w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Impacts
of
social
support
on
symptoms
in
Brazilian
women
with
fibromyalgia
Rodrigo
Pegado
de
Abreu
Freitas
a,∗,
Sandra
Cristina
de
Andrade
b,
Maria
Helena
Constantino
Spyrides
c,
Maria
Thereza
Albuquerque
Barbosa
Cabral
Micussi
b,
Maria
Bernardete
Cordeiro
de
Sousa
daUniversidadeFederaldoRioGrandedoNorte(UFRN),FaculdadedeCiênciasdaSaúdedeTrairí,SantaCruz,RN,Brazil bUniversidadeFederaldoRioGrandedoNorte(UFRN),DepartamentodeFisioterapia,Natal,RN,Brazil
cUniversidadeFederaldoRioGrandedoNorte(UFRN),DepartamentodeEstatística,Natal,RN,Brazil dUniversidadeFederaldoRioGrandedoNorte(UFRN),InstitutodoCérebro,Natal,RN,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14August2014
Accepted23May2016
Availableonline9August2016
Keywords:
Fibromyalgia
Socialsupport
Pain Functionality Depression
a
b
s
t
r
a
c
t
WeaimedtoassesstheimpactofsocialsupportonsymptomsinBrazilianwomenwithFM.
Anobservational,descriptivestudyenrolling66womenwhometthe1990AmericanCollege
ofRheumatology(ACR)criteria.SocialsupportwasmeasuredbytheSocialSupportSurvey
(MOS-SSS),functionalitywasevaluatedusingtheFibromyalgiaImpactQuestionnaire(FIQ),
depressionwasassessedusingtheBeckDepressionInventory(BDI),anxietywasmeasured
usingtheHamiltonAnxietyScale(HAS),affectivitywasmeasuredbyPositiveandNegative
AffectSchedule(PANAS),andalgometrywascarriedouttorecordpressurepainthreshold
(PPth)andtolerance(PPTo)at18pointsrecommendedbytheACR.Patientsweredivided
intonormal(NSS)orpoorsocialsupport(PSS)groupswithPSSdefinedashavinga
MOS-SSSscorebelowthe25thpercentileoftheentiresample.Mann–WhitneyorUnpairedt-test
wereusedtocompareintergroupvariablesandFisher’sforcategoricalvariables.Analysis
ofcovarianceandPearsoncorrelationtestwereused.Nodifferencesinsociodemographic
variablesbetweenPSSandNSSwerefound.DifferencesbetweenNSSandPSSgroupswere
observedforallfoursubcategoriesofsocialsupportandMOS-SSStotalscore.Significant
differencesbetweenNSSandPSSondepression(p=0.007),negativeaffect(p=0.025)and
PPTh(p=0.016)werefound.Affectionatesubcategoryshowedpositivecorrelationbetween
painandpositiveaffectinPSS.Positivesocialinteractionsubcategoryshowedanegative
correlationbetweenFIQanddepressionstate.Thereforesocialsupportappearstocontribute
toamelioratementalandphysicalhealthinFM.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND
license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](R.P.Freitas).
http://dx.doi.org/10.1016/j.rbre.2016.07.001
2255-5021/©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
Impacto
do
apoio
social
sobre
os
sintomas
de
mulheres
brasileiras
com
fibromialgia
Palavras-chave:
Fibromialgia
Apoiosocial
Dor
Funcionalidade Depressão
r
e
s
u
m
o
Objetivou-seavaliaroimpactodoapoiosocialsobreossintomasdemulheresbrasileiras
comfibromialgia(FM).Trata-sedeumestudoobservacionaldescritivoqueselecionou66
mulheresqueatendiamaoscritériosdoColégioAmericanodeReumatologia(ACR)de1990.
OapoiosocialfoimedidocomoSocialSupportSurvey(MOS-SSS),afuncionalidadecomo
QuestionáriodoImpactodaFibromialgia(FIQ),adepressãocomoInventáriodeDepressão
deBeck(BDI),aansiedadecomaEscaladeAnsiedadedeHamilton(HAS),aafetividadecom
oPositiveandNegativeAffectSchedule(Panas)efoifeitaalgometriapararegistrarolimiarda
doràpressão(LDP)eatolerânciaálgicaàpressão(TAP)nos18pontosrecomendadospelo
ACR.Ospacientesforamdivididosnosgruposapoiosocialnormal(ASN)ouruim(ASR);
oASRfoidefinidocomoumapontuac¸ãonosMOS-SSSabaixodopercentil25daamostra
total.Usou-seotestedeMann-Whitneyouotestetnãopareadoparacompararvariáveis
intergruposeodeFisherparaasvariáveiscategóricas.Usaram-seaanálisedecovariância
eotestedecorrelac¸ãodePearson.Nãohouvediferenc¸anasvariáveissociodemográficas
entreosgruposASNeASR.Observaram-sediferenc¸asentreosgruposASNeASRpara
todasasquatrosubcategoriasdeapoiosocialepontuac¸ãototaldoMOS-SSS.
Encontraram-sediferenc¸assignificativasentreoASNeoASRnadepressão(p=0,007),afetonegativo
(p=0,025)eLDP(p=0,016).Asubcategoriaapoioafetivomostroucorrelac¸ãopositivaentrea
doreoafetopositivonogrupoASR.Asubcategoriainterac¸ãosocialpositivamostrouuma
correlac¸ãonegativaentreoFIQeoestadodedepressão.Portanto,oapoiosocialparece
contribuirparaamelhorianasaúdementalefísicanaFM.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC
BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Fibromyalgia(FM) isa noprogressive rheumaticcondition,
without definitive pathophysiology or measurable
indica-torsofdiseaseactivity.Thisconditionismarkedbychronic
widespreadpainandfrequentlyassociatedsymptoms
includ-ing fatigue, sleep disturbances, cognitive dysfunction, and
depressiveepisodes.1,2 FMprevalencevariesbetween0.66%
and4.4%inthe Brazilianpopulationand ismorecommon
amongwomenthan men,particularlyinthe35-to60-year
agegroup.3ActivitylimitationsinFMhaveanimpactonwork
abilityandimposeaheavyburdenonpatientsintermsof
dis-ability,lossofqualityoflifeandcosts,aswellasaneconomic
burdenonsociety.4,5
Episodesofchronicpain,depressionandlowfunctionality
seem to affect interpersonal (including marital)
relation-shipsandwork activity.6,7 WomenwithFMfaceskepticism
andinadequatetreatmentfrommedicalprofessionals,
fam-ilyand friends,particularly iftheir disabilityisnot visible,
furthercompoundingphysicalandemotionaldistress.8Thus,
patientswithFMmayshowchangesinprosocialbehavioror
perceptionofsocialsupport.9Satisfactionwithsocialsupport,
socialparticipation,andlivingwithsomeonehadprotective
effectsondepression andother symptomsin womenwith
FM.9,10
Littleis knownabout the influenceofpsychosocial
fac-torsontheprocessingofpain,anxietyanddepressionamong
FMpatientsandnostudiesregardingsocialsupportandFM
symptoms have been conducted in Brazil. Social support,
whichincludesemotionalandinstrumentalsupport,isa
cop-ing resource inchronic diseases suchasFMand has been
reportedtobeamoreimportantfactorinhealthpromotion.11
Socialsupportrepresentsanexternalresourcethatisaccessed
fromothersandoperationalizedasasocialresource.The
lit-erature indicatesthatsocialsupportisavitalaspectoflife
in general and mental health and can be defined as
sub-conceptsofsocialnetworks.12,13Inotherwords,socialsupport
isasocialnetworkfunctionprovidedbymemberswithina
socialnetwork,generallyrelatedtothe numberand/or
fre-quencyofcontactswithfamily members,relatives,friends,
andcolleagues.13
Social support has been defined in numerous ways,
generally referring to resources supplied to individuals
in need by their social network, and can be measured
through the individual’sperceptionofthe degree towhich
interpersonal relationships can fulfill certain social
sup-port functions.14 Traditionally, four types ofsocialsupport
are suggested: emotional, instrumental, appraisal which
involvesinformationrelevanttoself-evaluation,and
informa-tion.
Social support varies among countries, cultures and
individualperception.FMpatientsmayhavechangesin
per-ceptionofsocialsupportaccordingtosymptomsseverity.The
purposeofthepresentstudywastoassesstheimpactofsocial
supportonperipheralpainsensibility,functionality,and
pos-itiveandnegativemoodstates,suchasdepression,affectivity
Methodology
Typeandstudysubjects
Anobservational,descriptivestudywasconducted.Subjects
wererecruitedfrom theMedicalClinicoftheOnofreLopes
UniversityHospital(HUOL)andfromthePhysiotherapyClinic
ofUniversidade Potiguar,Natal,Brazil.TheResearchEthics
CommitteeoftheFederalUniversityofRioGrandedoNorte
approvedalltheproceduresdescribedinthisreport(274/2010).
Informedconsentwasobtainedfromallsubjects,andstudy
protocolscompliedwithethicalguidelines.
Sixty-six women, aged 20–76 years, who met the 1990
AmericanCollegeofRheumatology(ACR)criteriaforFM,were
recruited.15Thefollowinginclusioncriteriawereadopted:(a)
medicaldiagnosisofFM,(b)abilitytounderstandstudy
objec-tivesandanswerthequestions,(c)notundergoingphysical
therapyorrehabilitationprogramsduringthethreeprevious
months,(d)donotusecorticosteroids,analgesicsand/or
anti-inflammatorydrugsduringtheweekofevaluation.Exclusion
criteria were:(a) physicaland/or organic difficulties, when
thesecompromisedquestionnaireapplicationandanalgesic
tests;(b)rheumaticand/or autoimmunediseases including
chronic fatigue syndrome, rheumatoid arthritis, gout and
lupus.
Assessment
Theexperimentwasperformedinaquietsettingwithoutany
interruptionsandwithsubjectsshieldedfromotherpatients.
Social supportwas measured by means of the Medical
OutcomesStudySocialSupportSurvey(MOS-SSS),a19-item
questionnairecoveringmultipledimensionsofsocialsupport,
anddesignedtobeeasilyapplied.16Theitemsinthis
instru-mentdonotspecifythesourceofsupport(e.g.,family,friends,
communityorothers),andtheymeasureperceivedavailability
offunctionalsupport.OriginallydesignedinEnglish,the
MOS-SSShasbeen translatedandadaptedtoPortugueseversion
thatshowedgoodpsychometricproperties.17Test–retest
reli-abilitywasconsistentlyhighforthesubscales(withintraclass
correlationcoefficientsrangingfrom0.78to0.87),and
inter-nalconsistency,asassessedbyCronbach’salpha,rangedfrom
0.75to0.91.Althoughtherearefivetheoreticaldimensionsin
theMOS-SSS,previousvalidityinvestigationshavesuggested
that questions related to emotional and information
sup-portshouldbegroupedinthesamedimension.Accordingly,
the present study used four dimensions: tangible support,
affectivesupport,emotional/informationsupportandpositive
socialinteraction.
Thesubjectswere divided into two groupsaccording to
their level ofsocial support.Poor socialsupport (PSS)was
definedashavingaMOS-SSSscorebelowthe25thpercentileof
theentiresample.11Normalsocialsupport(NSS)wasdefined
ashavingaMOS-SSSscoreabovethe25thpercentileofthe
entiresampleaccordingtoShinetal.(2008).11,16
Functionality was evaluated using the Brazilian version
of the Fibromyalgia Impact Questionnaire (FIQ), a
self-administeredquestionnairethatmeasuresfunctionalaspects
ofthepatientoverthepreviousfewweeks.18Itcontainsthree
Likertscaletypequestions(levelsofresponse)andsevenvisual
analogquestions.Allthescalesvaryfrom1to10andahigh
scoreindicatesnegativeimpactandmoreseveresymptoms.
The totalFIQ scoreisgraded from 1 to100 points. Higher
scoreswererelatedtogreaterimpactofthediseaseonpatient
functionalityandacorrespondingreductionintheirqualityof
life.
DepressionlevelswereassessedusingtheBeckDepression
Inventory(BDI), aself-reporting toolcomposedof21
ques-tionsrelatedtocognitivesymptomsandattitudes.19Foreach
question,patientsmustchooseoneormorephrasesthatbest
describehowtheyfeltinthepreviousweek.Themaximum
score is 63 points and high scoresindicate severe
depres-sion.Beck etal.suggestthe followingquantificationscores
fordepression:ascoreoflessthan10indicatesminimalor
nodepression;10–18signifiesmildtomoderatedepression,
19–29moderatetoseveredepressionandfrom30to63severe
depression.19
Theseverityofanxietysymptomswasmeasuredusingthe
HamiltonAnxietyScale(HAS).TheHASwasadministeredby
aninterviewerwho askedaseriesofsemi-structured
ques-tions relatedtosymptomsofanxiety.Theinterviewerthen
ratedtheindividualsonafive-pointscaleforeachofthe14
items.Sevenoftheitemsspecificallyaddresspsychic
anxi-etyandtheremainingsevensomaticanxieties.Thevalueson
the scalerangefromzerotofour:zeromeansthatthereis
noanxiety,oneindicatesmildanxiety,twoindicates
moder-ateanxiety,threeindicatessevereanxiety,andfourindicates
very severe or grossly disabling anxiety. The total anxiety
scorerangesfrom0to56.Highlevelsareindicativeofhigh
anxiety.20
Positiveaffect(PA)andnegativeaffect(NA)weremeasured
usingthePortugueseversionof20-itemPositiveandNegative
AffectSchedule.21Participantswereaskedtoindicateona
5-pointscalefrom1(veryslightlyornotatall)to5(extremely)the
extenttowhichtheyhadexperiencedeachaffectduringthe
pastweek.ThePAscaleincludeditemssuchas“interested,”
“excited,”and“proud,”andtheNAscaleincludeditemssuch
as“distressed,”“nervous,“andirritable”.Thescoresrangeis
10–50forbothpositiveaffectandnegativeaffect.Forpositive
affectscore:addthescoresonitems1,3,5,9,10,12,14,16,17,
and19.Andfornegativeaffectscore:addthescoresonitems
2,4,6,7,8,11,13,15,18,and20.
Algometrywascarriedouttorecordpressurepain
thresh-old(PPTh)andpressurepaintolerance(PPTo).Eighteentender
pointsweremarkedwithademographicpencilandassessed
while patientswere in anupright position, with their feet
slightly apart.Pain sensitivitytestswere performedon the
18pointsidentifiedbyACRinaccordancewithOkifujietal.22
Thiswasdoneperpendiculartotheskinat5–10sintervalsby
thesamequalifiedexaminer.Apressurealgometerwasused
(PainDiagnostics®,NY,EUA),througha1-cmdiameterrubber
tip.Painthresholdandtolerancetopressurewerequantified
inkg/cm2.Theexaminerpositionedtherubbertipabovethe
areatobeexaminedandgraduallyincreasedthepressureby
1kg/cm2/s.ThePPThwasmeasured whenthepatient said
“I’mstartingtofeelpain”.TomeasurePPTo,thepatientwas
asked tobear the maximumamount of pressure from the
algometerandusethephrase“Stop,Icannottakeanymore”
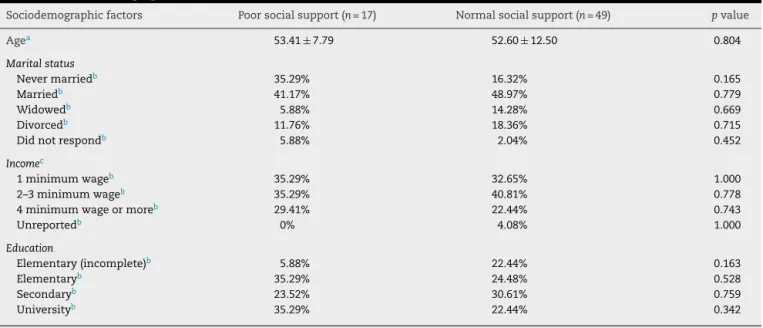
Table1–Sociodemographicvariables.
Sociodemographicfactors Poorsocialsupport(n=17) Normalsocialsupport(n=49) pvalue
Agea 53.41±7.79 52.60±12.50 0.804
Maritalstatus
Nevermarriedb 35.29% 16.32% 0.165
Marriedb 41.17% 48.97% 0.779
Widowedb 5.88% 14.28% 0.669
Divorcedb 11.76% 18.36% 0.715
Didnotrespondb 5.88% 2.04% 0.452
Incomec
1minimumwageb 35.29% 32.65% 1.000
2–3minimumwageb 35.29% 40.81% 0.778
4minimumwageormoreb 29.41% 22.44% 0.743
Unreportedb 0% 4.08% 1.000
Education
Elementary(incomplete)b 5.88% 22.44% 0.163
Elementaryb 35.29% 24.48% 0.528
Secondaryb 23.52% 30.61% 0.759
Universityb 35.29% 22.44% 0.342
Agedescribedwithmeanandstandarddeviation. a Calculatedwithunpairedt-test.
b CalculatedwithFisher’sexacttest.
c Braziliannationalminimumwage,US$252.14permonth.
tousetheseexactsentencesfortotalstandardizationofthe
test.
Statisticaltreatment
Statistical analyses were developed using SPSS 19.0 and
GraphPadPrism5(GraphPadSoftwareInc.,2009).Thefirststep
ofstatisticalanalysiswastotestthenormalpatternsusing
theShapiro–Wilktest.Thecharacteristicsofthesubjectsin
thePSSandNSSgroupswerecomparedusingMann–Whitney
orunpairedt-testandthe Fisher’sexacttestforcategorical
variables.Analysisofcovariance(ANCOVA)wasusedto
com-paretheclinicalcharacteristicsofthesubjectsinthePSSand
NSSgroups.ItwasusedPearsontestforcorrelationbetween
MOS-SSSandFMclinicalvariablesinPSSgroup.Thep-value
consideredwas≤0.05forstatisticallysignificantresults.
Results
Table1showsthedemographiccharacteristicsforboth
par-ticipantsgroups.Nosignificantdifferenceinageandothers
sociodemographic factors was found between two groups.
Table2describesthe comparisonofMOS-SSSand
subcate-goriesstatusbetweentheNSSgroupandthePSSgroup.
UsingANCOVAadjustedforagetoshowtheinfluenceof
PSS onclinical characteristics ofFMpatients, asignificant
influencein depressivestate (p=0.007), negative affectivity
(p=0.025)andPPTh(p=0.016)wasfound.Atendencyto
dif-ferencesbetweenPSSgroupandNSSgroupinFIQ(p=0.094)
withhigherscoresinthePSSgroupthan intheNSSgroup
(Figs. 1 and 2) was observed. For PSS (MOS-SSS score <25
percentile),the affectionate supportsubcategory showed a
significant positive correlation with PA (p=0.010; r=0.61),
PPTh (p=0.040; r=0.5) and PPTo (p=0.020; r=0.54) (Fig. 3).
0 20 40 60 80
NSS PSS
FIQ BDI HAS PA NA
*
*
Score
Fig.1–Influenceofpoorsocialsupport(PSS)ontheclinical characteristicsofpatientswithFM.*p<0.05,byANCOVA
adjustingage.NSS,normalsocialsupport;MOS-SSS, MedicalOutcomesStudySocialSupportSurveyscore<25 percentileforPSS;FIQ,FibromyalgiaImpactQuestionnaire; BDI,BeckDepressionInventory;HAS,HamiltonAnxiety Scale;PA,positiveaffect;NA,negativeaffect.
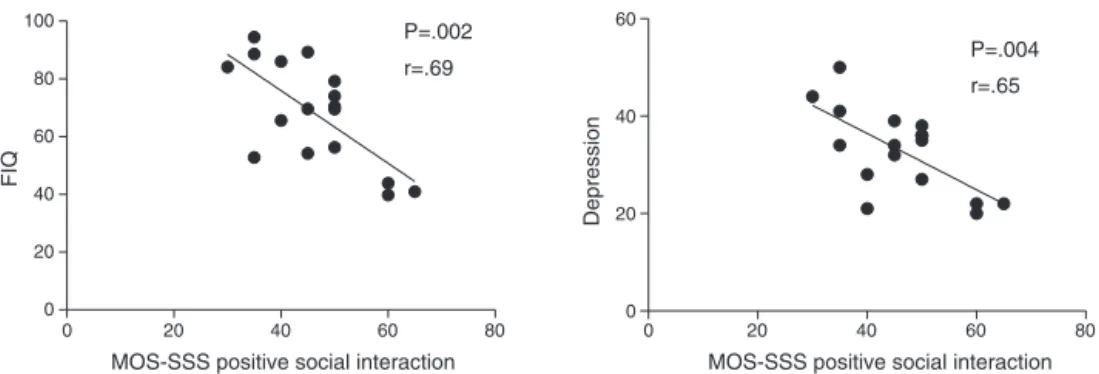
Furthermore,positivesocialinteractionsubcategoryshowed
asignificantnegativecorrelationwithFIQ(p=0.002;r=0.69)
anddepression(p=0.004;r=0.65)(Fig.4).
Discussion
Thepurposeofthisstudywastoassesstheinfluenceofsocial
support on peripheralpain, functionalityand positive and
negativemoodstates,suchasdepression,anxietyand
affec-tivityinBrazilianwomenwithFM.Theemotional/information
Table2–Comparisonofsocialsupportstatusbetweenthenormalsocialsupport(NSS)groupandthepoorsocialsupport
(PSS)group.a
ClinicalVariables Poorsocialsupport(n=17) Normalsocialsupport(n=49) pvalue
Median 75% 25% Median 75% 25%
MOS-SSS
Overall 51.5 54.95 45.83 85.83 93.75 71 <0.0001
Tangible 45 65 35 90 100 75 <0.0001
Affectionate 66 73 46.6 100 100 86 <0.0001
Positivesocialinteraction 45 50 37.5 80 92.5 60 <0.0001
Emotional/Information 42 51 36 85 95 62.5 <0.0001
CalculatedwithMann–Whitneynonparametrictest.Significantat5%.
a MedicalOutcomeStudySocialSupportSurvey(MOS-SSS)score<25percentile.
0 2 4 6
PPTh PPTo
*
Pressure (kg/cm
2)
NSS PSS
Fig.2–Influenceofpoorsocialsupport(PSS)onpressure painthreshold(PPTh)andpressurepaintolerance(PPTo). *p<0.05byANCOVAadjustingage.NSS,normalsocial
support;PSS,poorsocialsupportwithMOS-SSSscore<25 percentileforPSS.Pressurepaininkg/cm2.
expression, advice and guidance.23 Positive social
interac-tionsubcategoryinvolves sharingpleasurableactivities,the
affectionatesupportcategoryinvolvestheexpressionoflove
and tangible supportincludes materialaid and behavioral
assistance.23
Thestudyshowednodifferencesinsociodemographic
vari-ablesbetweenPSSandNSS.Nevertheless,differencesbetween
theNSSgroupandthePSSgroupwerefoundinthepatient
scoresinall4subcategoriesofsocialsupportandinthe
MOS-SSS total score. Apparently, with the same marital status,
incomeandeducationlevelitispossibletofindtwocategories
ofsocialsupportinFMwomen.ThesymptomsofFMcouldbe
moreimportantfactor?Ortheperceivedsocialsupportwas
alteredinFM?
TheresultsdemonstratedifferencesbetweenNSSandPSS
ondepression,negativeaffectandpainsensitivity.
Affection-atesubcategoryshowedpositivecorrelationbetweenpainand
positiveaffectinPSS.Furthermore,positivesocialinteraction
subcategoryshowedanegativecorrelationbetweenFIQand
depressionstate.
These findings are consistent withprevious research in
South Korea and USA, demonstrating that social support
is associated with lower levels of functionality and mood
0 20 40 60 80 100
15 20 25 30 35 40
MOS-SSS affectionate
MOS-SSS affectionate
MOS-SSS affectionate
Positive affect
0 20 40 60 80 100
0 1 2 3 4
Pain threshold
0 20 40 60 80 100
0 1 2 3 4 5
Pain tolerance
P=.01
r=.61
P=.04
r=.5
P=.02
r=.54
Fig.3–Pearsoncorrelationbetweenaffectionateand clinicalvariables.MedicalOutcomeStudySocialSupport Survey(MOS-SSS)score<25percentile.
states.11,18 In addition, there was also evidenced that FM
patientswithlowpositivesocialinteractionmayhavegreater
depressivesymptomsandlowerfunctionality.24Thiscouldbe
duetonotreceivingadequatesocialsupportandbeing
stig-matizedand invalidated,whichmightbequitecommonin
0 20 40 60 80 0
20 40 60 80 100
MOS-SSS positive social interaction MOS-SSS positive social interaction
FIQ
0 20 40 60 80
0 20 40 60
Depression
P=.002
r=.69 P=.004
r=.65
Fig.4–Pearsoncorrelationbetweenpositivesocialinteractionandclinicalvariables.MedicalOutcomeStudySocialSupport Survey(MOS-SSS)score<25percentile.
AnumberofstudieshavedescribedtheimpactofFMon
patientfunctionality,disabilityand qualityoflife.5,6
Study-ing the psychosocial profileofwomen withFMin Toronto
(Canada),Shusteretal.showedthatthesewomenreported
lessperceivedfamilysupportandlowermoodthancontrols.26
Theyalsofoundcorrelationsamongthesevariableswhenthey
wereexaminedwithintheFMgroup,andasignificant
associ-ationwasfound,withhigherratingsofanxietyanddepressed
mood.Theseresultssuggestthatperceivedfamilysupportby
womenwithFMmayhaveanimportantimpactontheirhealth
outcomes,andthatcomplementarytreatmentssuchas
phys-icaltherapymayconsiderablyimprovethequalityoflifeof
patientswithFM.26
In a study of patients with FM, rheumatoid arthritis,
ankylosingspondylitisandosteoarthritis,socialsupportwas
positivelyassociatedwithpatients’mentalbutnotphysical
health.26,27Thepresentstudyshowedanassociationbetween
physicalandmoodstateswithsocialaspects.Thissuggests
thatforimprovinghealthofpatientswithrheumaticdiseases
suchasFMsocialsupporttoenhanceemotionalstatusand
functionalityseemstoberequired.27
Higherratingsofdepressionandanxietyinwomenwith
FMare related tofactors other than maladaptivecognitive
schemas,suchasreducedabilitytoparticipateinenjoyable
activitiesandlackofsleepduetopain.28Supportingthisidea,
Cannellaetal.foundthatinterferencewithimportantdaily
activitiesmediatedtheassociationbetweenpainseverityand
depressedmood.28 Theseinfluencescouldbeanimportant
factortodescribetheinteractionbetweensymptomsand
per-ceptionofsocialsupport.
According to the social support theory, receiving
sup-port from others is generally beneficial to mental and
physicalhealthandmayblunttheharmfulimpactof
exter-nal stressors.29 Empirical confirmation of this buffering
hypothesisofsocialsupporthasbeenobtained.30 However,
invalidation caused by reduced physicalperformance may
be harmful for reasons other than lack of social support.
Invalidation includesan active component of social
rejec-tion,whichhasbeensuggestedtoamplifypain,e.g.,through
activationofneuralstructuressuchastheanteriorcingulate
cortex.31,32
It has been hypothesized that the presence of social
support may diminish one’s appraisal of threat, which in
turn might influenceone’s experience of pain byreducing
positiveandnegativeemotionssuchasdepression,affectivity
oranxiety.26,30,33Anotherplausibleexplanationforthe
bene-ficialeffectofthepresenceofsignificantsocialsupportisthat
the presenceofasupportivepersonhelpsdistractpatients
fromtheirexperienceofphysicalandmooddysfunction.26In
thisstudyitwasfoundacorrelationbetweenaffectionateand
positivesocialinteractionwithpainandmoodstates.Thus,
socialsupportislikelyapredictorofpaininthepopulationof
thisstudy.
Thestudyprovidedsupportfortherelationshipbetween
social support with mood and physical symptoms in FM
women.Thecurrentfindingsplayanimportantrolein
devel-oping comprehensive treatment that addressesthe variety
ofpsychologicalsymptomsassociatedwithFM.Thepresent
researchsupportsthecomprehensivebiopsychosocialmodel,
wherethephysiologyofemotionprovidesakeylinkbetween
mentalstatesandphysicaldisease.Therelationshipbetween
emotions and physical symptoms likely accounts for the
manyfactorsthatcontributedtodiseaseprogression.34The
findings suggest importantinterrelations amongbiological,
psychological,andsocialsystemsthatinfluencehealthand
diseaseprocessesinFM.Therefore,interventionsandefforts
toimprovesocialsupportforFMpatientsseemstobeacrucial
componenttobeincludedinthepracticetoimprovehealth
qualityforthispopulation.
Conclusion
FM women showed two different profiles according the
perceived social support, independently of marital status,
incomeandeducationlevel.PSSgroupshowedmore
depres-sive, negative affectivity state and pain than NSS. Social
Supportappearstocontributetomentalandphysicalhealth
inFMpatientsandtheperceptionofPSSmightbeinfluence
bysymptomsseverity.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. ClauwDJ.Fibromyalgia:anoverview.AmJMed.2009;12212 Suppl.:S3–13.
2. BennettRM,JonesJ,TurkDC,RussellIJ,MatallanaL.An internetsurveyof2,596peoplewithfibromyalgia.BMC MusculoskeletDisord.2007;9:8–27.
3. CavalcanteAB,SauerJF,ChalotSD,Assumpc¸ãoA,LageLV, MatsutaniLA,etal.Theprevalenceoffibromyalgia:a literaturereview.RevBrasReumatol.2006;46:40–8.
4. WhiteKP,SpeechleyM,HarthM,OstbyeT.Comparing self-reportedfunctionandworkdisabilityin100community casesoffibromyalgia.BMCPublicHealth.2012;12.Page6of7.
5. AnnemansL,LeLayK,TaiebC.Societalandpatientburdenof fibromyalgiasyndrome.Pharmacoeconomics.2009;27:547–59.
6. SchoofsN,BambiniD,RonningP,BielakE,WoehlJ.Deathofa lifestyle:theeffectsofsocialsupportandhealthcaresupport onthequalityoflifeofpersonswithfibromyalgiaand/or chronicfatiguesyndrome.OrthopNurs.2004;23:364–74.
7. SteinerJL,BigattiSM,HernandezAM,Lydon-LamJR,Johnston EL.Socialsupportmediatestherelationsbetweenrolestrains andmaritalsatisfactioninhusbandsofpatientswith fibromyalgiasyndrome.FamSystHealth.2010;28:209–23.
8. PhillipsLJ,StuifbergenAK.Therelevanceofdepressive symptomsandsocialsupporttodisabilityinwomenwith multiplesclerosisorfibromyalgia.IntJRehabilRes. 2010;33:142–50.
9. FranksHM,CronanT,OliverK.Socialsupportinwomenwith fibromyalgia:isqualitymoreimportantthanquantity?J CommunityPsychol.2004;32:425–38.
10.OkifujiA,TurkDC,ShermanJJ.Evaluationoftherelationship betweendepressionandfibromyalgiasyndrome:whyaren’t allpatientsdepressed?JRheumatol.2000;27:212–9.
11.ShinJK,KimKW,ParkJH,LeeJJ,HuhY,LeeSB,etal.Impacts ofpoorsocialsupportongeneralhealthstatusin
community-dwellingKoreanelderly:theresultsfromthe Koreanlongitudinalstudyonhealthandaging.Psychiatry Investig.2008;5:155–62.
12.RoweMA.Theimpactofinternalandexternalresourceson functionaloutcomesinchronicillness.ResNursHealth. 1996;19:485–97.
13.HupceyJE.Clarifyingthesocialsupporttheory-research linkage.JAdvNurs.1998;27:1231–41.
14.OliveiraAJ,LopesCS,deLeonAC,RostilaM,GriepRH, WerneckGL,etal.Socialsupportandleisure-timephysical activity:longitudinalevidencefromtheBrazilianPro-Saude cohortstudy.IntJBehavNutrPhysAct.2011;26:77.
15.WolfeF,SmytheHA,YunusMB,BennettRM,BombardierC, GoldenbergDL,etal.TheAmericanCollegeofRheumatology 1990criteriafortheclassificationoffibromyalgia:reportof themulticentercriteriacommittee.ArthritisRheum. 1990;33:160–72.
16.SherbourneCD,StewartAL.TheMOSsocialsupportsurvey. SocSciMed.1991;38:705–14.
17.GriepRH,ChorD,FaersteinE,WerneckGL,LopesCS. ConstructvalidityoftheMedicalOutcomesStudy’ssocial supportscaleadaptedtoPortugueseinthePro-SaudeStudy. CadSaúdePúblic.2005;21:703–14.
18.MarquesAP,SantosAMB,Assumpc¸ãoA,MatsutaniLA,Lage LV,PereiraCAB.ValidationoftheBrazilianversionofthe FibromyalgiaImpactQuestionnaire(FIQ).RevBrasReumatol. 2006;46:24–31.
19.BeckAT,WardCH,MendelsonM,MockJ,ErbaughJ.An inventoryformeasuringdepression.ArchGenPsychiatry. 1961;4:561–71.
20.HamiltonM.Theassessmentofanxietystatesbyrating.BrJ MedPsychol.1959;32:50–5.
21.GalinhaIC,Pais-RibeiroJL.Contribuic¸ãoparaoestudoda versãoportuguesadaPositiveandNegativeAffectSchedule (Panas):II–Estudopsicométrico.AnálPsicol.2005;2:219–27.
22.OkifujiA,TurkJD,SinclairD,StarzTW,MarcusDA.A standardizedmanualtenderpointsurvey.I.Development anddeterminationofathresholdpointforidentificationof positivetenderpointsinFibromyalgiaSyndrome.J Rheumatol.1997;24:377–83.
23.ShyuYI,TangWR,LiangJ,WengLJ.Psychometrictestingof thesocialsupportsurveyonaTaiwanesesample.NursRes. 2006;55:411–7.
24.MontoyaP,LarbigW,BraunC,PreisslH,BirbaumerN. Influenceofsocialsupportandemotionalcontextonpain processingandmagneticbrainresponsesinfibromyalgia. ArthritisRheum.2004;50:4035–44.
25.KoolMB,GeenenR.Lonelinessinpatientswithrheumatic diseases:thesignificanceofinvalidationandlackofsocial support.JPsychol.2012;146:229–41.
26.ShusterJ,McCormackJ,PillaiRiddellR,ToplakME. Understandingthepsychosocialprofileofwomenwith fibromyalgiasyndrome.PainResManag.2009;14:239–45.
27.KoolMB,vanMiddendorpH,LumleyMA,BijlsmaJW,Geenen R.Socialsupportandinvalidationbyotherscontribute uniquelytotheunderstandingofphysicalandmentalhealth ofpatientswithrheumaticdiseases.JHealthPsychol. 2013;18:86–95.
28.CannellaDTL,LobelM,GlassP,LokshinaI,GrahamJE.Factors associatedwithdepressedmoodinchronicpainpatients:the roleofintrapersonalcopingresources.JPain.2007;8:256–62.
29.CohenS,WillsTA.Stress,socialsupport,andthebuffering hypothesis.PsycholBull.1985;98:310–57.
30.MontoyaP,LarbigW,BraunC,PreisslH,BirbaumerN. Influenceofsocialsupportandemotionalcontextonpain processingandmagneticbrainresponsesinfibromyalgia. ArthritisRheum.2004;50:4035–44.
31.KoolMB,vanMiddendorpH,BoeijeHR,GeenenR.
Understandingthelackofunderstanding:invalidationfrom theperspectiveofthepatientwithfibromyalgia.Arthritis Rheum.2009;61:1650–6.
32.EisenbergerNI,LiebermanMD,WilliamsKD.Doesrejection hurt?AnfMRIstudyofsocialexclusion.Science.
2003;302:290–2.
33.HeinrichsM,BaumgartnerT,KirschbaumC,EhlertU.Social supportandoxytocininteracttosuppresscortisoland subjectiveresponsestopsychosocialstress.BiolPsychiatry. 2003;54:1389–98.