revbrashematolhemoter.2016;38(4):361–363
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
Report
A
closer
look
into
blood
group
discrepancy
arising
due
to
an
underlying
malignancy
Rajeswari
Subramaniyan
a,∗,
Balan
Louis
Gaspar
b aYashodaHospital,Malakpet,Hyderabad,IndiabPostgraduateInstituteofMedicalEducation&Research,Chandigarh,India
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20February2016
Accepted11April2016
Availableonline2May2016
Introduction
TheABH antigensare histo-bloodgroup antigens that are
present in circulating blood cells, tissues and body fluids.
Theassociationofbloodgroupswithvariousdisease states
hasbeenwelldocumentedintheliterature.Both
hematopoi-eticandnon-hematopoieticmalignanciesareassociatedwith
bloodgroupchanges.Insolidorganmalignancies,excessive
bloodgroupsubstancesproducedbythetumorleadtoblood
groupdiscrepancies.1 However,suchdiscrepanciesare rare
with a very few case reports in the literature. Herein, we
describeanunusualcaseofabloodgroupdiscrepancyina
48-year-oldladywhowasdiagnosedwithsignetringcellgastric
adenocarcinoma.
Case
description
Abloodsampleofa48-year-oldladywasreceivedforblood
groupingand cross-matching.Herhemoglobin, total
leuko-cyte and platelet counts were 5.6g/dL, 4800cells/L and
3.84×105cells/L, respectively.As per ourprotocol,we did
∗ Correspondingauthorat:DepartmentofTransfusionMedicine,YashodaHospital,Malakpet,Hyderabad500036,India.
E-mailaddress:[email protected](R.Subramaniyan).
thepreliminarybloodgroupingofthepatientwithunwashed
cellsusingthetubetechniquetocheckavailabilityofblood
inourinventory. Forwardgrouping resultswereasfollows:
noagglutinationwithanti-Aandanti-Bantiseraand,weak
agglutination withanti-A,Bmonoclonalantiserum. Reverse
grouping revealedAgroup.Theresultsweresimilarwitha
repeat sample and columnagglutination technology.
Reac-tionwithanti-A1lectinwasnegativeandreactionwithanti-H
lectinwas4+.TheinitialbloodgroupingwasmimickingtheAx
phenotype.Asperherpreviousbloodgrouprecords,shewas
ARhDpositive.Thepatienthadahistoryoftransfusionfive
yearspreviouslyduringahysterectomy.Thebloodgrouping
wasrepeatedafterwashingherredcellsthricewith
physiolog-icalsaline(0.9%)asperthedepartmentalstandardoperating
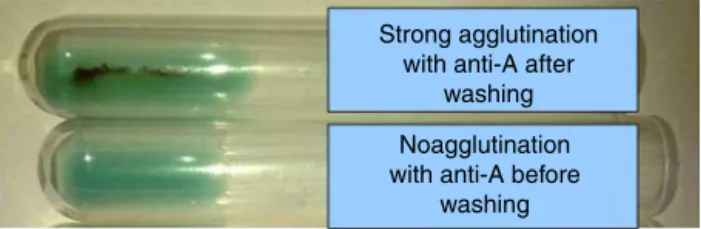
procedure. Strong agglutinationwasnotedwithanti-A and
anti-A,B(Figure1).Reactionwithanti-A1lectinwaspositive
andreactionwithanti-Hlectinwas4+.Hence,herbloodgroup
wasconfirmedasA1RhDpositive.Salivasecretorstatuswas
alsostudied.ShewasasecretorofbothAandHbloodgroup
substances.
Meanwhile, wegathereddetailsofthe patient’smedical
history. The patient was admitted two months previously
http://dx.doi.org/10.1016/j.bjhh.2016.04.007
1516-8484/©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.PublishedbyElsevierEditoraLtda.Thisisan
362
revbrashematolhemoter.2016;38(4):361–363Strong agglutination with anti-A after
washing
Noagglutination with anti-A before
washing
Figure1–Unwashedredcellsofthepatientshowedno
agglutinationwithmonoclonalanti-A,whileafterwashing
threetimes,redcellsshowedstrongagglutinationwith anti-A.
withahistoryofabdominalpain.Multislicespiralcomputed
tomography(CT)oftheabdomenrevealedaheterogeneously
enhanced transmural wallthickening (3.5cm) with a large
ulcerand irregularmucosainthegastric fundusand body.
Themass was invading the left adrenal gland. There was
noassociatedlymphadenopathyordistantmetastasis.These
findingswereconsistentwithadiagnosisoflocallyadvanced
gastriccancer.Uppergastrointestinalendoscopicbiopsy
con-firmed the diagnosis of a primary gastric signet ring cell
carcinoma.Shecompletedtwocyclesof5-flurorouraciland
cisplatin-based palliative chemotherapy. Thepresent blood
sample was taken three weeks after the second cycle of
chemotherapy.
WesuspectedthattheremightbeAbloodgroupsubstance
inthepatient’sserumwhichinhibitedthereactionwithanti-A
antiserum.Theamountofinhibitingsubstanceinthepatient’s
serum was tested based on the methodology described by
Treacyetal.2Monoclonalanti-AwastitratedagainstA2cells.
Thetiterofanti-Awas1:512andadilutionof1:16wasusedfor
thestudy(thenexttothelastdilutionshowinga4+reaction
withA2cellswasused).A2cellswerepreparedfroma
sin-gledonor.Doublingdilutionsofserum(eachtubecontaining
100LofthepatientandahealthybloodgroupAdonor)was
madeand100Lofdilutedmonoclonalanti-Awasaddedto
eachtube.Thesuspensionsweremixedwellandincubatedfor
30minatroomtemperature.Analiquotof100Lofwashed
Aredcellswasaddedtoalltubes,incubated atroom
tem-perature for30min and centrifuged at1000rpmfor 1min.
Completeneutralization(inhibitionofhemagglutination)was
seenupto1:64dilutionofthepatient’sserum,whilenormal
controlserumshowednoinhibition.Hence,itwasconcluded
thatthebloodgroupdiscrepancynotedinthispatientwasdue
tothepresenceofanexcessofAbloodgroupsubstanceinher
serum,probablysecretedbythetumorcells.Thepatientwas
transfusedwithoneunitofA1RhDpositivepackedredblood
cellsandthetransfusionwasuneventful.Herpost-transfusion
hemoglobinwas7g/dL.Shewasfollowed-upforthreeweeks
afterchemotherapy.Therewasnoapparentreductionin
neu-tralizationactivityoftheserum.
Discussion
Several studies in the past havereported on malignancies
andtheireffectsonbloodgroups.Otherthanredcells,
spe-cific substances of ABH blood groups have been detected
in mucous glands, epithelial cells, neurons, and vascular
endothelialcells.3,4Alterationsofredcellantigensoccurwith
bothhematologicand solidmalignancies.In hematological
malignancies,loss/weakeningofredcellantigenexpression
occurs duetogeneticand epigeneticchanges inthe Aand
Btransferasegenes.Insolidtumors(bladder,lung,headand
neck,cervical,andthyroid),lossofexpressionofthe
histo-bloodgroupABHantigensfromtumorcellsisaknownevent,
butredcellantigenexpressionmaynotbereduced.5Rather,
neutralizationoftypingantiserumbythebloodgroup-specific
soluble substances secreted by tumor cells can be seen.1
Thefirst reportofsuchassociation wasin1959when
Bar-berandDunsfordreportedexcessofbloodgroupAsubstance
in a female patient with gastric carcinoma resulting in a
bloodgroupdiscrepancy.6Thisfindinghasalsobeenreported
to occur in pancreatic, ovarian, colonic, and bile duct
car-cinoma and, pseudomucinous ovarian cysts.1,7,8 Secretions
from tumorcells enter the blood stream either directly or
through ascitic fluid absorption.8 Saeed and Fine
demon-strated excess A and H blood group substances in tumor
cell cytoplasmbyimmunofluorescencestudies inapatient
withstomachadenocarcinoma.Theseexcesssolubleantigens
probablyneutralizedanti-Aantiserumthatledtoambiguous
bloodgrouping.9 Rougeretal.studied70patientswith
gas-tricorcoloncarcinomaandconcludedthattheindividualsof
bloodgroupAhadhigherlevelsofAbloodgroupsubstance
inserumwhencomparedtocontrols,10 howeverthereason
forthisbiochemicalbehaviorisnotknown.Joshietal.from
Indiareportedacaseofbloodgroupdiscrepancyduetoexcess
secretionsofAbloodgroupsubstancebyovarianmucinous
cystadenoma.Afterresectionofthetumor,thediscrepancy
wasreversed.11Unusually,bloodgroupsubstanceshavebeen
foundinhealthyindividualsandevenatlowerconcentrations
innewborns.6,8,9
ABH blood group substances neutralize the commercial
antiserumprovidingnobindingsiteforredcellantigens.
Com-pletewashingofredcellsremovestheinhibitingsubstance
unmaskingthe effect.Inourcase,complete inhibitionwas
seen up to1:64 dilutionofthe patient’s serum.In aseries
offour patients, Treacyet al.notedhigh concentrationsof
Abloodgroupsubstanceinserumwithtitersrangingfrom
1:512to1:2048,whereasJoshietal.reported
hemagglutina-tioninhibitingactivityofAbloodgroupsubstanceonlyupto
a1:128dilution.2,10
Loss of ABH antigens from the dedifferentiated tumor
cells isalso known and has been associated witha
nega-tiveprognosticimpact.Itisevidentfrom theliteraturethat
most of the patients with carcinoma who were reported
to havethis neutralizationeffectinserum were diagnosed
with end stage/advanced disease and later succumbed to
the disease.2,6,9 Althoughthis statement seems quite
sim-ple, some questions still remainunanswered. (1) Is excess
ofblood groupsubstancesinserum relatedtotumor
clini-calbehaviorandprognosis?(2)Isthefindingofexcessblood
groupsubstancesmorecommoninadenocarcinomasofthe
gastrointestinaltractandovariesthantumorsatothersites?
Furtherexplorationisneededtocommentonthesequestions.
Notwithstanding, rapidly expanding molecular diagnostics,
serological methods undoubtedly have a first-line role to
solvebloodgroupdiscrepanciesinthepracticeoftransfusion
revbrashematolhemoter.2016;38(4):361–363
363
Weconcludethat excess blood groupsubstances inthe
serumneutralizingthetypingantiserumisaveryrare
phe-nomenon. This has been demonstrated in patients with
gastrointestinaltractcarcinomaandovariancysts.
Serologi-caltechniqueswouldbehelpfulinresolvingthesebloodgroup
discrepancieswheremolecularmethodsareunavailable
espe-ciallyinresource-limitedsettings.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
We thank Dr Karishma for assisting us in writing the
manuscript.
r
e
f
e
r
e
n
c
e
s
1. WintersJL,HowardDS.Redbloodcellantigenchangesin malignancy:casereportandreview.Immunohematology. 2001;17(1):1–9.
2.TreacyM,GeigerJ,GossMF.Substancesinserumcausing interferencewithbloodgroupdetermination.Transfusion. 1967;7(6):443–6.
3.GarrattyG.Bloodgroupsanddisease:ahistoricalperspective. TransfusMedRev.2000;14(4):291–301.
4.GarrattyG.Dobloodgroupshaveabiologicalrole?In: GarrattyG,editor.Immunobiologyoftransfusionmedicine. NewYork,USA:MarcelDekker,Inc;1994.p.201–55.
5.BiancoT,FarmerBJ,SageRE,DobrovicA.LossofredcellA,B, andHantigensisfrequentinmyeloidmalignancies.Blood. 2001;97(11):3633–9.
6.BarberM,DunsfordI.Excessblood-groupsubstanceAin serumofpatientdyingwithcarcinomaofstomach.BrMedJ. 1959;1(5122):607–9.
7.HattonJ,WalshRJ.Anunusualdifficultyinbloodgrouping. Interferencebysolubleantigeninapatient’sserum.Vox Sang.1961;6:568–73.
8.KleinHG,AnsteeDJ.Mollison’sbloodtransfusioninclinical medicine.12thed.Oxford:BlackwellPublishing;2013.p.128.
9.SaeedSM,FineG.ExcessiveserumlevelsofAandH substancesinapatientwithgastriccarcinoma.Transfusion. 1968;8(3):179–83.
10.RougerP,RiveauD,SalmonC,LoygueJ.Plasmabloodgroup changesingastrointestinaltractcarcinoma.JClinPathol. 1979;32(9):907–11.