REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
droperidol
and
ondansetron
prophylactic
effect
on
subarachnoid
morphine-induced
pruritus
夽
Fabio
Ferreira
da
Cunha
Brião
a,∗,
Marcio
Leal
Horta
a,
Bernardo
Lessa
Horta
b,
Guilherme
Antônio
Moreira
de
Barros
c,
Ana
Paula
Behrensdorf
d,
Ingrid
Severo
d,
Mariana
Antunes
Nunes
d,
Roberta
Boabaid
d,
André
Real
daAnesthesiology,UniversidadeCatólicadePelotas(UCPel),Pelotas,RS,Brazil
bEpidemiology,UniversidadeFederaldePelotas(UFPel),Pelotas,RS,Brazil
cUniversidadeEstadualPaulista,FaculdadedeMedicinadeBotucatu(UNESP),Pelotas,RS,Brazil
dUniversidadeCatólicadePelotas(UCPel),Pelotas,RS,Brazil
Received11August2013;accepted20November2013 Availableonline28April2015
KEYWORDS
Droperidol; Morphine; Ondansetron; Pruritus; Subarachnoid injection
Abstract
Backgroundandobjectives: Theprophylacticeffectofondansetrononsubarachnoid morphine-inducedpruritusiscontroversial,whileevidencesuggeststhatdroperidolprevents pruritus. Theaimofthisstudyistocomparetheeffectsofdroperidolandondansetrononsubarachnoid morphine-inducedpruritus.
Methods:180ASAIorIIpatientsscheduledtoundergocesareansectionsundersubarachnoid
anesthesiacombinedwithmorphine0.2mgwererandomizedtoreceive,afterthechild’sbirth, metoclopramide10mg(GroupI---control),droperidol2.5mg(GroupII)orondansetron8mg
(GroupIII).Postoperatively,thepatientswereassessedforpruritus(absent,mild,moderateor
severe)orothersideeffectsbyblindedinvestigators.Patientswerealsoblindedtotheirgroup allocation. Thetendency to presentmore severe forms ofprurituswas compared between groups.NNTwasalsodetermined.
Results:Patients assigned to receive droperidol [Proportional odds ratio: 0.45 (95% confi-denceinterval 0.23---0.88)]reportedlesspruritusthanthosewhoreceivedmetoclopramide. Ondansetroneffectwassimilartometoclopramide[Proportionaloddsratio:0.95(95% confi-dence interval 0.49---1.83)]. The NNT for droperidol and ondansetron was 4.0 and 14.7, respectively.
Conclusions:Ondansetrondoesnotinhibitsubarachnoidmorphine-inducedpruritus.
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
夽 StudyperformedattheAnesthesiologyDepartmentoftheUniversidadeCatólicadePelotas,Pelotas,RS,Brazil.
∗Correspondingauthor.
E-mail:[email protected](F.F.C.Brião).
http://dx.doi.org/10.1016/j.bjane.2013.11.005
PALAVRAS-CHAVE
Droperidol; Morfina; Ondansetron; Prurido; Injec¸ão subaracnoidea
Comparac¸ãodosefeitosprofiláticosdodroperidoledoondansetronsobreoprurido provocadopelamorfinasubaracnoidea
Resumo
Justificativaeobjetivos: O efeito profilático do ondansetron sobre prurido provocado pela morfinasubaracnoideaécontroverso,enquantoevidênciassugeremqueodroperidolprevine o prurido. O objetivo do presente trabalho é comparar o efeito do droperidol com o do ondansetronsobreopruridoprovocadopelamorfinasubaracnoidea.
Métodos: 180pacientesASAIouIIprogramadasparaseremsubmetidasacesarianassob
aneste-siasubaracnoideaàqualforamacrescentados0,2mgdemorfinaforamdivididasaleatoriamente parareceber,logoapósonascimentodacrianc¸a,10mgdemetoclopramida(grupoI---controle),
2,5mgdedroperidol(grupoII),ou8mgdeondansetron(grupoIII).Noperíodopós-operatórioas
pacientesforamavaliadasquantoaoprurido(ausente,leve,moderadoouintenso)ououtros efeitoscolateraisporobservadoresquenãosabiamaalocac¸ãodaspacientes.Aspacientes tam-bémnãosabiamdasuaalocac¸ão.Osgruposforamcomparadospelasuatendênciaaapresentar formasmaisseverasdeprurido.TambémdeterminamosoNNT.
Resultados: As pacientes alocadas para receber droperidol [Odds Ratio Proporcional: 0,45 (Intervalo de Confianc¸ade 95%0,23---0,88)]relataram menos pruridodo queasque rece-berammetoclopramida.Oefeitodoondansetronfoisemelhanteaodametoclopramida[Odds RatioProporcional:0,95(IntervalodeConfianc¸ade95%0,49---1,83)].ONNTdodroperidolfoi 4,0eodoondansetronfoi14,7.
Conclusões: Oondansetronnãoinibiuopruridoprovocadopelamorfinasubaracnoidea. ©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Inapreviouswork,1wecomparetheprophylacticeffectof
droperidol,alizapride,propofol,andpromethazineon sub-arachnoid morphine-induced pruritus. Droperidol was the most effective agent; propofol and alizapride were less efficient;andpromethazine,asotherantihistamines,2was
ineffective. Kjelberg and Tramér,3 in a review study of
pharmacological treatment of morphine-induced pruritus, concludedthatdroperidolwasmoreeffectivethananyother drug,otherthanmorphineantagonists.Buttheirreviewonly includedonestudyinwhichondansetronwasusedto antag-onizethealfentanil-inducedpruritusinpatientsundergoing generalsurgery.
Evidences of ondansetron effectiveness are contradic-tory.Somestudieshavereportedondansetroneffectiveness fortreating4orpreventingpruritus.5,6Ithasalsobeen
sug-gestedthatondansetron reducespruritusseveritywithout reducing its incidence.7 On the other hand, other
stud-ieshavereportedtheineffectivenessofondansetronorits lowerefficacycomparedtootherdrugs.8---10
Giventhiscontradictionandlackofcomparisonbetween droperidol and ondansetron, we decided to compare the prophylacticeffectofthetwodrugsinpatientsundergoing cesareansection(C-section).
Methods
ThisstudywasapprovedbytheResearchEthicsCommittee oftheUniversidadeCatólicadePelotas(Ref:2011/18),and written informedconsent wasobtained fromall patients.
Thisrandomizeddouble-blindtrialenrolled180patientsASA Ior II scheduled for C-section, regardless of thecause of obstetricindication.Inadditiontotherefusaltoparticipate in this research, patients were excluded in the following cases:inadequateanesthesia,anyitchyskindisease,recent use of opioids or any other drug that causes respiratory depression, hyperemesis,or inability to answer questions clearly.
Upon arrival at the operating room, patients received aninfusionofRinger’slactateand50mcgoffentanylwere intravenously(IV)administered.The total volumeoffluid infusedduringsurgerywasrecordedinthreemoments:at lumbar puncture; at the child’s birth, and at the end of surgery.Standard monitoring(non-invasivebloodpressure, SpO2,andECG)wasestablished.
Subarachnoid anesthesia was induced via the lateral approach11 with Quincke needle at L2-L3 or L3-L4, using
213 patients evaluated
Excluded (n=33)
Did not meet the inclusion criteria (28) Refused to participate (5)
Randomized (n=180)
Allocated in metoclopramide group (n=60)
Allocated in droperidol group (n=60)
Allocated in ondansetron group (n=60)
Evaluated (n=60) Evaluated (n=60) Evaluated (n=60)
Figure1 Flowchartofthestudy.
withfractionateddosesofmetaraminol.Shortlyafterbirth, 15---20units of oxytocin were usedto obtain good uterine contraction. In three cases, 0.2mg of methylergometrine wereusedforthesamepurpose.
The distribution of 180 participants in three groups of 60 patients was performed using a table of random numbers. According tothis allocation table, immediately after birth, the patients in Group 1 received metoclo-pramide(10mg); patients in Group II received droperidol (2.5mg); and patients in Group III received ondansetron (8mg)(Fig.1).InGroupI,metoclopramidewasusedbecause itwasshownthatithasnoeffectonmorphine-induced pru-ritus, so it can be used to prevent nausea and vomiting andasaplaceboformorphine-induced pruritus.Induction ofanesthesiaandadministrationofdrugsin theoperating roomwereperformedbyanesthesiologists(FFCBandMLH). Inthepostoperativeperiod,patientswereseenby anesthe-siologistsunawaretotheirexperimentalallocation(APB,IS, MAN,RB, and RA).The patients were alsoblinded tothe treatmentreceived,characterizingthedouble-blindnature ofthisstudy.Patientswereevaluatedeverysixhoursfora periodof24h.Afterthisperiod,theywereevaluatedtwice dailyuntildischargefromhospital.Inadditiontopruritus, anyotheradverseeffectsseenorreportedbythepatient, evenifonlyinoneofthevisits,wasrecordedandconsidered positive.
Prurituswasclassifiedasabsent;mild(restrictedtoone area,suchasfaceorarms,andnotdisturbingthepatient, sometimes denied and only reported after insistence); moderate(affectingalargerarea,suchasfaceandarmsor faceandanteriorsurface ofthe chest,but notdisturbing thepatientandthereforenotrequiringtreatment)or inten-sive (extensive or generalized pruritus, often disturbing
thepatient tothe pointwhere treatment isindicated). It was registered according to the highest intensity seen or reported. If treatment was necessary, droperidol 1.25mg wasusedintravenously.
Based on previous studies, we estimate that the inci-denceofmoderateorseverepruritusshouldbe30%inthe control group, and that an effective intervention would reduce theincidence by60%. The sample sizecalculation estimated60 patientspergroupforasignificancelevel of 95%andapowerof80%.
Fordataanalysis,weusedlogisticregressiontoestimate the trendof moderateor severe pruritus andthe propor-tionaltrendmodel toestimatethetendency topresent a moreseverepruritus.Inordinalregression,theproportional modelwasusedtoestimatetheoddsratioandthe presump-tionofproportionaloddswasassessedusingBranttest.NNT evaluationwasbasedontheincidenceofmoderateorsevere pruritus.
Results
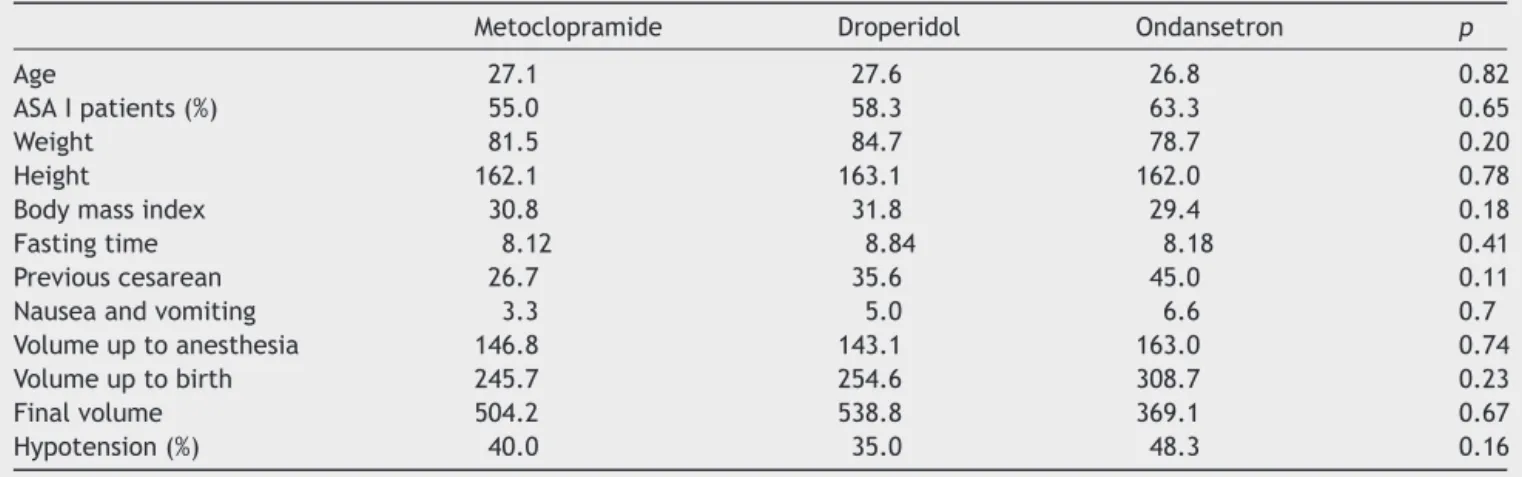
Table 1shows thatthe distributionof some basic charac-teristics (age, weight, height, BMI, fasting time, number ofpreviousC-sections,andincidenceofpostoperative nau-seaorvomiting)wassimilarbetweengroups.Therewasno differencebetweengroupsinfluidreplacementvolumeor proportionofpatientswhoreceivedtreatmentfor hypoten-sion.
Table1 Distributionofthebasiccharacteristicsofthethreegroups.
Metoclopramide Droperidol Ondansetron p
Age 27.1 27.6 26.8 0.82
ASAIpatients(%) 55.0 58.3 63.3 0.65
Weight 81.5 84.7 78.7 0.20
Height 162.1 163.1 162.0 0.78
Bodymassindex 30.8 31.8 29.4 0.18
Fastingtime 8.12 8.84 8.18 0.41
Previouscesarean 26.7 35.6 45.0 0.11
Nauseaandvomiting 3.3 5.0 6.6 0.7
Volumeuptoanesthesia 146.8 143.1 163.0 0.74
Volumeuptobirth 245.7 254.6 308.7 0.23
Finalvolume 504.2 538.8 369.1 0.67
Hypotension(%) 40.0 35.0 48.3 0.16
Table2 Incidenceandseverityofpruritusinthethreegroups.
Drugs Pruritus
Absent Mild Moderate Severe
Metoclopramide 9(15%) 19(31.7%) 25(41.7%) 7(11.7%)
Droperidol 14(23.3%) 29(48.3%) 12(20%) 5(8.3%)
Ondansetron 9(15%) 23(38.3%) 17(28.3%) 11(18.3%)
Moreover, the incidence of severe pruritus was lower in womenassignedtoreceivedroperidol.
Table 3 shows that the tendency to present with a strongerformofprurituswasloweramongpatientsassigned to receive droperidol. The tendency to present with a strongerformofprurituswas0.45(95%CI:0.23---0.88)for patients receiving droperidol comparedwith thosein the metoclopramide group. However, ondansetron group was similartometoclopramidegroup.Inanotherapproach,we alsoevaluatedthe tendency topresent withmoderate or severepruritus,usinglogisticregression.Theresultsofthis analysisweresimilartothoseobservedinordinalregression, withpatientsassignedtoreceivedroperidolpresentingless tendency tohave moderateor severe pruritus [oddsratio 0.35(95%CI,0.16---0.74)].
The NNT for droperidol was 4.0, while that for ondansetronwas14.7.
Discussion
Our results show that droperidol was more effective than metoclopramide and ondansetron both when we
approached the trend toward moderate or severe pruri-tus or when the severity of pruritus was the approach point.
Therearesomepossibleexplanationsforthedifferences inourresultsandthosereportedintheliterature.First, opi-oidsaredifferentintheirpharmacokinetics,andmorphine hasaverylongactionwhenadministeredbythe subarach-noid route.12 Therefore, it is very difficult to compare
fentanylorsufentanilwithmorphine.Anotherdifferenceis thattheincidenceofpruritusinC-sectionishigherthanin othersurgeries.5
Regardingthesafetyoftheuseofdroperidol,thereare reportsofarrhythmias,13 butitwasnotseen inour
previ-ousinvestigation,whenweuse1.25mgofdroperidolin60 patients,neitherinthisstudywiththedoseof2.5mg.Inany case,itseemsinterestingtouselowerdosesofdroperidol inordertostudyitseffectiveness.
Insummary,ourstudyshowsthatondansetrondoesnot inhibitsubarachnoidmorphine-inducedpruritusinpatients undergoingC-section.Theseresults,combinedwithour pre-viousresults,allowustosaythatdroperidolisasatisfactory drugtoantagonizethesubarachnoidmorphine-induced pru-ritus.
Table3 Ordinalandlogisticregressionofgroups2and3(droperidolandondansetron,respectively),havinggroup1 (metoclo-pramide)asareference.
Group1 Group2 Group3
Ordinalregression---oddsratio(95%confidenceinterval) Reference 0.45(0.24---0.88) 0.95(0.49---1.83) Logisticregression---oddsratioofpersistingmoderate
toseverepruritus(95%confidenceinterval)
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Horta ML, Morejón LCL, da Cruz AW, et al. Study of the prophylactic effect of droperidol, alizapride, propofol and promethazine on spinal morphine-induced pruritus. Br J Anaesth.2006;96:796---800.
2.Harrison DM, Sinatra R, Morgese L, et al. Epidural narcotis andpatient-controlledanalgesiaforpost-cesareansectionpain relief.Anesthesiology.1988;68:454---7.
3.Kjelberg F, Tramér MR. Pharmacological control of opioid-inducedpruritus:aquantitativesystematicreviewof random-izedtrials.EurJAnaesthesiol.2001;18:246---57.
4.Charuluxananan S, Somboonviboon W, Kyokong O, et al. Ondansetron for treatment of intrathecal morphine-inducedpruritus after cesarean delivery. Reg Anesth Pain Med.2000;25:535---9.
5.Yeh HM, Chen LK, Lin CJ, et al. Prophylactic intravenous ondansetron reduces theincidence ofintrathecal morphine-induced pruritus in patients undergoing cesarean delivery. AnesthAnalg.2000;91:172---5.
6.Iatrou CA, Dragoumanis CK, Vogiatzakis GI, et al. Prophy-lactic intravenous ondansetronand dolasetron inintrathecal
morphine-induced pruritus: a randomized, double-blinded, placebo-controlledstudy.AnesthAnalg.2005;101:1516---20.
7.KolmA,FerrazAAF,ModoloNSP,etal.Profilaxiadoprurido cau-sadopelaadministrac¸ãosubaracnóideadesufentanil:efeitos dodroperidol,danalbufina,doondansetronedacombinac¸ão deles.RevBrasAnestesiol.2006;56:28---33.
8.Siddik-SayyidSM,AquadMT,TahaSK,etal.Doesondansetron orgranisetronpreventsubarachnoidmorphine-inducedpruritus aftercesareandelivery?AnesthAnalg.2007;104:421---4.
9.TamdeeD,CharuluxanananS,PunjasawadwongY,etal.A ran-domized controlled trial of pentazocine versus ondansetron for the treatment of intrathecal morphine-induced pruri-tus in patients undergoing cesarean delivery. Anesth Analg. 2009;109:1606---11.
10.Sarvela PJ, Halonen PM, Soikkeli AI, et al. Ondansetron and topisetron do not prevent intraspinal morphine- and fentanyl-inducedpruritus in electivecesareandelivery. Acta AnaesthesiolScand.2006;50:239---44.
11.Hatfalvi B. Postulated mechanisms for postdural puncture headache and review of laboratory models. Reg Anesth. 1996;20:329---36.
12.BallantyneJ.TheMassachusetsGeneralHospitalhandbookof painmanagement. 2nd ed.Philadelphia: LippincottWilliams andWilkins;2002.p.117.