w w w . r b o . o r g . b r
Review
Article
Advances
in
treating
exposed
fractures
夽
Pedro
Nogueira
Giglio
∗,
Alexandre
Fogac¸a
Cristante,
José
Ricardo
Pécora,
Camilo
Partezani
Helito,
Ana
Lucia
Lei
Munhoz
Lima,
Jorge
dos
Santos
Silva
DepartmentofOrthopedicsandTraumatology,HospitaldasClínicas,SchoolofMedicine,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11April2014 Accepted1May2014
Availableonline26February2015
Keywords:
Exposedfractures/diagnosis Exposedfractures/classification Woundsandinjuries
a
b
s
t
r
a
c
t
Themanagementofexposedfractureshasbeendiscussedsinceancienttimesandremains ofgreatinteresttopresent-dayorthopedicsandtraumatology.Theseinjuriesarestilla challenge.Infectionandnonunionarefearedcomplications.Aspectsofthediagnosis, clas-sificationandinitialmanagementarediscussedhere.Earlyadministrationofantibiotics, surgicalcleaningandmeticulousdebridementareessential.Thesystemicconditionsof patientswithmultipletraumaandthelocalconditionsofthelimbaffectedneedtobetaken intoconsideration.Earlyskeletalstabilizationisnecessary.Definitivefixationshouldbe con-sideredwhenpossibleandprovisionalfixationmethodsshouldbeusedwhennecessary. Earlyclosureshouldbetheaim,andflapscanbeusedforthispurpose.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Avanc¸os
no
tratamento
das
fraturas
expostas
Palavras-chave:
Fraturasexpostas/diagnóstico Fraturasexpostas/classificac¸ão Ferimentoselesões
r
e
s
u
m
o
Omanejodasfraturasexpostasédiscutidodesdeaantiguidadeepermanecedegrande interessedaortopediaedatraumatologiamodernas.Sãolesõesaindadesafiadoras.Infecc¸ão enãouniãosãocomplicac¸õestemidas.Aspectosnodiagnóstico,classificac¸ãoemanejo inicialsãodiscutidos.Sãoessenciaisaadministrac¸ãoprecocedeantibióticos,alimpeza cirúrgicaeodebridamentometiculoso.Devemserlevadasemconsiderac¸ãoascondic¸ões sistêmicasdopacientepolitraumatizadoeascondic¸õeslocaisdomembroacometido.A estabilizac¸ãoesqueléticaprecoceénecessária.Afixac¸ãodefinitivadeveserconsiderada quandopossívelemétodosdefixac¸ãoprovisóriadevemserusadosquandonecessário.O fechamentoprecocedeveseralmejadoepode-sefazerusoderetalhosparaessefim.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
夽
WorkdevelopedattheInstituteofOrthopedicsandTraumatology,HospitaldasClínicas,SchoolofMedicine,UniversidadedeSão Paulo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](P.N.Giglio). http://dx.doi.org/10.1016/j.rboe.2015.02.009
Introduction
According to the historian Castiglione,1 orthopedics origi-nated“fromtheneedforimmediateassistance,evenifusing coarseempiricalinstruments”.
Althoughtheterm“orthopedics”wasonlycreatedbyAndry (1741)apudMaia,2evidenceoforthopedicprocedurescanbe seenintheancient archeologicalrecords fromour civiliza-tions.Itislikelythatmanyofthemnotonlyhadtherapeutic objectives but also involved some type of magic, such as trepanationperformedtoreleasethedemonsthatcausedthe diseasesandmalaisesofthatera.1
Thereisaconsensusamonghistoriansthattimesofwar havebeen fundamental forthedevelopmentand improve-mentoforthopedics.3
Definition
Exposedfracturesarethosethatpresentcommunicationwith theexternalenvironmentthroughasoft-tissuelesion.4These situationsareconsideredtobeorthopedicemergencies5and theaimofthetreatmentinsuchcasesistoenable consolida-tionwithoutoccurrencesofinfection.
Alargeproportionofexposedfracturesshowevident expo-sureatthetimeoftheirinitialpresentation.However,insome ofthesecases,itmaybeunclearwhetherthereiscontiguity betweenthefocusofthefractureandtheexternal environ-ment.Thus,it isrecommended thatit should beassumed thatthefractureisexposed,wheneversoft-tissuelesionsare present,adjacenttothefocusofthefracture.6
History
Thefirstdiscussionsregardingtreatmentsforexposed frac-tures date back to Hippocrates, who advocated that the treatmentshouldcompriseocclusivedressingsafter improve-mentoftheedemaanddebridementofthepurulentmaterial coming from the exposure.7 Galeno, apud Wangensteen,8 believedthatthepurulencewasinvolvedinthehealing pro-cess and therefore should be stimulated. In the sixteenth century,BrunschwigandBotello,apudTrueta,9werethefirst toobservethebenefitsofremovalofthedevitalizedtissue.
A physician in the French army named Paré (1517–90),
apud Castiglione,1 rejected the practice oftreating wounds andexposedfractureswithboilingoil,whichhadbeenoneof thepreceptsputforwardbyHippocrates.Instead,heobserved thattheevolutionwasmoresatisfactoryincasesinwhichthe woundwassimplycleanedandclosed.Paré,apudTrueta,9also observedthattherewasaneedtoexpandthewoundsinthe fracturedlimbs,inordertoallowfreedrainageofthematerial comingfromtheinjury.
In the eighteenth century, Desault also recommended, along with Botello and Brunschwig apud Trueta,9 that the necrotictissueinwoundsshouldbecleanedoutandremoved. Thisprocedurebecameknownasdebridement.Desault,apud
Trueta,9alsoobservedthatthetimeatwhichdebridementwas performedwasfundamentallyimportantfortheprognosisof thelesion.
The Second World War greatly contributed toward advances in treatments for exposed fractures. Widespread useofantibioticsdatesfromthisperiod.10DuringtheKorean and Vietnamwars, methodsfor temporary immobilization weredeveloped,alongwithsteriledressings,broad-spectrum antibiotics, debridement techniques, irrigation with saline solution and sequential approaches toward lesions. These servedasthefoundationforthemethodsusedtoday.10
Overthelastfewyears,theroleoftheAmericanCollegeof Surgeonscanbehighlighted.Thisbodyestablishedthe prin-ciplesoftheattendancesequenceknownasadvancedtrauma lifesupport(ATLS),whichproviderulesforpre-hospitaland hospitalcareformultiple-traumapatients,oftenpresenting exposedfractures.11
Diagnosis
Diagnosingexposedfracturesisnotalwaysanobvious mat-ter. Therefore, if skin lesions are observed on a fractured limb,thefirstprinciples fortreatingsuchfracturesneedto befollowed.12
Clinically, thediagnosis canbemade throughobserving the fracturedsegmentvia thewound.However,incasesof doubtfuldiagnoses,suchasinpunctiformorcontusedlesions, dropletsoffatthatarepresentinthebloodcomingoutofthe woundmaysuggestthisdiagnosis.Radiographically, subcu-taneousemphysemaseenonsimpleradiographsorimages suggestiveofthepresentofgasatthefocusofthefracture maycontributetowardthediagnosis.13
An accurate physical examination, including inspection and palpation of bone protuberances, is fundamental for the initialmanagementofthesepatients.Themusculature involvedshouldbeassessed;theexistenceofpulseand per-fusion alterationsshould beinvestigatedfrom thecoloring andtemperatureoftheextremities;andaneurological exam-ination should beperformed in orderto assess sensitivity, motricityandreflexes.Thesestepswillhelpinclassifyingthe lesionsandinmakinganearlydiagnosisofpossible compli-cations,suchascompartmentalsyndrome.14
Measurementofthecompartmentpressuremaybeuseful incasesinwhichthereissomedoubtregardingthe occur-rence of compartment syndrome.15 Ultrasonography with colorDopplermaybeusefulinmakingdiagnosticevaluations onsuspectedvascularlesionsandcanbecomplementedwith arteriography.16
Radiographscoveringtheentirefracturedsegment, includ-ing the joints proximal and distal to the fracture, are fundamentalforcharacterizingthefractureandforestimating thelevelofenergythatwasinvolvedintheinitialtrauma.17,18 Computedtomographymayberequestedincasesoffractures inwhichthejointsurfacesarecompromised,inordertoplan the surgerymore adequately,19 after emergency treatment measureshavebeenimplemented.
Classification
Table1–Gustiloclassificationforexposedfractures.
I–Lowenergy,exposurelessthan1cm,lowdegreesof
contaminationandcomminution.
II–Exposureofbetween1cmand10cm,contamination,
soft-tissueinjuryandmoderatecomminution.
III–Exposuregreaterthan10cm,highdegreeofsoft-tissue
injuryandcontamination. IIIA–Primarycoverageispossible. IIIB–Primarycoverageisnotpossible. IIIC–Arterialinjuryrequiringrepair.
The Gustilo classification, which is the one most used
nowadays,takesintoconsiderationtheenergyofthetrauma, thedegreeofsoft-tissueinjuryandthedegreeof contamina-tion,whichallhaveprognosticimplicationsand definethe treatment20,21(Table1).
The AO group (Arbeitsgemeinschaft für Osteosynthese-fragen)22hasalsodevelopedaclassificationsystem(Table2) forexposedfractures.Thissystem,alongwiththatof Tsch-erneandOuster23(Table3),alsoemphasizestheimportanceof soft-tissueinjuries,evenintheabsenceofcontiguitysolution withtheenvironment.
Advances
in
treating
exposed
fractures
Treatment of exposed fractures constitutes an orthopedic emergency and this should be included in the sequential attendance for multiple-trauma cases that is recognized within ATLS.24 Initially, efforts should be directed toward ensuringthepatient’ssurvivalandtheso-calledABCDEofthe traumashouldbeperformed25(Table4).
Table2–AOclassificationforsoft-tissueinjuryin
exposedfracturecases.
Skininjury
IO1–Punctiformskininjuryfrominsidetooutside. IO2–Skininjurywithcontusededgesfromoutsideto inside,smallerthan5cm.
IO3–Skininjurylargerthan5cm,withdevitalizededge. IO4–Injuryencompassingthefullthickness,withsevere contusion,lossofskinorextensivedegloving.
Muscleinjury
MT1–Nomuscleinjury.
MT2–Circumscribedmuscleinjury,inonecompartment only.
MT3–Considerablemuscleinjury,intwocompartments. MT4–Muscledefect,tendonlacerationandextensive contusion.
MT5–Compartmentalsyndrome,crushingsyndromeand broadinjuryzone.
Neurovascularinjury
NV1–Noneurovascularinjury. NV2–Isolateneurologicalinjury. NV3–Localizedvascularinjury.
NV4–Extensivesegmentalvascularinjury.
NV5–Combinedneurovascularinjury,includingsubtotalor totalamputation.
Table3–Tcherneclassificationforsoft-tissueinjuries
associatedwithexposedfractures.
Fr.1–Skinlaceratedbybonefrominsidetooutside,littleorno skincontusionandsimplefracturesresultingfromindirect trauma.
Fr.2–Skinlacerationorcircumferentialcontusionand moderatecontamination,includingallcasesexposeddueto directtrauma.
Fr.3–Extensivesoft-tissueinjuries,generallyassociatedwith vascularorneurologicalinjury.Includesfracturesrelatingto ischemia,severebonecomminution,compartment syndrome,injuriesinruralsettingsandhigh-velocity gunshotwounds.
Fr.4–Partialortotalamputations(separationofimportant anatomicalstructures,especiallyvessels,withtotal ischemia).
Table4–Sequenceofinitialattendanceformultiple
traumavictimsaccordingtotheATLS.
A–Keeptheairwaysopenandprotectthecervicalspine. B–Maintainadequateventilation.
C–Ensurecirculationandperfusion. D–Evaluateneurologicalinjuries.
E–Withwiderexposure,assessotherinjuriesandprotect againsthypothermia.
All individualswho haveinjuriestomorethanone
sys-temicorgan,suchthatatleastoneofthemislife-threatening orhasascoreofmorethan16intheinjuryseverityscore(ISS), shouldbeconsideredtobemultiple-traumacases.26,27
For multiple-trauma patients, becauseof the significant immunologicalresponse,thetreatmentshouldbesequenced intofourparts25(Table5).
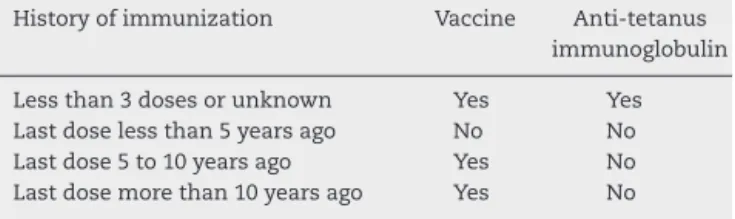
Thetreatmentforexposedfracturesisstartedatthe emer-gency service. After the patient has been brought to the emergency room, and as soon as the clinical stabilization phasehasbeenfinished,anorthopedicexaminationshould beconducted.Allthefindingsshouldbedocumentedinthe medicalfile,withphotosifpossible,andtheareaofexposure shouldbeprotectedwithasteriledressing.Multiple reevalu-ations ofthe woundare notrecommended,giventhat this has been correlated with greater risk of infection.28 Anti-tetanus prophylaxis shouldbeadministered,depending on the patient’svaccinationstatusandthedegreeof contami-nationofthewound29(Table6).
Assoonasvenousaccesscanbeachieved,antibiotic pro-phylaxis should be started.30 For Gustilo type I fractures, first-generationcephalosporinshouldbeprescribed,whilefor typeII orIII fractures,gentamicinand clindamycinshould beprescribed,foraninitialperiodof14days.Thislengthof
Table5–Phasesofsequentialattendanceformultiple
traumavictims.
1stphase–Resuscitation(firsthours)
Table6–Recommendationsforprophylaxisagainst
tetanusinhigh-riskwounds.a
Historyofimmunization Vaccine Anti-tetanus immunoglobulin
Lessthan3dosesorunknown Yes Yes Lastdoselessthan5yearsago No No Lastdose5to10yearsago Yes No Lastdosemorethan10yearsago Yes No
a High-risk wounds include exposed fractures, wounds due to
firearmsorcoldweapons,woundswithretentionofaforeignbody andpunctiformwoundscausedbysharpobjects.
timemay be extended, dependingon the patient’s clinical
evolution.29 Collectionofculturingmaterialfromtheinitial debridementhasbeenquestionedbecauseofthelow correla-tionbetweenthemicroorganismsisolatedfromthisandthe realcausativeagentsofpossibleinfections.31
Aftertheinitialclinicalstabilization,thepatientistaken tothesurgicalcenterforlocaltreatmentofthefracture.The woundisfirstlycoveredandasepsisandantisepsisare per-formedontheentirelimb.Afterthis,thewoundisuncovered and,ifnecessary,extendedinordertoviewthedeeptissues better. Irrigationwithsimplephysiologicalserum is imple-mented,usuallywithavolumeofaround 10L.Thiscanbe increased if necessary, until no more debris and dirt can beseen.Thisprocess aimsto diminishthe absolute num-berofcontaminating bacteriaand removedirtthat cannot beremoved manually.32 Afterthis irrigationhasbeen com-pleted,thesurgicalscrubsarechangedandnewantisepsisis implemented.Debridementofthedevitalizedtissuesisthen performed.Themusclesareevaluatedwithregardtocolor, consistency,contractilityandcapacityforbleeding.33Muscles thatdonotpresentthesecriteriahaveahigherchanceofbeing unrecoverable.Tendonsshouldbepreservedwhenever possi-ble,exceptincasesinwhichthereistotallossoftheirfunction orgrosscontamination.34,35
Somefractures,becauseoftheirhighdegreeofinitial con-tamination,require another debridement procedure within 48hafterthefirstsurgicalcleaning,whichisknownasa “sec-ondlook”atthelesion.36
Aftercompletingthesurgicalcleaninganddebridementof thetissues,stabilizationofthefractureisperformed.Theaims ofthisstagearetorestorethelengthandalignmentofthe limb,reconstructthe jointsurfaceinvolvedand protectthe softtissues.37Thedifferentfixationmethodsshouldenable easy access to the surgical wound and early mobilization. Immobilizationinaplastercastdoesnotservethese objec-tives,especiallybecausethismakesitdifficulttoaccessthe wound.Therefore,plastercastsshouldnotbeusedforthis purpose.
Immediatedefinitivefixationofthefracturemaybe per-formedatthe emergency service ifthe localand systemic conditionsallowthis,i.e. insituations ofabsencesof soft-tissuelesions,majorcontaminationandclinicalinstability.12 Thisapproachisknownasearlytotalcare.Classically, imme-diateinternalfixationwasonlyanoptionifdonewithinthe first6hafterthetrauma.38However,reviewsoftheliterature conductedmorerecentlyhaveshownthatdebridement fol-lowedbydefinitivefixationattheemergencyservicecanbe
doneafterthis6-hperiod,withoutanyincreaseinthe inci-denceofinfection.39
Incasesinwhichdefinitivefixationisnotpossible,external fixationhasbeenshowntobethefixationmethodthatismost suitableforstabilizingexposedfracturesinlongbones, includ-ingwithinthecontactofso-called“damagecontrol”.Thisisa rapidandminimallyinvasivemeansofprovidingstabilityand restoringthealignmentandlengthofthelimb.Itcontributes towarddiminishingtheinflammatoryresponserelatingtothe trauma, avoidssubsequent damagetothe softtissues and enableseasyaccesstothewound,bothfordressingsandfor surgicalproceduresforsubsequentskincoverage.4,12,40
Oneimportantconsiderationinusingexternalfixators con-cernstheirconversiontoaninternalfixationmethod(plate orintramedullarynail). Intheliterature,ithasbeenshown thatawindowofopportunityexistsbetweentheseventhand fourteenthdaysafterinstallationoftheexternalfixation,for conversiontobeimplemented.37Afterthisperiod,theriskof infectionwithinternalosteosynthesisbecomesgreater,such that it is recommended that decontamination of the path of the externalfixation pins should beperformed through exchangingthem,before performingthe definitiveinternal fixation.
Theskincoverageincasesofexposedfracturesisanother topic with a diversity of opinions. One option is to per-formimmediateprimaryclosure.Alternatively,thiscouldbe delayedfor48–72h.Thefirstoptioncanbeimplementedin casesofsmallwoundswithlittlecontamination,providedthat thereisnotensionontheedgesofthewound(whichwould leadtoariskofcontaminationthroughanaerobicbacteria), andthatadministrationofantibioticsisstartedwithinthefirst 12hafterthefracturing.41Second-intentclosureisonlyrarely performedbuthasrecentlypresentedbetterresults,thanksto theadventofvacuumdressings.42
Closurebymeansofgraftsorflapscanalsobeused.The development oflocalflap rotation techniquesand the dis-seminationofmicrosurgicalflaptechniqueshavehadamajor impactontheprognosisforcasesofexposedfractures,given thattheyhaveenabledstablegood-qualityskincoverageand thushavedecreasedtheinfectionratesandincreasedthe frac-tureconsolidationrates.43
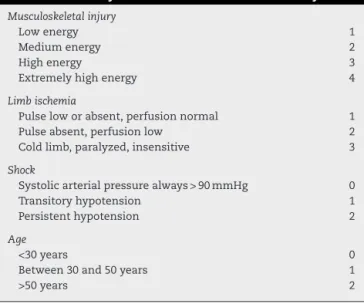
Table7–Severityscoreformutilationofextremity.
Musculoskeletalinjury
Lowenergy 1
Mediumenergy 2
Highenergy 3
Extremelyhighenergy 4
Limbischemia
Pulseloworabsent,perfusionnormal 1
Pulseabsent,perfusionlow 2
Coldlimb,paralyzed,insensitive 3
Shock
Systolicarterialpressurealways>90mmHg 0
Transitoryhypotension 1
Persistenthypotension 2
Age
<30years 0
Between30and50years 1
>50years 2
ofsevenpointsormoreonthisscalesignifiesapredictionof amputationof100%.25
Expectations
Treatmentsforexposedfracturesarecontinuingtoadvance. Theadvancesthatcanbeexpectedincludedevelopmentof theuseofmesenchymalcells,whichwouldincreasethe con-solidation successrates;dissemination oftheuse ofgrafts comingfromtissuebanks;anddevelopmentofreplacement bones48 and growth factors,49,50 which would reduce the obstacles and the time needed for treating patients with exposedfractures,therebyrestoringtheirsocialand occupa-tionalfunctionswithinashortertime.Inparallel,continual improvementofprosthesesmayserveasencouragementfor patientswhosufferedseveretraumathatresultedin ampu-tation,suchthattheseindividualsmightbecomefunctional andproductiveagain.51
Final
remarks
Aspresentedabove,manyadvancesintreatmentsforexposed fractureshavebeenattained.Themainpointsregardingthis progressareasfollows:
1. Attendanceformultipletraumavictimshasbecome sys-tematized,withthecreationofwell-definedmanagement protocolsgoingfromthepre-hospitalphasetothehospital phase.Thishasmadeitpossibleforpatientstobebrought morerapidlytoreferralcentersfortraumacare,inabetter stabilizedcondition.
2. Morehospitalcenters havebecomeequippedtoprovide careforsuchpatients.
3. Awareness that exposed fractures constitute a medical emergency has become greater among the physicians responsiblefortheinitialmanagementofmultipletrauma victims.
4. Antibioticshaveundergonedevelopment.
5. Fracturefixationtechniqueshavedeveloped,withtheuse ofexternalfixationforcontrollingdamageanddefinitive fixationwhen thepatient’s systemic conditionsand the locationofthefractureonthelimballowthis.
6. Surgicaltechniquesforconstructinglocalflapsand micro-surgicaltechniqueshavedevelopedandphysicianswith the capacity to perform these procedures have been trained,therebyassuringstableskincoverageforpatients withexposedfractures.
7. Therehavebeenadvancesinthetechniquesfordressings, amongwhichthedevelopmentofvacuumdressingscanbe highlighted,thusenablingbetterlocalcontroloverwounds.
Nonetheless,theseinjuriescontinuetoposeachallenge, withthepossibilityoffearedcomplications,suchasinfection andnon-consolidation,alongwiththeinherentdifficultyof dealingwithhigh-energyinjurieswithsignificantboneand soft-tissueimpairment.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.CastiglioneA.Ahistóriadamedicina.SãoPaulo:Companhia EditoraNacional;1947.
2.MaiaABS.Bibliografiabrasileiradeortopediaetraumatologia 1797–1977.Recife:EditoradaUniversidadedePernambuco; 1967.
3.NapoliM,BlancC.Ortopediabrasileira–Momentos,crônicas efatos.SãoPaulo:SociedadeBrasileiradeOrtopediae Traumatologia;2000.
4.CrossWW3rd,SwiontkowskiMF.Treatmentprinciplesinthe managementofopenfractures.IndianJOrthop.
2008;42(4):377–86.
5.Jorge-MoraA,Rodriguez-MartinJ,Pretell-MazziniJ.Timing issueinopenfracturesdebridement:areviewarticle.EurJ OrthopSurgTraumatol.2013;23(2):125–9.
6.KeeseGR,BoodyAR,WongworawatMD,JobeCM.The accuracyofthesalineloadtestinthediagnosisoftraumatic kneearthrotomies.JOrthopTrauma.2007;21(7):442–3. 7.PapeHC,WebbLX.Historyofopenwouldandfracture treatment.JOrthopTrauma.2008;22(Suppl10):S133–4. 8.WangensteenOH,WangensteenSD.Theriseofsurgeryfrom
empiriccrafttoscientificdiscipline.Minneapolis:University ofMinnesotaPress;1978.
9.TruetaJ.“Closed”treatmentofwarfractures.Lancet. 1939;1(6043):1452–5.
10.HauserCJ,AdamsCAJr,EachempatiSR.Surgicalinfection societyguideline:prophylacticantibioticuseinopen fractures:anevidence-basedguideline.SurgInfect(Larchmt). 2006;(74):379–405.
11.FrinkM,ZeckeyC,MommsenP,HaasperC,KrettekC, HildebrandF.Polytraumamanagement–asinglecentre experience.Injury.2009;40(Suppl4):S5–11.
12.DunbarRP,GardnerMJ.Initialmanagementofopenfractures. In:BucholzRW,HeckmanJD,Court-BrownCM,TornettaP, editors.RockwoodandGreen’sfracturesinadults.7thed. Philadelphia:Lippincott:Williams&Wilkins;2010.p.285. 13.AufrancOE,JonesWN,BierbaumBE.Gasgangrene
14.TurenCH,BurgessAR,VancoB.Skeletalstabilizationfortibial fracturesassociatedwithacutecompartmentsyndrome.Clin OrthopRelatRes.1995;(315):163–8.
15.McQueenMM,Court-BrownCM.Compartmentmonitoringin tibialfractures.Thepressurethresholdfordecompression.J BoneJointSurgBr.1996;78(1):99–104.
16.HalvorsonJJ,AnzA,LangfittM,DeonananJK,ScottA, TeasdallRD,etal.Vascularinjuryassociatedwithextremity trauma:initialdiagnosisandmanagement.JAmAcadOrthop Surg.2011;19(8):495–504.
17.GarbuzDS,MasriBA,EsdaileJ,DuncanCP.Classification systemsinorthopaedics.JAmAcadOrthopSurg. 2002;10(4):290–7.
18.MartinJS,MarshJL.Currentclassificationoffractures. Rationaleandutility.RadiolClinNorthAm.
1997;35(3):491–506.
19.WuerzTH,GurdDP.Pediatricphysealanklefracture.JAm AcadOrthopSurg.2013;21(4):234–44.
20.GustiloRN,MendozaRM,WilliansDN.Problemsinthe managementoftypeIII(severe)openfractures:anew classificationoftypeIIIopenfractures.JTrauma. 1984;24(8):742–6.
21.GustiloRB,AndersonJT.Preventionofinfectioninthe treatmentofonethousandandtwenty-fiveopenfracturesof longbones:retrospectiveandprospectiveanalyses.JBone JointSurgAm.1976;58(4):453–8.
22.RüediTP,BuckleyRE,MoranCG.AOprinciplesoffracture management.2nded.Stuttgart/NewYork:GeorgThieme Verlag;2007.
23.TscherneH,OusterHJ.Anewclassificationofsoft-tissue damageinopenandclosedfractures.Unfallheikunde. 1982;85(3):111–5.
24.GiannoudisPV,PapeHC.Managementofthemultiplyinjured patient.In:BucholzRW,HeckmanJD,Court-BrownCM, TornettaP,editors.RockwoodandGreen’sfracturesinadults. 7thed.Philadelphia:Lippincott:Williams&Wilkins;2010.p. 261–7.
25.TheAmericanCollegeofSurgeons.AdvancedTraumaLife Support(ATLS)studentsmanual.6thed.Chicago:American CollegeofSurgeons;1997.
26.AmericanCollegeofSurgeons/CommitteeofTrauma. NationalTraumaDataBankannualreport2005,dataset version5.0.Chicago:AmericanCollegeofSurgeons CommitteeonTrauma;2005.
27.BakerSP,O’NeillB,HaddonWJr,LongWB.Theinjuryseverity score:amethodfordescribingpatientswithmultipleinjuries andevaluatingemergencycare.JTrauma.1974;14(3):187–96. 28.PetersonN,StevensonH,SahniV.Sizematters:howaccurate
isclinicalestimationoftraumaticwoundsize?Injury. 2014;45(1):232–6.
29.Subcomissãodecontroledeinfecc¸ãohospitalarIOT. Padronizac¸ãodousodeantimicrobianos–2012/2013.São Paulo:HospitaldasClínicasdaFaculdadedeMedicinade UniversidadedeSãoPaulo;2012.
30.ProkuskiL.Prophylacticantibioticsinorthopaedicsurgery.J AmAcadOrthopSurg.2008;16(5):283–93.
31.ValenzianoCP,Chattar-CoraD,O’NeillA,HubliEH,CudjoeEA. Efficacyofprimarywoundculturesinlongboneopen extremityfractures:aretheyofanyvalue?ArchOrthop TraumaSurg.2002;122(5):259–61.
32.AnglenJO.Woundirrigationinmusculoskeletalinjury.JAm AcadOrthopSurg.2001;9(4):219–26.
33.ArtzCP,SakoY,ScullyRE.Anevaluationofthesurgeon’s criteriafordeterminingtheviabilityofmuscleduring débridement.AMAArchSurg.1956;73(6):1031–5.
34.OlsonSA,SchemitschEH.Openfracturesofthetibialshaft: anupdate.InstrCourseLect.2003;52:623–31.
35.TscherneH.Themanagementofopenfractures.In:Tscherne H,GorzenL,editors.Fractureswithsofttissueinjuries.New York:SpringerVerlag;1984.p.10–32.
36.HiernerR,Nast-KolbD,StoelAM,LendemansS,TägerG, WaydhasC,etal.Deglovinginjuriesofthelowerlimb. Unfallchirurg.2009;112(1):55–62.
37.GardnerMJ,MehtaS,BareiDP,NorkSE.Treatmentprotocol foropenAO/OTAtypeC3pilonsfractureswithsegmental boneloss.Reportof38casestreatedwithastandardprotocol. JBoneJointSurgAm.1984;66(9):1349–56.
38.RobsonMC,DukeWF,KrizekTJ.Rapidbacterialscreeningin thetreatmentofcivilianwounds.JSurgRes.
1973;14(5):426–30.
39.SchenkerML,YannascoliS,BaldwinKD,AhnJ,MehtaS.Does timingtooperativedebridementaffectinfectious
complicationsinopenlong-bonefractures?Asystematic review.JBoneJointSurgAm.2012;94(12):1057–64. 40.HildebrandF,GiannoudisP,KretteckC,PapeHC.Damage
control:extremities.Injury.2004;35(7):678–89.
41.DunbarRP,GardnerMJ.Initialmanagementofopenfractures. In:BucholzRW,HeckmanJD,Court-BrownCM,TornettaP, editors.RockwoodandGreen’sfracturesinadults.7thed. Philadelphia:Lippincott:Williams&Wilkins;2010. p.295.
42.HerscoviciDJr,SandersRW,ScadutoJM,InfanteA,
DiPasqualeT.Vacuum-assistedwoundclosure(VACTherapy) forthemanagementofpatientswithhigh-energysofttissue injuries.JOrthopTrauma.2003;17(10):683–8.
43.GopalS,MajumderS,BatchelorAG,KnightSL,DeBoerP, SmithRM.Fixandflap:theradicalorthopaedicandplastic treatmentofsevereopenfracturesofthetibia.JBoneJoint SurgBr.2000;82(7):959–66.
44.MoghadamianES,BosseMJ,MacKenzieEJ.Principlesof mangledextremitymanagement.In:BucholzRW,Heckman JD,Court-BrownCM,TornettaP,editors.Rockwoodand Green’sfracturesinadults.7thed.Philadelphia;Lippincott: Williams&Wilkins;2010.p.333.
45.LangeRH,BachAW,HansenST,JohansenKH.Opentibial fractureswithassociatedvascularinjuries:prognosisforlimb salvage.JTrauma.1985;25(3):203–8.
46.HelfetDL,HoweyT,SandersR,JohansenK.Limbsalvage versusamputation.PreliminaryresultsoftheMangled ExtremitySeverityScore.ClinOrthopRelatRes. 1990;(256):80–6.
47.KumarMK,BadoleC,PatondK.Salvageversusamputation: utilityofmangledextremityseverityscoreinseverelyinjured lowerlimbs.IndianJOrthop.2007;41(3):183–7.
48.KurienT,PearsonRG,ScammellBE.Bonegraftsubstitutes currentlyavailableinorthopaedicpractice:theevidencefor theiruse.BoneJointJ.2013;95-B(5):583–97.
49.RongaM,FagettiA,CantonG,PaiuscoE,SuraceMF, CherubinoP.Clinicalapplicationsofgrowthfactorsinbone injuries:experiencewithBMPs.Injury.2013;44(Suppl1):S34–9. 50.BlokhuisTJ,LindnerT.Allograftandbonemorphogenetic
proteins:anoverview.Injury.2008;39(Suppl2):S33–6. 51.HarveyZT,PotterBK,VanderseaJ,WolfE.Prosthetic