REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Anesthesiologist:
the
patient’s
perception
Carolina
Sobrinho
Ribeiro
a,∗,
Joana
Irene
de
Barros
Mourão
b,caFaculdadedeMedicinadaUniversidadedoPorto,Porto,Portugal bCentroHospitalarSãoJoão,Porto,Portugal
cDepartamentodeCirurgiaeMedicinadoPerioperatório,FaculdadedeMedicina,UniversidadedoPorto,Porto,Portugal
Received19March2014;accepted6May2014
Availableonline28September2015
KEYWORDS
Anesthesiology; Doctor---patient relationship; Patientsatisfaction
Abstract
Backgroundandobjectives: Anesthesia is still a major concern for patients, although the anesthetic complicationshavedecreasedsignificantly. Additionally,therole assignedtothe anesthesiologistremainsinaccurate.Theaimofthisstudywastoevaluatetheconcernswith anesthesiaandassessthepatient’sknowledgeabouttheanesthesiologist’sduties.
Methods:Prospective study conducted overthreemonths withpatients inthepreoperative anestheticvisitinauniversityhospital.Demographicinformationaboutthelevelofeducation andprioranesthesiawasobtained.Theknowledgeofpatientsregardingtheanesthesiologists’ educationwasevaluated.Patients’concernsandanesthesiologistandsurgeonresponsibilities wereclassifiedwitha5-pointscale.TheanalysiswasperformedwithSPSS21,andp<0.05was consideredstatisticallysignificant.
Results:Weincluded204patients,and135(66.2%)recognizedtheanesthesiologistasa special-istphysician.Notwakingupaftersurgeryandpostoperativeinfectionwerethemainconcerns comparedtoallothers(p<0.05).Womenexpressedmoreconcernthanmenaboutnot wak-ing upafter surgery,nausea andpostoperative vomiting,medical problems,andwaking up duringsurgery(p<0.05).Ensurethatpatients donotwake upduringsurgerywasthe anes-thesiologist task most recognized,compared to all other (p<0.05). The surgeon was more recognized (p<0.05) thantheanesthesiologist inpost-operative,antibioticsadministration, andbloodtransfusionspainmanagement.
Conclusions: Patientsneedtobeinformedaboutthecurrentsafetyofanesthesiaandthe anes-thesiologist’sfunctions.Thepatientinvolvementwilldemystifysomefearsandreassurethe confidenceinthehealthsystem.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mails:carolinamdl@hotmail.com,mimed08056@med.up.pt(C.S.Ribeiro). http://dx.doi.org/10.1016/j.bjane.2014.05.014
PALAVRAS-CHAVE
Anestesiologia; Relac¸ão
médico---doente; Satisfac¸ãododoente
Oanestesiologista:avisãododoente
Resumo
Justificativa/objetivos: A anestesia ainda é uma preocupac¸ão importantepara osdoentes, embora as complicac¸ões anestésicas tenham diminuído significativamente. Adicionalmente, opapel atribuídoao anestesiologistapermanece impreciso. Avaliaraspreocupac¸ões coma anestesiaeverificaroconhecimentodosdoentesacercadasfunc¸õesdoanestesiologistaforam osobjetivosdesteestudo.
Métodos: Estudoprospetivodecorridodurante3mesesem doentescomconsultade aneste-siapré-operatórianumHospitalUniversitário.Foiquestionadainformac¸ãodemográfica,nível de educac¸ão e anestesiaprévia. Foi avaliado o conhecimentodos doentesrelativamente à educac¸ãodoanestesiologista.Aspreocupac¸õesdosdoentes,responsabilidadesdos anestesiol-ogistasecirurgiõesforamclassificadasusandoumaescalade5pontos.Aanálisefoirealizada comSPSS21,p<0,05foiconsideradoestatisticamentesignificativo.
Resultados: Foramincluídos204doentes.135(66,2%)reconheceramoanestesiologistacomo médicoespecialista.Nãoacordarapósacirurgiaeinfec¸ãopós-operatóriaforamasprincipais preocupac¸ões,comparativamenteatodasasoutras(p<0,05).Asmulheresmanifestarammaior preocupac¸ãodoqueoshomenscom(p<0,05):nãoacordarapósacirurgia,náuseasevómitos pós-operatórios,problemas médicoseacordar duranteacirurgia.Assegurarqueosdoentes nãoacordem duranteacirurgia foiatarefamaisreconhecidanoanestesiologista, compara-tivamenteatodas asoutras(p<0,05). Ocirurgiãofoi maisreconhecido(p<0,05) doqueo anestesiologistanagestãodadorpós-operatória,administrac¸ãodeantibióticosetransfusões sanguíneas.
Conclusões:Osdoentesnecessitamdeserinformadosacercadaatualseguranc¸adaanestesia esobreas func¸ões doanestesiologista. Envolverodoenteirádesmistificar algunsreceiose reasseguraraconfianc¸anosistemadesaúde.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Understandingtheroleoftheanesthesiologistandits recog-nitionintheeyesof thecontemporaryworldhasbeen an undervalued subject, being considered as a ‘‘behind the screen’’specialty, inwhich the mainactor is the surgeon andtheanesthesiologisthasonlyasecondaryfunction.1---3
Despiteseveralstudiesonpatients’perceptionof anes-thesiology, there has been no significant evolution in the results or efforts to expose this area of interest to the general public.1---7 The lack of patients’ knowledge is not limitedtotheanesthesiologist’sroleintheoperatingroom, butalsotohisfunctionsinintensivecareunits(ICU), pain management,and teaching medicalstudents.1---6 Patients’ concerns about anesthesia were also the subject of sev-eralstudiesinrecentyears,andalthoughthedevelopment ofanesthesia hassignificantly decreased the incidenceof complications,itisstillamajorcauseofconcern.1,6,8,9 More-over,moststudiescomparingtheknowledgeofpatientswith andwithoutanestheticexperiencedoesnotshowsignificant differencesintheresults,whichmaytranslatelimitationsin patient---anesthesiologistrelationship.3,10
With the recent explosion of information through the mediaand internet, one would expectthe recognition of anesthesiology. This was an area of great development in recent years, which allowed boosting numerous surgi-cal techniques and overcome physiological obstacles.2,5,7
However,weassumethatthedisseminationand apprecia-tionofthismedicalspecialtyisnotsuccessfuland,assuch, toprepareanactionplanwemustfirstevaluatewhatneeds tobedebated.Thus,itisimportanttoknowthepatients’ perceptionoftheanesthesiologist,sothatwecanpromote measuresthatstrengthentherelationshipoftrustbetween doctor andpatient,demystifythe perioperativeprocesses causinganxiety,andclarifytheroleoftheanesthesiologist asanimportantresourceinvestmentarea.
In this line of thought,our study aimed to assess the patient’sknowledgeoftheanesthesiologist’srole,concerns regarding anesthesia, and the functions assigned to the anesthesiologist and the surgeonduring the perioperative period in a university central hospital. For this, we used a questionnaire similar to the one used in the study by Gottschalketal.
Methods
After approval by the Research Ethics Committee of the Centro Hospitalar São João EPE, we began a prospective study for 3months, withpatients undergoing anesthesiol-ogyconsultationattheHospital.Allparticipantswereaged
≥18 yearsand gavewritten informedconsentafter
Table1 Demographicdataofrespondentpatients:gender, age,numberofpreviousanesthesia,andeducation.
Gender(M/F;%) 82/122;40.2/59.8
Age(median;M/F) 59/49
Previousanesthesia(%)
--- No 19(9.3)
--- One 41(20.1)
--- Morethanone 143(70.1)
---NR 1(0.5)
Education(%)
---Notfinishedhighschool 81(39.7)
---Highschool 81(39.7)
---Graduation 32(15.7)
---Postgraduateeducation 9(4.4)
---NR 1(0.5)
NR,didnotrespond.
occurredonlyduringthetimepriortoconsultation,always beforethepatients hadcontactwiththeanesthesiologist. Therewasnohelpfromanyexpertteaminthedistribution. Eachpatientreceivedastandardizedquestionnaireof11 questions(AppendixA),6 withthefollowing issues: demo-graphic data of patients, maximum level of education, and number of previous anesthetic procedures they have undergone. The knowledge of the education and train-ingof anesthesiologistswasevaluated. Patients’ concerns regardingtheperioperativeperiodweregradedonascale offivepoints,from1=noconcernto5=veryconcerned.The questionsabouttheresponsibilitiesofanesthesiologistsand responsibilities ofsurgeons intheoperatingroomand the roleofanesthesiologistsinthehospitalwereclassifiedona scaleoffivepoints,from1=noresponsibility/notinvolved to5=greatresponsibility/veryinvolved.
StatisticalanalysiswasperformedusingSPSS21software (Chicago,IL, USA).Theinformationof questionsclassified 1---5 was evaluated using the Friedman analysis and pair-wisecomparisons.Wilcoxontest wasusedtocompare the responsibilitiesassignedtoanesthesiologistsandsurgeons. Inthecomparativeanalysisofgroupswithandwithout anes-theticexperienceweusedtheKruskal---Wallistest,andthe Mann---WhitneyUtest was usedtocompare between gen-ders.Resultsarepresentedasmedian(25thpercentile,75th percentile)orpercentages.Ap-value<0.05wasconsidered astatisticallysignificantresult.
Results
204 patients participated in the study, with 122 (59.8%) women and 82 (40.2%) men. Fifteen questionnaires were excluded for notfulfillinginformedconsent.Demographic analysis is presented in Table 1. The median age was 52 years.The maximum levelsofeducationprevalentamong patientsweresecondary orlowereducation(39.7%each). Regarding previous experience with anesthesia, 9.3% of patientshadneverundergoneanesthesia,20.1%hadaprior anesthesia,70.1%hadmorethantwopreviousanesthesias, andonepatientdidnotrespond.Thegroupswithand with-outprevious anestheticexperiencewerecomparablewith regardtogender,age,andeducation.
Table2 Patients’understandingoftheanesthesiologist’s roleandestimatedtimerequiredfortraining.
Ananesthesiologistis(%)
---Aspecialistnurse 5(2.5) ---Aspecialistphysician 135(66.2) ---Aspecialisttechnician 28(13.7) ---Aspecialistsurgeon 8(3.9)
--- Donotknow 28(13.7)
Necessarystudytimetobeananesthesiologistafterhigh school(%)
---5years 44(21.6)
---9years 37(18.1)
---12years 13(6.4)
---15years 2(1)
---Donotknow 108(52.9)
Theanesthesiologistwasrecognizedasaspecialistby135 (66.2%)patients,althoughmanyhaveconsideredhima spe-cializedtechnician(13.7%)or didnotknowhowtoanswer thisquestion(13.7%).Theanesthesiologistwasonly consid-eredanexpert surgeonandaspecialistnurseby3.9%and 2.5%ofpatients,respectively(Table2).
Thetimerequiredfortheeducationandtrainingof anes-thesiologistswasgenerallyunderestimated,with44(21.6%) patientsreportingfiveyearsand37(18.1%)patients repor-ting nine years.However, most patients (52.9%) reported notknowingtheeducationandtrainingtimerequired.Only 6.4% attributedthe correct number of years and only 1% overestimatedthetrainingtime(Table2).Comparedtothe educationandtrainingofGeneralpracticeandSurgery,most patients(53.4%)didnotknowdifferentiatethedurationof eachspecialtyeducation,although17.2%recognizethatthe anesthesiologisttrainingislongerthanthegeneralpractice, butshorterthanthesurgery.
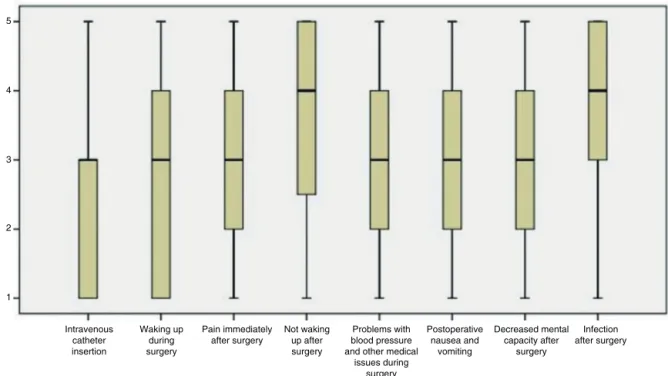
Ingeneral,patientswereconcernedwithvarious situa-tions in the perioperative period (Fig. 1). Not waking up aftersurgeryandinfectionaftersurgerywerethemain con-cernsof patients [3 (4---5),p<0.05compared toall other concerns].Medicalproblemsduringsurgery[3(2---4)],pain immediately aftersurgery [3 (2---4)], and decreased men-tal ability after surgery[3 (2---4)] were concerns similarly classified,all having a significantly higherscore (p<0.05) comparedtoan IVcatheterinsertion. Concern with post-operativenauseaandvomiting(PONV)[3(2---4)]andwaking upduring surgery [3 (1.25---4)] was lowerthan the previ-ous ones, while an IV catheter insertion was the major perioperative concern [3 (1---3), p<0.05 compared to all concernsexcept wakingupduring surgery].Analyzing the answersfromeachgender,thescoresofwomenwerehigher (p<0.05)forwakingupduringsurgery,notwakingupafter surgery,medicalproblemsduringsurgery,andPONV.There were no statistically significant differences between the groupswithandwithoutpreviousexperiencewith anesthe-siaregardingtheassessedconcerns.
5
4
3
2
1
Intravenous catheter insertion
Waking up during surgery
Pain immediately after surgery
Not waking up after surgery
Problems with blood pressure and other medical
issues during surgery
Postoperative nausea and
vomiting
Decreased mental capacity after
surgery
Infection after surgery
Figure1 Concernsofpatientsintheperioperativeperiod.1=noconcernto5=veryconcerned.
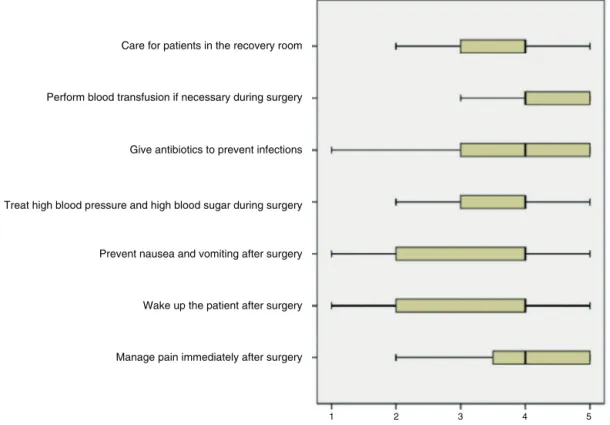
responsibilities, except medical conditions management duringsurgery,p>0.05](Fig.2).Othertaskshavealsobeen recognized as the anesthesiologist’s responsibility but on a smaller scale, such asmanaging medicalproblems dur-ingsurgery[4(3---4),p<0.05comparedtoperformingblood transfusions],takingcareofpatientsintherecoveryroom[4
(3---5)],managingpainimmediatelyaftersurgery[4(3---4)], andpreventingPONV[4(3---4)].Givingantibiotics[3(1---4)] andperformingblood transfusions[3(1---4)]duringsurgery were the least recognized tasks. Women attributed more responsibility to the anesthesiologist than men regarding the tasks of postoperative pain management and waking
Care for patients in the recovery room
Perform blood transfusion if necessary during surgery
Give antibiotics to prevent infections
Treat high blood pressure and high blood sugar during surgery
Prevent nausea and vomiting after surgery
Wake up the patient after surgery
Manage pain immediately after surgery
Ensure that patients do not wake up during surgery
1 2 3 4 5
Figure2 Knowledgeofpatientsregardingtheanesthesiologist’sresponsibilitiesintheperioperativeperiod.1=noresponsibility
Care for patients in the recovery room
Perform blood transfusion if necessary during surgery
Give antibiotics to prevent infections
Prevent nausea and vomiting after surgery
Wake up the patient after surgery
Manage pain immediately after surgery Treat high blood pressure and high blood sugar during surgery
1
2
3
4
5
Figure3 Knowledgeofpatientsregardingtheinvolvementofsurgeonintheperioperativeperiod.1=noinvolvementto5=very involved.
thepatientupaftersurgery(p<0.05).The previous anes-theticexperiencedidnotsignificantlyaffecttheratingsof theanesthesiologist’sperioperativeresponsibilities.
As for the surgeon’s involvement of the on the tasks described in the questionnaire, the patients considered blood transfusion during surgery as the task withgreater involvementofthesurgeon(Fig.3).Womenattributed sig-nificantly higher scores (p<0.05) for the responsibility of wakingthe patientupafter surgeryand givingantibiotics thanmen.Similarlytothepreviousquestion,theanesthetic experiencedidnotchangetheratingsofpatientsregarding thesurgeon’sinvolvementinthedescribedtasks.
Comparison of the functions assigned to anesthesiolo-gistsandsurgeons duringtheperioperative periodreveals thattheanesthesiologistwasratedmoreresponsibilityfor waking the patient up after surgery (p<0.05), preven-ting PONV,and takingcare of thepatientin therecovery room.Ontheotherhand,thesurgeonwasconsideredmore involved in pain management in the early postoperative period(p<0.05),givingantibiotics(p<0.05),and perform-ingbloodtransfusionsduringsurgery(p<0.05).
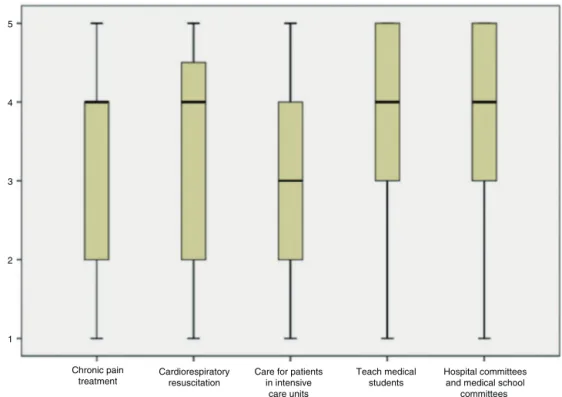
As for anesthesiologists’ in-hospital tasks outside the operatingroom, thepatients showed some recognitionof the anesthesiologists’ involvement in this task (Fig. 4). Teachingmedicalstudentswastheanesthesiologist’smost recognizedtaskoutsidetheoperatingroom[4(3---5),p<0.05 comparedtoallothertasks,exceptcomparedto participa-tioninhospitalcommitteesandmedicalschools[4(3---5)]. Cardiopulmonary resuscitation [4 (2---40.75)] and chronic pain treatment [4 (2---4)] were recognized as anesthesiol-ogist’sfunctions,buttoalesserextent.Theinvolvementof anesthesiologistsincaringforpatientsinintensivecareunits
(ICU)wastheleastrecognizedtaskbypatientsquestioned [3(2---4)].Theratingofanesthesiologists’in-hospital func-tionsbetweenbothgenderswassimilar.Ontheotherhand, patients who had never undergone anesthesia assigned moreresponsibilityregardingcaringforpatientsintheICU (p<0.05) compared to patients with prior experience in anesthesia.
Discussion
The knowledge of patientsabout therole and trainingof anesthesiologistsisshallowandpoorlyunderstood,ignoring many of their functions. In this study, most patients rec-ognizedtheanesthesiologistasamedicalexpert,although 27.4% of the patients considered him a specialized tech-nician or did not know how to answer. These data are consistentwithpreviousliteratureinwhichtherecognition ofanesthesiologistsasexpert doctorsranged from50% to 99%.1,3,6,7,10
More than half of patients are unaware of the edu-cation and training time of anesthesiologists, with its duration underestimated by most respondents. Similarly, most patients did not know to distinguish the training timeforSurgery,FamilyMedicine,andAnesthesiology. Sur-prisingly, although the anesthesiologist training time is underestimated, only 5.4% of patients considered it the shortestofall.
5
4
3
2
1
Chronic pain
treatment Cardiorespiratoryresuscitation
Care for patients in intensive
care units
Teach medical students
Hospital committees and medical school
committees
Figure4 Knowledge ofpatientsregarding theanesthesiologist’sfunctions outsidetheoperating room.1=noinvolvementto
5=veryinvolved.
surgery),althoughpost-operativepainhasbeenhighlighted asthesecondmainconcerninthesestudies,havingoccupied thefourth positionin ourstudy.1 Mattheyet al. reported greaterconcernforwakingupduringsurgery,braindamage ormemory loss,withthemajority of patientsshowing no concernaboutpost-operativepain.Itiscontrastingthefact thatinthisstudythemajorityofpatientshavenoconcern aboutcomplicationsregardinganesthesia,alsodescribedin ourstudy.However,therespondentsconsistedofarandom populationinanon-hospitalsetting,whichdemonstratesthe variabilityofresultsaccordingtothetypeofstudy popula-tionandthemediumusedforinvestigation.8
Within the perioperative concerns presented, women expressed greater concern. These findings are consis-tent with previous studies reporting increased anxiety by females. This reinforces the perioperative need for doctor---patientindividualizedandpersonalizedrelationship based on personal, social, and cultural characteristics of eachpatient.8,11Therewerenosignificantdifferencesinthe intensityofperioperativeconcernsamongindividualswith andwithout previousanestheticexperience.Theseresults mayreflecttheabsenceofprogressinknowledgeand famil-iaritywiththeperioperativeproceduresaftertheanesthetic experience,unliketheevolution reportedin thestudy by Leiteetal.7
As for patients’knowledge ofthe intraoperativetasks, theroleoftheanesthesiologistwasmuchundervalued com-paredto that of surgeon.PONV prevention, management of medical problems during surgery, and taking care of thepatientin the recovery roomwere similarlyclassified responsibilitiesbetweenthetwomedicalspecialties. How-ever,thesurgeonwassignificantlyvaluedinpostoperative painmanagement,givingantibiotics,andbloodtransfusions comparedtothe anesthesiologist.The onlytaskdistinctly
classified asbeing theanesthesiologist’s greater responsi-bilitywaswakingthepatientupaftersurgery,althoughthe surgeon has also been considered involved. These results differ from the study by Gottschalk et al. regarding the lessrecognitionoftheanesthesiologist’sfunctionsandthe clearovervaluationofthesurgeon.6Itisalsoimportantto notethat,ingeneral,patientsconsideredbothsurgeonsand anesthesiologistsatleastsomewhatinvolvedinall periop-erativefunctionsdescribed,whichraisesthepossibilitythat thepatientsareunawareoftheroleofbothinthe operat-ingroom, butconsiderasthemost involved theonethey aremostfamiliarwith.Again,thepreviousexperiencewith anesthesiadidnotappeartobea modifyingfactor in the knowledge of thepatients askedabout the intraoperative functions.Thisinformationhasbeenasimilarfindingamong various studies in this area, which highlights the existing weaknessinthe communicationandtransmissionof infor-mation between the anesthesiologist and the patient.5,10 Therefore,inourstudy,thepreviousanestheticexperience seemedtohavenoinfluenceonpatientinformation.
reflect agreater uncertainty of patients without previous anestheticexperienceandhencegreaterneed toconsider thedoctorandgivehimmorefunctions.However,this dif-ferencewasisolated,andthereforenotfullyunderstood.
The interpretations of our study may have several limitations,suchas:theselectionofindividualsinthe pre-operativeanesthesiaconsultationmayhaveselectedagroup ofpatientswithmoresurgicalandanestheticprior experi-enceinsteadofcommonpatients,theuseofaquestionnaire asameansofdatacollectionmayhavelimitedthe under-standingofthesubjectsaskedandpossibleanswers,unlike aninterview,forexample.
The proper education of patients about anesthesiol-ogycompetesprimarilytoanesthesiologists.Thisimpliesa greater interest bythe medicalspecialty in communicate andfostertieswiththepatient,becausepatient satisfac-tionis clearly involved in clinical quality andtherapeutic success.7,12,13Thereisstillcontroversyabouttheamountof informationandhowitshouldbetransmittedtothepatient, inordertoreducetheanxietyregardingtheproceduresand preventitsaggravation,whichhasbeendiscussedinseveral studies.12,14,15Itisimportanttoreassurethepatientabout thesafetyoftheprocedures,asthelevelofperioperative concernremains in disharmonywiththerealincidenceof anestheticcomplications.8,9
Inconclusion,thisstudydemonstratedthatthepatients’ perceptionofanesthesiologistsisstillunderestimated,and it is not clear to the studied population what is anes-thesiology and what are the specific areas in which the anesthesiologistcanintervene.
Engagingthepatientinthisprocessisimportant,asmuch of the success will depend on him. For such,it is neces-sarythatthepatientunderstands,ratherthanbeingamere puppetinthehandoftheartist.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
ToProfessorFernandoAbelha,ProfessorAndréNovo,andDr. JoselinaBarbosa,forthepreciouscollaboration.
Appendix
A.
Supplementary
data
Supplementary data associated with this article can be found, in the online version, at doi:10.1016/j.bjane. 2014.05.014.
References
1.HariharanS.Knowledgeandattitudesofpatientstowards anes-thesia and anesthesiologists. Areview. Anestesiaen Mexico. 2009;21:174---8.
2.Simini B.Anaesthetist:thewrong namefor theright doctor. Lancet.2000;355:1892.
3.deOliveiraKF,ClivattiJ,MunechikaM,etal.Whatdopatients knowabouttheworkofanesthesiologists?RevBrasAnestesiol. 2011;61:720---7.
4.HariharanS,Merritt-CharlesL,ChenD.Patientperceptionof theroleofanesthesiologists:aperspectivefromtheCaribbean. JClinAnesth.2006;18:504---9.
5.CalmanLM,MihalacheA, EvronS,etal.Current understand-ingofthepatient’sattitudetowardtheanesthetist’sroleand practice inIsrael: effectofthe patient’s experience.J Clin Anesth.2003;15:451---4.
6.GottschalkA,SeelenS,TiveyS,etal.Whatdopatientsknow aboutanesthesiologists?Resultsofacomparativesurveyinan U.S.,Australian,andGermanuniversityhospital.JClinAnesth. 2013;25:85---91.
7.Leite F,da SilvaLM,BiancolinSE,etal. Patientperceptions aboutanesthesiaandanesthesiologistsbeforeandaftersurgical procedures.SaoPauloMedJ.2011;129:224---9.
8.Matthey P, Finucane BT, Finegan BA. The attitude of the general public towards preoperative assessment and risks associatedwithgeneral anesthesia.CanJ Anaesth.2001;48: 333---9.
9.Royston D.CoxF ---anaesthesia: thepatient’spointofview. Lancet.2003;362:1648---58.
10.MavridouP,DimitriouV,PapadopoulouM,etal.Effectof pre-viousanesthesiaexperienceonpatients’knowledgeanddesire for informationaboutanesthesia and theanesthesiologist: a 500 patients’ survey from Greece. Acta Anaesthesiol Belg. 2012;63:63---8.
11.MasoodZ,HaiderJ,JawaidM,etal.Preoperativeanxietyin femalepatients:theissueneedstobeaddressed.KUSTMedJ. 2009;1:38---41.
12.Snyder-RamosSA,SeintschH,BottigerBW,etal.Patient sat-isfaction and information gain after the preanesthetic visit: acomparisonofface-to-faceinterview,brochure, andvideo. AnesthAnalg.2005;100:1753---8.
13.Rozenblum R, Donzé J, Hockey PM, et al. The impact of medical informatics on patient satisfaction: a USA-based literature review. Int J Med Inform. 2013;82: 141---58.
14.KakinumaA,NagataniH,OtakeH,etal.Theeffectsofshort interactiveanimationvideoinformationonpreanesthetic anx-iety,knowledge,andinterviewtime:arandomizedcontrolled trial.AnesthAnalg.2011;112:1314---8.