www.jped.com.br
ORIGINAL
ARTICLE
Medication
use
among
children
0-14
years
old:
population
baseline
study
夽
Maria
J.B.
Cruz
a,∗,
Lays
F.N.
Dourado
a,
Emerson
C.
Bodevan
b,
Renata
A.
Andrade
a,
Delba
F.
Santos
aaFaculdadedeCiênciasBiológicasedaSaúde,UniversidadeFederaldosValesdoJequitinhonhaeMucuri(UFVJM), Diamantina,MG,Brazil
bFaculdadedeCiênciasExataseTecnológicas,UniversidadeFederaldosValesdoJequitinhonhaeMucuri(UFVJM), Diamantina,MG,Brazil
Received29January2014;accepted28March2014 Availableonline20June2014
KEYWORDS
Children; Adolescent; Druguse; Self-medication; Pharmacoepidemiology; Nursing
Abstract
Objective: Determinetheprevalenceofmedicationuseinchildrenandadolescentsin20 munic-ipalitiesofValedoJequitinhonha,MinasGerais-Brazil,showingthemaingroupsandvariables thatmayhaveinfluenceduse.
Methods: Descriptivepopulation-based survey sampleof555interviews, selectedby simple randomclustersamplingof137censustracts.Inclusioncriteriawereage≤14years,mandatory interviewwiththelegalguardians,andregardlessofhavingreceivedmedications.Regardingthe usagepattern,participantsweredividedintotwogroups:consumptionandnon-consumption ofdrugs.Adescriptiveanalysisofthevariablesandtestsofassociationwereperformed. Results: Theprevalenceofdrugconsumptionwas56.57%,and42.43%showednoconsumption. Theuseofmedicinalplantswas72.9%fordrugusersand74.3%fornon-users.Thehealth condi-tionsforconsumptionwerecough,commoncold,flu,nasalcongestionorbronchospasm(49.7%), fever(5.4%),headache(5.4%),diarrhea, indigestion,andabdominalcolic(6.7%).In casesof self-medication,30.57%ofthedrugsweregivenbythemother,and69.42%wereprescription drugs.Self-medicationwasprevalent usingparacetamol(30.2%),dipyrone(20.8%),andcold medicine(18.8%).Therewasincreaseduseofanalgesics/antipyretics,followedbyrespiratory medications,systemicantibiotics,histamineH1antagonists,andvitamins/antianemics. Conclusions: Theprevalenceofdrugsuseinchildrenwashigh,indicatingtheneedfor formu-latingeducationalprogramsaimingattheawarenessofcaregiversregardingrationaluse. ©2014SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:CruzMJ,DouradoLF,BodevanEC,AndradeRA,SantosDF.Medicationuseamongchildren0-14yearsold: populationbaselinestudy.JPediatr(RioJ).2014;90:608---15.
∗Correspondingauthor.
E-mail:[email protected](M.J.B.Cruz).
http://dx.doi.org/10.1016/j.jped.2014.03.004
PALAVRAS-CHAVE
Crianc¸as; Adolescentes; Usode
medicamentos; Automedicac¸ão; Farmacoepidemiologia; Enfermagem
Usodemedicamentosentrecrianc¸asde0-14anos:estudodebasepopulacional
Resumo
Objetivo: Determinaraprevalênciadoconsumodemedicamentoemcrianc¸aseadolescentes de20municípiosdoValedoJequitinhonha,MinasGerais-Brasil,mostrandoosprincipaisgrupos evariáveisquepossamterinfluenciadoouso.
Métodos: Estudodescritivotipoinquéritopopulacionaldomiciliar,amostraconstituídapor555 entrevistasselecionadasdemaneiraaleatóriasimplespormeiodeamostragempor conglom-erado de137setores censitários.Oscritériosdeinclusão foramidade≤14anos, entrevista obrigatória com os responsáveis legais, independente de terem consumido medicamento. Quanto ao padrãode usoosparticipantes foramdivididos emdoisgrupos consomem enão consomem medicamentos. Realizada análise descritiva das variáveis e aplicados testes de associac¸ão.
Resultados: Aprevalênciadeconsumodemedicamentosfoi56,57%eonãoconsumo42,43%. Ousodeplantasmedicinaisfoide72,9%paraoconsumodemedicamentoe74,3%paraonão consumo. Assituac¸õesde saúdeparaoconsumo foramtosse,resfriadocomum,gripe, con-gestãonasaloubroncospasmo(49,7%);febre(5,4%);cefaléia(5,4%);diarréia,‘‘mádigestão’’ ecólicaabdominal(6,7%).Naautomedicac¸ão,30,57%dosmedicamentosforamindicadospela mãe,e69,42%de prescric¸ões médicas.Destaca-senaautomedicac¸ãoousodeparacetamol (30,2%),dipirona(20,8%)eantigripais(18,8%).Eummaiorusodeanalgésicos/antipiréticos, seguidodoaparelhorespiratório,antibióticossistêmicos,antagonistasH1dahistaminae vita-minas/antianêmicos.
Conclusões: A prevalência do consumo de medicamentos na populac¸ão infantil foi alta, indicando a necessidade de formulac¸ão de programas educativos visando principalmente à conscientizac¸ãodoscuidadoressobreousoracional.
©2014SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
The main users ofhealth servicesin developing countries arechildren,andtheirpatternofillnessisreflectedin med-ication use.1 This use, in turn, can be excessive due to self-medication, a widespread practice in Brazil, induced bythemediaandperformed withoutindicationand medi-calprescription.InBrazil,approximately80millionpeople practiceself-medication,andtheriskofthispracticeis cor-relatedwiththelevel ofeducationandinformationabout drugs, as well as the accessibility of medications in the healthsystem.2
Inthissense,someauthorsrecommendspecialattention tothemedicationsusedbychildren,consideringthe reser-vationsregardingtheirefficacyandsafetycausedbylackof clinicaltrialsduetoethical,legal,andeconomic reasons, and limited knowledge about the effects of the medica-tion on the body.3,4 In the case of children, the practice of medicationuse isbasedprimarily onextrapolation and adaptationsoftheuseinadults,ontheinformationobtained fromrareobservationalstudies,andonexpertconsensuses.5 Although scarce in developing countries, population-based studies are required to evaluate the use of medications in children.6,7 A study conducted in Brazil demonstratedaprevalenceof56%, whichindicatesahigh consumptionbychildren,indicatingasignificantuseof med-icationswithindication andage restrictions,especiallyin childrenyoungerthan2years.8Consideringthesefacts,itis advisabletoestablishaspecificlistofessentialmedications
accordingtotheneedsofchildren,aimingtopromotetheir rationaluse.9
Inordertocontribute tothisarea, apopulation-based epidemiologicalstudywasconductedinchildrenaged0-14 yearslivinginurbanareasofValedoJequitinhonha,located inthenorthernregionofthestate ofMinasGerais,Brazil. Theobjectivewastoidentifytheprevalenceandpatternof medicationuse,withorwithoutprescription,demonstrating themaingroupsandtypesofdrugsused,aswellasvariables thatmayhaveinfluencedthisuse.
Methods
This descriptive, exploratory, cross-sectional, population-basedhousehold-surveystudywascarriedoutfromApril10 toJuly20,2013.Inclusioncriteriawereage≤14yearsold, mandatoryinterviewwiththelegalguardians,regardlessof havingreceived medications. All guardians whowere not presentatthetimeoftheintervieworwhorefusedto par-ticipatewereexcludedfromthestudy,aswellaswhenthe selectedhouseholdwasacommercialproperty, ordidnot haveresidentsaged≤14years.
used,showinga totalof approximately88,936 individuals aged≤14yearsin20municipalities oftheIntermunicipal HealthcareConsortiumofAltoJequitinhonha,Diamantina, MinasGerais,Brazil.
Regarding the Human Development Index (HDI) of the municipalitiesstudied,18fivehadanHDIbetween0.558and 0.582;14,between0.616-0.682,andone,0.716,reflecting indicatorsofeducation,housing,health,work,income,and vulnerability.
Simplerandomclustersamplingwasusedtoselect house-holds,usingasreferenceunit137urbancensussectorsfora sampleof672householdsdefinedbyIBGE(2010).11However, a greater number of sectorswas chosen, estimating that therequiredminimumnumberofindividualswouldnotbe met,especiallyincentralsectors(commercialproperties) and in old neighborhoods withelderly residents. An IBGE map(2010)wasprintedforeachselectedsector,11allowing theinterviewer tofind itin the fieldandwalk aroundit, followingapre-establishedsystemforhouseholdselection. Datawerecollectedbyfourinterviewerstrainedinapilot study tovalidatethe collection, using astructured open-andclosed-questionquestionnaire.Inhouseholdswithmore thanone child,only onequestionnaire wasapplied,after theindividualwasselectedbydrawinglotsusingatableof randomnumbers.
The dependent variable was medication use, and the participantsweredividedintotwostudygroups:uses med-icationand does notuse medication.Self-medication was defined as medication use due to lay advice, and medi-calprescription wasdefined asmedication use motivated by medical consultation and prescription for the disease thatoriginateduse.Themedicationsusedweredividedinto groupsandsubgroupsaccordingtothelatestversionofthe AnatomicalTherapeuticChemical(ATC)Classificationofthe World Health Organization (WHO).12 Two groups of varia-bles,socioeconomicindicatorsanduseofhealthcare(public or private) services,were considered. The socioeconomic indicatorsconsideredinthestudyweretheheadofthe fam-ily’soccupation(employedorunemployed/retired);family income in minimum wages at the time of the interview; andthecriteriaoftheBrazilianAssociationofBusinessand Research(Associac¸ão Brasileirade Empresas ePesquisas -ABEP),consideringameasureofpotentialandconsumption habits.13
For data analysis, a descriptive analysis of the dependentvariableandtheexplanatory variableswas ini-tially conducted, and association tests (chi-squared and Fisher’sexact) were subsequently applied.Analyses were processed using the statistical software Epi-Info, release 7.0(CDC/WHO,Atlanta, GE,USAs); and R,release2.12.2 (CDC/WHO-Atlanta,UnitedStates).14
ThestudyprotocolwasapprovedbytheResearchEthics CommitteeofUniversidadeFederal dosValesdo Jequitin-honha e Mucuri (UFVJM; Opinion 044/11); the participant population wasinformedof thestudy purpose andsigned theinformedconsent.
Results
Thestudy included 672individuals,of whom117(17.41%) werelosses andrefusals, resultingin 555 interviews. The
0
2 4 6 8 10 12 14
Age (years)
Received Did not receive
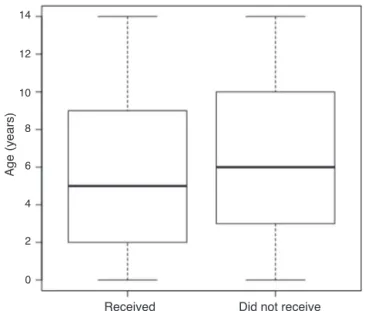
Figure1 Graphicalrepresentationofgroupsofchildrenand
adolescentswhoreceivedmedicationsonthe15dayspriorto thehouseholdinterview,according toage-Valedo Jequitin-honhaMunicipalities(MG),Brazil,2014.
Thedataareshownwithoutbox-and-whiskerplots;ineach rect-angle(boxplot),thelower,intermediate,andupperhorizontal linesrepresentthe1stquartile(25thpercentile),median(50th percentile),and3rdquartile(75thpercentile),respectively.The lowerandupperlimitsoftheverticallinesrepresentthelowest andhighestvalue,respectively.p=0.88(Mann-WhitneyU-test).
validated interviews followed a similar pattern of distri-bution during the four-month study in 20 municipalities (138.5±34.6interviews/week).Themeanageofthe indi-viduals whoused medications was2-7 years (38.9%), and 7-14years(43.9%)in thoseusingmedicationsaccordingto medicalprescriptionandself-medication(Fig.1).
Considering the use of medicationsin the previous 15 days, theprevalence of use was 56.57%, withno statisti-cally significant difference when comparing the 20 cities (chi-squared,p=0.5).Regardingtheuseofmedicinalherbs andplantsamongchildrenwhousedanddidnotuse medi-cations,itwas72.9%and74.3%,respectively(Table1).
Mostparticipants livedin brickhouses(97.5%) andhad sanitation facilities (92.9%), public water supply (99.5%), andpublicgarbagecollectionservice(99%).Itwasobserved thattheuseofself-medicationwasnotstatistically signifi-cant(p<0.05)regardingageranges,gender,familyincome, andaccesstohealthcareservices(Table2).
The main health conditions thatmotivated medication use were cough, common cold, flu, nasal congestion, or bronchospasm(49.7%);fever (5.4%);headache(5.4%);and diarrhea,indigestion,andcolic (6.7%).Inself-medication, 30.57% ofthe medicationsweregivenby themother,and 69.42%resultedfrommedicalprescriptions.
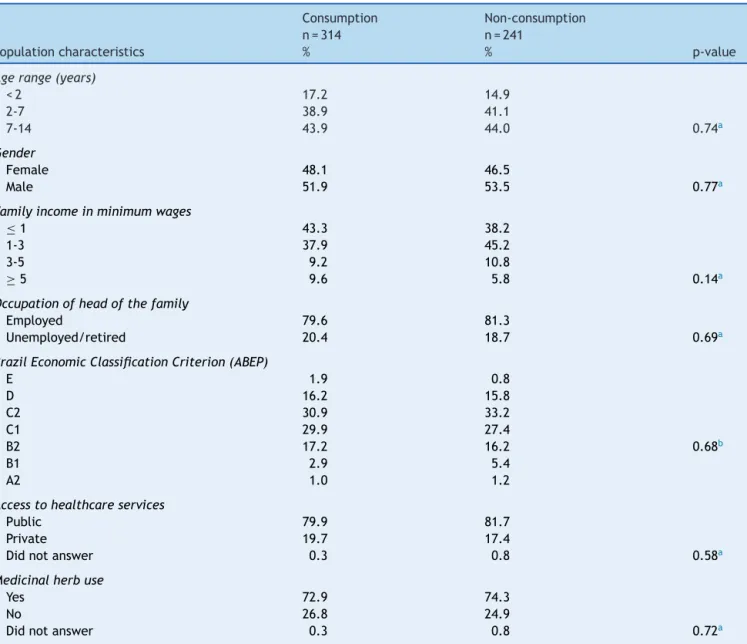
Table1 Distributionofsociodemographicvariablesaswellasofconsumptionandnon-consumptionofmedicationsonthe15 dayspriortothehouseholdinterview---ValedoJequitinhonhamunicipalities(MG),Brazil,2014.
Consumption Non-consumption
Populationcharacteristics
n=314 %
n=241
% p-value
Agerange(years)
<2 17.2 14.9
2-7 38.9 41.1
7-14 43.9 44.0 0.74a
Gender
Female 48.1 46.5
Male 51.9 53.5 0.77a
Familyincomeinminimumwages
≤1 43.3 38.2
1-3 37.9 45.2
3-5 9.2 10.8
≥5 9.6 5.8 0.14a
Occupationofheadofthefamily
Employed 79.6 81.3
Unemployed/retired 20.4 18.7 0.69a
BrazilEconomicClassificationCriterion(ABEP)
E 1.9 0.8
D 16.2 15.8
C2 30.9 33.2
C1 29.9 27.4
B2 17.2 16.2 0.68b
B1 2.9 5.4
A2 1.0 1.2
Accesstohealthcareservices
Public 79.9 81.7
Private 19.7 17.4
Didnotanswer 0.3 0.8 0.58a
Medicinalherbuse
Yes 72.9 74.3
No 26.8 24.9
Didnotanswer 0.3 0.8 0.72a
ABEP,Associac¸ãoBrasileiradeEmpresasdePesquisas. a Chi-squaredtest.
b Fisher’sexacttest.
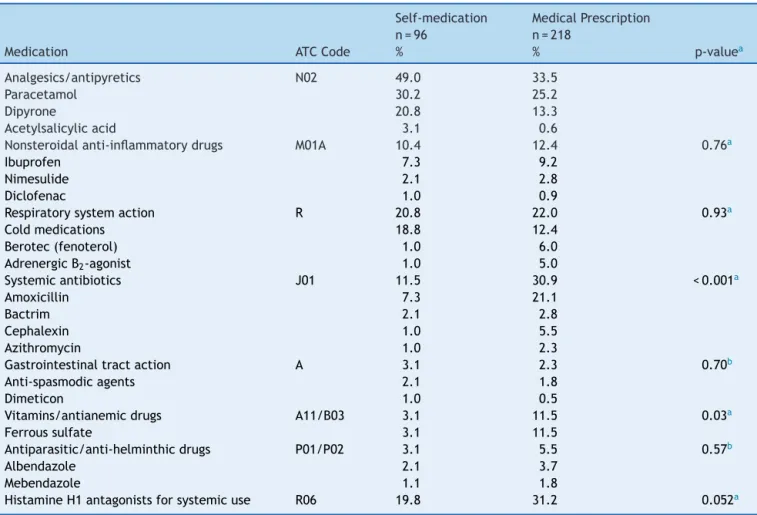
self-medicationusers,whiletheotherswerehigherincases ofmedicalprescription.Asforthedrug’sactiveagent,the authorshighlightthehighfrequencyofuseofparacetamol (30.2%),dipyrone(20.8%),andcoldmedicine(18.8%)in self-medicated individuals; in those receiving drugs according tothemedicalprescription, prevalentdrugs included his-tamineH1antagonist(31.3%), amoxicillin(21.1%),ferrous sulfate(11.5%),andibuprofen(9.2%)(Tables1-3;Fig.1).
Discussion
Theprevalenceofdruguseinchildrenupto14yearsofage estimatedinthisstudywas56.57%,basedonthemother’s recallperiodof 15days,similartoother Brazilianstudies inwhich itranged from48%to56%.6,8 Duetothe hetero-geneityofthemethodsusedinotherstudies,itisdifficult
tocomparethedata,astheagegroupinvestigatedandthe recallperiodvarysignificantly,aswellastheoriginofthe medicationuse.
Whilesomestudieshaveinvestigatedtheuseof medica-tionsbymedicalprescription,3othersassessedtheirusein self-medication.7,15 Somecharacteristicsofthisstudy sam-ple must be taken into account when comparing it with literaturedata,asthesocioeconomicconditionsareknown determinants of medication consumption.16,17 Therefore, wheninterpreting these data, itmust be considered that thestudiedpopulationlivesinalargegeographicalareain northernMinasGerais,andisslightlyeconomically hetero-geneous,notincludingthemoreprivilegedstrataofsociety regardingincome,education,andaccesstohealthcare ser-vices.
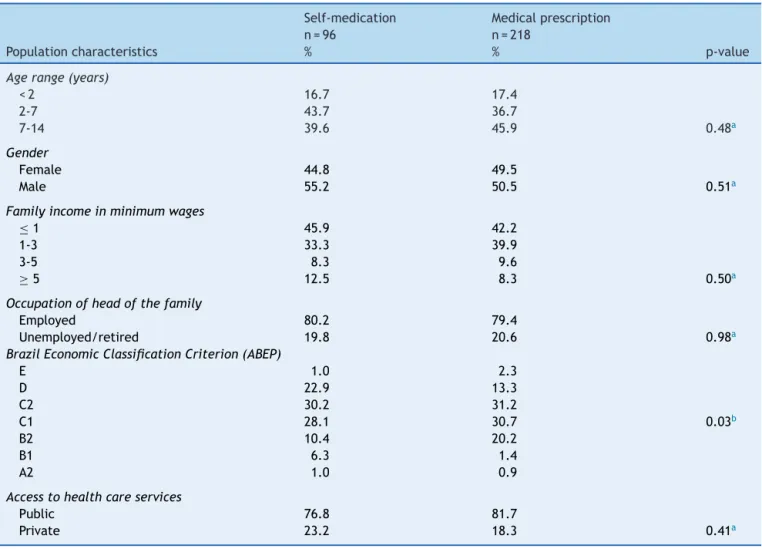
Table2 Distribution ofsociodemographic variables and of health care access, considering medication use through self-medicationandprescriptiononthe15dayspriortothehouseholdinterview-ValedoJequitinhonhamunicipalities(MG),Brazil, 2014.
Self-medication Medicalprescription
Populationcharacteristics
n=96 %
n=218
% p-value
Agerange(years)
<2 16.7 17.4
2-7 43.7 36.7
7-14 39.6 45.9 0.48a
Gender
Female 44.8 49.5
Male 55.2 50.5 0.51a
Familyincomeinminimumwages
≤1 45.9 42.2
1-3 33.3 39.9
3-5 8.3 9.6
≥5 12.5 8.3 0.50a
Occupationofheadofthefamily
Employed 80.2 79.4
Unemployed/retired 19.8 20.6 0.98a
BrazilEconomicClassificationCriterion(ABEP)
E 1.0 2.3
D 22.9 13.3
C2 30.2 31.2
C1 28.1 30.7 0.03b
B2 10.4 20.2
B1 6.3 1.4
A2 1.0 0.9
Accesstohealthcareservices
Public 76.8 81.7
Private 23.2 18.3 0.41a
ABEP,Associac¸ãoBrasileiradeEmpresasdePesquisas. aChi-squaredtest.
b Fisher’sexacttest.
associatedwithmedicationuseandareprobablyassociated with low family income, considered as a determinant of medicationuse:17individualswithincome≤threeminimum wagesconsume1.3timesmoremedicationthanthosewith income≥threeminimumwages.Furthermore,thesample wasrestricted totheurban areaof20municipalities with lowHDI,whosehouseholdincomewassupplementedbythe federalgovernmentincometransferprogram,andwhoare usersofthepublichealthcareservicenetwork.18
As reported by the mothers, 69.42% of the medica-tions used had been prescribed by physicians and 30.57% were given by the mothers at their own discretion. As previously demonstrated,19 there was a predominance of non-prescription medications administered to children by themothers.Thisattitudehasbeenattributedtosocialroles traditionallyassignedtomothers,amongthem,toprovide familyhealth.
Thetenmostoftenadministeredmedicationscomprised 77.16% of the total, with a predominance of anal-gesics/antipyretics,decongestants,iodinesyrups, expecto-rants, and mucolytics. The commercialization of medica-tionsinSwedenisunderstrictcontrol;however,inastudy
carriedoutinchildren,thetenmostpopulardrugs consti-tuted70%ofthetotal.20
Analgesics/antipyreticsareoftenusedinchildren, prob-ably becausefeveris acommonmanifestation, aswellas thetrivializationofuseofthisclassofmedicationsdueto unrestrictedcommercialization.Althoughmedicationssuch asparacetamolanddipyroneareanalgesicsand antipyret-icsofrelativelysafeuseinchildren,consideringappropriate doses,chronicandabusiveusemustbeprevented.21
Paracetamolandibuprofenareonthelistofchildren’s medicationsof theWHO.22 The safetyof dipyrone,a low-costanalgesic/antipyreticandpartofthelistofmedications subsidized by the federal government’s Popular Pharmacy program,hasbeenquestionedinseveralpartsoftheworld. ResultsoftheLatinstudy,amulticentercase-control study conductedinsevenlocationsinBrazil,twoinArgentina,and oneinMexico,indicatealowincidenceofaplasticanemia (1.6 cases per one million inhabitants/ year) and lack of associationwithdipyrone.23
Table3 Main medicationsfound in home pharmacies, according to groups andsubgroups ofthe AnatomicalTherapeutic Chemical(ATC/WHO)classificationandthepatternsofuseonthe15dayspriortothehouseholdinterview-ValedoJequitinhonha municipalities(MG),Brazil,2014.
Self-medication MedicalPrescription
Medication ATCCode
n=96 %
n=218
% p-valuea
Analgesics/antipyretics N02 49.0 33.5
Paracetamol 30.2 25.2
Dipyrone 20.8 13.3
Acetylsalicylicacid 3.1 0.6
Nonsteroidalanti-inflammatorydrugs M01A 10.4 12.4 0.76a
Ibuprofen 7.3 9.2
Nimesulide 2.1 2.8
Diclofenac 1.0 0.9
Respiratorysystemaction R 20.8 22.0 0.93a
Coldmedications 18.8 12.4
Berotec(fenoterol) 1.0 6.0
AdrenergicB2-agonist 1.0 5.0
Systemicantibiotics J01 11.5 30.9 <0.001a
Amoxicillin 7.3 21.1
Bactrim 2.1 2.8
Cephalexin 1.0 5.5
Azithromycin 1.0 2.3
Gastrointestinaltractaction A 3.1 2.3 0.70b
Anti-spasmodicagents 2.1 1.8
Dimeticon 1.0 0.5
Vitamins/antianemicdrugs A11/B03 3.1 11.5 0.03a
Ferroussulfate 3.1 11.5
Antiparasitic/anti-helminthicdrugs P01/P02 3.1 5.5 0.57b
Albendazole 2.1 3.7
Mebendazole 1.1 1.8
HistamineH1antagonistsforsystemicuse R06 19.8 31.2 0.052a
a Chi-squaredtest. b Fisher’sexacttest.
reviewshaveshownthatthereisinsufficientevidencethat thesemedicationsshowgreaterbenefitthanplacebointhe treatmentofsymptomscausedbyupperairwayrespiratory infections,suchasnasalcongestionandrhinorrhea associ-atedwiththecommoncold24andacutecough.25
Although some of the medications used to treat the respiratory tract, such as dexchlorpheniramine and the association of phenylephrine-brompheniramine are con-traindicated for children younger than two years, it was observedthatapproximately17.18%ofchildrenusingthese medicationswereinthisagegroup.8,26,27Inadditiontothe intrinsicadverseeffectsofeachactivesubstance,thereare otherfactorsthatcanmakethempotentiallydangerousfor thisagegroup,includingtheincorrectdoseinterpretation ordoseinterval,useofinappropriatedispensingmeasures, orthesimultaneousadministrationofseveralmedications, inordertoachievegreatersymptomrelief.8,22
Theauthorsalsoemphasizethesignificantuseof nime-sulideanddiclofenacinchildrenyoungerthan1year,anage groupforwhichthemedicationiscontraindicated.The effi-cacyandsafetyofthisdrugforuseinpediatricpatientshas yettobeestablished.8,27
Inthisstudy,thehighpercentageofmedicinalherband plant use (74.9%) is noteworthy, corresponding to 37.7% teas and 37% infusions. Even if the evidenceof safety or
effectivenessofcomplementary therapiesis limitedwhen compared to conventional therapies, such products are generallyconsidered safe and/or natural by the parents, whoadministerthemtotheirchildrenwithorwithoutthe doctor’s awareness.28 The results of this study show the importanceofastudytounderstandthepsychologicaland socioculturalaspectsthatexplainthereasonswhyparents feelencouragedtousetheseresourcestoeasethe discom-fortoftheirchildren.
Antibiotics arethesecond most often usedmedication subgroupin theinvestigatedsample. Inseveral studies,1,4 antibiotics appear in the list of the most common drugs used by children, especially those receiving prescribed medications.8 Itis knownthat themain respiratory infec-tions areresponsible for a large proportionof outpatient antimicrobialprescriptions,demonstratingtheintendeduse ofantibiotics.29Amongthemoststudiedantibiotics, amox-icillinwasthemostoftenusedbychildren,andsimilarto resultswerefoundbyotherresearchers.8Amoxicillinis men-tionedininternationalguidelinesasfirstchoiceoftreatment for themost common childhoodinfections, suchasacute otitismedia,sorethroats,andsinusitis.1
commonly used medications in the sample (paracetamol, amoxicillin,ibuprofen,anddipyrone)havegood documen-tation for pediatric use, although their indication is not recommendedforsomeageranges.8,26,27
Moreover, drugs used for the treatment of respiratory tractdiseasesshowlittleevidenceofefficacy,asmentioned previously.Oneofthemostimportantfactorstobe consid-eredinassessingtheavailableevidenceinpediatricsishow todealwiththeethicalissuesofchildprotectionwhen per-formingcontrolledclinicaltrials.Bydefinition,thesealways involvesome degreeofrisk, whichinpediatricsshouldbe assumedby parents, basedonpotentialbenefits thatwill notbeimmediatelyavailabletotheirownchildren.
Despite the benefits that the pharmaceutical industry providesindrugdevelopmentforadults,itisimportantto emphasize thateconomic motivation is notprominent for pediatricuse.
The reduced drug market for the pediatric age range when compared to other ranges, such as adults and the elderly,inadditiontothedifficultiesinherenttoperforming clinicaltrialsinchildren,makesthedevelopmentofthese drugsunattractive tothe pharmaceuticalindustry.30 How-ever,asproposedbyCoelhoetal.,theuseofaspecificlist ofessentialdrugsmaybepartofacomprehensivepolicyto stimulatethedevelopmentandmanufacturingofmedicines forchildreninBrazil.9
Some limitations of the present study should be con-sidered. The household survey is subject to biases from interviewersand interviewees,which are notalways pos-sible tocontrol. The period in which data collection was conducted,April toJuly of 2013,coincided withthe win-terseasonintheregion,whenthereisincreasedincidence of viral diseases and respiratory infections, which may have contributed to the higher consumption of certain drugclasses, suchas analgesics, antipyretics, antibiotics, antitussives, expectorants, mucolytics, and antiasthmatic drugs.26
Inthepresentstudy,datacollectionstandardization fol-lowed some procedures aimed at minimizing recall bias, includingthe15-day recallperiod,to evaluatetheuse of medicines in children and request that the drug package and/ordrugprescriptionbepresented.
The prevalence found in this study corroborates the resultsoftheliterature,whichindicateahighconsumption ofmedicationbychildren.Itisalsoimportanttounderstand thatmedicationuseappearstobeassociatedtolow-income, asitissubsidizedbythegovernment.
Moreover,childrenaged0to14years,ingeneral,arein aphaseinlifewhenhealthproblemsthatrequiretheuseof medicationsshouldconsiderindicationandagerestrictions. The use of medications, in addition to being an indica-torofhealthproblems,alsoreflectssocialinequalitiesand deficiencies,qualityofthehealthcaresystem,regulations relatedtomedicationsinthecountry, medicaleducation, cultural habits, and the pharmaceutical market composi-tion,amongothersfactors.
Theepidemiologicalrealityofmedicationuseshouldbe consideredbyhealthcareprofessionalsandmanagersto cre-ateeducationalprograms.In thissense, thenursing work processstartswithdrugprescription in primarycare,and mayinvolvestudiesofpharmacoepidemiologyand pharma-covigilanceinordertounderstandtheconsumptionprofile,
resultinginknowledgethatwillallowinterventionsaimed atpromotingrationaluseofmedications.
Funding
Fundac¸ãodeAmparoàPesquisadoEstadodeMinasGerais (FAPEMG-Processn.CDS-APQ-02522-11).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The authors would like to thank the interviewers (Alex, Lays,and Guilherme),theinterviewedfamilies,and Prof. Dr.Delba.
References
1.SantosDB, Barreto ML, CoelhoHL. Druguse and associated factors in children living in poor areas. Rev Saude Publica. 2009;3:768---78.
2.deAquinoDS.Porqueousoracionaldemedicamentosdeveser umaprioridade?CienSaudeColet.2008;13:733---6.
3.StraandJ,RokstadK,HeggedalU.Drugprescribingforchildren ingeneralpractice.AreportfromtheMøre&Romsdal Prescrip-tionStudy.ActaPaediatr.1998;87:218---24.
4.ClavennaA, Bonati M.Drugprescriptions to outpatient chil-dren: a review of the literature. Eur J Clin Pharmacol. 2009;65:749---55.
5.StephensonT.ThemedicinesforchildrenagendaintheUK.Br JClinPharmacol.2006;61:716---9.
6.Béria JU, Victora CG, Barros FC, Teixeira AB, Lombardi C. Epidemiology of drug consumption in children of a urban center ofthe southern regionof Brazil. Rev SaudePublica. 1993;27:95---104.
7.PereiraFS,BucaretchiF,StephanC,CordeiroR.Self-medication inchildrenandadolescents.JPediatr(RioJ).2007;83:453---8.
8.Moraes CG, Mengue SS, Tavares NUL, Pizzol TSD. Utilizac¸ão de medicamentos entre crianc¸as de zero a seis anos: um estudodebasepopulacionalnosuldoBrasil.CienSaudeColet. 2013;18:3585---93.
9.CoelhoHL1,ReyLC,MedeirosMS,BarbosaRA, CruzFonseca SG,CostaPQ.AcriticalcomparisonbetweentheWorldHealth Organizationlistof essentialmedicines for childrenand the Brazilianlistofessential medicines(Rename).JPediatr (Rio J).2013;89:171---8.
10.GomesMF.Estudoda automedicac¸ãoinfantil emuma região administrativanomunicípiodo RiodeJaneiro [dissertation]. RiodeJaneiro:UniversidadeFederaldoRiodeJaneiro.2000.
11.InstitutoBrasileirodeGeografiaeEstatística(IBGE).Populac¸ão eDomicílios-Censo 2010comDivisãoTerritorial2001,Minas Gerais. 2010. [cited 02 Oct 2011]. Available from: http:// downloads.ibge.gov.br/downloadsgeociencias.htm
12.WHO Collaborating Centre for Drug Statistic Methodology. ATC/DDD Index 2014. [cited 15 Jan 2014]. Available from:
http://www.whocc.no/atcdddindex
13.Associac¸ãoBrasileiradeEmpresasePesquisas(ABEP).Critério Brasil de Classificac¸ão Econômica 2013 [cited20 Mar 2014]. Availablefrom:http://www.abep.org/new/criterioBrasil.aspx
15.Du Y, Knopf H. Self-medication among children and ado-lescents in Germany: results of the National Health Survey for Children and Adolescents(KiGGS). Br J Clin Pharmacol. 2009;68:599---608.
16.Bertoldi AD, Barros AJ, Hallal PC, Lima RC. Utilizac¸ão de medicamentosemadultos:prevalênciaedeterminantes indi-viduais.RevSaudePublica.2004;38:228---38.
17.ArraisPS,BritoLL,BarretoML,CoelhoHL.Prevalênciaefatores determinantesdoconsumodemedicamentosnoMunicípiode Fortaleza,Ceará.BrasilCadSaudePublica.2005;21:1737---46.
18.Instituto de Pesquisa Econômica Aplicada --- IPEA. Atlas do DesenvolvimentoHumanodoBrasil2013.MunicípioseFaixade DesenvolvimentoHumano.[cited18Jan2013].Availablefrom: http://www.atlasbrasil.org.br/2013
19.BricksLF,LeoneC.Utilizac¸ãodemedicamentosporcrianc¸as atendidasemcreches.RevSaudePublica.1996;30:527---35.
20.Al-WindiA,ElmfeldtD,SvärdsuddK.Determinantsofdrug uti-lizationinaSwedishmunicipality.PharmacoepidemiolDrugSaf. 2004;13:97---103.
21.BricksLF.Usojudiciosodemedicamentosemcrianc¸as.JPediatr (RioJ).2003;79:S107---14.
22.WorldHealth Organization (WHO). Who model listof essen-tial medicines for children 2013. [cited 17 Jan 2014]. Available from:http://www.who.int/medicines/publications/ essentialmedicines/18thEMLFinalweb8Jul13.pdf
23.MalufE,Hamerschlak N,CavalcantiAB,JúniorAA, Eluf-Neto J,FalcãoRP,etal.Incidenceandriskfactorsofaplastic ane-miainLatinAmericancountries:theLATINcase-controlstudy. Haematologica.2009;94:1220---6.
24.DeSutterAI,Lemiengre M,CampbellH. Withdrawn: antihis-tamines for thecommon cold.Cochrane Database Syst Rev. 2009;(4.).
25.Susan M, Smith KS, Fahey T. Over-the-counter (OTC) medi-cationsfor acutecoughinchildrenand adultsinambulatory settings.TheCochraneLibrary.2011:8.
26.Pitrez PM, Pitrez JL. Acute upper respiratory tract infec-tions: outpatientdiagnosis and treatment.JPediatr (Rio J). 2003;79:S77---86.
27.DRUGDEX® System. Thomson MICROMEDEX. 2010. [cited 13 Oct 2010]. Available from: http://www.thomsonhc.com/ home/dispatch
28.Gentil LB, Robles AC, Grosseman S. Use of complementary therapiesbymothersintheirchildren:studyatanuniversity hospital.CienSaudeColet.2010;15:1293---9.
29.Oliveira EA, Bertoldi AD, Domingues MR, Santos IS, Bar-ros AJ. Medicine use from birth to age two years: the 2004 Pelotas (Brazil) Birth Cohort study.Rev Saude Publica. 2010;44:591---600.