www.jped.com.br
ORIGINAL
ARTICLE
Correlation
between
hemoglobin
levels
of
mothers
and
children
on
exclusive
breastfeeding
in
the
first
six
months
of
life
夽
,
夽夽
Rosa
de
Fátima
da
Silva
Vieira
Marques
a,
José
Augusto
de
Aguiar
Carrazedo
Taddei
b,
Tulio
Konstantyner
b,∗,
Affonso
Celso
Vieira
Marques
c,
Josefina
Aparecida
Pellegrini
Braga
daUniversidadeFederaldeSãoPaulo,EscolaPaulistadeMedicina,SãoPaulo,SP,Brazil
bUniversidadeFederaldeSãoPaulo,DepartamentodePediatria,DisciplinadeNutrologia,SãoPaulo,SP,Brazil cHospitaldoServidorPúblicoMunicipaldeSãoPaulo,DisciplinadeObstetrícia,SãoPaulo,SP,Brazil
dUniversidadeFederaldeSãoPaulo,DepartamentodePediatria,DisciplinadeEspecialidadesPediátricas,SãoPaulo,SP,Brazil
Received26July2015;accepted13November2015 Availableonline4May2016
KEYWORDS
Hemoglobins; Breastfeeding; Anemia; Infant; Linearmodels
Abstract
Objective: Toevaluatethecorrelationbetweenhemoglobinlevelsofmothersandtheirchildren
onexclusivebreastfeedinginthefirstsixmonthsoflife.
Methods: Cross-sectionalstudywith221binomials(mother---child)enrolledinabreastfeeding
supportprogram,whowerestratifiedintosixgroupsaccordingtothechildren’sagegroup.The
sampleconsistedofchildrenbornattermwithnormalweight,withnoneonatalcomplications
andwhosemothersdidnothaveanemiaorinfectiousdiseaseatthetimeofdatacollection.
Interviewswere carried outwiththemothers,bloodwas collectedby peripheral
venipunc-turefrommothersandchildren,andchildren’santhropometricdatawereassessed.Pearson’s
correlationcoefficientsbetweenthehemoglobinlevelsofmothersandchildren were
calcu-lated.Sixmultiplelinearregressionmodelswereadjustedwithregressioncoefficientestimates,
consideringasstatisticallysignificantassociationswithp≤0.05.
Results: The correlation coefficients ofhemoglobin levelsof mothers and children ranged
from 0.253, at three months, to 0.601, at fivemonths. The hemoglobin level of mothers
夽 Pleasecitethisarticleas:MarquesRF, TaddeiJA,KonstantynerT,MarquesAC,BragaJA.Correlationbetweenhemoglobinlevelsof
mothersandchildrenonexclusivebreastfeedinginthefirstsixmonthsoflife.JPediatr(RioJ).2016;92:479---85.
夽夽StudyconductedattheDepartmentofPediatrics,EscolaPaulistadeMedicina(EPM),UniversidadeFederaldeSãoPaulo(UNIFESP),São
Paulo,SP,Brazil. ∗Correspondingauthor.
E-mail:[email protected](T.Konstantyner).
http://dx.doi.org/10.1016/j.jped.2015.11.006
wascorrelatedwiththehemoglobinleveloftheirchildrenatfourmonths(r=0.578)andatfive
months(r=0.601).Intheadjustedmultiplelinearregression,theregressioncoefficientswere
higheratfourmonths(ˇ=1.134;p=0.002)andatfivemonths(ˇ=0.845;p<0.001).
Conclusion: Thesefindings allow for theconclusionthatthereisacorrelationbetweenthe
hemoglobinofmothersandthehemoglobinoftheirchildrenonexclusivebreastfeedinginthe
firstsixmonthsoflife.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
PALAVRAS-CHAVE
Hemoglobinas; Aleitamento materno; Anemia; Lactente; ModelosLineares
Correlac¸ãoentreníveisdehemoglobinademãesefilhosemaleitamentomaterno exclusivonoprimeirosemestredevida
Resumo
Objetivo: Avaliaracorrelac¸ão entreosníveis dehemoglobina demães ede seusfilhos em
aleitamentomaternoexclusivo,noprimeirosemestredevida.
Métodos: Estudotransversalcom221binômios(mãe-filho)matriculadosemprogramade
incen-tivoaoaleitamentomaterno,queforamestratificadosemseisgruposdeacordocomafaixa
etáriadascrianc¸as.Aamostraconsistiudecrianc¸asnascidasatermo,compesonormal,sem
intercorrênciasneonataisecujasmãesnãoapresentavamdoenc¸ainfecciosaeanemianaépoca
dacoletadedados.Foramrealizadasentrevistascomasmães,coletadesangueporpunc¸ão
deveiaperiféricadasmãesedascrianc¸aseantropometriadascrianc¸as.Foramcalculadosos
coeficientesdecorrelac¸ãodePearsonentreosníveisdehemoglobinadasmãesedascrianc¸as.
Foramajustadosseismodelosderegressãolinearmúltiploscomestimativasdecoeficientesde
regressão,considerando-seestatisticamentesignificantesassociac¸õescomp≤0,05.
Resultados: Oscoeficientesdecorrelac¸ãodosníveisdehemoglobinadasmãesedascrianc¸as
variaramentre0,253,aostrêsmeses,e0,601,aoscincomeses.Oníveldehemoglobinadas
mãesestevemaiscorrelacionadocomodascrianc¸asaosquatromeses(r=0,578)eaoscinco
meses(r=0,601).Naregressão linearmúltiplaajustada,oscoeficientes deregressãoforam
maioresaosquatromeses(=1,134;p=0,002)eaoscincomeses(=0,845;p<0,001).
Conclusão: Essesachadospermitemconcluirquehácorrelac¸ãoentreahemoglobinademãese
ahemoglobinadeseusfilhosemaleitamentomaternoexclusivonoprimeirosemestredevida.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo
OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
In the first year of life, iron-deficiency anemia is associated with psychomotor and cognitive development problems,whichmaybeirreversibleevenafterappropriate treatment.1Therefore,knowledgeoftheriskfactors,which
maybealreadypresentinearlylife,isessentialtosupport
controlandpreventionstrategies. InBrazil,the best
esti-matesoftheprevalenceofanemiaininfantsandmothers
arerespectively 24.1% and 29.4%,highlighting the
impor-tanceofthesubject.2---4Specifically,healthcareresearchers
have been discussing the influence of the nutritional
sta-tusofmaternalirononthehemoglobin(Hb)levelsoftheir
childrenforseveraldecades.Astheconcentrationsofiron
andlactoferrininbreastmilkareneededtomaintainbody
ironlevelsinthefirstmonthsoflife,maternalanemiacould
affect these concentrations in breast milk. However, two
studiescarriedoutbythesamegroupofresearchersinIndia,
whichevaluatedtheconcentrationsofironandlactoferrinin
anemicandnonanemicmothers’milkwhobreastfed
exclu-sivelyforthe firstsixmonthsoflife, concludedthatboth
ironandlactoferrinconcentrationshadnoassociationwith
themothers’ironstatus.5,6
The results of studies that evaluated the association
betweenanemiaininfantsandmaternalanemiaremain
con-troversial. While some studies suggest no association,7---10
othersshowevidencethatchildrenborntoanemicor
iron-deficientmothers morefrequentlydevelopiron-deficiency
anemiainthefirstyearoflife,whencomparedtochildren
of non-anemicmothers.11---14 However,none ofthese
stud-iesinvestigatedthe influenceof serumlevelsofmaternal
hemoglobin (Hb) onthe children’s Hb profile in a sample
ofexclusivelybreastfedinfants,whichaffectsthevalidity
oftheir findings,asother sourcesofironinthechildren’s
diets canberesponsiblefordissimilar findings,generating
thecontroversyintheliterature.
Inthiscontext,thisstudyaimedtoevaluatethe
corre-lationbetweenHblevelsofmothersandtheirchildrenon
exclusivebreastfeedinginthefirstsixmonthsoflife.
Methods
unit in Belém (Brazil), from October 2006 to December 2008.
In this healthcare service, thereis a care program for mothersandchildrenthatincluderegularconsultationswith amultidisciplinaryteamduringthefirstsixmonthsoflife.Its focusisonbreastfeedingpromotionandtheeffectivenessof childcare,sothatmotherscansuccessfullymaintain exclu-sivebreastfeedinginaccordancewiththerecommendations ofthe BrazilianMinistry ofHealth,which followthe stan-dardsof theWorld HealthOrganization and theAmerican AcademyofPediatrics.15,16
Initially,allinfantsenrolledintheunitwhowereneara
full-monthage(1,2,3,4,5,or6months)wereconsidered.
Thus,childrenwere stratifiedintosixgroups accordingto
age(agein months±5days).Childrenwhose agewasout
ofthisten-daymargininthesixstratawerenotincludedin
thestudy.
Inaddition,theinclusioncriteriacomprisedonlyinfants
who were exclusively breastfed frombirth, born at term
(gestational age between 37 and 42 weeks), who did
nothave low birth weight(birth weight<2500g),withno
complicationsintheneonatalperiodandwhosemothershad
Hb levels<12g/dL at the timeof data collection. Infants
who had suspected infectious or inflammatory processes
at the time of the blood sample collection (presence of
morbidsigns/symptomsand/orwhitebloodcellcount
alter-ations)andthechildrenofmotherswhoreportedahistory
ofmalariaorhadaninfectiousdiseaseatthetimeofdata
collectionwereexcluded.
The samplesizewascalculatedbasedonthemeanand
standard deviationvalues ofHb fromthepilot study
con-ducted before the start of data collection. To meet the
objectiveoftheresearch,theestimateresultedin40
chil-drenineach agegroup,consideringabetavalue=0.1and
bilateralalpha=0.05.
Children who received breast milk directly from the
breast or expressed,or human milk fromanothersource,
withnootherliquidsorsolids,withtheexceptionofdrops
orsyrupsconsistingofvitamins,oralrehydrationsalts,
min-eralsupplements,ormedicationswereconsideredtobeon
exclusivebreastfeeding.16
Thus, 245 motherswhose children metthe criteriafor
inclusion in the study were interviewed during the data
collection. However, fivechildren were excluded for
pre-senting at least oneof the exclusioncriteria, resultingin
240children.Later,19other childrenwereexcludedfrom
theanalysisduetoinsufficientmaterialtocarryoutthe
lab-oratorytests,resultinginasamplinglossof7.9%.Thus,the
study included 221 binomials (mother---child), which were
distributed in six groups according to age: 1 (n=40), 2
(n=27),3(n=39),4(n=38),5(n=40)and6(n=37)months.
Nobinomial(mother---child)wasincludedinmorethanone
agegroupofthesample.
Duringthecareactivitiesprovidedtotheselected
chil-dren, the main investigator (RFVM) filled out, together
withthemothers,avalidated,structured,pre-coded
ques-tionnaire with information about the gestational history,
delivery,andpost-partumconditions,neonatalhistory,and
thefamily’ssocioeconomicstatus.
Thecollectionofbloodsamplesfromchildrenand
moth-erswerecarriedoutafteramedicalconsultation,through
puncture of the radial or cubital peripheral vein on the
anterior arm surface. The Cell-Dyn® 3.500 (ABBOTT, IL,
USA) equipment was used for the determination of Hb
concentrationofmothersandchildren.Serumferritin
val-ueswere obtained by immunoenzymaticdetermination in
serumorplasmausingtheenzymelinkedfluorescentassay
(ELFA)techniquethroughtheautomatedtestVIDAS®Ferritin
(Biomerieux,Paris, France) which allowsthe quantitative
measurementofferritininserumorplasma.
Childrenwereweighedina pediatricscale certifiedby
theNationalInstituteofMetrology,Quality,andTechnology
(InstitutoNacional de Metrologia, Qualidadee Tecnologia
[INMETRO])withamaximumcapacityof16kg.An
anthro-pometricrulerwithamovablecursorwasusedtomeasure
height.The anthropometric proceduresused in the study
werethoserecommendedbytheMinistryofHealth.17
The anthropometric indicator chosen for nutritional
assessment wasthe weightfor age ratio and the criteria
usedtoexpressitwastheZ-score.18 Thedifferenceinthe
Z-score of the weightfor age ratiobetween the time of
datacollection and the birth of the child was defined as
theproportionalweightgainindicator.19
Completed questionnaires were evaluated regarding
theirinternalconsistency.Theinformationwastransferred
todatabaseswithdoubleentryandsubsequentlyvalidated
inordertocorrectinputerrors.Thestatisticalpackageused
wasSPSS(SPSSInc.Released2007.SPSSforWindows,
Ver-sion16.0,IL,USA).20
Consistency analyses and univariate and bivariate
descriptivestatisticswereperformed.Analysisofvariance
(ANOVA)wasusedtocomparemeans,andPearson’s
correla-tioncoefficientswerecalculatedtoquantifythecorrelation
betweenHb levelsof mothersand childrenin the sixage
groups.21
For the control of confounding variables in the
corre-lationbetweenmothers’Hb andchildren’sHb,a multiple
linearregressionmodelwasadjustedwithregression
coef-ficientestimates.22
Thecriteriafortheselectionofcontrolvariablesforthe
finalmodelconsideredthesituationswithplausibleeffect
onmaternal Hb level (age, iron use at the time of data
collection,andtimeofironuseduringpregnancy)andHb
ofchildren(weightgain,serumferritinlevel,andgender).
Amaximumlevel of0.05 wasconsideredasastatistically
significantassociation.
ThestudywasapprovedbytheResearchEthics
Commit-teeoftheEscolaPaulistadeMedicina/UniversidadeFederal
deSãoPaulo(UNIFESP/EPM) andauthorizedbytheHealth
Unit of Belém do Pará. An informed consent form was
signed by all mothers who agreed to participate in the
study.
Results
Table1shows the characteristics ofthe assessedmothers
andchildren, according tothe children’sage groups. The
mean Hb levels of mothers and children ranged,
respec-tively,from12.9to13.3g/dLand11.4to12.0g/dL.
Inthesixagegroupsassessed,comparisonsofthemean
serumferritinlevel(p<0.001)andtheproportionalweight
gain(p<0.001) showedstatisticallysignificant differences
Table1 Comparisonbetweenthemeanswiththeirrespectivestandarddeviationsofthecharacteristicsofmothersandchildren
inexclusivebreastfeeding,accordingtoagegroup(2006---2008).
Characteristics (continuous variables)
Agerange(months) pvaluea
1(n=40) 2(n=27) 3(n=39) 4(n=38) 5(n=40) 6(n=37)
¯
x(SD) ¯x(SD) ¯x(SD) ¯x(SD) ¯x(SD) ¯x(SD)
MaternalHb
(g/dL)
13.0(0.8) 12.9(0.6) 13.0(0.7) 13.3(0.8) 13.2(1.0) 13.1(1.0) 0.293
Children’sHb
(g/dL)
11.9(1.8) 11.4(1.6) 11.4(1.4) 12.0(1.8) 11.9(1.7) 11.8(1.7) 0.468
Children’sferritin
(ng/mL)
193.6(148.9) 110.7(114.1) 70.4(61.3) 45.4(36.5) 32.6(23.0) 31.2(23.2) <0.001
Birthweight(kg) 3.32(0.41) 3.22(0.30) 3.24(0.28) 3.23(0.37) 3.18(0.41) 3.24(0.32) 0.653
W/Aatbirthb 0.03(0.85) −0.18(0.69) −0.12(0.58) −0.16(0.78) −0.27(0.87) 0.13(0.72) 0.642
Currentweight (kg)
4.24(0.53) 5.38(0.42) 6.45(0.78) 7.08(0.76) 7.33(0.92) 8.13(0.71) <0.001
CurrentW/Ab −0.18(0.83) 0.01(0.64) 0.38(0.93) 0.39(0.78) 0.13(0.99) 0.53(0.81) 0.003
Proportional weightgainc
−0.22(0.51) 0.18(0.51) 0.51(0.87) 0.55(0.78) 0.40(0.99) 0.66(0.87) <0.001
Birthlength(cm) 49.4(2.2) 49.2(1.3) 49.0(1.6) 49.0(1.9) 48.2(1.8) 48.9(1.5) 0.136 Currentlength
(cm)
54.4(1.7) 58.3(1.6) 61.5(2.2) 63.4(2.4) 63.9(2.3) 67.3(1.7) <0.001
Maternalage (years)
20.9(5.5) 20.5(5.5) 20.4(5.3) 19.7(4.9) 19.8(4.9) 21.6(5.7) 0.664
Maternalschooling (yearsofstudy)
8.8(2.4) 8.1(2.7) 8.5(2.1) 8.3(2.2) 8.1(2.2) 8.5(2.5) 0.836
Ironuseduring pregnancy(m)
2.4(2.3) 2.6(2.0) 3.0(2.4) 3.2(2.3) 3.0(2.3) 1.9(1.9) 0.098
Prenatal(number ofconsultations)
6.8(1.7) 6.4(2.0) 6.7(1.3) 6.4(1.8) 7.0(2.1) 6.8(2.0) 0.752
¯
x,mean;SD,standarddeviation;Hb,hemoglobin;g/dL,gramperdeciliter;ng/mL,nanogrampermilliliter;kg,kilogram;cm,centimeter; m,months;W/A,weightforageratio.
aANOVA. b Z-score.
c ProportionalweightgaininZ-scorecorrespondstothedifferenceoftheZ-scoreoftheweightforageratiobetweenthetimeofdata collectionandthechildren’sbirth.
ofmothers andchildren,not entirelysensitive totheage difference(weightand length at birth, maternal age and education,ironuseduringpregnancy,andnumberof prena-talvisits),werestatisticallysimilar(p>0.05).
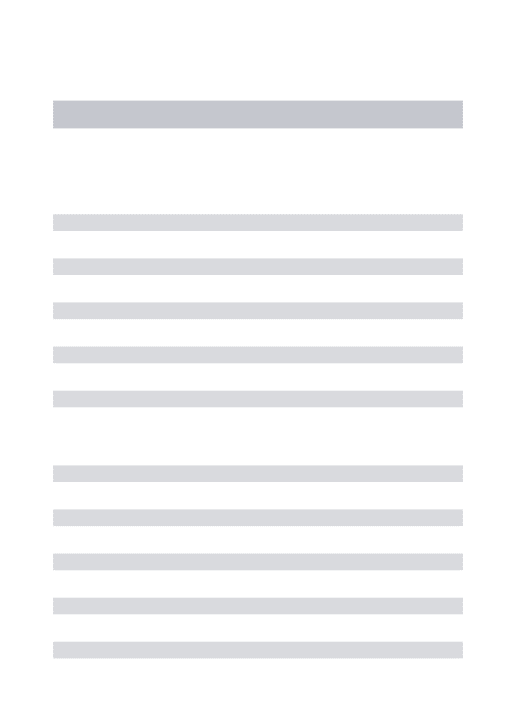
Fig. 1 presents Pearson’s correlation coefficients
between Hb levels (g/dL) of mothers and children in
each age group. The coefficients ranged from 0.253 at
theage of 3 monthsto0.601, at theage of 5 months.It
canbe observed thatthe Hb level ofmothers wasbetter
correlatedwiththeHb ofchildren at theage groups of4
months(r=0.578)and5months(r=0.601).
Amultiplelinearregressionmodelwasadjustedtoeach
ofthesixagegroups(Table2).Theregressioncoefficients
werehigherat theagegroups of4months(ˇ=1.134)and
5 months (ˇ=0.845), meaning that for each increase of
1g/dLinmaternal Hb, therewasan estimated increaseof
approximately1.1---0.8g/dLHbinthechildrenatthesetwo
agegroups, respectively.These estimateswerecontrolled
in themodels for threematernal variables (age, ironuse
at the time data collection, and time of iron use during
pregnancy)andthreevariablesofthechildren(weightgain,
serumferritinlevel,andgender).
Discussion
The mean Hb levels of mothers and Hb and birth weight of the children in the six age groups were greater than 12.5g/dL,11.0g/dL,and3.0kg,respectively. Lowermean serumferritinlevelswereobservedmonthtomonth,from thefirsttothesixthmonth,andthedistributionsofZscores ofW/Aratioatbirthandatthetimeofdatacollectionwere normal.
The highest correlation coefficients between Hb levels of mothers and children occurred in the age groups of 4 and5months.The sixlinearregressionmodelsresulted in positiveregressioncoefficientsandastatisticallysignificant association atages1,3,4,5,and6months,regardless of threecharacteristicsofmothers(ageandiron supplemen-tationduringpregnancyandatthetimeofdatacollection) andthreecharacteristicsofthechildren(weightgain,serum ferritinlevel,andgender).
18
16
14
12
10
12 13 14
Maternal Hb (g/dL)
Adjusted values Children’s Hb (g/dL) 1 month (n=40)
r=0.324
15 16
8
18
16
14
12
10
12 13 14
Maternal Hb (g/dL) 3 months (n=39)
r=0.253
15 16
18
16
14
12
10
12 13 14
Maternal Hb (g/dL) 5 months (n=40)
r=0.601
15 16
8
18
16
14
12
10
12 13 14
Maternal Hb (g/dL) 2 months (n=27)
r=0.339
15 16
8
18
16
14
12
10
12 13 14
Maternal Hb (g/dL) 4 months (n=38)
r=0.578
15 16
8
18
16
14
12
10
12 13 14
Maternal Hb (g/dL) 6 months (n=37)
r=0.355
15 16
8 8
Figure1 Pearson’scorrelationcoefficientsbetweenhemoglobinlevelsofmothersandchildren(g/dL),accordingtoagegroup (2006---2008).
Table2 Linearregressionmodelsbetweenhemoglobinlevelsofmothersandchildren,accordingtotheagerange(2006---2008).
Children’shemoglobinlevel(g/dL) Agerange ˇ (95%CI) pvalue B
Maternal
hemoglobinlevel
(g/dL)
1m 0.735 (0.024;1.447) 0.043 0.335
2m 1.135 (−0.067;2.337) 0.063 0.422
3m 0.763 (0.060;1.466) 0.034 0.368
4m 1.134 (0.447;1.820) 0.002 0.520
5m 0.845 (0.436;1.255) <0.001 0.506
6m 0.568 (0.055;1.080) 0.031 0.318
ˇ,coefficientofregression;CI,confidenceinterval;B,standardizedbetacoefficient;m,month.
Modelsadjustedformaternalage,timeofironuseduringpregnancy,ironuseatthetimeofdatacollection,weightgain,children’s ferritinlevel,andgender.
understandingofthisassociationinhumans,asthegrowth rate in experimental animals is significantly higher when comparedtohumans (i.e.,in the firstfourweeks of life, a rabbit increases six times their body weight, while a
with humans (e.g., ratio of 1:6 in rats and 1:16 in humans).7
A study in humans that evaluated iron concentrations
inbreastmilkshowedadecreaseinmeanironlevels
dur-ing the duration of lactation from 0.6 to 0.3mg/L, but
withgreatvariabilityamongthevalues,which potentially
reflectsthemultifactorialnatureofdeterminingiron
defi-ciencyanditsconcentrationinbreastmilk.23Infact,Kumar
et al.24 found lower iron levels in the breast milk of
mothers withsevere anemia,when compared to
nonane-micmothers’milk. However,themagnitudeof the effect
was approximately 2.6mmol/L, that is, a mean
reduc-tion of only 17% in iron concentration, which potentially
does not result in differences in the iron status of their
children.
Domellof et al.,25 when assessing breast milk samples
collected from 191 mothers at nine months postpartum,
found no association between levelsof zinc, copper, and
iron(hemoglobin,plasmaferritin,transferrinreceptors,and
zincprotoporphyrin)andthelevelsofthesemicronutrients
inthemother’smilk.
Even though there may be an association between Hb
of mothers and children in the first months of life,13 the
typeofinfantfeeding,particularlyexclusivebreastfeeding,
hasbeenpoorlyconsideredintheanalysisoftheresultsof
existingstudies.ThestudybyKilbrideetal.,12which
longi-tudinallyevaluatedchildreninthefirst12monthsoflifeand
consideredfeedingpracticesinthisperiod,foundexclusive
breastfeedingdurationofonly2.3months,whichaffectsthe
interpretationofthefindingsasitdoesnotconstitutethe
idealsettingoftheyounginfantnutrition.
Thepresentstudyfoundastatisticallysignificant
corre-lationbetween hemoglobinlevelsofmothersandchildren
infiveofthesixagegroupsanalyzed,showingthatmaternal
Hbstatus,asanindicatorofbodyironavailability,influences
theHbstatusofchildreninthefirstsixmonthsoflife,even
withadequate ironstores, acquired by newborns at term
andnormalweightinlatepregnancy.
The age groups shown here presented homogeneity
betweentheassessedcharacteristics,minimizing
misinter-pretationsrelatedtofactorsthataredeterminantsofserum
Hb levels. Additionally, the adjustment in the
multivari-ate analysis of mothers and children, which potentially
interferes with iron status, reinforces this influence and
thereforehighlightstheimportanceofexclusive
breastfeed-inginthefirstsixmonthsoflife,eveninchildrenwithgood
ironstoresatbirth.
Hayetal.26 concludedthatserumferritinlevelsincord
bloodcouldbeapredictorofironstatusinthefirsttwoyears
oflife.Although thetimeofclamping andtheironstatus
intheumbilical cordblood mayinfluencethe hemoglobin
levelsofchildren, thecorrelation between ferritin values
incordbloodandthoseintheinfant’smotherhasnotbeen
demonstrated.12,24,27,28
Itisworthmentioningthattheironstatusinthe
umbili-calcordbloodandtimeofclampingwerenotconsideredin
thisstudy,asthese datawerenotavailable andthe
eval-uation started withhemoglobin and ferritin levels in the
children’sfirstmonthoflife.Thismayhaveinfluencedthe
resultsshownhere.
Inturn,theexclusionofmothersandchildrenwith
infec-tiousdiseases duringthe data collectionperiodruled out
thepossibilitythattheseconditionscouldinterferewiththe
results.AlthoughC-reactiveproteinwasnotmeasured,the
motherswereaskedaboutthepresenceofrecentinfections,
and abnormalities in the levels of circulating leukocytes
wereverified.
Particularly,the exclusionof subjectswithahistory of
malaria from the sample, as the present study was
per-formed in an endemicareaof the disease,prevented the
influence of this infection on Hb levels, which has been
demonstratedinwomenandinfants.14
Thisstudy evaluatedonlymothers without anemiaand
their children on exclusive breastfeeding in the first six
monthsoflife,controlling,duringthesampleselection
pro-cess,theeffectsofmaternalanemiaanddifferentchildren’s
dietsonthecorrelationbetweenHblevelsofmothersand
oftheirchildren.Thisinferentialcharacteristicisuniquein
humanstudies.
Itis noteworthy thatthe six age groups assessed here
consistedofdifferentbinomials(mother---child),and
follow-up was not conducted, but rather a separate assessment
ofsixdifferentagegroupsaccordingtotheadopted study
design(cross-sectional).Evenifthegroupshadsimilar
char-acteristics,alongitudinalstudywouldbeclosertotheideal
methodologytoachievethegoalproposedherein.However,
itislessfeasibleduetotheneedtocollectrepeatedblood
samplesfromhealthychildrenandmothers,whichissurely
more uncomfortable and, consequently, results in sample
loss.
Inthiscontext,regardlessofthemultifactorialnatureof
anemiaassessmentinchildhood,thepresent findings
indi-cate that thereis a correlation betweenthe mother’s Hb
levelsandtheirchildren’sonexclusivebreastfeedinginthe
firstsixmonthsoflife.Despitetheoriginalityand
method-ologicalstrengthofthisresearch,additionalfollow-upand
ideallycontrolledstudiesappeartobenecessaryinorderto
confirmtheresultsfoundhere.
Finally, the authors recommend the adoption of three
strategies to ensure the appropriate level of body iron
in early life: effective iron supplementation of pregnant
womenduringprenatalcare,timelycordclamping(atleast
1min after birth), and continuous support of exclusive
breastfeeding in the first six months of life, which,
com-binedwiththegoodcareatbirth,providesthechildenough
ironquantityandqualitytomeetthedemandsofphysical
growth.24,29
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
References
1.LozoffB.Irondeficiencyandchilddevelopment.FoodNutrBull. 2007;28:S560---71.
2.Brasil.Ministérioda Saúde.Pesquisa NacionaldeDemografia eSaúdedaCrianc¸aedaMulher(PNDS),2006: dimensõesdo processoreprodutivoedasaúdedacrianc¸a.Brasília:Ministério daSaúde;2009.
3.BresaniCC,BresaniAI,BatistaFilhoM,FigueroaJN.Anemiae ferropeniaemgestantes:dissensosderesultadosdeumestudo transversal.RevBrasSaudeMaternInfant.2007;7:S15---21. 4.SatoAPS,FugimoriE,SzarfacSC,SatoJR,BonadioIC.
Prevalên-ciadeanemiaemgestanteseafortificac¸ãodasfarinhascom ferro.TextoContextoEnferm.2008;17:474---81.
5.RajM,FaridiMM,SinghO,RusiaU.Mother’sironstatus, breast-milkironand lactoferrin---aretheyrelated?EurJClinNutr. 2006;60:903---8.
6.RajS,FaridiMM,RusiaU,SinghO.Aprospectivestudyofiron statusinexclusivelybreastfedterminfantsupto6monthsof age.IntBreastfeedJ.2008;3:3.
7.Lanzkowsky P. The influence of maternal iron-deficiency anaemia on the haemoglobin of the infant. Arch Dis Child. 1961;36:205---9.
8.Paiva AA, Rondó PH, Pagliusi RA, Latorre MR, Cardoso MA, GondimSS.Relationshipbetween theironstatusofpregnant womenandtheirnewborns.RevSaudePublica.2007;4:321---7. 9.RaoR,GeorgieffMK.Ironinfetalandneonatalnutrition.Semin
FetalNeonatalMed.2007;12:54---63.
10.Teixeira Mde L, Lira PI, Coutinho SB, Eickmann SH, Lima MC.Influenceofbreastfeedingtypeandmaternal anemiaon hemoglobinconcentrationin6-month-oldinfants.JPediatr(Rio J).2010;86:65---72.
11.SinglaPN,GuptaVK,AgarwalKN.Storageironinhumanfoetal organs.ActaPaediatrScand.1985;74:701---6.
12.Kilbride J, Baker TG, Parapia LA, Khoury SA, Shugaidef SW, JerwoodD.Anaemiaduringpregnancyasariskfactorfor iron-deficiencyanaemiaininfancy:acase---controlstudyinJordan. IntJEpidemiol.1999;28:461---8.
13.dePeeS,BloemMW,SariM,KiessL,YipR,KosenS.Thehigh prevalenceoflowhemoglobinconcentrationamongIndonesian infantsaged3---5monthsisrelatedtomaternalanemia.JNutr. 2002;132:2215---21.
14.KouraKG,OuédraogoS,CottrellG,LePortA,MassougbodjiA, GarciaA.Maternalanaemiaatdeliveryandhaemoglobin evolu-tioninchildrenduringtheirfirst18monthsoflifeusinglatent classanalysis.PLoSONE.2012;7:e50136.
15.AAP.AmericanAcademy ofPediatrics.Breastfeedingand the useofhumanmilk.Pediatrics.2012;129,e827---41.
16.Brasil. Ministério da Saúde. Secretaria de Atenc¸ão à Saúde. DepartamentodeAtenc¸ãoBásica(CadernosdeAtenc¸ãoBásica, n.23).Saúdedacrianc¸a:nutric¸ãoinfantil:aleitamentomaterno ealimentac¸ãocomplementar.(SérieA.NormaseManuais Téc-nicos).Brasília:MinistériodaSaúde;2009.
17.Brasil.MinistériodaSaúde.SecretariadePolíticasdeSaúde -áreatécnicadesaúdedacrianc¸a.Acompanhamentodo cresci-mentoedesenvolvimentoinfantil.Brasília:MinistériodaSaúde; 2002.
18.WHO. WHO Child Growth Standards. Length/height-for-age, weight-for-age,weight-for-heightandbodymassindex-for-age. Methods and development. Geneva: World Health Organiza-tion;2006.Availablefrom:http://www.who.int/childgrowth/ standards/technicalreport/en/16[cited14.05.15].
19.KonstantynerT,TaddeiJA,OliveiraMN,PalmaD,ColugnatiFA. Riscosisoladoseagregadosdeanemiaemcrianc¸as frequentado-rasdeberc¸áriosdecreches.J.Pediatr(RioJ).2009;85:209---16. 20.StataCorp. Stata Statistical Software: Release 14. College
Station,TX:StataCorpLP;2015.
21.KirkwoodBR,SterneJA.Essentialmedicalstatistics.2nd ed. Malden(MA):BlackwellScience;2003.p.165---76.
22.KleinbaumDG,KupperLL,NizamA,MullerKE.Applied regres-sionanalysisandothermultivariablemethods.4thed.Pacific Grove:DuxburyPress;2008.
23.Siimes MA,Vuori E,Kuitunen P.Breast milkiron --- declining concentration during the course of lactation. Acta Paediatr Scand.1979;68:29---31.
24.Kumar A, RaiKA, Basu S, DashD, SinghJS. Cordblood and breastmilkironstatusinmaternalanemia.Pediatrics.2008;21: e673.
25.Domellof M, Lonnerdal B, Dewey KG, Cohen RJ, Hernell O. Iron,zinc,andcopperconcentrationsinbreastmilkare inde-pendentofmaternalmineralstatus.AmJClinNutr.2004;79: 111---5.
26.HayG,RefsumH,WhitelawA,MelbyeEL,HaugE,Borch-Iohnsen B. Predictorsofserum ferritin and serum solubletransferrin receptor innewborns and theirassociations withironstatus duringthefirst2yoflife.AmJClinNutr.2007;86:64---73. 27.Harthoorn-LasthuizenEJ,LindemansJ,LangenhuijsenMM.Does
irondeficienterythropoiesisinpregnancyinfluencefetaliron supply?ActaObstetGynecolScand.2001;80:392---6.
28.ShaoJ,LouJ,RaoR,GeorgieffMK,KacirotiN,FeltBT,etal. Maternalserumferritin concentrationispositivelyassociated withnewbornironstoresinwomenwithlowferritinstatusin latepregnancy.JNutr.2012;142:2004---9.