI ENTAÇÃO PARA A COMUNI DADE
O obj et ivo dest e est udo foi avaliar, na percepção dos doent es, o desem penho dos Serviços de Saúde responsáveis pelo cont role da t uberculose ( TB) em relação às dim ensões enfoque na fam ília e orient ação para a com unidade. Com o m ét odo, foi u sada a pesqu isa av aliat iv a t r an sv er sal com 1 0 8 doen t es de TB. Ut ilizou - se qu est ion ár io elabor ado por St ar f ield e Macin k o, adapt ado par a a at en ção à TB por Villa e Ru f f in o- Net t o. Os r esu lt ados apont am que, na pr im eir a dim ensão, os pr ofissionais de saúde ( PS) dem onst r am pr eocupação em r elação aos si n a i s/ si n t o m a s d o s p a ci e n t e s e , e m m e n o r g r a u , so b r e o u t r o s p r o b l e m a s d e sa ú d e d o s f a m i l i a r e s, com pr om et endo a int egr alidade do cuidado. Na segunda dim ensão, os PS m ost r am pouca pr eocupação quant o à busca at iva dos casos, deficiência na capacit ação de PS, baixa t axa de cont at os exam inados. Conclui- se pela necessidade de am pliar a v isão epidem iológica dos PS, cuj a at enção est á focalizada no doent e, com poucas ações pr ev en t iv as sobr e a fam ília/ com u n idade, o qu e ev iden cia ser im pr escin dív el m aior apr ox im ação en t r e PS/ d oen t es/ f am iliar es/ com u n id ad e.
DESCRI TORES: at enção pr im ár ia à saúde; t uber culose; av aliação de ser v iços de saúde
Escola de Enferm agem de Ribeirão Pret o, da Universidade de São Paulo, WHO Collaborat ing Cent re for Nursing Research Developm ent , Brazil: 1Mast er’s st udent , e- m ail: [email protected]; 3Full Professor, e- m ail: t it [email protected]; 5RN, e- m ail: [email protected]; 6Ph.D., Professor PRODOC/ CAPES, e- m ail: lm scat [email protected] .br.
Faculdade de Medicina de Ribeirão Pret o, Universidade de São Paulo, Brazil: 2Full Professor, e- m ail: aruffino@fm rp.usp.br.
Faculdade de Medicina de São José do Rio Pret o, Brazil:1Faculty, e- m ail: [email protected]; 4Ph.D., Facult y, e- m ail: [email protected].
I NTRODUCTI ON
I
n t e r a c t i o n a m o n g p a t i e n t s , h e a l t h pr ofessionals ( HP) and com m unit y, as w ell as fam ilyfocus dur ing t he car e pr ocess should be em phasized
t o en su r e com pr eh en siv e an d ef f icien t car e. Healt h services are im port ant in t his cont ext , since t hey can
facilit at e or lim it t heir use by pat ient s w ho dem and
car e. Th u s, d ealin g w it h ch r on ic con d it ion s im p lies o p t i m i zi n g r e so u r ce s t h r o u g h p r e v i o u s p l a n n i n g ,
t r ai n i n g HP i n t ech n i cal an d h u m an p er sp ect i v es,
e m p h a si zi n g p r e v e n t i o n i n se l f - m a n a g e m e n t a n d est a b l i sh i n g st r at eg i es a i m i n g t o i m p r o v e ser v i ce
p er f or m an ce( 1 ).
I t is w or t h highlight ing t hat , dur ing t he last decade, Br azil ex per ien ced gr eat ch an ges in h ealt h
sy st em or g an izat ion . Pr im ar y car e r eceiv ed sp ecial
at t en t ion b ecau se of t h e in t r od u ct ion of in n ov at iv e and st r at egic pr ogr am s t o change t he car e m odel in
t he Unified Healt h Syst em – SUS( 2).
Est ablishing new dim ensions like fam ily focus and com m unit y or ient at ion in pr im ar y car e ser v ices
i s n e c e s s a r y t o s u p p o r t c h a n g e s i n q u a l i t y a n d
st r engt hen com m it m ent and inv olvem ent am ong HP, pat ient s, fam ily and com m unit y. Thus ever y body can
feel like “ act ive subj ect s” in t he search for bet t er living
con dit ion s.
I n 1992, t he World Healt h Organizat ion ( WHO)
declared t uberculosis ( TB) an em ergency in t he world.
Accor d in g t o it s est im at es, on e t h ir d of t h e w or ld
populat ion is infect ed w it h M t uber culosis. Of t hose,
eight m illion w ill develop t he disease and t w o m illion
w ill die every year. Current ly, Brazil is ranked 16t h in
a ranking of 22 count ries concent rat ing 80% of global
TB cases( 1).
St udies show t he need t o creat e alt ernat ives
for TB cont rol focused on part icipat ory, collect ive and
co m p r eh en si v e h ea l t h p r a ct i ce, co n n ect ed t o t h e
com m unit y realit y and able t o surpass t he borders of
t h e h e a l t h u n i t s ( U B S ) . Th e f a m i l y f o c u s a n d
c o m m u n i t y o r i e n t a t i o n d i m e n s i o n s a r e a n e w
p a r a d i g m i n S U S , a n d a r e e s s e n t i a l f o r t h e
reorganizat ion of t he services and in t he Fam ily Healt h
St r at egies. This focus com pulsor ily inv olv es a Healt h
Su r v eillan ce sy st em t h at pr ior it izes t h e su r v eillan ce
of t he space/ populat ion/ fam ily / com m unit y w her e t he
d isease occu r s, in st ead of classic, p at ien t - f ocu sed
su r v eillan ce( 3 - 4 ).
Due t o t he m agnit ude of t uber culosis in t he
abov e consider at ions, t his w or k aim ed t o assess, in
p a t i e n t s ’ p e r c e p t i o n , t h e o r g a n i z a t i o n a l a n d
p er f or m an ce ch ar act er ist ics of t h e h ealt h ser v ices
responsible for t uberculosis cont rol, in t erm s of fam ily focus and com m unit y or ient at ion, in t he cit y of São
José do Rio Pret o, st at e of São Paulo, in 2007.
MATERI AL AND METHOD
Th i s i s an ev al u at i v e, q u an t i t at i v e, cr o
ss-sect ion al r esear ch , u sin g t h e Pr im ar y Healt h Car e
( PHC) d i m en si o n s as t h eo r et i cal f r am ew o r k( 5 ). TB p at ien t s f r om São José d o Rio Pr et o, a cit y in t h e
N o r t h w e s t o f S ã o Pa u l o , B r a z i l , w i t h 4 5 0 0 0 0
inhabit ant s, w er e inquir ed.
The st udy sam ple consist ed of 108 pat ient s,
under follow - up in t he Tuber culosis Cont r ol Pr ogram
( TCP) at t he healt h unit s, from June 2006 t o July 2007. Th e Pr i m a r y Ca r e As s e s s m e n t To o l ( PCAT) w a s
used( 5). This inst rum ent was adapt ed and validat ed in
Brazil for TB car e( 6 ). I n a br oader st u dy, eigh t PHC d i m e n s i o n s w e r e c o n s i d e r e d . I n t h i s s t u d y, t h e
f ollow in g dim en sion s w er e assessed: Fa m ily focu s
( u sin g eig h t in dicat or s – HP ask in f or m at ion ab ou t your life and fam ily circum st ances; about diseases in
your fam ily; if people living t oget her have cough and/
or fever; if a sput um reservoir was given t o all people
in t he house; if healt h professionals know t he people
living wit h t he pat ient ; if t hey t alk t o t hem about your
disease, y our t r eat m ent and ot her healt h pr oblem s)
an d t h e com m u n it y or ie n t a t ion dim en sion ( u sin g
five indicat ors – HP ask if t he services offered t o solve
y o u r h eal t h p r o b l em s; i f y o u h av e ev er o b ser v ed
adv er t isem ent s, cam paigns, educat ional w or k s done
b y HP t o in f or m com m u n it y ab ou t TB; if HP h av e
dev eloped act ions w it h chur ches and associat ions in
t h e n e i g h b o r h o o d t o su p p l y r e se r v o i r s t o co l l e ct
sput um for ex am inat ion; if y ou hav e obser v ed v isit s
of t he HP in t he neighbor hood t o giv e r eser v oir s t o
collect sput um for exam inat ion; and if HP require t he
p a r t i ci p a t i o n o f so m eo n e f r o m t h e co m m u n i t y t o
discuss t he TB pr oblem ) .
I n t er v iew ees an sw er ed qu est ion s accor din g
t o a pr e- est ablished, Lik er t - t y pe scale, r anging fr om
0 t o 5 ( 0 was at t ribut ed t o t he answer “ I do not know”
or “ it does not apply” and values from 1 t o 5 regist ered
t he degree of preference or concordance relat ion wit h
t he st at em ent s) . Befor e dat a collect ion, ex planat or y
s c r i p t s w e r e u s e d t o c l a r i f y p a t i e n t s a b o u t t h e
e x p l a i n e d i n t e r v i e w e e s a b o u t a n sw e r s’ n u m e r i ca l
m ean in g ( 1 t o 5 scor es) , f or in st an ce: n ev er = 1 ;
seldom = 2; som et im es = 3; oft en = 4; always = 5. I n t e r v i e w e r s w e r e t r a i n e d b e f o r e a p p l y i n g t h e
inst r um ent ( quest ionnair e) . Ex plor at or y analy sis w as
u sed t o m easu r e t h e cat eg or ies of an sw er s t o t h e quest ionnair e quest ions, as w ell as t o v er ify possible
i n co n si st e n ci e s i n d a t a b a se s. Ea ch i n d i ca t o r w a s
d ev elop ed t h r ou g h t h e t ot al scor es ( cat eg or ies) of p at ien t s’ an sw er s, d iv id ed b y t h e t ot al n u m b er of
i n t e r v i e w e d p a t i e n t s, r e su l t i n g i n a m e a n v a l u e .
Descr ipt iv e st at ist ics w as used for dat a analy sis. Th e r esear ch p r oj ect w as ap p r ov ed b y t h e
Resear ch Et hics Com m it t ee of t he Univ er sit y of São
Paulo at Ribeir ão Pr et o College of Nur sing, accor ding t o t he guidelines of Resolut ion 196/ 96 CNS ( Nat ional
Healt h Cou n cil) .
RESULTS
Char act er izat ion of TB pat ient s
Of the 108 interviewed patients in the city, 83.3% undergo supervised t reat m ent , of t hose 77.8% in t he
m unicipal reference outpatient clinic, and only 22.2% in
UBS. Of the total, 65.7% are m ale, 66.7% have prim ary
education (com plete or incom plete), 55.6% live in owned
h ou ses an d 9 8 . 1 % l i v e i n m ason r y h ou ses. As t o
socioeconom ic charact erizat ion, m ore t han 95% have piped wat er, refrigerat or, elect ricit y, bat hroom at hom e
and TV, 50% have car and 65% , telephone.
Fa m ily focu s dim e n sion – regards pat ient s
in t heir daily env ir onm ent , t ak ing int o consider at ion
t h at h ealt h n eed s assessm en t sh ou ld con sid er t h e
fam ily cont ex t and any healt h t hr eat , besides coping w it h lim it ed fam ily r esour ces( 5).
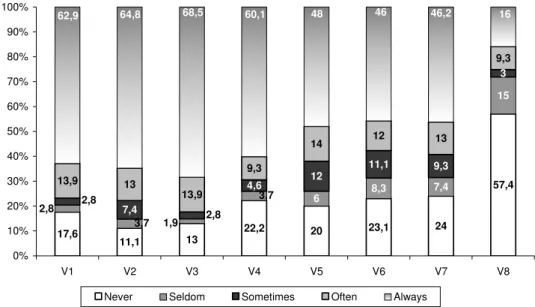
Figur e 1 pr esent s t he fr equency dist r ibut ion
o f a n sw er s r eg a r d i n g ca r e p r o v i d ed b y HP t o TB pat ient s and t heir r elat iv es.
I t i s o b s e r v e d i n Fi g u r e 1 t h a t h e a l t h
pr ofessionals alw ay s ask infor m at ion about pat ient s’ and fam ily’s life circum st ances, about diseases in t he
fam ily, and cough or fever, wit h frequencies of 63, 65
and 69% , r espect ively. These per cent ages r eflect , in a way, t he concern wit h pat ient s and/ or t heir relat ives.
As t o t he supply of reservoir for sput um exam inat ion,
knowledge about relat ives, if HP t alk wit h t hem about t h e d i se a se o r t r e a t m e n t o r a b o u t o t h e r h e a l t h
problem s, “ alw ays” w as answ ered in 60 ( t he Minist ry
of Healt h –MS- suggest s 100% ) , 48, 46, 46 and 16% of cases, r espect ively. Healt h pr ofessionals t alk lit t le
a b o u t o t h e r h e a l t h p r o b l e m s, co m p r o m i si n g t h e
com pr ehensiv e aspect of healt h car e.
Figure 1 – Dist ribut ion of TB pat ient s’ answers regarding t he fam ily focus dim ension variables. São José do Rio
Pr et o, SP, 2007
17,6
11,1 13
22,2 20 23,1 24
57,4
6 8,3
7,4
15
7,4
4,6 12
11,1 9,3
3
13,9 13
13,9
9,3
14 12 13
9,3
3,7 1,9
3,7 2,8
2,8 2,8
16 46,2
46 48
60,1 68,5
64,8 62,9
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
V1 V2 V3 V4 V5 V6 V7 V8
Never Seldom Sometimes Often Always
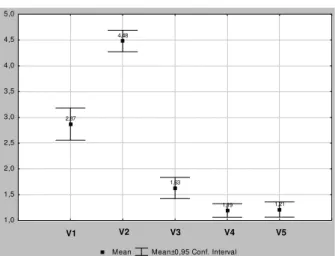
For a bet t er underst anding and illust rat ion of su ch in f or m at ion , Fig u r e 2 p r esen t s t h e v ar iab les’ dist r ibu t ion of t h e con fiden ce in t er v als, w it h r egar d t o t he fam ily focus dim ension.
Mean Mean±0,95 Conf. Interval
4,02
4,17 4,23 3,81
3,64
3,48 3,50
2,11
V70 V71 V72 V73 V74 V75 V76 V77
1 2 3 4 5
V1 V2 V3 V4 V5 V6 V7 V8
Figur e 2 – Dist r ibut ion of t he confidence int er v als of t he variables regarding TB patients’ answers, as to the fam ily focus dim ension, São José do Rio Preto, SP, 2007
I n Figu r e 2 , it is obser v ed t h at v ar iable V3
h ad t h e h igh est scor e, 4 . 2 3 . Th is scor e pr esen t s a
st at ist ically sign if ican t dif f er en ce w it h v ar iables V5 ,
V6 , V7 an d V8 . I t is also obser v ed t h at t h er e is n o
s t a t i s t i c a l l y s i g n i f i c a n t d i f f e r e n c e a m o n g t h e
v ar iables V3 , V4 , V2 an d V1 . On t h e ot h er h an d, it
i s o b se r v e d t h a t t h e V8 v a r i a b l e h a d t h e l o w e st
scor e, t h at is, 2 . 1 1 , st at ist ically sign if ican t dif f er en t
f r om t h e ot h er v ar iab les of t h is d im en sion .
Th e co m m u n i t y o r i e n t a t i o n d i m e n si o n
im p lies t h e ack n ow led g m en t t h at all h ealt h n eed s
of t h e popu lat ion occu r in a specif ic social con t ex t ,
w h i c h s h o u l d b e k n o w n a n d t a k e n i n t o
co n si d er a t i o n( 5 ).
Figu r e 3 pr esen t s t h e f r equ en cy dist r ibu t ion
a s t o t h e k i n d o f c a r e p r o v i d e d b y h e a l t h
p r o f e s s i o n a l s w i t h r e s p e c t t o t h e c o m m u n i t y
o r i en t a t i o n d i m en si o n .
Figur e 3 – Dist r ibut ion of TB pat ient s’ answ er s as t o t he fam ily focus dim ension v ar iables. São José do Rio
Pr et o, SP, 2007
36,1
5,6
65,7
91,7 91,7
4,6
4,6
24,1
12,0
5,6 0,9 1,9
18,5
2,8 9,3
1,9
6,5
8,3
2,8 1,9
1,9 0,9
3,7 75,0
22,2
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
V1 V2 V3 V4 V5
Never Seldom Sometimes Often Always
Legend: V1. Do health professionals (HP) ask if the services offered solve patients’ and family’s health problems? V2. Do patients observe advertisements/campaigns/educational works by HP about TB in the community? V3. Do HP provide reservoirs for sputum examination in neighborhood churches and associations? V4. Do HP visit the community to supply sputum reservoirs? V5. Do HP ask community participation to discuss the problem of TB?
I n t his figure, t he result s of quest ion 2 st ands
o u t , t h a t i s, i f p a t i e n t s o b se r v e a d v e r t i se m e n t s,
cam paigns, et c. car r ied out HP, w it h a fr equency of
75% . All ot her quest ions had v er y low fr equencies.
Figure 4 provides a bet t er underst anding and
illust rat ion of t his inform at ion, wit h t he dist ribut ion of
t h e v a r i a b l e s ’ c o n f i d e n c e i n t e r v a l s , w h a t t h e
Fi g u r e 4 – D i st r i b u t i o n o f v a r i a b l e s’ co n f i d e n ce
in t er v als, w it h r egar d t o TB pat ien t s an sw er s as t o t h e com m u n it y or ien t at ion d im en sion , São José d o
Rio Pret o, SP, 2007
Figure 4 show s t hat t he variable V2 had t he
h i g h e s t s c o r e ( 4 . 4 8 ) . Th i s v a r i a b l e s h o w e d a
st a t i st i ca l l y si g n i f i ca n t d i f f e r e n ce f r o m a l l o t h e r
variables. Next , variable V1 scored 2.87. I n t he sam e
w ay, var iable V3 was also differ en t fr om all ot h er s.
The v ar iables V4 and V5 had equal scor es.
DI SCUSSI ON
Re g a r d i n g t h e s o c i o e c o n o m i c a n d
dem ogr aph ic fact or s, st u dies h av e been car r ied ou t
in t h e sam e cit y, ad d r essin g t h ese ep id em iolog ical
f act or s, f ocu sin g on t h e or g an izat ion of t h e h ealt h
s e r v i c e s a n d s t r u c t u r i n g o f t h e TCP. Th r o u g h
secondary dat a sources, it was observed t hat , despit e
t he sat isfact or y socioeconom ic indicat or s, t he r isk of
get t ing TB is t wo t im es higher in t he area wit h worse
socioeconom ic levels. This show s t he need t o change
t he cur r ent m edical car e st andar d, hum an r esour ces
t r ain in g an d t o r ed ir ect p u b lic p olicies. I d en t if y in g
ar eas w it h d if f er en t TB r isk s allow s t h e m u n icip al
h eal t h sy st em t o d eal w i t h d i f f er en t r eal i t i es an d
p r i o r i t i ze r e g i o n s w i t h a h i g h e r i n ci d e n ce o f t h e
disease( 7 ).
As t o t h e f a m i l y f o cu s d i m en si o n, o n t h e
w h o l e , h e a l t h p r o f e s s i o n a l s a r e c o n c e r n e d w i t h
pat ient s’ signs/ sym pt om s and, t o a lesser ext ent , wit h
f am ily lif e cir cu m st an ces an d d iseases, ev id en cin g
lit t le concern wit h ot her healt h problem s of t he fam ily.
The sear ch for r espir at or y sym pt om at ic ( RS)
p a t i e n t s i n TB c o n t r o l i s c o m p l e x a n d r e q u i r e s
k n o w l ed g e b ey o n d t ech n i cal / sp eci f i c ab i l i t i es. Th e
fam ily appr oach sur passes t he biological k now ledge.
I t is ch ar act er ized by a sequ en ce of act iv it ies t h at i n cl u d e s co n t a ct a t h o m e ; o r i e n t a t i o n a b o u t t h e
disease, signs and sy m pt om s; w ay s of t r ansm ission;
ident ificat ion of RS; orient at ion on sput um collect ion; forwarding and recept ion of t he m at erial by t he Basic
H e a l t h Un i t ( UBS) ; f l o w o f e x a m i n a t i o n s t o t h e
labor at or y ; r eceiv in g r esu lt s by t h e u n it an d u ser s, a n d f o r w a r d i n g d i a g n o se d ca se s f o r f o l l o w - u p i n
out pat ient clinics( 8).
A st udy carried out in São José do Rio Pret o point s out dat a about service organizat ion, and shows
t heir lack of sy st em at izat ion in cont r ol m onit or ing of
TB pat ien t s’ con t act s. Car e is st ill pat ien t - cen t er ed, w i t h l i m i t e d a ct i o n s t o w a r d s co n t a ct s a n d l i t t l e
v alor izat ion of pr ev ent iv e act ions( 9 ).
S h a r e d c o m m i t m e n t , i n v o l v i n g h e a l t h se r v i ce s, p a t i e n t s a n d f a m i l y, i s r e q u i r e d f o r TB
t reat m ent success, t hrough agreem ent s t hat consider
needs of all par t s inv olv ed( 10). Pat ient s and r elat iv es sh ou ld becom e pr ot agon ist s of t h eir ow n t r eat m en t
a n d a ct i v e su b j e ct s i n d e ci si o n - m a k i n g o n t h e i r
t her apeut ic pr oj ect( 11).
I n c l u d i n g r e l a t i v e s i n t r e a t m e n t i s a n
ext rem ely im port ant act ion and should be considered
in all cases. The TCP t eam should w or k j oint ly w it h
t h e UBS a n d PSF/ PACS ( Fa m i l y He a l t h Pr o g r a m /
Com m unit y Healt h Agent s Pr ogr am ) t eam s.
I n t h e co m m u n i t y o r i e n t a t i o n d i m e n si o n,
act ivit ies t hat depend on pat ient s ( i.e.: observing what
i s o f f e r e d i n t e r m s o f a d v e r t i s e m e n t / p o s t e r s /
educat ional m at erial) present ed high scores. The sam e
did not occur wit h t he responsibilit y t o offer services,
su ch a s RS a ct i v e se a r ch i n g t h e co m m u n i t y f o r
s p u t u m c o l l e c t i o n a n d r e q u i r i n g c o m m u n i t y
par t icipat ion t o discu ss TB- r elat ed h ealt h pr oblem s.
H P i n v o l v e m e n t i n a c t i o n s t o s e a r c h f o r RS i s
considered t heir form of part icipat ing in planning and
put t ing t his act ivit y in pract ice( 12).
Bet w een 1 9 9 9 and 2 0 0 3 , t he sear ch for TB
ca se s d e cr e a se d 2 1 % i f co m p a r e d t o t h e p e r i o d
bet w een 1 9 9 6 / 1 9 9 9 , pr obably du e t o t h e em ph asis
of t he Municipal Healt h Secr et ar y on dengue cont r ol,
leav in g TB in secon d place. Accor din g t o t h e WHO,
t he det ect ion rat e of baciliferous cases in TB program s
w it h DOTS v ar ied , in 2 0 0 5 , in t h e d if f er en t w or ld
regions: from 35% in Europe t o 76% in t he West ern
Pacific, and, in Brazil, t he det ect ion rat e of all TB form s
was 73% , in 2005. Mean Mean±0,95 Conf. Interval
2,87
4,48
1,63
1,19 1,21
V78 V79 V80 V81 V82
1,0 1,5 2,0 2,5 3,0 3,5 4,0 4,5 5,0
A st udy carried out in São José do Rio Pret o,
in 2005, show ed low pr oblem solving capacit y in t he
cit y’s Prim ary Healt h Care net work ( det ect ion t hrough spu t u m baciloscopy ) . Bias w as ev iden ced in h ealt h
s e r v i c e s , s i n c e 5 4 % w e r e f o r w a r d e d b y p u b l i c ,
philant hr opic and pr iv at e hospit als, and only 1 0 . 7 % by UBSs( 9).
Lo w p r o b l e m s o l v i n g c a p a c i t y w a s a l s o
ob ser v ed in Ribeir ão Pr et o, f r om 1 9 9 8 t o 2 0 0 6 ( in t h is per iod, t h e per cen t age of baciloscopies car r ied
out varied from 15 t o 26% of t he expect ed) and t he
d et ect ion of n ew cases v ar ied f r om 4 0 t o 8 0 . 5 % . These dat a suggest t he basic healt h net w or k is not
sear ching for RS in t he com m unit y( 12).
Also in Rib eir ão Pr et o, a st u d y car r ied ou t w it h a g r ou p of n u r ses sh ow ed t h ey b eliev ed HP’s
way of act ing, as t o RS, is direct ly relat ed t o t he way
car e is deliv er ed t o pat ien t s. Th e act iv e sear ch f or RS in t he com m unit y occurs in a lim it ed way or t hrough
specific dem ands( 12).
The need t o int roduce new work st rat egies in t he car e m odel, t o r em odel t he “ old” and dev elop a
“ n ew ” sy st em is h igh ligh t ed( 1 3 ). Th e t r adit ion al car e
m o d el n eed s t o b e r ep l aced b y a m o d er n m o d el , i n co r p o r a t i n g p a t i e n t s’ e x p e ct a t i o n s, w i t h a ct i v e
inv olv em ent of fam ilies and or ganized sect or s of t he
com m unit y wit h a view t o a great er inclusion of social
a c t o r s i n t h e d i s e a s e ’ s t r e a t m e n t , t h e m o s t
com pr eh en siv e dim en sion f or t h e con cept ion of t h e
healt h pr om ot ion m odel( 14).
Healt h services ( HS) are organized t o provide
car e in severe condit ions, leaving chr onic diseases in
secon d place. Sev en t y - f iv e per cen t of t h e diseases
t hat occur in Brazil are relat ed t o chronic condit ions( 13).
I n fam ilies facing chr onic healt h condit ions,
bonding bet ween HS and fam ily should be priorit ized.
Alt h ou gh TB is a ch r on ic disease, t h e n eed t o t r ain
h u m an r esou r ces su it able t o ach iev e t h ese aim s is
em p h asized .
The fact ors m ost com m only associat ed t o low
effect iveness are HS’s lack of organizat ion, bad social
condit ions and low t r eat m ent adher ence. TB cont r ol s h o u l d b e u n d e r s t o o d b e y o n d a b i o m e d i c a l
i n t e r v e n t i o n a n d a d d r e s s c o n s i d e r i n g p a t i e n t s ’
perspect ive and t he cont ext of t he healt h pract ices( 15). The part icipat ion of t he organized civil societ y
an d n on - gov er n m en t al or gan izat ion s is essen t ial in
TCP a ct i v i t i es. So ci a l m o v em en t s sh o u l d w o r k t o benefit fr om t r aining oppor t unit ies. Ther e hav e been
a d v a n ce s, su ch a s t h e cr e a t i o n o f t h e Br a z i l i a n
Par t n er sh ip Again st Tu ber cu losis, b y t h e Min ist r y of Healt h, in 2004, proposed by t he St op TB Part nership
in Genev a. Besides t his, t her e is a br oad discussion
o f TB c o n t r o l s t r a t e g i e s i n B r a z i l , t a k i n g i n t o c o n s i d e r a t i o n a r t i c u l a t i o n , i n t e r s e c t o r i a l i t y,
int er disciplinar it y and par t icipat ion of civ il societ y. I n
t he cur r ent cont ex t of t he fight against TB in Br azil, t he per for m ance of t he com m unit y sect or is bey ond
discussion and indispensable( 16).
FI NAL CONSI DERATI ONS AND CONCLUSI ONS
The perform ance of the city in the fam ily focus
dim ension showed that HP are concerned with patients’
signs and sym ptom s and, to a lesser extent, with other
h eal t h p r o b l em s o f t h ei r r el at i v es, en d an g er i n g
com pr ehensiv e healt hcar e. Regar ding t he com m unit y
orient at ion dim ension, it is observed t hat HP are less
concerned with the active search for cases. I n the variable
that requires patient observation of advertisem ents, scores
were high, however, the sam e does not happen for the
offering of services provided by HP.
I t i s i m p o r t a n t t o m e n t i o n t h a t p o o r H P
t raining, few RS and exam ined cont act s, and t he need
for int er v ent ion st r at egies t o im pr ov e t he qualit y of
t h e ser v ices of f er ed t o p at ien t s ar e asp ect s w or t h
highlight ing.
REFERENCES
1. Or ganização Mundial da Saúde. Cuidados inovador es par a co n d i çõ e s cr ô n i ca s: co m p o n e n t e s e st r u t u r a i s d e a çã o : r elat ór io m u n dial. Br asília ( DF) : OPAS/ OMS; 2 0 0 3 . 2 . Villa TCS, Ru f f in o A Net t o, Ar cên cio RA, Gon zales RI C. As p o l ít i ca s d e co n t r o l e d a t u b e r cu l o se n o si st e m a d e s a ú d e n o B r a s i l e a i m p l a n t a ç ã o d a e s t r a t é g i a D O TS ( 1 9 8 0 - 2 0 0 5 ) . I n : Villa TCS, Ru f f in o A Net t o. Tu b er cu lose: i m p l a n t a ç ã o d o D O TS e m a l g u m a s r e g i õ e s d o B r a s i l : h ist ór ico e p ecu liar id ad es r eg ion ais. Rib eir ão Pr et o ( SP) :
FMRP/ USP; 2 0 0 6 . p . 2 9 - 4 7 .
3 . Ru f f in o- Net t o A. Pr og r am a d e Con t r ole d a Tu b er cu lose n o B r a s i l : s i t u a ç ã o a t u a l e n o v a s p e r s p e c t i v a s . I n f Ep i d e m i o l SUS 2 0 0 1 ; 1 0 ( 3 ) : 1 2 9 - 3 8 .
4 . Men d es EV. Um n ov o p ar ad ig m a san it ár io: a p r od u ção so ci al d a saú d e: u m a ag en d a p ar a a saú d e. 2 ª ed . São Pa u l o ( SP) : Hu ci t e c; 1 9 9 9 .
6 . Villa TCS, Ru f f in o- Net t o A. Qu est ion ár io p ar a av aliação d e d esem p en h o d e ser v iços d e at en ção b ásica n o con t r ole d a t u b er cu lose n o Br asil. J Br as Pn eu m ol j u n 2 0 0 9 ; 3 5 ( 6 ) no pr elo.
7 . Ve n d r a m i n i S H F, S a n t o s M L S G , G a z e t t a C E, Ch i a r av a l l o t i - Ne t o F, Ru f f i n o - Ne t t o A. Tu b e r cu l o si s r i sk s a n d so ci o - eco n o m i c l ev el : a ca se st u d y o f a ci t y i n t h e Br a zi l i a n so u t h - e a st , 1 9 9 8 - 2 0 0 4 . I n t J Tu b e r c Lu n g D i s 2 0 0 6 ; 1 0 ( 1 1 ) : 1 2 3 1 - 5 .
8. Nogueira J, Ruffino A Net t o, Monroe AA, Cardoso Gonzales RI , Villa TCS. Bu sca at iv a de sin t om át icos r espir at ór ios n o cont role da t uberculose na percepção do Agent e Com unit ário de Saúde. Rev Elet r Enfer m 2 0 0 7 ; 9 ( 0 1 ) : 1 0 6 - 1 8 .
9. Gazet t a CE, Sant os ML, Vendr am ini SH, Polet t i NA, Pint o Net o JM, Villa TCS. Tuber culosis cont act cont r ol I n Brazil: a lit er at ur e Rev iew ( 1 9 8 4 - 2 0 0 4 ) . Rev Lat ino- am Enfer m agem 2 0 0 8 ; 1 6 ( 2 ) : 3 0 6 – 1 3 .
1 0 . Sa LD, Sou za KMJ, Nu n es MG, Palh a PF, Nog u eir a JA, Villa TCS. Trat am ent o da t uber culose em unidades de saúde da fam ília: hist ór ia de abandono. Tex t o Cont ex t o – Enfer m 2 0 0 7 ; 1 6 ( 4 ) : 7 1 2 - 8 .
11. Arcêncio RA. A organização do t rat am ent o supervisionado n o s 3 6 m u n i cíp i o s p r i o r i t á r i o s d o Est a d o d e Sã o Pa u l o :
f aci l i d ad es e d i f i cu l d ad es ( 2 0 0 5 ) . [ d i sser t ação ] . Ri b ei r ão Pr et o ( SP) : Escola de En f er m agem de Ribeir ão Pr et o/ USP; 2 0 0 6 .
1 2 . Mu n iz JN, Palh a PF, Mor oe AA, Car d ozo Gon záles RI , Ruffino Net t o A, Villa TCS. A incorporação da busca at iva de sint om át icos r espir at ór ios par a o cont r ole da t uber culose na prát ica do agent e com unit ário da saúde. Ciênc Saúde Colet iva 2 0 0 5 ; 1 0 ( 2 ) : 3 1 5 - 2 1 .
1 3 . Men des EV. At en ção pr im ár ia à saú de n o SUS. Cear á: Escola de Saú de Pú blica; 2 0 0 2 .
1 4 . Lim a MB, Mello DA, Mor ais APP, Silv a WC. Est u d o d e c a s o s o b r e o a b a n d o n o d a t u b e r c u l o s e : a v a l i a ç ã o d o at endim ent o, per cepção e conhecim ent os sobr e a doença na perspect iva dos client es ( Fort aleza, Ceará, Brasil) . Cad Saúde Pú b l i ca 2 0 0 1 ; 1 7 ( 4 ) : 8 7 7 - 8 5 .
1 5 . Sou za FBA, Villa TCS, Cav alcan t e SC, Ru f f in o Net o A, Lo p e s LB , Co n d e M B . Pe c u l i a r i d a d e s d o c o n t r o l e d a t u b er cu l o se em u m can ár i o d e v i o l ên ci a u r b an a d e u m a com unidade carent e do Rio de Janeiro. J Bras Pneum ol 2007; 3 3 ( 3 ) : 3 1 8 - 2 2 .
16. Sant os ET Filho, Gom es ZMS. Est rat égias de cont role da t uberculose no Brasil: art iculação e part icipação da sociedade civ il. Rev Saúde Pública 2007 set em br o; 41( supl. 1) : 111- 6.