REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
the
conventional
CMAC
and
the
D-blade
CMAC
with
the
direct
laryngoscopes
in
simulated
cervical
spine
injury----a
manikin
study
Divya
Jain
∗,
Mandeep
Dhankar,
Jyotsna
Wig,
Amit
Jain
DepartmentofAnaesthesiologyandIntensiveCare,PostgraduateInstituteofMedicalEducationandResearch,Chandigarh,India
Received17February2013;accepted10June2013 Availableonline25December2013
KEYWORDS
CMAC
videolaryngoscope; D-bladeCMAC; Simulatedcervical spine;
Manikinstudy
Abstract
Background: CMACvideolaryngoscopehasrecentlybeenintroducedforvideoscopeguided intu-bation.Theaimofourstudywastocompare andevaluatetheefficacy oftheconventional bladeandtheangulatedDbladeoftheCMACvideolaryngoscopewiththedirectlaryngoscopes insimulatedcervicalspineinjurypatientsontheairwaymanikin.
Materialsandmethods: Followingpoweranalysis,33residentdoctorswereenrolledtoperform endotrachealintubationusingall the4differentlaryngoscopesnamely theMacintosh laryn-goscope,McCoylaryngoscope,conventionalCMACvideolaryngoscopeandtheDbladeofthe CMACvideolaryngoscopesontheairwaymanikininsimulatedcervicalspineinjury.The demo-graphicvariablesoftheresidentdoctorswererecorded.Theoutcomesmeasuredincludedvocal cordvisualization(Cormack---Lehanegrading),timetakentointubate,numberofattemptsfor successfulintubationandoptimizingmaneuversrequired.
Results:Theuseofindirectvideolaryngoscopesresultedinbetterglotticvisualizationin com-parisontothedirectlaryngoscopes(CL-I)in20/33(60.6%)intheMacintoshgroup,24/33(72.7%) inMcCoygroup,30/33in(90.9%)inVlcgroupand32/33(96.9%)inVldgroup.Thetimetakento intubateaveragedto15.54±2.6inMacintoshgroup,18.90±4.47inMcCoygroup,20.21±7.9 inVlcgroupand27.42±9.09inVldgroup.The1stattemptintubationsuccessratewas84.8% (Macintosh),72.7%(McCoy),90.9%(Vlc)and,78.7%(Vld).
Conclusions: TheoverallperformanceoftheconventionalCMACbladeprovedtobethebest whencomparedwiththeD-bladeCMAC,MacintoshbladeandtheMcCoybladeforintubation insimulatedcervicalspinepatientsbyanesthesiaresidents.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](D.Jain).
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Videolaringoscópio C-MAC;
C-MACD-blade; Simulac¸ãodelesão dacolunacervical; Estudoemmodelo
Comparac¸ãodoC-MACconvencionaleC-MACD-bladecomlaringoscópiosdiretosem
simulac¸ãodelesãodacolunacervical---estudoemmodelo
Resumo
Justificativaeobjetivo:OvideolaringoscópioC-MACfoirecentementeintroduzidopara orien-taraintubac¸ão.OobjetivodesteestudofoicomparareavaliaraeficáciadolaringoscópioC-MAC delâminaconvencionaleC-MACdelâminaangulada(D-blade)comlaringoscópiosdiretosem simulac¸ãodepacientescomlesãodecolunacervicalusandomodelodeviasaéreas.
Materiaisemétodos:Após a análise do poder do estudo, 33 médicos residentes foram inscritospararealizarintubac¸õesendotraqueais,usandotodososquatrolaringoscópios difer-entes:laringoscópioMacintosh,laringoscópioMcCoy,videolaringoscópiosC-MACconvencionale C-MAC D-blade em modelos de viasaéreas comsimulac¸ão de lesão da coluna cervical. As variáveis demográficas dos médicos residentes foram registradas. Os resultados avaliados incluíramvisualizac¸ãodaspregasvocais(classificac¸ãodeCormack-Lehane),temponecessário paraintubar, númerodetentativaspara intubac¸ãobem-sucedidaemanobrasdeotimizac¸ão necessárias.
Resultados: Ousode laringoscópios indiretos resultou em melhorvisualizac¸ão daglote em comparac¸ãocomoslaringoscópiosdiretos(CL-I)em20/33(60,6%)nogrupoMacintosh,24/33 (72,7%)nogrupoMcCoy,30/33(90,9%)nogrupoVlce32/33(96,9%)nogrupoVld.Amédiado temponecessárioparaentubarfoide15,54±2,6nogrupoMacintosh,18,90±4,47nogrupo McCoy,20.21±7,9nogrupoVlce27,42±9,09nogrupoVld.Ataxaparaaprimeiratentativa deintubac¸ãobem-sucedidafoide84,8%(Macintosh),72,7%(McCoy),90,9%(Vlc)e78,7%(Vld).
Conclusão:OdesempenhogeraldalâminadoC-MACconvencionalmostrousermelhorquando comparadocomodaslâminasdoC-MACD-blade,MacintosheMcCoyparaintubac¸ãoemmodelo desimulac¸ãodelesãodacolunacervicalrealizadapormédicosresidentesdeanestesia. ©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Ability to intubate the trachea and secure the airway is one of the life saving skills to be acquired by all the training medical students. Failure to do so can result in hypoxia,airway trauma,oesophageal intubationand even cardiorespiratory arrest.1 Successful intubation requires
proper alignment of the oro-pharangeal-laryngeal axis.2
However, in cervical spine patients this alignment is not possibleresultinginincreasedriskoffailedintubations.3---6
Due to morbidity and mortality associated with failed intubation,7,8 anesthetists are constantly improvising on
newermeanstoreducetheincidenceoffailedintubations. Tilldate,thecurvedMacintoshbladeiscommonlybeing usedby the anesthetists for airway management of such patients.9 Over the years many different types of
laryn-goscopeshavebeenintroducedtoreducetheincidenceof thesecomplications.McCoylaryngoscopewithitshingedtip hasshowntoprovidebetterglottisvisualizationin compar-isontotheMacintoshblade.10---12
Inthepastfewyearswehavewitnessedanincreasinguse ofvideolaryngoscopesforthemanagementofthepatients withdifficultintubation.13,14
CMACvideolaryngoscope(KarlStorz,Tuttligen,Germany) hasbeen recentlyintroduced for videoscopeguided intu-bation. This portable videolaryngoscope comes with the originalMacintoshblademadeofsteelalongwiththeCMOS digital cameraand high power LED. Due to the presence of the normal Macintosh blade CMAC (Vlc) provides both directandindirectglottic visualization.15,16 CMAC-Dblade
(Vld) videolaryngoscope is a newer additionto the CMAC system.IncomparisontotheconventionalCMACblade,the Dblade hasan inbuiltangulation.17 Duetothehighly
pro-nouncedcurvature,itprovidesabetterviewofthelaryngeal structures.
Tilldate, nostudyhascomparedthetwobladesofthe CMACvideolaryngoscopewiththeMacintoshandtheMcCoy laryngoscopes.
Theaimofourstudywastocompareandevaluatethe efficacyoftheconventionalbladeandtheangulatedDblade of the CMAC videolaryngoscope with the direct laryngo-scopes in simulated cervical spine injury patients on the airwaymanikin.
Materials
and
methods
This studywasconductedover aperiodof 3monthsfrom January2012toMarch2012.
As this study did not involve any human subjects, approvalfromtheinstitutionalethicsreviewcommitteewas nottaken.
Participation of the resident doctors wason voluntary basis. Fortyresident doctorswithaminimumof 6months anesthesiatrainingexperiencewereenrolledinthestudy.
the two different blades of the CMAC videolaryngoscope ontheairwaymanikininitsnormalstate.Onlythirty-three residentswhosucceedtointubatewithallthefourblades ontwoconsecutiveattemptswereenrolledinthestudy.
Theairwaymanikin(Ambu®AirwayManagementTrainer) withcervical collarinsituwasusedin thestudy for simu-lated cervicalspine injury.Size 3blade ofthe Macintosh, McCoy andthe CMACvideolaryngoscope wereused in the study.A7mmcuffedendotrachealtubemountedonawell lubricatedangulatedstylet waskeptpreparedfor intuba-tion.
Intubation was performed by all the resident doctors usingall the 4different laryngoscopesnamely the Macin-toshlaryngoscope,McCoylaryngoscope,conventionalblade C-MACvideolaryngoscopeandtheDbladeoftheCMAC vide-olaryngoscopes.
Thesequenceofthedevicesusedforintubationwas ran-domizedusingslipinaboxtechnique.
Demographic dataof theresident doctorsincludingthe age,durationofexperience,andnumberofintubations per-formedwithMacintoshlaryngoscopewererecorded.
Theprimaryoutcomewasthedurationoftimetakenfor successfultrachealintubation.Thetimetakenforsuccessful intubationwasdefinedasthe timetakenfor ofthe inser-tionoftheblade betweentheteeth,tilltheconfirmation of the tube by connecting it tothe AMBUbag and inflat-ingthe lungs.Weusedthe similartechniquefor both the directandindirectlaryngoscopestostandardizethe proto-col.The numberof optimization maneuversrequired (use ofabougie,BURPorbackward-upward-rightwardpressure onlarynx,secondassistant)toaidtrachealintubation,and theCormackandLehanegradeatlaryngoscopywerenoted. Afailedintubationattemptwasdefinedasinabilityto intu-bateafterthreelaryngoscopicattemptsorwithin120s.
Statisticalanalysis
Graphpad Prism6 (by Graphpad SoftwareInc.Avenida de laPlayaLaJolla,CA92037,USA)wasusedtoanalyzethe data. The data for duration of successful tracheal intu-bation, number of intubation attempts, Cormack Lehane laryngoscopic view and number of optimizing maneuvers were analyzed using repeated measures ANOVA. Post hoc analyses among individual groups were carried out using Tukey---KramerMultipleComparisonsTest.Apvalueof<0.05 wasconsideredassignificant.
Results
Demographicvariablesoftheparticipants(Table1)
A total of 33 residents enrolled completed the study. All residentshadperformedmorethan100intubationswiththe
Macintosh
15.5
±2.6
18.9
±4.4
20.2
±7.9
27.4
±9.1
McCoy Vlc Vld
0 10 20 30 40
Ti
m
e (seconds)
Figure1 TimetakentointubateusingMacintosh,McCoy,Vlc andVldblades.
Macintoshlaryngoscope. The residents were familiar with theuse ofMcCoy laryngoscope, especiallyinsituations of difficultairway.
However, none of them had any experience with the CMACvideolaryngoscope.
Themeanage,theyearsofclinicalexperienceand num-berofintubationsperformedwithMacintoshlaryngoscope aregiveninTable1.
TimetakentoIntubate(Fig.1,Table2)
Time taken to intubate using either of the blades of the CMAC wasprolonged in comparison to the Macintosh laryngoscope(p<0.05withVlcandp<0.001withVld). How-evertimetakentointubateusingMcCoylaryngoscopewas comparablewiththeMacintoshblade.Timetakento intu-bateusingtheDbladeCMACwasprolongedincomparison tothe McCoylaryngoscope.Conventionalblade CMACwas comparable to McCoy laryngoscope with regard to time takentointubate.
Laryngoscopicview(Tables2and3)
Cormack Lehane grading system was used to grade the laryngoscopicviewobtainedonthe1stintubationattempt. Statistically significant improvement in the laryngoscopic viewwasseenwithVlcandVldincomparisontheMacintosh laryngoscopeandtheMcCoylaryngoscope.McCoy laryngo-scopeprovidedslightimprovementinthelaryngoscopicview incomparisontotheMacintoshlaryngoscopebutthe differ-encewasnotstatisticallysignificant.
Table1 Demographicvariablesoftheresidents.
Numberofresidents Meanage(years) Clinicalexperience(years) Noofintubations(Macintosh)
33 24(3) 1.8(1) 120(100---300)
Table2 ResultsoftrachealintubationusingMacintosh,McCoy,conventionalCMACbladeandtheD-bladeofCMACincervical spinescenarioinmanikin.
Macintosh McCoy Vlc Vld p-Value
Timeforsuccessfulintubation(s) 15.55±2.69 18.91±4.47a 20.21
±7.9a 27.42
±9.1a,b p<0.0001
Laryngoscopicview(Cormack---Lehane) 1.39±0.49 1.27±0.45 1.09±0.29a,b 1.03±0.17a,b p=0.001
Dataexpressedasmean±SD.
ap<0.05whencomparedwithMacintoshLaryngoscope. b p<0.05whencomparedwithMcCoyLaryngoscope.
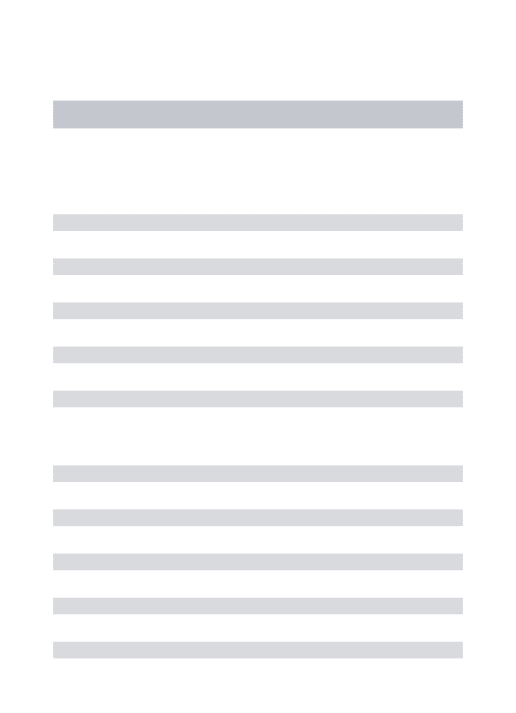
Numberofintubationattempts(Table3)
The percentage of 1st attempt successful intubation was highestwithVlcandlowestwithMcCoylaryngoscope. How-everthesedifferenceswerenotstatisticallysignificant.
Numberofmaneuversrequired(Table3)
Significantly less number of optimizing maneuvers were requiredbytheVlcandVldwhencomparedwiththe Macin-toshlaryngoscope.McCoylaryngoscopewascomparableto theMacintoshlaryngoscope withregard tothe numberof optimizingmaneuversrequired.
Discussion
Inability to successfully secure the airway is one of the mostdreadedcomplicationsofanesthesia.Intubationofthe tracheainvolves twobasic components--- exposure ofthe glottic opening and negotiation of the endotracheal tube throughthevocalcords.
Direct laryngoscopy requires head flexion and neck extensionforthealignmentoftheoro-pharangeal-laryngeal axis to obtain glottis exposure. Manual in line stabiliza-tionin cervical spine patients prevents neck movements, therebyresultinginpoorglotticexposure.18---20Thishasled
toincreasedmorbidityincervicalspinepatientsduetothe difficultiesencounteredintheairwaymanagementofsuch patients.21,22
Various alternative devices have been developed to reduce the incidenceof suchcomplications. McCoy laryn-goscopewithadistalleveringtiprequireslessforceforthe alignmentoftheaxisandimprovesthelaryngoscopicview.23
Recently, indirect laryngoscopes aregaining popularity in themanagement ofpatients withcompromised airway. Thesedevicesincorporatevideooroptictechnologyforthe visualizationofthetracheawithoutalignmentoftheoral, pharangealandlaryngealaxis.24CMACvideolaryngoscopein
manikinmodelshaveshowntoprovidebettervisualization of the glottis and faster intubation time.25 In trials
con-ductedonhumansubjects CMAChasshown itssuperiority overangulatedvideolaryngoscopes.26
InitialevaluationoftheCMAC-Dbladevideolaryngoscope hasshownitssuperiorityovertheMacintoshlaryngoscope.27
However, thereis paucity of literature on the use of the CMAC-Dbladevideolaryngoscopeincervicalspinepatients. Wehad designed thestudy toevaluate the efficacy of recently introduced D-blade CMAC with the conventional CMACanddirectlaryngoscopes.
In the present trial, greater prolongation of the intubationtimewasshownusingtheCMAC-Dblade video-laryngoscopeincomparisontotheMacintosh,McCoyandthe CMACvideolaryngoscope.Lesser amount oftimetaken by thedirectlaryngoscopescanbeattributedtothefamiliarity of theparticipantstotheMacintoshandtheMcCoy laryn-goscopes. The difference in the intubation time between the C MAC and the CMAC-D blade videolaryngoscope can beduetothedifferenceintheshapeofthe twodevices. TheconventionalCMACincorporatesthenormalMacintosh laryngoscopewhiletheCMAC-Dbladevideolaryngoscopehas
Table3 Resultsofattemptsoftrachealintubationandoptimizingmaneuversused.
Parameterassessed Macintosh McCoy Vlc Vld
Noofintubationattempts
1 29(87.9%) 24(72.7%) 30(90.9%) 26(78.7%)
2 4(12.1%) 9(27.3%) 3(9.1%) 7(21.2%)
Optimizingmaneuvers
Notused 24(72.7%) 28(84.8%) 32(96.9%) 30(90.9%)
Used 9(27.3%) 5(15.2%) 1(3%)a 3(9.1%)a
Laryngoscopicview(CLgrading)
I 20/33(60.6%) 24/33(72.7%) 30/33(90.9%)a 32/33(96.9%)a
II 13/33(39.3%) 9/33(27.2%) 3/33(9%)a 1/33(3%)a
Dataexpressedasnumber(percentage).
Figure2 Figure showing theconventional CMACblade and theD-bladeCMACvideolaryngoscope.
aninbuilt pronouncedangulation(Fig.2).Thisincreasein angulationfrom18◦ inCMAC(size3)to40◦ intheDblade
CMACnecessitatestheuseofacurvedstyletandresultsin greater manipulation in negotiating the tube through the vocalcords.
CMACandtheCMAC-Dbladevideolaryngoscopeprovided bettervisualizationoftheglottisopeningincomparisonto the directlaryngoscopes. This findingis supported by the earliertrialscomparingtheindirectlaryngoscopeswiththe directlaryngoscopesonmanikin.28
We would like to highlight that in comparison to the CMAC, theCMAC-Dblade videolaryngoscopeprovided bet-terglottisvisualizationasgraded bytheCormack---Lehane laryngoscopicview.Thisdifferenceagaincanbeexplained bytheincreasedangulationoftheDblade.
InourstudythenewerD-bladeundoubtedlyprovidedthe best laryngoscopicview; however our residents had diffi-cultyinnegotiationofthetube.Similarproblemhasearlier been encountered with the other available videolaryngo-scopeswithangulatedblades.29
Recent studies comparing the CMAC, glidescope, storz DCI with the Macintosh laryngoscope found better glottis visualizationwiththeCMACincomparisontotheother indi-rectanddirectlaryngoscopes.29
Whether angulated blade videolaryngoscopes require moreskillandpracticetoperformendotrachealintubation needstobeevaluatedthroughlargerrandomizedcontrolled trials.
Themajorlimitationofourstudyisthatitwasconducted onmanikinandnotonhumansubjects.Theresultsobtained fromthisstudycannotbedirectlyextrapolatedtothehuman population.Thesimulationofdifficultairwayonamanikin can reproduce some aspects of difficult laryngoscopy and tosome extentmimic thedifficultiesencountered in cer-vical spine patients. Another limitation of the study was thattheanesthetistswerenotblindedtothedevicebeing used.Wedidnotrecordthetimeofbestlaryngoscopicview andtimetakenforintubationseparately.Comparisonofthe D-bladeCMACwith other angulatedvideolaryngoscopes is
requiredthroughlargerrandomizedtrialstoprovethefact thatangulationcanincreasethedifficultyinnegotiatingthe endotrachealtubethroughtheglotticaperture.
However,wefeelsuchtrialscanprovideaninitial eval-uationof the device and canbe a stepping stonefor the futuretrialsonthehumansubjects.
Conclusion
Indirectvideolaryngoscopes providedbetter glottis visual-izationand1stattemptsuccessfulintubationsincomparison tothedirectlaryngoscopes.Therewasaprolongationinthe intubationtimewiththeDbladeCMACvideolaryngoscopein comparisontotheconventionalCMACandthedirect laryn-goscopes.However, asthis is a manikin study the results cannotbe similar in actual situations of human subjects; thereforelargerrandomizedhumantrialswouldberequired infuturetoverifytheresultsofourstudy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
WewouldliketothankKarlStorzEndoscopyIndiaPvt.Ltd., NewDelhi, India for providing usthe CMAC videolaryngo-scopeonloanforourstudy.
References
1.Mort TC.Emergency trachealintubation:complications asso-ciated withrepeated laryngoscopic attempts. Anesth Analg. 2004;99:607---13.
2.EzriT,WartersRD.Indicationsfortrachealintubation.In: Hag-bergCA,editor.Benumof’sairwaymanagement:principlesand practice.2nded.Philadelphia:Mosby;2007.p.371.
3.CriswellJC, Parr MJA,Nolan JP. Emergency airway manage-ment in patients with cervical spine injuries. Anaesthesia. 1994;49:900---3.
4.RheeKJ,GreenW,HolcroftJW,MangiliJA.Oralintubationin themultiplyinjuredpatient:theriskofexacerbatingspinalcord damage.AnnEmergMed.1990;19:511---4.
5.SudermanVS,CrosbyET,LuiA.Electiveoraltrachealintubation incervicalspineinjuredadults.CanJAnaesth.1991;38:785---9.
6.CaplanRA,PosnerKL,WardRJ,CheneyFW.Adverserespiratory eventsinanesthesia:aclosedclaimsanalysis.Anesthesiology. 1990;72:828---33.
7.CheneyFW.TheAmericanSocietyofAnesthesiologistsClosed ClaimsProject: what have we learned, how has it affected practice,and howwill itaffectpracticeinthefuture? Anes-thesiology.1999;91:552---6.
8.PetersonGN,DominoKB,CaplanRA,PosnerKL,LeeLA,Cheney FW.Managementofthedifficultairway:aclosedclaims analy-sis.Anesthesiology.2005;103:33---9.
9.MacintoshRR.Anewlaryngoscope.Lancet.1943;1:205.
10.McCoyEP,MirakhurRK.Theleveringlaryngoscope.Anaesthesia. 1993;48:516---9.
12.CarleyS,ButlerJ.UseoftheMcCoylaryngoscopeinpatients with suspected cervical spine fracture. J Accid Emerg Med. 2000;17:364---5.
13.Stroumpoulis K, Pagoulatou A, Violari M, et al. Video-laryngoscopy in the management of the difficult airway: a comparison with the Macintosh blade. Eur J Anaesthesiol. 2009;26:218---22.
14.AsaiT.Videolaryngoscopes---dotheytrulyhaverolesindifficult airways?Anesthesiology.2012;116:515---7.
15.CavusE,KieckhaeferJ,DoergesV,MoellerT,TheeC,Wagner K.TheC-MACvideolaryngoscope:firstexperienceswithanew deviceforvideolaryngoscopy-guidedintubation.AnesthAnalg. 2010;110:473---7.
16.ByhahnC,IberT,ZacharowskiK,etal.Trachealintubationusing themobileC-MACvideolaryngoscopeforpatientswitha simu-lateddifficultairway.MinervaAnestesiol.2010;76:577---83.
17.MissaghiSM,KrasserK, ZadrobilekE.TheD-BLADE:a signifi-cantlymodifiedbladefortheStorzC-MACVideolaryngoscopy System.IntJAirwayManage.2010---2011;6.
18.SmithCE,PinchakAB,SidhuTS,RadesicBP,PinchakAC,Hagen JF.Evaluationoftrachealintubationdifficultyinpatientswith cervicalspineimmobilization:fiberoptic(WuScope)versus con-ventionallaryngoscopy.Anesthesiology.1999;91:1253---9.
19.HeathKJ.Theeffectoflaryngoscopyofdifferentcervicalspine immobilizationtechniques.Anaesthesia.1994;49:843---5.
20.Nolan JP, WilsonME.Orotrachealintubationin patientswith potentialcervicalspineinjuries:anindicationforthegum elas-ticbougie.Anaesthesia.1993;48:630---3.
21.HastingsRH,KelleySD.Neurologicdeteriorationassociatedwith airwaymanagementinacervicalspine-injuredpatient. Anes-thesiology.1993;78:580---3.
22.Fitzgerald RD, Krafft P, Skrbensky G, et al. Excursions of the cervical spine during tracheal intubation: blind oral intubation compared with direct laryncoscopy. Anaesthesia. 1994;49:111---5.
23.McCoyEP,MirakhurRK,RaffertyC,etal.Acomparisonofthe forcesexertedduringlaryngoscopy.TheMacintoshversusthe McCoyblade.Anaesthesia.1996;51:912---5.
24.JungbauerA,SchumannM,BrunkhorstV,BorgersA,Groeben H.Expecteddifficulttrachealintubation:aprospective com-parisonofdirectlaryngoscopyand videolaryngoscopyin200 patients.BrJAnaesth.2009;102:546---50.
25.McElwain J, Malik MA, Harte BH, Flynn NM, Laffey JG. Comparison of the C-MAC videolaryngoscope with the Mac-intosh, Glidescope, and Airtraq laryngoscopes in easy and difficult laryngoscopy scenarios in manikins. Anaesthesia. 2010;65:483---9.
26.AzizMF,DillmanD,FuR,BrambrinkA.Comparative effective-nessoftheC-MACvideolaryngoscopeversusdirectlaryngoscopy inthesettingofthepredicteddifficultairway.Anesthesiology. 2012;116:629---36.
27.CavusE, NeumannT, Doerges V, et al. Firstclinical evalua-tionoftheC-MACD-bladevideolaryngoscopeduringroutineand difficultintubation.AnesthAnalg.2011;11:482---5.
28.TeohWH,SaxenaS,ShahMK,SiaAT.Comparisonofthree video-laryngoscopes:PentaxAirwayScope,C-MAC,Glidescopevsthe Macintoshlaryngoscopefor tracheal intubation.Anaesthesia. 2010;65:1126---32.