w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Review
article
Nailfold
capillaroscopy:
relevance
to
the
practice
of
rheumatology
Eduardo
José
do
Rosário
e
Souza
a,b,
Cristiane
Kayser
a,∗aDisciplineofRheumatology,UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazil bSantaCasadeBeloHorizonte,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27April2014 Accepted14September2014 Availableonline2December2014
Keywords:
Capillaroscopy
Raynaud’sphenomenon Systemicsclerosis
a
b
s
t
r
a
c
t
Nailfoldcapillaroscopyisasimple,low-costmethod,thatisextremelyimportantinthe evaluationofpatientswithRaynaud’sphenomenonandofpatientswithsystemicsclerosis (SSc)spectrumdiseases.BesidesitsimportancefortheearlydiagnosisofSSc,nailfold capil-laroscopyisausefultooltoidentifysclerodermapatientswithhighriskfordevelopmentof vascularandvisceralcomplicationsanddeath.Theinclusionofcapillaroscopyinthenew classificationcriteriaforSScoftheAmericanCollegeofRheumatology(ACR)andEuropean LeagueAgainstRheumatism(Eular)givesanewimpetustotheuseanddisseminationof themethod.Inthispaper,wepresentadidactic,non-systematicreviewonthesubject,with emphasisonadvancesrecentlydescribed.
©2014ElsevierEditoraLtda.Allrightsreserved.
Capilaroscopia
periungueal:
relevância
para
a
prática
reumatológica
Palavras-chave:
Capilaroscopia FenômenoRaynaud Esclerosesistêmica
r
e
s
u
m
o
Acapilaroscopiaperiunguealéummétodosimples,debaixocusto,edeextremarelevância naavaliac¸ãodepacientescomfenômenodeRaynaudouportadoresdedoenc¸asdoespectro daesclerosesistêmica(ES).AlémdesuaimportânciaparaodiagnósticoprecocedaES, con-stituiinstrumentoútilnaidentificac¸ãodepacientesesclerodérmicoscomriscoelevadopara odesenvolvimentodecomplicac¸õesvasculares,visceraisedeóbito.Ainclusãoda capilaro-scopianosnovoscritériosparaclassificac¸ãodaESdoColégioAmericanodeReumatologia (ACR)edaLigaEuropeiaContraoReumatismo(Eular)dánovoimpulsoparaautilizac¸ãoe disseminac¸ãodométodo.Nopresenteartigo,pretendemosapresentarumarevisãodidática, nãosistemática,sobreotema,comênfasenosavanc¸osrecentementedescritos.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
∗ Correspondingauthor.
E-mail:[email protected](C.Kayser).
http://dx.doi.org/10.1016/j.rbre.2014.09.005
Introduction
and
brief
history
Vascularchangescharacterizedbyfunctionalandstructural abnormalitiesofthe microcirculationplayacentral role in thepathogenesisofsystemicsclerosis(SSc)andmayalsobe present indermatomyositis (DM) and inthe SSc spectrum diseases.1 Nailfold capillaroscopy (NFC) is a non-invasive, inexpensiveandreproducibleimagingmethodallowingthe evaluationofstructuralchangesintheperipheral microcircu-lation.Itismainlyusedinthedifferentiationofprimaryand secondaryRaynaud’sphenomenon(RP)andinthediagnosis ofSSc.2,3
Thehistoryofcapillaroscopystarted400yearsago,whenJC Kolhausdescribedthepossibilityofvisualizationofcapillary loopsofthenailfoldregionthrougharudimentarysystemof opticalmagnification.3However,onlyinthesecondhalfofthe 20thCenturyNFCbeginstobeusedmoresystematicallyinthe evaluationofRP,inparticular,thankstothestudiesof Hilde-gardMaricqandEdwardCarwileLeRoy,whodescribedin1973 specificcapillaroscopicpatternsofSScandrelateddiseases.4 In Brazil,the method was introduced and standardized in the 80sby LuísEduardo Coelho Andrade.5 Inrecent years, researchershaveturnedtheirattentiontotheNFCbecause ofnewevidenceoftheimportanceofthemethodforearly diagnosisofSScanditsprognosticvalue.Inaddition,NFChas recentlybeenincorporatedintothenewclassification crite-riaoftheACR/EULAR2013forSSc,confirmingtheimportance ofthemethodinthediagnosisofthedisease.6Inthispaper, wepresentadidactic,non-systematicreviewonthesubject, highlightingtheindicationsofNFCandclinicalimplications ofitsmainfindingsinthedailypracticeoftherheumatologist.
Indications
of
capillaroscopy
in
rheumatology
Patientswith RPrepresentacommon diagnostic challenge in the practice of Rheumatology, with a broad differential diagnosis. Moreover, they constitute the main indication forNFC.RPisanexaggeratedphysiologicalresponseofthe microcirculationoftheextremities,facetoprecipitating fac-torssuchasexposuretocoldoremotionalstress.Itsclassic presentationincludesthreephases:(1)thefirstisrepresented by ischemia, when the fingers assume a white color; (2) then, with the occurrence ofblood stasis, the extremities turn toabluecolor (cyanosis);(3) andfinallythe redcolor appears,indicatingthestageofreperfusion.RPmaybe pri-mary,orsecondarytoanumberofconditionsanddiseases. PrimaryRPisabenignconditioncharacterizedbyfunctional changes of blood vessels and/or their innervation, and by definitiondoesnotprogresstoanirreversibletissuedamage. DiagnosticcriteriaforprimaryRPwereproposedin1992by LeRoyet al., and includedthe presenceofa normalNFC.7 Morerecently,newcriteriawereproposed,including:(1)the presenceofaclinicaldiagnosisofbiphasicRP;(2)anormal NFC;(3)aphysicalexaminationwithnofindingssuggestive ofasecondarycauseforRP(ulceration,gangrene,necrosis, sclerodactyly,calcinosisorskinthickening);(4)nohistoryof autoimmunerheumaticdisease;and(5)negativeorlow-titer ANA.8
Attheotherextreme,inpatientswithRPsecondarytoSSc spectrum diseases,RPattacks tend tobemore severe and maybeassociatedwithcomplicationssuchasulceration, scar-ring,gangreneand/ordigitalamputation.Variousrheumatic diseases may present with RP, including, in addition to SSc, systemic lupus erythematosus (SLE), dermatomyosi-tis/polymyositis (DM/PM), mixed connective tissue disease (MCTD), rheumatoid arthritis, Sjögren’s syndrome, vasculi-tidesandantiphospholipidsyndrome.However,RPassumes greaterimportanceinthesclerodermaspectrumofdiseases. Notably, RP is often the first manifestation of the disease in about 75% of patients with SSc, besides being associ-ated with significant morbidity and increased therapeutic difficulties.9–11
In this context,NFC plays a key role inthe distinction betweenprimaryandsecondaryRP,andcanalsoaidin clin-icaland evolutionary characterizationofthesesubjects, as well asreducing costswithan unnecessaryworkup.12–14 A meta-analysisshowedthat12.6%ofpatientsinitially identi-fiedassufferingfromprimaryRPdevelopasecondarycause for this phenomenon.10 Another recent study showed that approximately20%ofthesepatientsprogresstoadefinitive orsuspecteddiagnosisofsecondaryRPata10-year follow-up.9DifferentstudieshavebeenuniforminassigningtoNFC acrucialrole inmonitoring thetransitionfrom primaryto secondary RP.15–18 A meta-analysis bySpencer-Green et al. showedapositivepredictivevalueof47%forthepresenceof alterationsinNFC,avaluehigherthanthepredictivevalue forthepresenceofautoantibodies(30%).10Whenpresenceof specificautoantibodiesinSScwereassociatedwithabnormal capillaroscopyfindings,thepositivepredictivevalueforthe developmentofSSc reaches79.5% in15 years.18 Themain indicationsforNFCaresummarizedinTable1.
Technical
aspects
Equipment
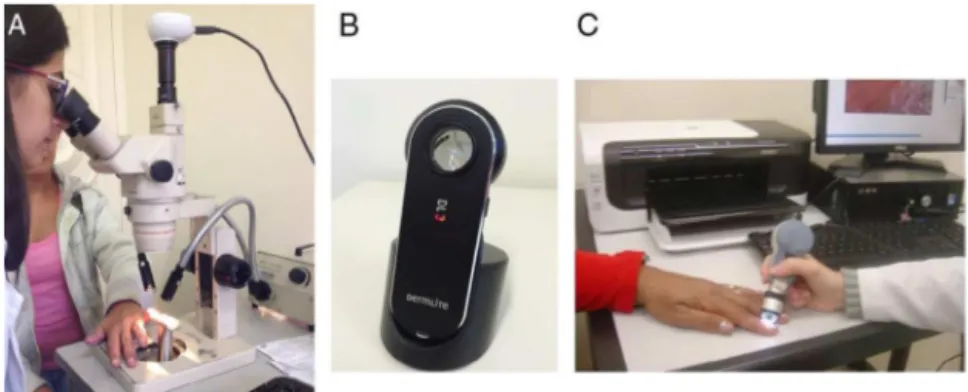
Didactically,wecanenumeratethreepossibilitiesforthe visu-alizationoftheterminalrowofcapillaryloops(Fig.1):
(1) Stereomicroscope: magnification capacity 10–50 times; allowsthe realizationof panoramicNFC. Withthe ste-reomicroscope, it is possible an overall assessment of nailfold beds, to register qualitative and quantitative parameters.5,19Thisremainsthemainmethodstillused
Table1–Mainindicationsforcapillaroscopy.
(a)EvaluationofpatientswithRaynaud’sphenomenon (b)MonitoringthetransitionfromprimarytosecondaryRP (c)EarlydiagnosisofSSc
(d)DifferentialdiagnosisofSSc-relatedconditions,suchas localizedSScandeosinophilicfasciitis,whichusuallyhavea normalcapillaroscopicpattern
(e)Detectionofseveremicroangiopathyandprognosticevaluation inSSc
Fig.1–Devicesthatcanbeusedfornailfoldcapillaroscopy:stereomicroscope(A);dermatoscope(B);videocapillaroscope(C).
todayinnationalandinternationalcenters,duetoitsease ofuseandlowcost.
(2) Ophthalmoscopeanddermatoscope:provideimageswith lower magnification and quality. These techniques can beanalternative tothe bedsideexams,orasaformof screeninginmedicalofficesthatdonothavea stereomi-croscopeoravideocapillaroscope20,21;and
(3) Videocapillaroscopy: consists of the combination of a microscope with a larger magnification lens coupled witha digital videocamera. Thistechnique provides a significantlyhigherincrease(200–600-fold) comparedto thestereomicroscope;and,withtheaidofspecific soft-wares,allowsaprecisemeasurementofcapillaroscopic parameters(capillarylength,widthanddensity).13,22One of the disadvantages of the technique is the loss of panoramic view of the capillary loops; only one area of the nailfold region may be examined at any given time.
Recently,astudy fromourgroup,comparing videocapil-laroscopeversusstereomicroscope,showedsimilardiagnostic performanceandreproducibilityofthetwomethods.22
Howtoperformtheexamination
Whichevermethodisused,initiallythepatientmustremain inanacclimatizedroomfor15–20minwithitstemperature around20–22◦C.Forbettervisualizationofthecapillaries,a
dropofimmersionoilisplacedonthecuticleofthefingersto beevaluated.Theperiungualregionofthetenoreightfingers (excludingthethumb)shouldbeexamined.Inthisregion,the distalrowofcapillaryloopsprotrudesintothedermalpapillae,
allowingalongitudinalviewofitsthree(afferent,efferentand transition) segments,arrangedinadirectionparalleltothe skinsurface.23
Thefollowingparameters areroutinely evaluated: num-berofloops/mm,numberofdilatedcapillaries(withectasia and/or megacapillaries), devascularization, the presenceof micro-hemorrhages,and meandering,tortuousorbranched capillaries.Thepresenceofdevascularizationcanbeassessed by the number of loops/mm or by a devascularization score, graded 0–3, where 0 corresponds to the absence of devascularization, and 3toextensive areas ofavascularity. Capillaroscopic parameters may also be graded using the methodproposedbyCutoloetal.,inwhichthecapillary abnor-malities are gradedaccording totheirintensity, asfollows: score0–nochanges;score1–<33%ofcapillarychanges;score 2–33–66%ofcapillarychanges;score3–>66%ofcapillary changes.24Byconvention,anabnormalcapillaroscopic find-ing isconsideredsignificantifitisobservedinatleasttwo fingersoftheindividual.12,13,25
Capillaroscopic
patterns
Normalcapillaroscopicpattern
Inhealthyindividuals,thecapillarieshavehomogeneoussize, shape and color, and are arranged transversely across the cuticle(Fig.2A).Thecapillaryloopsmaypresentdiscreet mor-phologicalvariations, suchascrossed ormeandering loops (with intertwining). The subpapilar venous plexus can be seeninvaryingextentinapproximately60%ofthe popula-tion,withgreatervisibilityexpectedinchildrenandinwhite
people.5,19Thenormalcapillarydensity,obtainedbycounting thenumberofloops inonemillimeter,rangesfrom7to12 capillaries,averaging9capillaries/mm;mostresearchers con-siderasaparameterofnormalityinadultsthe presenceof
≥9loops/mm.22,25Asmallnumberofcapillarydilations
(ecta-sia)mayalsobeobserved,butthefindingofmegacapillaries orareasofdevascularizationshouldbeconsideredabnormal, except in the latter case, if the devascularization is asso-ciatedwithtraumatic microscarsin the periungualregion. Similarly,smallareasofmicro-bleedingwithfocal distribu-tioncanbeobservedinhealthyindividuals,associatedwith everydaymicrotrauma.Duringtheexam,itisusefulto con-siderthatthereisgreatvariationintheshapeandsizeofthe capillaryloopsamonghealthyindividuals,andevenamong fingersofthesameperson.Therefore,inthesecasesa mis-diagnosisofmicroangiopathyshould beavoided.Thus,the traininganddevelopmentareessentialfactorsinthe forma-tionofcapillaroscopists.26
SD(scleroderma)pattern
Firstdescribed byMaricqetal.,theSDpatterncorresponds toasetoftypicalNFCchangescharacterizedbythepresence ofdilatedcapillaries(ectasiaand/ormegacapillaries),lossof capillary loops, with consequent reductionin the number ofcapillaries,micro-bleedingandneoangiogenesis(branched capillaries)(Fig.2B).4,27TheSDpatternispresentin83–98%of casesofSSc,althoughitisalsoobservedinMCTD,DMandin overlapsyndromes.13,28
Additionally,Cutoloetal.classifiedcapillaroscopychanges associatedwithSDpatterninthreestages:recent,activeand late.24Inthe“recent”pattern,micro-hemorrhages,and ecta-sia(includingmegacapillaries)predominate,witharelatively preservedcapillarydistributionandwithnosignificant devas-cularization.Thesefindingsarecrucialforearlydiagnosisof SSc.In the “active” pattern,an increase inthe number of giantcapillaries(megacapillaries)andmicro-hemorrhagesare observed,inassociationwithamoderatelossofcapillaries andmilddistortionofcapillaryarchitecture.The“late”pattern ischaracterizedbyaseverelossofcapillariesandby exten-siveavascularareas,neoangiogenesisanddisorganizationof capillaryarchitecture.Inthisstudy,thelatepatternchanges correlatedwiththedurationofRPanddiagnosisofSSc.
Nonspecificmicroangiopathy
Nonspecificchangescharacterizedbythepresenceof elon-gated or tortuous capillaries, discreet presence of dilated capillariesandincreasedvisibility ofthesubpapilarvenous plexusaredescribedinanumberofconditions.Theirreal sig-nificancemustbeinterpretedwithintheclinical contextof eachpatient.
Capillaroscopy
in
autoimmune
rheumatic
diseases
Systemicsclerosis
As previously mentioned, approximately 90% of patients withSSc exhibittheSDpattern inNFC.Amicroangiopathy
typical of SSc is found in the early stages of the disease, often only when RP is present. The correlation between capillaroscopic findings and the duration of the disease is controversial. Some authors describe a more pronounced presence of dilated capillaries and micro-hemorrhages in the earlyyearsofdisease,andamoreintense disorganiza-tionanddevascularizationinlaterstages.However,itisnot uncommontofindpatientswithmanyyearsofillnessand littledevascularization;ontheotherhand,patientswith lit-tlediseasedurationandintensedegreeofdevascularization anddisorganizationofthecapillaryarchitecturecanalsobe seen.2
SSc is a chronic disease associated with high morbid-ity and mortality. In this sense, it has been increasingly emphasized theneedforanearlydiagnosisofthedisease, when there is as yet no evidence of fibrosis of internal organsandofirreversibledamage.6,13,28Inthisscenario,NFC acquiresitsgreatpracticalimportance.Itisnoteworthythat the ACR (1980) classificationcriteria forSSc, based mainly onclinicalmanifestationsofawell-establisheddisease,did not allow its early recognition. In this context, LeRoy and Medsger proposed in 2001 criteria for the early diagnosis ofSSc, which includeacombination of clinical (Raynaud’s phenomenon),imaging(nailfoldcapillaroscopywithSD pat-tern)andlaboratory(presenceofSSc-specificautoantibodies) data.29
Recently,theResearchGrouponSclerodermafromEULAR suggestedpreliminarycriteriafortheveryearlydiagnosisof SScusingthesamethreedomains,withtheadditionofthe presenceofswollenfingersandapositiveresultfor antinu-clearfactor.30
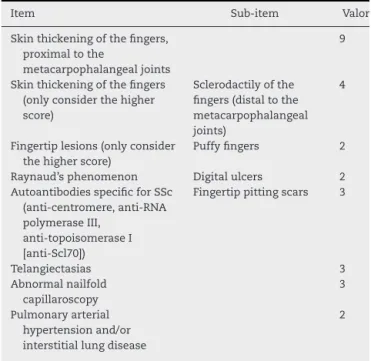
CorroboratingtheimportanceofNFC inthediagnosisof SSc,ACRandEULARproposedin2013newcriteriaforthe clas-sificationofSSc.6Accordingtothesenewcriteria,thepatient isclassifiedashavingSScifhe/shegetatotalofnineormore pointsamongthoseeightitemslistedinTable2,witha sensi-tivityof91%andspecificityof92%inacohortstudy,compared toasensitivityof75%andspecificityof72%withthe applica-tionofthe1980ACRcriteria.
Systemiclupuserythematous
CapillaroscopychangesinSLEarelessspecificthan inSSc, beingcharacterizedbythepresenceoftortuousand mean-deringcapillaries,bizarreloopsandaprominentsubpapilar plexus,leadingsomeauthorstopostulatethepresenceofa typicalcapillaroscopicpattern.31Thepresenceofalterations inNFCismorefrequentinpatientswithSLEpresentingRP.32 However,50%ofpatientswithSLEhavenormalNFC.SD pat-ternisalesscommonfindingandhasbeendescribedin2–9% ofpatients.33,34Inthesepatients,thereseemstobea correla-tionbetweenthepresenceofSDpattern,fingertipsvasculitis andanti-U1-RNPantibodies.34,35
Table2–ClassificationcriteriaforSScproposedbyACR andEULAR(2013).6
Item Sub-item Valor
Skinthickeningofthefingers, proximaltothe
metacarpophalangealjoints
9
Skinthickeningofthefingers (onlyconsiderthehigher score)
Sclerodactilyofthe fingers(distaltothe metacarpophalangeal joints)
4
Fingertiplesions(onlyconsider thehigherscore)
Puffyfingers 2
Raynaud’sphenomenon Digitalulcers 2
AutoantibodiesspecificforSSc (anti-centromere,anti-RNA polymeraseIII,
anti-topoisomeraseI [anti-Scl70])
Fingertippittingscars 3
Telangiectasias 3
Abnormalnailfold capillaroscopy
3
Pulmonaryarterial hypertensionand/or interstitiallungdisease
2
hypertension,suggestingamajorroleofNFCinidentifying thissubtypeofpatients.36
Dermatomyositisandpolimyositis
TheprevalenceofDM/PMinRPrangesfrom10to60%,butthe presenceofcomplicationssuchasdigitalnecrosisisrare.37 TheSDpatternisobservedinabout20–60%ofpatientswith DM/PM,withmorefrequentandpronouncedfindingsinDM thaninPM;itcorrelateswiththepresenceofRPand inter-stitialpulmonaryinvolvement.38 Thepresenceofbranched capillariesismorecommoninDM,buttheirpresenceisnot specificandcanalsobefoundlessfrequentlyinpatientswith SSc.InstudieswithjuvenileDM,theSDpatternismost com-mon,havingapositiveassociationwithseverityandclinical andlaboratoryactivityofthedisease.39–41
Mixedconnectivetissuedisease
RPisoneoftheinitialmanifestationsofthedisease, occur-ringinapproximately85%ofpatientswithMCTDandisalso partofthemainclassificationcriteriaforthisdisease.42SD patternisobservedin50–65%ofcases.Acorrelationbetween capillaroscopyfindingsandpulmonaryinvolvementinMCTD isalsodescribed.43
Undifferentiatedconnectivetissuedisease(UCTD)
The term UCTD is used when, in the presenceof clinical manifestationssuggestiveofsystemicautoimmunedisease, ashortageofclinicaland/orlaboratorydatadoesnotallow thecharacterizationofaspecificclinicalentity.The follow-upofthisgroupofpatientspointstoaclinicaloutcomefor SSc,SLE,rheumatoidarthritisorSjögren’ssyndromein30% ofcases.Nagyetal.foundaprevalenceof13.8%forSD pat-tern in65 patients withUCTD and suggestedthat NFC be
performedinallcasesofUCTDwiththeaimofidentifying patientsathigherriskforprogressiontoSScortoitsspectrum diseases.33
PrimarySjögrensyndrome(SS)
In SS, thecapillaroscopic findingsdiffer, dependingon the presenceorabsenceofRP,presentin13–30%ofpatients.44,45 InprimarySSwithoutRP,NFC isnormalinmorethanhalf ofpatients;theotherpatientspresentnonspecific capillaro-scopicfindings,includingthepresenceoftortuous,irregular capillaries and ofamoreevidentsubpapilar plexus. When thereispresenceofRP,mostpatientsalsoshownonspecific capillaroscopic findings. The SD pattern was described in two of 16 patients (12.5%) with SS in one study.46 In the subgroupofpatientswithSSandwithpositivityfor anticen-tromere, the researchersfound aprevalenceof 80% ofthe SDpattern,indicatingapotentialforsubclinicaloverlapwith SSc.46
Rheumatoidarthritis(RA)
InpatientswithRAthereisnodescriptionofaSDpattern.2 Somestudiesshowthepresenceofchangesofuncertain rel-evanceinaproportionofpatients,suchasthepresenceof elongatedcapillaries.2
Antiphospholipidsyndrome(APS)
Presence of microbleeding distributed symmetrically is described in APS patients and in SLE patients with pres-ence of IgG and IgM anticardiolipin antibodies, suggesting adirectdamageofvascularendotheliumtriggeredbythese antibodies.47,48
Capillaroscopyasamarkerofseverityofsystemicsclerosis
Despite some controversial results, capillaroscopy also assumesanimportantroleinevaluatingtheseverityofthe disease,visceralinvolvement,andprognosisofpatientswith SSc.In1976,Maricqetal.previouslyhadfoundacorrelation betweenmorphologicalchangesofNFCand thenumberof organsinvolvedbythedisease.49Overtheyears,most stud-ies foundacorrelation withthe degreeofmicroangiopathy evaluatedbyNFCandperipheralvascular,cutaneousand pul-monaryinvolvement.2,16,50 Recently,astudyoftwocohorts ofBelgianandItalianpatientsfoundanassociationbetween the severity of capillaroscopy patterns and risk of severe clinical involvement. Nine systems and/or organs (periph-eralvascular,general,skin,joints,muscles, gastrointestinal tract,lung, heartand kidneys)were evaluatedaccordingto Medsger severity scale. There was an association between riskofseriousvisceralinjuryandearly,activeandlate pat-terns,andtheriskwashigherinpatientspresentingthelate pattern.51
index(CSURI)topredicttheemergenceofnewulcersinSSc patients.53Takentogether,theseresultssuggesttheNFC rou-tine use in patients with SSc, aiming the identification of patientswithincreasedriskfordevelopmentofthis compli-cation.
Regarding pulmonaryinvolvement,a study founda sig-nificantlylowercapillarydensityinpatientswithpulmonary arterial hypertension associated with SSc, compared with patientswithoutpulmonaryhypertension.54Inanotherstudy, Bredemeieretal.foundacorrelationbetweenhigherscoresfor avascularareasandground-glassopacitiesin91patientswith SSc.55
Finally, a study from our group demonstrated an asso-ciation between risk of death and higher scores for devascularization(>1.5)inNFCinagroupof125patientswith SSc.56
Conclusions
Capillaroscopy isan extremely useful and reliable method forthedifferentialdiagnosisbetweenprimaryandsecondary RP.Additionally, theuseofNFCmayaggregate information about the disease severity and degree ofvisceralization in patients with SSc. Currently, two methods are most used forperformingNFC:panoramicnailfoldcapillaroscopy,using a stereomicroscope, and videocapillaroscopy, which uses largermagnifications anda computerizedsystem ofimage acquisition.3Bothhaveadvantagesanddisadvantages; how-ever, they are equivalent for the identification of classical abnormalities,allowingtherecognitionofthreepatterns: nor-malpattern,nonspecificmicroangyopathyandSDpattern.23 The inclusion of capillaroscopic abnormalities in the new classificationcriteriaoftheACR/EULARforSSc givesanew impetustotheuseanddisseminationofcapillaroscopy.The education andtraining ofrheumatologistsqualified to per-formthecapillaroscopywasanissueneglectedforyears,with prevalenceofself-teaching.EULARpromotesregularcourses incapillaroscopy.InBrazil,thefirstcourseofcapillaroscopyin autoimmunerheumaticdiseaseswasconductedin2011bythe DisciplineofRheumatologyofUniversidadeFederaldeSãoPaulo. Dissemination,trainingandimprovementofthemethodmust remaininthespecialtyagenda.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. HerrickAL.PathogenesisofRaynaud’sphenomenon. Rheumatology(Oxford).2005;44:587–96.
2. GrassiW,DeAngelisR.Capillaroscopy:questionsand answers.ClinRheumatol.2007;26:2009–16.
3. KayserC,AndradeLEC.Capilaroscopiaperiungueal: importânciaparaainvestigac¸ãodofenômenodeRaynaude
doenc¸asdoespectrodaesclerosesistêmica.RevBras Reumatol.2004;44:46–52.
4.MaricqHR,LeRoyEC.Patternsoffingercapillary abnormalitiesinconnectivetissuediseaseby‘widefield’ microscopy.ArthritisRheum.1973;16:619–28.
5.AndradeLE,GabrielJúniorA,AssadRL,FerrariAJ,AtraE. Panoramicnailfoldcapillaroscopy:anewreadingmethod andnormalrange.SeminArthritisRheum.1990;20: 21–31.
6.VandenHoogenF,KhannaD,FransenJ,JohnsonSR,BaronM, TyndallA,etal.2013classificationcriteriaforsystemic sclerosis:anAmericancollegeofrheumatology/European leagueagainstrheumatismcollaborativeinitiative.Ann RheumDis.2013;72:1747–55.
7.LeRoyEC,MedsgerTAJr.Raynaud’sphenomenon:a proposalforclassification.ClinExpRheumatol.1992;10: 485–8.
8.MaverakisE,PatelF,KronenbergDG,ChungL,FiorentinoD, AllanoreY,etal.Internationalconsensuscriteriaforthe diagnosisofRaynaud’sphenomenon.JAutoimmun. 2014:48–9,60–5.
9.HirschlM,HirschlK,LenzM,KatzenschlagerR,HutterHP, KundiM.TransitionfromprimaryRaynaud’sphenomenon tosecondaryRaynaud’sphenomenonidentifiedby diagnosisofanassociateddisease:resultsoftenyearsof prospectivesurveillance.ArthritisRheum.2006;54: 1974–81.
10.Spencer-GreenG.OutcomesinprimaryRaynaud’s phenomenon:ameta-analysisofthefrequency,rates,and predictorsoftransitiontosecondarydiseases.ArchIntern Med.1998;158:595–600.
11.HerrickAL.Thepathogenesis,diagnosisandtreatmentof Raynaud’sphenomenon.NatRevRheumatol.2012;8: 469–79.
12.CutoloM,SulliA,SecchiME,OlivieriM,PizzorniC.The contributionofcapillaroscopytothedifferentialdiagnosisof connectiveautoimmunediseases.BestPractResClin Rheumatol.2007;21:1093–108.
13.CutoloM,GrassiW,MatucciCerinicM.Raynaud’s
phenomenonandtheroleofcapillaroscopy.ArthritisRheum. 2003;48:3023–30.
14.IngegnoliF,BoracchiP,GualtierottiR,LubattiC,MeaniL, ZahalkovaL,etal.Prognosticmodelbasedonnailfold capillaroscopyforidentifyingRaynaud’sphenomenon patientsathighriskforthedevelopmentofascleroderma spectrumdisorder:Prince(PrognosticIndexforNailfold CapillaroscopicExamination).ArthritisRheum. 2008;58:2174–82.
15.CutoloM,SmithV.Stateoftheartonnailfoldcapillaroscopy: areliablediagnostictoolandputativebiomarkerin
rheumatology?Rheumatology(Oxford).2013;52: 1933–40.
16.HerrickAL,CutoloM.Clinicalimplicationsfrom capillaroscopicanalysisinpatientswithRaynaud’s phenomenonandsystemicsclerosis.ArthritisRheum. 2010;62:2595–604.
17.RossiD,RussoA,MannaE,BinelloG,BaldovinoS,SciasciaS, etal.Theroleofnail-videocapillaroscopyinearlydiagnosisof scleroderma.AutoimmunRev.2013;12:821–5.
18.KoenigM,JoyalF,FritzlerMJ,RoussinA,AbrahamowiczM, BoireG,etal.Autoantibodiesandmicrovasculardamageare independentpredictivefactorsfortheprogressionof Raynaud’sphenomenontosystemicsclerosis:atwenty-year prospectivestudyof586patients,withvalidationofproposed criteriaforearlysystemicsclerosis.ArthritisRheum. 2008;58:3902–12.
aplicac¸ãoemindivíduoshígidoseportadoresde enfermidadesreumáticas.RevBrasReumatol.1990;30: 71–81.
20.AndersHJ,SiglT,SchattenkirchnerM.Differentiation betweenprimaryandsecondaryRaynaud’sphenomenon:a prospectivestudycomparingnailfoldcapillaroscopyusingan ophthalmoscopeorstereomicroscope.AnnRheumDis. 2001;60:407–9.
21.BergmanR,SharonyL,SchapiraD,NahirMA,Balbir-Gurman A.Thehandhelddermatoscopeasanail-foldcapillaroscopic instrument.ArchDermatol.2003;139:1027–30.
22.SekiyamaJY,CamargoCZ,AndradeLE,KayserC.Reliabilityof widefieldnailfoldcapillaroscopyandvideocapillaroscopyin theassessmentofpatientswithRaynaud’sphenomenon. ArthritisCareRes.2013;65:1853–61.
23.SangiorgiS,ManelliA,CongiuT,BiniA,PilatoG,ReguzzoniM, etal.Microvascularizationofthehumandigitasstudiedby corrosioncasting.JAnat.2004;204:123–31.
24.CutoloM,SulliA,PizzorniC,AccardoS.Nailfold
videocapillaroscopyassessmentofmicrovasculardamagein systemicsclerosis.JRheumatol.2000;27:155–60.
25.SulliA,SecchiME,PizzorniC,CutoloM.Scoringthenailfold microvascularchangesduringthecapillaroscopicanalysisin systemicsclerosispatients.AnnRheumDis.2008;67: 885–7.
26.KayserC,CorreaMJU,AndradeLEC.FenômenodeRaynaud. RevBrasReumatol.2009;49:48–63.
27.MaricqHR,LeRoyEC,D’AngeloWA,MedsgerTAJr,Rodnan GP,SharpGC,etal.Diagnosticpotentialofinvivocapillary microscopyinsclerodermaandrelateddisorders.Arthritis Rheum.1980;23:183–9.
28.CutoloM,SulliA,SmithV.Assessingmicrovascularchanges insystemicsclerosisdiagnosisandmanagement.NatRev Rheumatol.2010;6:578–87.
29.LeRoyEC,MedsgerTAJr.Criteriafortheclassification ofearlysystemicsclerosis.JRheumatol.2001;28: 573–6.
30.AvouacJ,FransenJ,WalkerUA,RiccieriV,SmithV,MullerC, etal.Preliminarycriteriafortheveryearlydiagnosisof systemicsclerosis:resultsofaDelphiConsensusStudyfrom EularSclerodermaTrialsandResearchGroup.AnnRheum Dis.2011;70:476–81.
31.KabasakalY,ElvinsDM,RingEF,McHughNJ.Quantitative nailfoldcapillaroscopyfindingsinapopulationwith connectivetissuediseaseandinnormalhealthycontrols. AnnRheumDis.1996;55:507–12.
32.Pavlov-DolijanovicS,DamjanovNS,VujasinovicStuparNZ, MarceticDR,Sefik-BukilicaMN,PetrovicRR.Istherea differenceinsystemiclupuserythematosuswithand withoutRaynaud’sphenomenon?RheumatolInt. 2013;33:859–65.
33.NagyZ,CzirjácL.Nailfolddigitalcapillaroscopyin447 patientswithconnectivetissuediseaseandRaynaud’s disease.JEurAcadDermatolVenereol.2004;18: 62–8.
34.FurtadoRNV,PucinelliML,CristoVV,AndradeLE,SatoEI. Scleroderma-likenailfoldcapillaroscopicabnormalitiesare associatedwithanti-U1-RNPantibodiesandRaynaud’s phenomenoninSLEpatients.Lupus.2002;11:
35–41.
35.LambovaSN,Müller-LadnerU.Theroleofcapillaroscopyin differentiationofprimaryandsecondaryRaynaud’s
phenomenoninrheumaticdiseases:areviewoftheliterature andtwocasereports.RheumatolInt.2009;29:
1263–71.
36.KhannaD,GladueH,ChannickR,ChungL,DistlerO, FurstDE,etal.Recommendationsforscreeningand detectionofconnectivetissuedisease-associated
pulmonaryarterialhypertension.ArthritisRheum. 2013;65:3194–201.
37.ParodiA,CaproniM,MarzanoAV,DeSimoneC,LaPlacaM, QuaglinoP,etal.Dermatomyositisin132patientswith differentclinicalsubtypes:cutaneoussignsconstitutional symptomsandcirculatingantibodies.ActaDermVenereol. 2002;82:48–51.
38.GanczarczykML,LeeArmstrongSK.Nailfoldcapillary microscopyinpolymyositisanddermatomyositis.Arthritis Rheum.1988;31:116–9.
39.NascifAK,TerreriMT,LenCA,AndradeLE,HilárioMO. Inflammatorymyopathiesinchildhood:correlationbetween nailfoldcapillaroscopyfindingsandclinicalandlaboratory data.JPediatr.2006;82:40–5.
40.Spencer-GreenG,CroweWE,LevinsonJE.Nailfoldcapillary abnormalitiesandclinicaloutcomeinchildhood
dermatomyositis.ArthritisRheum.1982;25: 954–8.
41.SilverRM,MaricqHR.Childhooddermatomyositis:serial microvascularstudies.Pediatrics.1989;83:
278–83.
42.SmolenJS,SteinerG.Mixedconnectivetissuedisease:tobe ornottobe?ArthritisRheum.1998;41:
768–77.
43.deHolandaMalfadoDiógenesA,BonfáE,FullerR,Correia CaleiroMT.Capillaroscopyisadynamicprocessinmixed connectivetissuedisease.Lupus.2007;16:
254–8.
44.García-CarrascoM,SisóA,Ramos-CasalsM,RosasJ,DelaRed G,GilV,etal.Raynaud’sphenomenoninprimarySjögren’s syndrome.Prevalenceandclinicalcharacteristicsinaseries of320patients.JRheumatol.2002;29:
726–30.
45.SkopouliFN1,TalalA,GalanopoulouV,TsampoulasCG, DrososAA,MoutsopoulosHM.Raynaud’sphenomenonin primarySjögren’ssyndrome.JRheumatol.1990;17: 618–20.
46.TektonidouM1,KaskaniE,SkopouliFN,MoutsopoulosHM. MicrovascularabnormalitiesinSjögren’ssyndrome:nailfold capillaroscopy.Rheumatology(Oxford).1999;38:
826–30.
47.BongardO,BounameauxH,MiescherPA,DeMoerlooseP. Associationofanticardiolipinantibodiesandabnormal nailfoldcapillaroscopyinpatientswithsystemiclupus erythematosus.Lupus.1995;4:142–4.
48.SulliA,PizzorniC,CutoloM.Nailfoldvideocapillaroscopy abnormalitiesinpatientswithantiphospholipidantibodies.J Rheumatol.2000;27:1574–6.
49.MaricqHR,Spencer-GreenG,LeRoyEC.Skincapillary abnormalitiesasindicatorsoforganinvolvementin scleroderma(systemicsclerosis)Raynaud’ssyndromeand dermatomyositis.AmJMed.1976;61:
862–70.
50.SatoLT,KayserC,AndradeLE.Nailfoldcapillaroscopy abnormalitiescorrelatewithcutaneousandvisceral involvementinsystemicsclerosispatients.ActaReumatol Port.2009;34:219–27.
51.SmithV,RiccieriV,PizzorniC,DecumanS,DeschepperE, BonroyC,etal.Nailfoldcapillaroscopyforpredictionofnovel futuresevereorganinvolvementinsystemicsclerosis.J Rheumatol.2013;40:2023–8.
52.SmithV,DeKeyserF,PizzorniC,VanPraetJT,DecumanS, SulliA,etal.Nailfoldcapillaroscopyforday-to-dayclinical use:constructionofasimplescoringmodalityasaclinical prognosticindexfordigitaltrophiclesions.AnnRheumDis. 2011;70:180–3.
prognostictoolfordigitalskinulcerdevelopmentinsystemic sclerosispatients.ArthritisRheum.2009;61:
688–94.
54.HofsteeHM,VonkNoordegraafA,VoskuylAE,DijkmansBA, PostmusPE,SmuldersYM,etal.Nailfoldcapillarydensityis associatedwiththepresenceandseverityofpulmonary arterialhypertensioninsystemicsclerosis.AnnRheumDis. 2009;68:191–5.
55.BredemeierM,XavierRM,CapobiancoKG,RestelliVG, RohdeLE,PinottiAF,etal.Nailfoldcapillarymicroscopy cansuggestpulmonarydiseaseactivityinsystemic sclerosis.JRheumatol.2004;31:286–94.