w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
A
randomized
trial
study
on
the
effect
of
amniotic
membrane
graft
on
wound
healing
process
after
anal
fistulotomy
Ghahramani
Leila
a,
Pirayeh
Saeideh
a,
Khazraei
Hajar
a,
Bagher
pour
Ali
a,
Hosseini
Seyed
Vahid
a,
Noorafshan
Ali
b,
Safarpour
Ali
Reza
c,∗,
Mousavi
Laleh
aaShirazUniversityofMedicalSciences,ColorectalResearchCenter,Shiraz,Iran
bShirazUniversityofMedicalSciences,AnatomyDepartment,StereologyResearchCenter,Shiraz,Iran
cShirazUniversityofMedicalSciences,GasteroentrohepatologyResearchCenter,Shiraz,Iran
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19December2016 Accepted27March2017 Availableonline15May2017
Keywords:
Analfistula
Humanamnioticmembrane Woundhealing
Post-operativecomplication
a
b
s
t
r
a
c
t
Objective:Humanamnioticmembrane(HAM)usedasawoundcoverageformorethana century.Theaimofthisstudyistoevaluatetheefficacyofamnioticmembraneonwound healingandreducepost-operativecomplication.
Studydesign: Randomizedclinicaltrialstudy.
Placeanddurationofstudy:SurgeryDepartment,ShahidFaghihiHospital,Shiraz,intheperiod ofbetweenSep.2014andNov.2015.
Methodology:73patientswithanalfistulaweredividedintotwogroups.Thepatientssuffered fromsimpleperianalfistula(lowtype)withoutanypastmedicalhistory.Fistulotomywere performedforallofthemandininterventionalgroupHAMwereappliedasbiologicdressing. Theirwoundhealingimprovementwasevaluatedpost-operativeintwogroups.
Results:From73patientsparticipatedinthestudy,36patientswereincontrolgroupand 37patientswereininterventiongroup.Accordingtotheanalysisofimagestakenfromthe wound,therateofwoundhealingwas67.39%ininterventiongroupand54.51%incontrol group(p<0.001).Discharge,pain,itchingandstoolincontinencywaslowerinintervention group.Analysisofpathologysamplestakenfromthewoundshowednodifferencesbetween twogroups.
Conclusion: HAMapplicationcouldleadtoimprovementofwoundhealingandreduced post-operativecomplications.Inconclusion,HAMmayactasabiologicdressinginthepatients withanalfistula.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](S.A.Reza).
http://dx.doi.org/10.1016/j.jcol.2017.03.006
Ensaio
clínico
randomizado
sobre
o
efeito
do
enxerto
de
membrana
amniótica
sobre
o
processo
de
cicatrizac¸ão
após
fistulotomia
anal
Palavras-chave:
Fístulaanal
Membranaamnióticahumana Cicatrizac¸ãodaferida Complicac¸ãopós-operatória
r
e
s
u
m
o
Objetivo: Membranaamnióticahumana(MAH)temsidousadaparacobrirferidaspormais de um século.Oobjetivodesteestudo éavaliar a eficáciada membranaamniótica na cicatrizac¸ãodeferidasereduzircomplicac¸õespós-operatórias.
Desenhodoestudo: Ensaioclínicorandomizado.
Localedurac¸ãodoestudo: DepartamentodeCirurgia,ShahidFaghihiHospital,Shiraz,Irã, entresetembrode2014anovembrode2015.
Método:73pacientescomfístulaanalforamdivididosemdoisgrupos.Ospacientessofriam defístulaperianalsimples(tipobaixo)semhistóricomédicoprévio.Afistulotomiafoi real-izadaemtodoselesenogrupointervenc¸ão,MAHfoiaplicadacomocurativobiológico.A melhoradacicatrizac¸ãofoiavaliadanoperíodopós-operatórioemdoisgrupos.
Resultados:De73pacientesqueparticiparamdoestudo,36pacienteseramdogrupocontrole e37pacientesdogrupointervenc¸ão.Deacordocomaanálisedasimagensdaferida,ataxa decicatrizac¸ãofoi67,39%nogrupointervenc¸ãoe54,51%nogrupocontrole(p<0,001). Secrec¸ão,dor,pruridoeincontinênciafecalfoimenornogrupointervenc¸ão.Aanálisedas amostraspatológicasretiradasdaferidanãomostroudiferenc¸asentreosdoisgrupos.
Conclusão: Aaplicac¸ãodeMAHpodelevaràmelhoriadacicatrizac¸ãodeferidasereduziras complicac¸õespós-operatórias.Emconclusão,aMAHpodeatuarcomoumcurativobiológico nospacientescomfístulaanal.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Introduction
Fistula-in-anodiseaseusuallyexistsafteranorectalinfection. Therearemanytreatmentoptionsformanagementofanal fis-tulaswithminimumchanceofincontinenceandrecurrence. Surgicalmanagementshavetoeliminatethesepticfociand anyassociatedepithelizedtracttoavoidrecurrenceand pre-servetheanalsphincterfunction.
Alloftheoptionshavedifferentsuccessrates.Fistulotomy usedintheunderlyingsphinctertissueandisrecommended forlowfistulaswithreportedsuccessratesvaryingfrom29%to 53%.Successrateswithplughavebeencomparableorinferior totheadvancementflap(48–62%).Theflapshouldconsistof thepartoftheinternalsphincterandmucosawithabroad baseofbloodsupplyandshouldbesuturedwithouttension. Thesuccessratecanberaisedbyremovingthe underlying infectedanalglandandcurettingtherestofthetract.1
Setonisalessinvasiveapproachwithminimaldamageto thesphincter.Howeverthediscomfortcausedtothepatient duringthelongtimerequiredforwoundhealingisthemain disadvantageofthisapproach.However,acuttingsetoncan havebetter(upto99%)successrate,itcancausesevere dis-comforttothepatientandalso,canhave18–25%incidence ofincontinence.Drainingsetoncanhave20–40%persistent fistularate,butwithalowincidenceofincontinence.2
In2006,ligationofintersphinctericfistulatract(L.I.F.T.) introducedbyRojanasakulforthefirsttimeasatotal sphinc-tersavingprocedure.3Healingrateafter6–7weeksisusually
rangingfrom 68% to83%.Videoassisted anal fistula treat-ment(VAAFT)describedbyProf.Meinero,thatisdonewith
therigidendoscopeandthetractiscauterized,curettedand theinternalopeningisstapled.4
Cochranedatabasehavedescribedthatnomajordifference wasseenbetweenthevarioustechniquesusedifrecurrence ratesareconcerned.5Thusthereisnosinglemethodthatis
perfect andphysicianhastochoosethesurgerydepending onhis/herexperience,thetypeoffistulaandtheotherlocal conditions.
Manypost-operativecomplicationsarebecauseof dysfunc-tionofwoundhealing.Vascularityofanalcanalisimportant butthemainreasonisinfectionandlackofscarerecoverydue toscaresituationandhumiddressing.So,complicationslike pain,itching,dischargeandrecurrenceoccurred.
Humanamnioticmembrane(HAM)istheinnerlayerofthe fetalmembranesandhasbio-compatibility,easyavailability, elasticityandstabilityandithasbeenusedasanalternative biomaterialforresearchinmanysurgeriesandwound-healing procedures.Amnioticmembranehasbeenusedindifferent organs forexample, many surgeons evaluated the efficacy ofHAMasabiologicdressinginburnwoundsorincorneal epitheliumreconstructionwithtransplantation ofepithelial cellsonalyophilizedamnioticmembrane(LAM)orin gastroin-testinaltractsurgeries.6,7Manystudiesassessedtheefficacy
ofHAMasabiologic dressinginskinulcers reportedbetter outcomesincomparisontosomeother methods.Moreover, inafewstudies,HAMhasbeenevaluatedinGItractofanimal modelsandthe resultsshowedacceleratingwoundhealing process.8Uludagetal.usedHAMpatchincolon
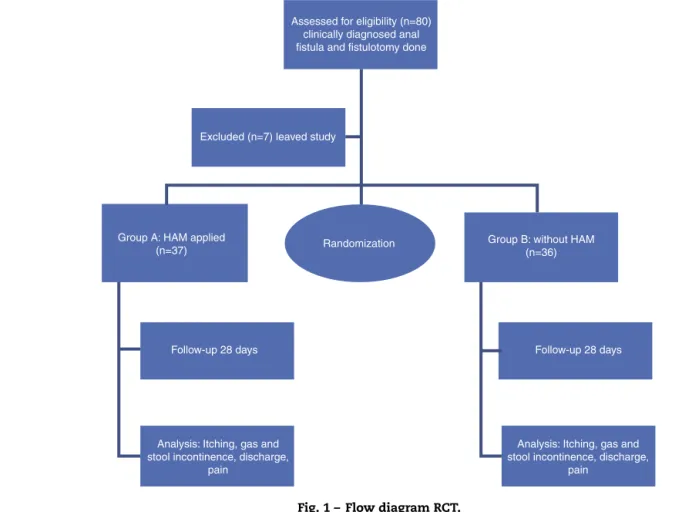
Assessed for eligibility (n=80) clinically diagnosed anal fistula and fistulotomy done
Excluded (n=7) leaved study
Group A: HAM applied
(n=37) Randomization
Group B: without HAM (n=36)
Follow-up 28 days
Analysis: Itching, gas and stool incontinence, discharge,
pain Follow-up 28 days
Analysis: Itching, gas and stool incontinence, discharge,
pain
Fig.1–FlowdiagramRCT.
However,HAMhasbeenputintopracticeforlessthana decadeandmorestudiesareneededforbetterevaluationand theprobablelong-termadverseeffectsofHAMshouldbe eval-uatedinfurtherstudies.Theaimofthisstudywastoevaluate the HAMeffect on woundhealingaccelerationinthe post fistulotomyprocedure.
Methodology
Thestudy hasbeendesignedasarandomizedclinicaltrial toevaluateefficacy ofHAMinhealingoffistulain-Ano.73 patientswithclinicaldiagnosis offistulain-Anowere eval-uated in Shahid Faghihi Hospital of Shiraz University of Medical Sciences between September 2014 and November 2015.Allpatientssufferedlowtypefistulain-Anothatwas confirmedbycolorectalsurgeonwithphysicalexamination andanoscopy.Thepatientwererandomlyallocatedintotwo groups;fistulotomywithmarsupializationandHAMapplying onwoundingroupAandfistulotomywithmarsupialization ingroupBascontrolgroup(standardprocedureforlowtype fistula).
Theinclusioncriteriawereasfollows:clinicaldiagnosisof lowtypefistula(sphincterinvolvement<30%),age18–65years, andAmerican societyofanesthesiologistsclassIorII. The exclusioncriteriaincludedthefollowing;1)immune compro-misedpatientssuchasT.B,AIDSorDMreceivedsteroiddrugs >20mg/day;2) inflammatorybowel disease;3) pastmedical
history ofpreviousanal surgeries;4) historyofgasorstool incontinence;5)allergytoegg;6)refusetoparticipationinthis study;7)BMI>30;8)fistulawithabscess;9)hightypefistula (sphincterinvolvement>30%);10)previous pelvicradiation; 11)perianaldermatitis.
Table1–DemographicdatafrompatientsundersimplesurgeryandHAMwithsurgery(percent).
Group Male Female Meanage±SD
Simplesurgery 31(86.1%) 5(13.9%) 39.94±10.77
SurgerywithHAM 20(54.1%) 17(45.9%) 37.32±10.27
Table2–Discharge,itching,pain,incontinenceparameters.
Parameter p-value Oddsratio 95%confidenceinterval
Lower Upper
Discharge 0.000 2.29 1.53 3.42
Itching 0.000 4.82 2.65 8.78
Pain <0.0001 1.61 1.34 1.93
Fecalincontinence 0.007 – −0.72 −0.11
visitedthepatients3,7,14,21and28thdayspostoperation thathewasblindedtoallocationofthetwogroups.Follow-up dataformwascompletewithattentiontosignandsymptom ofthepatients(Fig.1).Itching,gasandstoolincontinence, dis-charge,painscoringwasdeterminedbyusingVASsystem.In secondvisit(2weekspostoperation),digitalphotographwas takenagaininthesamedistance.Tissuebiopsywastakenof 10patientsinbothgroupsrandomly.Therefore,primary out-comeinthisstudywaswoundhealingaccelerationbyHAM that was evaluated subjectively and objectively. Secondary outcomewasinfectionandabscessformation.Questionforms evaluatedwoundhealingandinfectionsubjectivelyand digi-talphotograph(digitalimage:stereolith),tissuebiopsytaken helped usfor objective evaluation (10 participantsin each group).
ThisstudywasapprovedbytheethicscommitteeofShiraz UniversityofMedicalSciencesand wasregisteredwiththe IranianClinicalTrialRegister(IRCT:201310219936N6).
Statistics
StatisticalanalysiswasperformedbySPSSsoftware(version 16)andalsoSAS(forcategoricalrepeatedmeasurement).In descriptiveanalysisquantitativevariables wererevealed by mean±SD, and qualitative variables were showed by fre-quencyandpercent.Qualitativevariableswerepain,discharge anditching.Quantitativevariablewaspercentofscarrecovery. Theyweremeasuredduringtimesaftersurgery.Repeated measurementanalysis(RMA)wasdoneforevaluationof sig-nificantchangesintheoutcome variables.Qualitative RMA andquantitativeRMAwereperformedbySPSSandSASsoft waresrespectively.Generalizedestimatingequation(GEE)was themethodfordischargeassay.Twosamplest-test,2testand
fisherexactedtestalsowereusesinappropriatecomparisons.
p-valuegreaterthan0.05wasconsideredsignificant.
Results
80patientsevaluatedand7ofpatientsleavethestudy,36of themhadsimplefistulatomy(5femaleand31male)and37 ofpatientshadfistulatomywithHAMgraft(17femaleand20 male).Inthisstudy,meanageofpatientswithsimple fistu-latomywas39.9yearsandmeanageofpatientswithHAM was37.3yearswithnosignificantdifference(Table1).
Inthisstudy,variableslikesex,age,historyoffissurebefore surgery,timeandtypeofsurgeryandtheireffectsondischarge assayed(Table2).Timeanddischargehadsignificant differ-ence(p=0.003),thatmeansincreaseoftimedecreasechance ofdischarge(OR=0.96).Also,surgerywithHAMincomparison withsimplefistulatomydecreasechanceofdischargemore thantwotimes(OR=2.29).Sex,ageandfissuredidnothave significantdifferenceandshowedthattwogroupswereequal assexandage.
Itchingandfissurebeforesurgery,typeofsurgeryandtime hadsignificantdifference.GEEresultsinitchingshowed sig-nificantdifferenceintime(p=0.004)andbyincreaseoftime, chanceoflackofitchingincreased(OR=1.04).Therewas sig-nificant differencebetweentwogroups foritching(p<0.05) and chance oflackofitchingin group1was morethan 4 timesofgroupzero(OR=4.82).Fissureinclinicalexambefore surgeryaffectsitchingsignificantly(p<0.05).Chanceoflackof itchinginpatientswithfissurewaslowerthanpatients with-outfissure(OR=0.17).Sexandagedidnotshowanydifference onitching(p=0.421,p=0.07),respectively.
ForAnalysisthedataforPainSASsoftwareusedandGEE marginal modeling method showed that time significantly affected(p<0.05)andbyspendingmoretimechanceoflack ofpainincreased(OR=2.14).Twogroupsdemonstrated signif-icantdifferenceinpain(p<0.05)andchanceoflackofpainin groupzerowaslessthangroup1(OR=0.47).So,surgerywith HAM suggestedasbettersurgeryincomparisontoanother surgery.Sexandagedidnotshowanydifferenceonpain.
Percentofhealing
Accordingtothephotographicdataindayofsurgeryand14 days afterthat,percentofscarerecoveryobtainedby digi-talimageanalysis.Mean±SDofpercentofrecoveryingroup without HAMwas54.51±4.86andingroupthatusedHAM graftwas67.39±4.69.Thedifferencebetweentwogroupswas significant(p<0.0001)thatmeansuseofHAMincreasedrate ofscarerecovery.
Fecalincontinenceparameter
Pathology
Mann–Whitneytestusedforcomparisonbetweentwogroups and there was no significant difference between them as pathologicdata(p-value=0.76).
Discussion
Usually 70.7% offistulas were healed in atleast 1 year of follow-up.Fistula-in-anoisachallengingconditionto man-agedespitethetechnological advancesandit isnotagold standardtreatmentalgorithmforit.Lowtranssphincteric fis-tulasaretreatedbyfistulotomysuccessfullywhilecomplex fistulas are managed by advancement flap repair, cutting seton,partialfistulotomy,stemcellinjection,fibrinordermal collagenglueinjection,plug,VAAFT,LIFT,andFiLaC,but evi-denceonhealing,recurrence,andsafetyoftheseoptionsisnot clarifiedcompletely.Astudyonanalfistulaisneededtodefine kindoffistula(low,high,transsphincteric, intersphincteric) andoutcomemeasures(healingtime,incontinence).
Humanamnioticmembrane(HAM)hasbio-compatibility, easyavailability,elasticityandstabilitythatresearchershave encouragedtoconsideritasabiologicdressingand appro-priatebio-prosthesisformorethan100years.Manysurgeons examinedtheefficacyofHAMasabiologicdressingintheir treatment methods such as burn wounds treatment or in gastrointestinaltractsurgeriesanddesirableoutcomeswere reported.6 Amnion cells synthesize peptides of the innate
immunitysystem,likeasbeta-defensins,elastase-inhibitors, elafin, lactoferrin,or IL-1-RA.HAM had antimicrobialeffect duetotheseimmunefactors.Also,HAMsynthesizes numer-ous growth factors such as epithelial growth factor (EGF), humangrowthfactor(HGF),keratinocytegrowthfactor(KGF), basicfibroblastgrowthfactor(bFGF),andtissuegrowth fac-tors(TGF-alpha,TGF-beta-1,TGF-beta-2,andTGF-beta-3)and expectedtoacceleratereepithelializationandwound-healing by the activation of keratinocytes.10 Collagen type IV and
lamininaremainlycompositionsofbasementmembraneand ispivotalforcoherencebetweendermallayersandthe epithe-lial.
OurfindingsshowedthatrepairinganalfistulawithHAM resultsinbetteroutcomecomparedtosimplerepair.Thisisin concordancewiththeresultsofotherstudieswhichreported theapplicationofHAMinrepairingrecto-vaginalfistulas.6
Westandardizedhistologicfindings byusingamodified scoringsystemandprovideaquantitativecomparative con-text.Althoughquantitativeassessmentofanalfistulahealing processischallenging,webelieveitwouldhelpresearchers formoreaccuratecomparison.
Manysurgicalapproachesfordecreasehealingtimeused suchas:Fistulotomywith8.3%minorincontinenceand8.3% recurrencerate,11Advancementflapwith29%incontinence
and10% recurrence,12 YorkMasonapproach,13 Seton,Plug,
fibringlue14orStemcellinjectionwithcomplex(highor
trans-sphincteric)analfistulae.
Accordingtoourknowledge,thisstudyisfirststudyto eval-uatetheeffectofHAMonwoundhealingpostfistulotomy. ThemainpositivepointseemscomparisonofHAMeffectby quantitativeandqualitativemeasurement.
Conclusion
Though the anal fistula istroublesome to the surgeons, it seemsbeimprovedbyusingtheHAMgraft.Ourresultsseemto demonstratethatthistechniqueisbothsimpleandeffective andwouldresultinbettersurgicalandhistologicaloutcomes comparingtosimplerepair.HAMincreasedrateofrecovery anditsuggestedthatHAMcouldbeusedforfurtherresearch onpatients’treatment.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ThisarticlewasextractedfromthethesisofDr.Pirayeh,no. 5180,andapprovedbytheresearchvice-chancellorofShiraz UniversityofMedicalSciences.Hereby,theauthorswouldlike tothankthisvice-chancelleryforfinanciallysupportingthe study.
r
e
f
e
r
e
n
c
e
s
1.MushayaC,BartlettL,SchulzeB,HoYH.Ligationof
intersphinctericfistulatractcomparedwithadvancement
flapfor.AmJSurg.2012;204:283–9.
2.Galis-RozenE,TulchinskyH,RosenA,EldarS,RabauM,
StepanskiA,etal.Long-termoutcomeofloosesetonfor
complexanalfistula:atwo-centrestudyofpatientswithand
withoutCrohn’sdisease.ColorectalDis.2010;12:358–62.
3.RojanasakulA.LIFTprocedure:asimplifiedtechniquefor
fistula-in-ano.TechColoproctol.2009;13:237–40.
4.MeineroP,MoriL.Video-assistedanalfistulatreatment
(VAAFT):anovelsphincter-savingprocedurefortreating
complexanalfistulas.TechColoproctol.2011;15:417–22.
5.JacobTJ,PerakathB,KeighleyMR.Surgicalinterventionfor
anorectalfistula.CochraneDatabaseSystRev.2010;12.
CD006319.
6.RoshanravanR,GhahramaniL,HosseinzadehM,
MohammadipourM,MoslemiS,RezaianzadehA,etal.Anew
methodtorepairrecto-vaginalfistula:Useofhumanamniotic
membraneinananimalmodel.AdvBiomedRes.2014;3:114.
7.AhnJI,LeeDH,RyuYH,JangIK,YoonMY,ShinYH,etal.
Reconstructionofrabbitcornealepitheliumonlyophilized
amnioticmembraneusingthetiltingdynamicculture
method.ArtificialOrgans.2007;31:711–21.
8.GhahramaniL,JahromiAB,DehghaniMR,AshrafMJ,
RahimikazerooniS,RezaianzadehA,etal.Evaluationofrepair
induodenalperforationwithhumanamnioticmembrane:an
animalmodel(dog).AdvBiomedRes.2014;17:113.
9.UludagM,CitgezB,OzkayaO,YetkinG,OzcanO,PolatN,
etal.Effectsofamnioticmembraneonthehealingofprimary
colonicanastomosesinthececalligationandpuncture
modelofsecondaryperitonitisinrats.IntJColorectalDis.
2009;24:559–67.
10.LoeffelbeinDJ,RohlederNH,EddicksM,BaumannCM,
StoeckelhuberM,WolffKD,etal.Evaluationofhuman
amnioticmembraneasawounddressingforsplit-thickness
skin-graftdonorsites.BioMedResInt.2014:572183.
11.PescatoriM,AyabacaSM,CafaroD,IannelloA,MagriniS.
improveshealinganddecreasesbleeding:arandomized
controlledtrial.ColorectalDis.2006;8:11–4.
12.PerezF,ArroyoA,SerranoP,CandelaF,PerezMT,CalpenaR.
Prospectiveclinicalandmanometricstudyoffistulotomy
withprimarysphincterreconstructioninthemanagementof
recurrentcomplexfistula-in-ano.IntJColorectalDis.
2006;21:522–6.
13.CadedduF,SalisF,LisiG,CiangolaI,MilitoG.Complexanal
fistularemainsachallengeforcolorectalsurgeon.IntJ
ColorectalDis.2015;30:595–603.
14.MalikAI,NelsonRL.Surgicalmanagementofanalfistulae:a