CEREBROVASCULAR DISEASE IN PEDIATRIC PATIENTS
New ra Tellechea Rot t a
1, Alexandre Rodrigues da Silva
2, Flora Luciana Figueira da Silva
3,
Lygia Ohlw eiler
4, Eraldo Belarmino Jr
2, Valéria Raimundo Font eles
3, Josiane Ranzan
3,
Orlando Javier Ramos Rodriguez
3, Régis Osório M art ins
3ABSTRACT - Alt hough rare in childhood, st roke may have a serious impact w hen it happens in t his st age of life. Also, it may be t he first sign of a syst emic disease. We report 12 cases of pat ient s w it h st roke t reat ed in t he Neuropediat rics Unit of Hospit al de Clínicas de Port o Alegre (HCPA) from M arch 1997 t o M arch 2000. All pat ient s, from t erm infant s t o 12-year-old children hospit alized in t he Pediat rics Unit of HCPA, had clinical suspicion of st roke, w hich w as lat er confirmed by radiological st udies. Pat ient follow up ranged from 1 t o 6 years (mean = 3.4 years). Present ing sympt oms w ere hemiparesis in 9 pat ient s, seizures in 7, deviat ion of labial commissure in 3, and loss of consciousness in 1. The increase in t he number of cases of childhood st roke ident ified and lat er confirmed by noninvasive met hods had helped in t he det erminat ion of different et hiologies of st roke: t he most frequent being hemat ologic, cardiac and genet ic diseases. How ever, our st udy included 6 new borns w it h st roke w hose et hiology w as not ident ified. Seven children w it h seizures received phenobarbit al. Six t erm infant s had neonat al seizures secondary t o st roke and rest rict ed t o t he first 72 hours of life.
KEY WORDS: cerebrovascular disease, st roke, children.
Doença cerebrovascular em pacientes pediátricos
RESUM O - Doença cerebrovascular isquêmica (DCVI) é rara na infância, mas quando ocorre, o impact o pode ser muit o sério. Pode ser a primeira manifest ação de uma doença sist êmica. Relat amos a ocorrência de 12 casos de DCVI. Foram diagnost icados e t rat ados no Hospit al de Clínicas de Port o Alegre (HCPA) na Unidade de Neuropediat ria de março de 1997 a março de 2000. Todos os casos com suspeit a clínica de DCVI foram confirmados por avaliação radiológica de recém-nascidos de t ermo (RNT) a crianças at é 12 anos de idade, que int ernaram na Unidade de Pediat ria do HCPA. Eles foram acompanhados de um a seis anos (média 3,4 anos). Os sint omas iniciais foram: hemiparesia em 9 pacient es, convulsões em 7, desvio da comissura labial em 3 e perda da consciência em um. O aument o do reconheciment o de DCVI em crianças, auxiliado pela confirmação do diagnóst ico at ravés de exames não invasivos, t em auxiliado na ident ificação da et iologia. As et iologias mais frequent es foram doenças hemat ológicas, cardíacas e genét icas. Cont udo, nosso est udo most rou 6 recém -nascidos com DCVI em que não f oi ident if icada et iologia. Set e crianças com convulsões usaram fenobarbit al. Em seis RNT com DCVI as convulsões est iveram rest rit as às primeiras 72 horas de vida.
PALAVRAS-CHAVE: doença cerebrovascular aguda, infância, AVC isquêmico.
Pediat ric Neurology Unit , Hospit al de Clínicas de Port o Alegre, and Universidade Federal do Rio Grande do Sul (UFRS), Port o Alegre RS, Brazil: 1Head of Pediat ric Neurology Unit , Associat e Professor of Pediat rics, UFRS; 2M edical Resident;3M edical Student; 4Pediat ric Neurologist .
Received 16 November 2001, received in final form 13 June 2002. Accept ed 21 June 2002.
Dr. New ra Tellechea Rot t a - Rua Luiz M anoel Gonzaga 650 - 90470-280 Port o Alegre RS - Brazil.
Although rare in childhood, stroke may have a very serious impact and it may also be the first sign of systemic disease. Although its etiology may often be obscure, investigation must be as thorough as pos-sible, not only to identify its cause, but also to esti-mate the risk of recurrence and to establish prognosis and adequate therapy1. The incidence of stroke in the pediat ric populat ion is of 2-3 cases per 100 000 children per year2, w hich is 20 times low er than the incidence among 45- to 54-year-old adults.
Five fact ors should be considered in t he pat ho-physiology of st roke in childhood: cerebral blood
flow, endot helial fact ors, serum prot ein, plat elet s, and prostaglandins3. The most common predisposing fact ors are: cardiopat hy4, vasculit is5, complicat ions of cancer treatment6, vascular thrombosis7, and intra-cranial vascular malformat ions7. Ot her risk fact ors can also be involved in the onset of the disease: gene-t ic predisposigene-t ion, gene-t rauma, infecgene-t ion, and nugene-t rigene-t ional deficiencies8-10.
960 Arq Neuropsiquiat r 2002;60(4)
long list of genet ic fact ors t hat predispose t o st roke in childhood, t he full breadt h of t his int eract ion has not been accurat ely explained yet . There is a link bet -w een human leukocyt e ant igen B51 and st roke in childhood. M oyamoya disease seems t o be linked t o markers on chromosome 3p. Williams syndrome sult s from a mut at ion on chromosome 7q in t he re-gion t hat includes t he elast in gene7.
The HIV-infect ion diagnosis must be considered w hen focal neurologic sympt oms are observed in t he pediat ric populat ion11,12, since st roke and seizures in childhood may be t he first HIV-infect ion manifest a-t ion13. Necropsy invest igat ions of HIV-infect ed chil-dren have revealed ischemic infarct ion of t he t hala-mus, hypot halamus or int ernal capsule13.
Sickle cell anemia is a st rong risk fact or for st roke secondary t o t he development of st enosis in t he mid-dle cerebral and int ernal carot id art eries14. Clinically and radiologically conf irm ed st enosis, associat ed w it h hemat ocrit < 20% and plat elet s < 500 000, is an independent risk f act or f or cognit ive im pair-ment15. Therefore, t herapy should be st art ed early t o prevent neurological disabilit ies caused by st roke4. Hyd roxyurea, a d rug cap ab le of d ecreasing t he number of plat elet s and increasing hemat ocrit , has been used t o prevent lesions15,16.
The int elligence quot ient (IQ) of children w it h di-sabilit ies caused by st roke is in t he normal range, but is significant ly low er t han t he IQ for t he general population17. There is no evidence of gender differen-ces in cognit ive recovery. This st udy, how ever, does not discuss t he lat eralizat ion of cerebral funct ion and t he applicat ion of different IQ scales18. Abnormal findings on convent ional angiography or magnet ic resonance imaging are observed for about 80% of children w it h st roke14, but longit udinal st udies have show n t hat 25-50% of t he children w it h abnormal
findings on init ial cerebral angiography have normal angiogram s at f ollow -up19. Several st udies20 have report ed ext remely favorable prognosis for st roke in t erm infant s, and only one has report ed focal sei-zures and apnea – also observed in ot her age gro-ups10 - rest rict ed t o t he first t hree days of life9.
St roke is less frequent in children t han in adult s. How ever, t he large num ber of possible et iologies suggest s t hat t his disease is underdiagnosed. St roke in children may indicat e t he presence of concomit ant diseases, such as sickle cell anemia and AIDS2-6,13,15,16. This st udy report s 12 cases of st roke in pat ient s t reat ed in t he Neuropediat rics Unit of Hospit al de Clínicas de Port o Alegre (HCPA) from M arch 1997 t o M arch 2000.
M ETHOD
Pat ient s w it h st roke w ere prospect ively follow ed up at t he out pat ient service of t he Neuropediat rics Unit of HCPA from M arch 1997 t o M arch 2000. Inclusion crit eria: chil-dren younger t han 12 years of age, clinically suspect ed of st roke lat er confirmed by radiological st udies, t reat ed in t he Pediat rics Unit of HCPA, and w hose parent s signed t he informed consent document . Exclusion crit eria: all pa-t ienpa-t s for w hom radiological findings had nopa-t confirmed st roke. We st udied t he follow ing variables: race, sex, age at onset of sympt oms and at t he t ime of diagnosis, pre-sence of neurological cognit ive disabilit y, concom it ant di-sease, brain CT and EEG findings. IQ of pat ient s under t he age of 5 w as measured w it h t he WIPSI t est . For 3 ot her pat ient s, w e used t he WISC t est21. The SPSS and Epi Info
6.04 soft w are w ere used for st at ist ical analyses.This st udy w as approved by t he Scient ific and Et hics Commit t ee of HCPA under t he number 00.304.
RESULTS
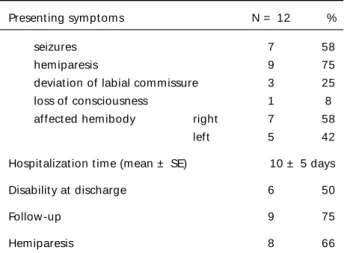
Of t he 12 pat ient s w it h st roke, 11 w ere w hit e and 7 w ere boys. Six w ere t erm new borns at t he onset of sympt oms. The ot hers w ere 9 mont hs t o 6 years old w hen st roke occurred. Hemiparesis w as ob-served in 9 pat ient s, seizures in 7, deviat ion of labial commissure in 3, and loss of consciousness in one. The right hemibody w as affect ed in 7 pat ient s, and t he left in 5. M ean hospit alizat ion t ime w as 10 days. Half of t he pat ient s show ed some disabilit y at hos-pit al discharge (Table 1).
The middle cerebral art ery t errit ory w as affect ed in all pat ient s, and radiological signs of cerebral at rophy w ere found on brain CT of 4 pat ient s. One new -born had cerebral at rophy; five pat ient s underw ent repeat brain CT at least one year aft er t he st roke, and f indings show ed a reduct ion of t he involved area; in 2 patients, diffuse cortical atrophy w as obser-ved in comparison w it h previous brain CT findings.
Table 1. Clinical f indings.
Present ing sympt oms N = 12 %
seizures 7 58
hemiparesis 9 75
deviat ion of labial commissure 3 25
loss of consciousness 1 8
affect ed hemibody right 7 58
left 5 42
Hospit alizat ion t ime (mean ± SE) 10 ± 5 days
Disabilit y at discharge 6 50
Follow -up 9 75
Hemiparesis 8 66
observed in 100% of t he older children and absent in new borns (p= .001); predominance of damage t o
t he right hemisphere w as higher in older children
(p= .03) (Table 3).
DISCUSSION
Cerebrovascular disease in children is less frequent than in adults, and it is underdiagnosed because phy-sicians do not usually include it in different ial
diag-Fig 1. CT. Pacient 1 - Lef t midle cerebral art ery t errit ory involved. Fig 2. CT. Pacient 4 - Lef t midle cerebral art ery t errit ory involved.
Tw o pat ient s show ed concomit ant hemiparesis and t heir IQ scores w ere low er (below 79) in bot h Per-formance and Verbal IQ t est s (Figs 1, 2, and 3). There w ere no signs of cerebral at rophy on brain CT for t he ot her 3 pat ient s, w ho st ill had hemiparesis but w hose IQ scores w ere normal.
EEG findings w ere recorded for all pat ient s, and 10 show ed a correlat ion w it h brain CT findings. Nine patients show ed some type of disability at outpatient follow -up: t he most frequent being hemiparesis (8 pat ient s), w it h right side involvement in 7 pat ient s (Table 1). Half of t hem had a concomit ant disease t hat may have been t he cause of st roke: congenit al cardiopathy in 2 patients, sickle cell anemia in 1, AIDS in 1, acut e lymphoblast ic leukemia in 1, and delet ion of long arm of chromosome 18 (18q - 21.3) in 1. Laborat ory and radiological invest igat ions, careful clinical hist ory, and physical exam inat ion did not reveal any underlying et iology f or t he ot her six pat ient s (all t erm new borns) (Table 2).
Pat ient s w ere divided int o t w o groups: pat ient s w it h onset of sympt oms in t he neonat al period, and pat ient s w it h onset at 9 mont hs t o 6 years of age. There w ere no st at ist ical differences bet w een t he groups in relat ion t o race, sex, signs of brain at rophy on CT, and correlat ion of EEG and CT findings. Ho-w ever, some significant differences Ho-w ere observed: at diagnosis, hemiparesis w as present in 100% of t he pat ient s in t he older children group and in 33%
962 Arq Neuropsiquiat r 2002;60(4)
Table 2. Descript ion of cases.
Pat ient Race Sex Present ing sympt oms Age at on set Concomit ant disease Disabilit ies 1 black female right hemiparesis 6 years sickle cell anemia right hemiparesis 2 w hit e male right hemiparesis, left deviat ion of labial
commissure and loss of consciousness 3 years 18 - 21.3 right hemiparesis 3 w hit e male right focal seizures 48 hours absent right hemiparesis 4 w hit e male left hemiparesis, right deviat ion of 2 years Tet ralogy of Fallot absent
labial commissure
5 w hit e male seizures in right hemibody 24 hours absent right hemiparesis
6 w hit e male right hemiparesis 48 hours absent right hemiparesis
7 w hit e female right focal seizures 48 hours absent right hemiparesis
8 w hit e male left hemiparesis 2 years AIDS absent
9 w hit e female left hemiparesis and seizures 9 mont hs Noonan’s syndrome absent
10 w hit e male left hemiparesis 6 years ALL left hemiparesis
11 w hit e female right hemiparesis 48 hours absent right hemiparesis
12 w hit e female seizures - right arm 48 hours absent right hemiparesis
ALL, acut e lymphoblast ic leukemia; AIDS, acquired immunodeficiency syndrome; 18-21.3, delet ion of long arm of chromosome 18.
Table 3. Comparison bet w een new borns and children older t han 1 mont h.
New borns Older children Charact erist ics
No. % No. % p
Tot al 6 100 6 100 NS
Race
w hit e 6 100 5 83 NS
black 0 0 1 17
Sex
female 3 50 2 33 NS
male 3 50 4 67
Present ing sympt oms
seizures 4 66 3 50 NS
hemiparesis 2 33 6 100 .03*
Concomit ant disease 0 0 6 100 .001*
Cort ical at rophy 1 17 3 50 NS
Overlapping EEG and CT findings 5 83 5 83 NS Hemiparesis
right 6 100 2 33 .03*
left 0 0 4 67
NS, not significant .
noses. Higher rat es of ident ificat ion of st roke in chil-dren, prom ot ed by conf irm at ion of diagnosis by noninvasive t est s, have helped in t he det erminat ion of et iology. Hemat ologic, cardiac and genet ic
conduct ed in an at t empt t o ident ify ot her et iolo-gies18,19,22.
Some st udies have st ressed t he import ance of suspect ing st roke in HIV-inf ect ed pat ient s w hen neurological focal signs are present13,14. We identified sympt oms of hemiparesis in addit ion t o episodes of focal seizures in one previously healt hy pat ient , w ho had AIDS confirmed at et iologic invest igat ion.
The incidence of seizures associat ed w it h st roke is high in childhood, mainly in t he first t w o years of life, and seizures occur at t he onset of disease in most cases. Cort ical involvement is a risk fact or for t he development of seizures23.
Of our 12 pat ient s, 8 w ere administ ered t he WIPSI t est for children younger t han 5 years, and 3 t ook t he WISC t est . Only 2 children had IQ scores below normal, w hich is in agreement w it h findings in t he lit erat ure21,24-26.
Our clinical f indings f or new borns are also in agreement w ith data in the literature9,22,23: most cases of stroke occur in term babies w ith a high Apgar score, w ho have seizures 24-48 hours after birth; and these patients respond better to the use of anticonvulsants. Our findings stress the importance of considering the hypothesis of stroke in new borns w ith seizures, even in the absence of hypoxic events. M ultiple possible etiologies should be considered: sickle cell anemia, re-ported as the most common etiology; rare conditi-ons, such as chromosomal anomalies; and even a first clinical sign of neuroAIDS in children8,13.
Neuroimaging studies show ed involvement of the middle cerebral art ery in all pat ient s, 66% on t he left side. Cort ical at rophy w as found in 2 pat ient s, exact l y t h o se w h o p r esen t ed w i t h co g n i t i ve impairment at out pat ient follow -up. EEG changes w ere in agreem ent w it h radiological f indings, as report ed in lit erat ure19,22,23.
Acut e onset of focal signs w it h acut e onset in children should alw ays suggest st roke, and act ive invest igat ion may reveal new causes t o be added t o t he list of ot her bet t er know n et iologies13,17,18.
REFERENCES
1. Gherpelli JLD. Afecções vasculares cerebrais In Diament A, Cypel, S (Eds.). Neurologia infantil 3.Ed., São Paulo: Atheneu, 1996:1218-1224. 2. Schoenberg BS, Mellinger JF, Schoenberg DG. Cerebrovascular disease in infants and children: a study of incidence, clinical features, and survival. Neurology 1978; 28:763-768.
3. Shuman RM. The molecular biology of occlusive stroke in childhood. Neurol Clin 1990; 8:553-570.
4. Tyler HR, Clark DB. Cerebro vascular accidents in patients w ith congenital heart disease. Arch Neurol Psychatr 1957;77:483-487. 5. Hess DC, Adams RJ, Nichols FT. Valvular heart disease,
antiphos-pholipid antibodies and stroke. Neurology 1990;40 (Suppl.):354. 6. Packer MJ, Rorke LB, Lange BJ. Cerebrovascular accidents in children
with cancer. Pediatrics 1985;76:194-201.
7. Pavlakis SG, Gould RJ, Zito JL. Stroke in children. Adv Pediatr 1991; 38:151-157.
8. Kirkham FJ, Prengler BC, Hewes DKM, Ganesan V. Risk factors for arterial ischemic stroke in children. J Child Neurol 2000; 15:299-307. 9. Jan MMS, Camfield PR. Outcome of neonatal stroke in full-term infants
without significant birth asphyxia. Eur J Pediatr 1998;157:846-848. 10. Po w ell FC, Hanigan C, McCluney KW. Subco rtical infarctio n in
children. Stroke 1994;25:117-121.
11. Park YD, Belman AL, Kim TS. Stroke in pediatric acquired immunode-ficiency syndrome. Ann Neurol 1990;28:303-311.
12. Nass R, Peterson H, Koch D. Differential effects of congenital left and right brain injury on intelligence. Brain Cogn 1989; 9:258-266. 13. Ro tta NT. A cidente vascular isquêmico na infância. Rev Neuro l
2000;31:221-237
14. Visudtibhan A, Visudtibhan P, Chiemchanya S. Stroke and seizures as the presenting signs of pediatric HIV infection. Pediatr Neurol 1999;20:53-56. 15. Adams RJ. Lessons from the stroke prevention trial in sickle cell anemia
(STOP) study. J Child Neurol 2000;15:344-349.
16. Wang WC, Langston JW, Steen G, et al. Abnormalities of the central nervous system in very young children with sickle cell anemia. J Pediatr 1998;132:994-998.
17. Moura-Ribeiro MVL, Ferreira LS, Montenegro MA , et al. Doença cerebrovascular na infância: aspectos clínicos em 42 casos Arq Neuro-psiquiatr 1999;57:594-598.
18. Riela, AR, Roach ES. Etiology of stroke in children. J Child Neurol 1993; 8:201-220.
19. Ganesan V, Savvy L, Chong WK, et al. Conventional cerebral angiography in children with ischemic stroke. Pediatr Neurol 1999; 20:38-42.
20. Moura-Ribeiro MVL, Pessoto MA, Marba STM. Cerebrovascular disease in neonates. Arq Neuropsiquiatr 1999; 57:84-87.
21. Wechsler D. The Wechsler Preschool and Primary Scales of Intelligence-Revised, Sidcup, UK: Psychological Corporation, 1990.
22. Mercuri E, Rutherford M, Cowan F, et al. Early prognostic indicators of outcome in infants w ith neonatal cerebral infarction: a clinical, electro encephalo gram, and magnetic reso nance imaging stud y. Pediatrics 1999;103:39-46.
23. Montenegro MA, Guerreiro MM, Scotoni AE et al. Doença cerebrovascular na infância: manifestações epilépticas Arq Neuropsiquiatr 1999;57:587-593. 24. Turkheimer E, Farace E, Yeo R, et al. Quantitative analysis of gender differences in the effects of lateralized lesions on verbal and perfor-mance IQ. Intelligence 1993;17:461-474.
25. Bernaudin F, Verlhac S, Fréard F, et al. Multicenter prospective study of children with sickle cell disease: radiographic and psychometric correlation. J Child Neurol 2000;15:333-343.