www.jped.com.br
ORIGINAL
ARTICLE
Comparison
of
two
maintenance
electrolyte
solutions
in
children
in
the
postoperative
appendectomy
period:
a
randomized,
controlled
trial
夽
Maria
Clara
da
Silva
Valadão
a,b,∗,
Jefferson
Pedro
Piva
c,d,
João
Carlos
Batista
Santana
a,e,f,
Pedro
Celiny
Ramos
Garcia
g,haPontifíciaUniversidadeCatólicadoRioGrandedoSul(PUCRS),PortoAlegre,RS,Brazil
bHospitalUniversitáriodeSantaMaria(HUSM),UniversidadeFederaldeSantaMaria(UFSM),SantaMaria,RS,Brazil cFaculdadedeMedicina,UniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
dEmergencyandPediatricIntensiveMedicineService,HospitaldeClínicasdePortoAlegre(HCPA),UniversidadeFederaldoRio
GrandedoSul(UFRGS),PortoAlegre,RS,Brazil
eUniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
fHospitalSãoLucas,PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUCRS),PortoAlegre,RS,Brazil gUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
hPediatricService,HospitalSãoLucas,PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUCRS),PortoAlegre,RS,Brazil
Received26May2014;accepted11November2014 Availableonline23April2015
KEYWORDS
Hyponatremia; Hypernatremia; Fluidtherapy; Isotonicsolutions; Hypotonicsolutions; Postoperativeperiod
Abstract
Objective: Tocomparetwoelectrolytemaintenancesolutionsinthepostoperativeperiodin childrenundergoingappendectomy,inrelationtotheoccurrenceofhyponatremiaandwater retention.
Methods: Arandomizedclinicalstudyinvolving50pediatricpatientsundergoingappendectomy, whowererandomizedtoreceive2,000mL/m2/dayofisotonic(Na150mEq/Lor0.9%NaCl)or
hypotonic(Na30mEq/LNaClor0.18%)solution.Electrolytes, glucose,urea,andcreatinine weremeasuredatbaseline,24h,and48haftersurgery.Volumeinfused,diuresis,weight,and waterbalancewereanalyzed.
Results: Twenty-fourpatientshadinitialhyponatremia;inthisgroup,13receivedhypotonic solution. Seventeen patients remained hyponatremic 48h after surgery, of whom ten had receivedhypotonicsolution.Inbothgroups,sodiumlevelsincreasedat24h(137.4±2.2and 137.0±2.7mmol/L),withnosignificantdifferencebetween them (p=0.593).Sodiumlevels
夽
Pleasecitethisarticleas:ValadãoMC,PivaJP,SantanaJC,GarciaPC.Comparisonoftwomaintenanceelectrolytesolutionsinchildren inthepostoperativeappendectomyperiod:arandomized,controlledtrial.JPediatr(RioJ).2015;91:428---34.
∗Correspondingauthor.
E-mail:[email protected](M.C.d.S.Valadão).
http://dx.doi.org/10.1016/j.jped.2015.01.004
48haftersurgerywere136.6±2.7and136.2±2.3mmol/Linisotonicandhypotonicgroups, respectively,withnosignificantdifference.Theinfusedvolumeandurineoutputdidnotdiffer betweengroupsduringthestudy.Thewaterbalancewashigherintheperiodbeforesurgeryin patientswhoreceivedhypotonicsolution(p=0.021).
Conclusions: Inthepost-appendectomyperiod,theuseofhypotonicsolution(30mEq/L,0.18%) didnotincreasetheriskofhyponatremiawhencomparedtoisotonicsaline.Theuseofisotonic solution(150mEq/L,0.9%)didnotfavorhypernatremiainthesepatients.Childrenwhoreceived hypotonicsolutionshowedhighercumulativefluidbalanceinthepreoperativeperiod ©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Hiponatremia; Hipernatremia; Hidratac¸ão; Soluc¸õesisotônicas; Soluc¸õeshipotônicas; Pós-operatório
Comparac¸ãodeduassoluc¸õesparamanutenc¸ãohidroeletrolíticanopós-operatório
deapendicectomiaemcrianc¸as:umestudocontroladoerandomizado
Resumo
Objetivo: Compararduassoluc¸õesdemanutenc¸ãohidroeletrolíticanoperíodopós-operatório (PO)decrianc¸assubmetidasàapendicectomia,quantoàocorrênciadehiponatremiaeretenc¸ão hídrica.
Métodos: Estudoclínicorandomizadoenvolvendo50pacientespediátricossubmetidosà apen-dicectomia,randomizadosareceber2000ml/m2/diadesoluc¸ãoisotônica(Na150mEq/Lou
NaCl0,9%)ouhipotônica(Na30mEq/LouNaCl0,18%).Eletrólitos,glicose,ureiaecreatinina forammensuradosnoiníciodoestudo,24e48horasapósacirurgia.Foramanalisadosvolume infundido,diurese,pesoebalanc¸ohídrico.
Resultados: 24 pacientes apresentaram hiponatremia inicial, destes 13 receberam soluc¸ão hipotônica. Dezessetepacientespermaneceramhiponatrêmicas 48horasapósacirurgia,10 haviamrecebidosoluc¸ãohipotônica. Nosdoisgruposos níveisde sódioaumentaram na24a
hora PO(137,4±2,2e137,0±2,7),não havendodiferenc¸aentreeles(p=0,593).Níveisde sódio48hapósacirurgiaforam136,6±2,7e136,2±2,3nogrupoisotônicoehipotônico respec-tivamentesemdiferenc¸asignificativa.Osvolumesinfundidosediuresenãodiferiramentreos gruposduranteoestudo.Obalanc¸ohídricofoimaiornoperíodoanterioràcirurgianogrupode pacientesquereceberamsoluc¸ãohipotônica(p=0,021).
Conclusões: Noperíodopós-apendicectomia,ousodasoluc¸ãohipotônicanãoaumentouorisco dehiponatremia,quandocomparadoaumasoluc¸ãosalinaisotônica.Ousodasoluc¸ãoisotônica nãofavoreceuahipernatremianestespacientes.Crianc¸asquereceberamsoluc¸ãohipotônica apresentarammaiorbalanc¸ohídricocumulativonoperíodopré-operatório.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Hyponatremia is an electrolyte disorder commonly seen in hospitalized patients, defined as serum sodium lev-els<136mmol/L.1---5 Its etiology has been related to fluid retention. If the infused fluid volume exceeds that of renal excretion capacity, dilution of extracellular solutes reduces osmolarity.1 The presence of hypotonicity pro-motes cerebral edema due to imbalance between the intracellular and extracellular osmolarity in neuronal tis-sue.Intheoccurrenceof acutedecreasein serumsodium (Na+< 130mmol/L), extracellular water penetrates the nervecells,aimingtoequalizetheintra-andextra-cellular tonicities.2,6
ThemaintenancesolutionproposedbyHolliday&Segar in 1957, still widely used, was based on the metabolism of healthy children and calculated basedon body weight (<10kg, 11-20kg,>20kg;3mEq/LofNa+ and2 mEq/Lof K+), resulting in a hypotonic solution and excessive fluid
intakeforcritically-illchildren,whichmaycausetheonset of hyponatremia.7,8 The presence of stress (pain, fever, surgery),nausea,vomiting,anesthesia,intestinal manipula-tion,andhypovolemiaarenon-osmoticstimulithatincrease thesecretionandactivityoftheantidiuretichormone(ADH) (argininevasopressin).1 HighADH action limitsfreewater excretion and acute disease leads to the production of endogenouswater,increasingtheextracellularvolumeand resultinginorworseningtheoccurrenceofhyponatremia.9 A recent review involving more than 500 children in six prospectivestudiesshowedthattheuseofisotonicsolutions prevents hyponatremia in the postoperative (PO) period and that the use of hypotonic fluids results in decreased sodium.10
and neurological complications in previously healthy patients.
The use of isotonic solutions during and after surgery hasbeen suggestedasameantopreventhyponatremiain thePOperiod.13,14Someauthorsdefendthattheincidence ofhyponatremiamaybeassociatedwiththeadministered solutionvolumeratherthanitssodiumcontent.15Moreover, a prospective, randomizedtrial comparedisotonic versus hypotonicintravenousfluidandmaintenancevolumesof50% or100%,andconcludedthattherisk ofhyponatremiawas lowerwiththeuseofisotonicsalinesolutionandnotbyuse ofwaterrestriction.13
Inthe lastdecade,theprevention ofhospital-acquired hyponatremiahasbeensystematicallydebated,withsome authors strongly recommending the use of isotonic solu-tion,whereasothersrecommendtheuseofisotonicfluids associatedwithwaterrestriction.6,16Othersopposetheuse ofisotonicfluid,claimingthathyponatremiaismainlythe resultofhemodilutionand,therefore,fluidrestrictioncould preventhyponatremia.17 Theaimofthisstudywasto com-pare the use of hypotonic and isotonic solutions in fluid maintenance(2,000mL/m2)inthepre-operativeand post-operative periods in children and adolescents undergoing appendectomy.
Methods
BetweenMarchof2012andJanuaryof2013,aprospective, double-blind,randomizedtrial wasconducted after being approved by the Research Ethics Committee of Pontifícia UniversidadeCatólicadoRioGrandedoSul(CEP11/05688) andtheDepartmentofTeachingandResearchofthe Hospi-talUniversitáriodeSantaMaria,wheredatacollectionwas performed. Aninformedconsent wassignedby the childs parent/guardianprior tostudy enrollment, and whenever possible,theinformedconsentwasalsosignedbythechild. Childrenaged1-14yearswithadiagnosisofacute appen-dicitis and eligiblefor surgical treatment were included. Thetypeofappendicitiswasclassifiedasnon-complicated incaseswheretheappendixwasintactorcomplicatedwhen therewasorganperforationand/orperitonitis.Thepatients wereweighedonadmissionand48hafterthesurgical pro-cedure. Patients that had severe hemodynamic disorder, shock,and/orwerereceivingvasoactivedrugsonadmission wereexcluded.
Participantswererandomlyassignedtoreceiveisotonic or hypotonic solution at the time of admission to the pediatricemergencyroom.Aimingtomaintainabalanced allocationinbothgroupsatalltimesofthestudy, random-ization wasperformed in groups of ten patients, five for eachofthesolutions.Theresearcherandmedicalassistants were blinded tothe solution contentand the emergency nursing staffprepared the solutions, labeledA or B,plus theinfusioninmL/hour.Theisotonicsolutioncontained150 mEq/L of sodium chloride, 30 mEq/L of potassium chlo-ride,and5% glucose,whereasthehypotoniccontained30 mEq/Lofsodiumchloride,withthesamecontentofglucose andpotassium.Thetotalinfusedvolumeestimatedforboth solutionswas2,000mL/m2/24h(Fig.1).
Test collection wasperformed at the time of random-ization.Allpatientsreceivedinitialfluidlossreplacement
with0.9%salinesolutionwithavolumeof20mL/kgbefore the specific solutions.The infusion during the intraopera-tiveperiodwasperformedwith0.9%saline,withthevolume established by the anesthesiologist and considered in the totalvolumeofthestudy.
Thesolutionwasadministeredfromadmissionto48hof thePOperiod,exceptfortheperioperativeperiod.Samples forlaboratorytests(Na+,K+,Ca++,chloride,glucose,urea, creatinine, and bicarbonate levels)were collected at the startoftheinfusion,24h,and48haftersurgery,andthen analyzedbytheion-selectivemethod.Diuresisandfluid bal-ancewereperformedatthreeintervals:fromadmissionto surgery, surgery to24h, and 24h to 48h after appendec-tomy.Theothermeasuresofpatientcarewereperformed bytheassistingmedicalteam.
The primary endpoint wasserum sodium levels during the intervention and at the end of 48h of the protocol. Hypernatremia was defined asserum Na>145 mEq/L and hyponatremiaasserumNa<136mEq/L.Moderate hypona-tremiawasconsideredwhenserumNawasbetween130and 135mEq/L,andsevere when<130 mEq/L.Secondary out-comes were the presence of hypervolemia (estimated by the cumulativepositive fluidbalance and/or weightgain) andthepresenceofotherelectrolytedisturbances.
Quantitative variables with normal distribution were expressed asmean and standard deviation and compared byStudent’st-test,whereasvariableswithoutanormal dis-tribution were compared using the Mann-Whitney Utest. Categorical variableswereshown asabsoluteandrelative frequencies and association was verified using the chi-squaredtest.Valueswereconsideredstatisticallysignificant with p-values<0.05. The analyses were performed using SPSS(SPSSInc.Released2008.SPSSStatisticsforWindows, Version17.0.Chicago,USA).
Results
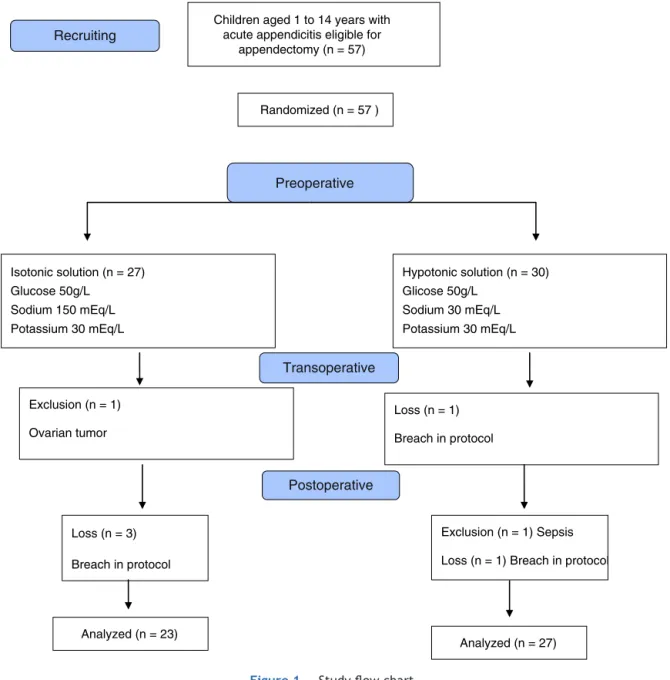
During the study period,a total of 57 children aged1 to 14yearssubmittedtoappendectomywereadmitted.These individuals were randomized to receive intravenous iso-tonic orhypotonic maintenancesolution.Onepatientwas excluded in the isotonic group due to ovarian tumor and therewerethreelossesduetoprotocolbreach,totaling23 patientsinthisgroup.Onepatientwasexcludedfromthe hypotonic groupdue tosepsisand thereweretwolosses, resultingin27subjects.Initialsodiumwasnotmeasuredin onepatientandinfourpatientsafter24h.
Theanthropometriccharacteristicsweresimilarinboth groups (Table 1). Foreach individual,sodiumlevels were measured at admission, after 24h, and after 48h. There werenosignificantdifferencesbetweenthethree measure-mentperiods.Atadmission,24(49%)patientshadmoderate hyponatremia(Na+>130and<135mEq/L)and25(51%)had normalsodium(Na>136mEq/L).
After24h,12patientshadhyponatremia,ofwhomseven hadreceivedhypotonicsolution.After48h,17childrenhad hyponatremia, of whom ten hadreceived hypotonic solu-tion. The anthropometric and biochemicalcharacteristics areshowninTables1and2,respectively.
Children aged 1 to 14 years with acute appendicitis eligible for
appendectomy (n = 57)
Loss (n = 3)
Breach in protocol Exclusion (n = 1)
Ovarian tumor Isotonic solution (n = 27) Glucose 50g/L
Sodium 150 mEq/L Potassium 30 mEq/L
Loss (n = 1)
Breach in protocol
Hypotonic solution (n = 30) Glicose 50g/L
Sodium 30 mEq/L Potassium 30 mEq/L
Exclusion (n = 1) Sepsis
Loss (n = 1) Breach in protocol Preoperative
Postoperative Transoperative Randomized (n = 57 ) Recruiting
Analyzed (n = 23)
Analyzed (n = 27)
Figure1 Studyflowchart.
Table1 Characteristicsofthetwogroupsofpatientsundergoingappendectomyaccordingtotheadministeredsolution.
Isotonic(n=23) Hypotonic(n=27) p
Age,years;mean,SD 8.8±3.6 10.3±2.9 0.106a
Weight,kg;mean,SD 35.1±14.0 37.1±12.2 0.596a
Malegender,n(%) 13(43.3%) 17(56.7%) 0.643b
BMI;mean,SD 18.5±3.4 20.7±4.7 0.205c
Complicatedappendicitis,n(%) 14(45.1%) 17(54.9%) 0.879b
Non-complicatedappendicitis,n(%) 9(47.4%) 10(52.6%) 0.880b
Preoperativefasting,hours,IQ 5(3-9) 6(4-12) 0.190a
Postoperativefasting,hours,IQ 33(25-48) 38(28-48) 0.748a
Hospitallengthofstay,days,IQ 6(4-8) 6(5-7) 0.745a
SD,standarddeviation;BMI,bodymassindex;IQ,interquartilerange. p-valuesbasedontest.
Table2 Initialelectrolytesandosmolarity24and48hoursPO.
Isotonic(n=23) Hypotonic(n=27) Pa
InitialNa(mEq/L)49/50;mean,SD 135.7±3.3 135.8±2.9 0.882
24hNa(mEq/L)46/50;mean,SD 137.4±2.2 137.0±2.7 0.548
48hNa(mEq/L)50/50;mean,SD 136.6±2.7 136.2±2.3 0.593
InitialK(mEq/L)49/50;mean,SD 3.9±0.4 3.9±0.4 0.846
24hK(mEq/L)46/40;mean,SD 4.0±0.4 4.2±0.3 0.093
48hK(mEq/L)50/50;mean,SD 4.3±0.4 4.2±0.3 0.405
InitialCl(mEq/L)45/50;mean,SD 100.3±2.3 99.0±3.5 0.162
24hCl(mEq/L)46/50;mean,SD 103.2±2.5 101.4±2.7 0.797
48hCl(mEq/L)48/50;mean,SD 101.0±3.0 99.7±2.2 0.085
Initialcreatinine(mg/dL)49/50;mean,SD 0.6±0.1 0.6±0.1 0.157
24hcreatinine(mg/dL)46/50;mean,SD 0.5±0.1 0.5±0.1 0.797
48hcreatinine(mg/dL)50/50;mean,SD 0.5±0.2 0.6±0.2 0.146
24hosmolarity(mOsm/L)42/50;mean,SD 281.7±4.5 280.2±5.4 0.356
48hosmolarity(mOsm/L)50/50;mean,SD 279.5±5.9 279.3±4.2 0.853
SD,standarddeviation.
ap-valuesbasedonStudent’st-test.
betweenadmissionandthe24-hourmeasurement,whereas thegrouptreatedwithhypotonicsolutionhadanincrease of1.2mEq/L.Betweenthe24-and48-hourmeasurements, therewasadecreaseof0.8mEq/Linbothgroups.Between theinitial Na+ and finalNa+ (48h), therewasan increase
of 0.9 mEq/L in the isotonic group and of 0.4 mEq/L in hypotonic group. These differences were not significant (Table3).
Inthegroupofeightpatientswithnormalinitialsodium (>136mEq/L) andlowfinal sodium(<135 mEq/L),three receivedisotonicandfivereceivedhypotonicsalinesolution withaninitialvariationof136to140mEq/Landfinal(48h) of132to135mEq/L.
Inthegroupadmittedwithlowsodium(130-135mEq/L), ninechildren remained hyponatremic(132-135 mEq/L) at theend,ofwhomfourhadreceivedisotonicsolution,and fivehypotonicsolution.
Of the 15 patients that hadinitial hyponatremia (130-135mEq/L)andnormalNa+at48h(136-140mEq/L),seven receivedisotonicsolutionandeighthypotonicsolution.
Of the 17 patients that showednormal sodiumlevels, eightreceivedisotonicandninehypotonicsolution.
Regardingsodiumevolutionfrom24to48hPO,eight chil-dren had normal sodium (136-142 mEq/L) after 24h, but had hyponatremia after 48h (132 to 135 mEq/L); half of themreceivedisotonicsolution,andhalfreceivedhypotonic solution.
Eight patients remained hyponatremic (24h: 131-135 mEq/Land48h:132-135mEq/L);fourreceivedisotonicand fourhypotonicsolution.Theother 30childrenhadnormal sodium48haftersurgery.Sodiumlevelmeasurementswere notperformedinfourpatients24haftersurgery.
Four children required volume expansion in the PO period: three from the isotonic group and one from the hypotonicgroup;noneofthechildrenrequiredelectrolyte correction.
Bothgroups(isotonicandhypotonic)showedweightgain during the first 48h, but with no significant differences betweenthem.However,thefluidbalanceinthe preoper-ativeperiodwassignificantlyhigherinthegroupreceiving
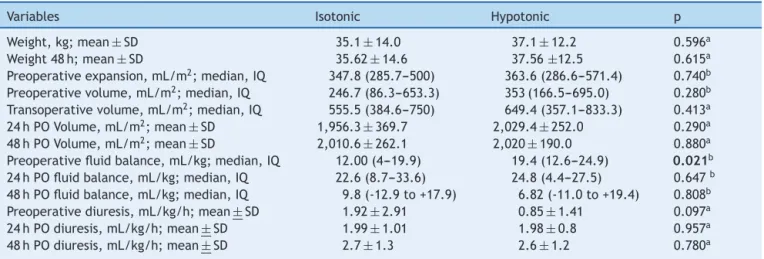
Table3 Infusedvolumes,fluidbalance,anddiuresisinbothgroups.
Variables Isotonic Hypotonic p
Weight,kg;mean±SD 35.1±14.0 37.1±12.2 0.596a
Weight48h;mean±SD 35.62±14.6 37.56±12.5 0.615a
Preoperativeexpansion,mL/m2;median,IQ 347.8(285.7---500) 363.6(286.6---571.4) 0.740b
Preoperativevolume,mL/m2;median,IQ 246.7(86.3---653.3) 353(166.5---695.0) 0.280b
Transoperativevolume,mL/m2;median,IQ 555.5(384.6---750) 649.4(357.1---833.3) 0.413a
24hPOVolume,mL/m2;mean±SD 1,956.3±369.7 2,029.4±252.0 0.290a
48hPOVolume,mL/m2;mean±SD 2,010.6±262.1 2,020±190.0 0.880a
Preoperativefluidbalance,mL/kg;median,IQ 12.00(4---19.9) 19.4(12.6---24.9) 0.021b
24hPOfluidbalance,mL/kg;median,IQ 22.6(8.7---33.6) 24.8(4.4---27.5) 0.647b
48hPOfluidbalance,mL/kg;median,IQ 9.8(-12.9to+17.9) 6.82(-11.0to+19.4) 0.808b
Preoperativediuresis,mL/kg/h;mean±SD 1.92±2.91 0.85±1.41 0.097a
24hPOdiuresis,mL/kg/h;mean±SD 1.99±1.01 1.98±0.8 0.957a
48hPOdiuresis,mL/kg/h;mean±SD 2.7±1.3 2.6±1.2 0.780a
hypotonicsolution(median19.4ml/kg;IQ:12.6---24.9)than inthegroupreceivingisotonicsolution(median12.0ml/kg, IQ:4---19.9)(p=0.021).Duringthisinterval,whichwas sim-ilarin bothgroups, theisotonicgroup showedatendency towardshigherdiuresis(p=0.097).
Volume expansion after surgery was necessary in four patients:threereceivingisotonicsolutionandonefromthe hypotonicgroup.On thesecond dayof protocol,only one patient receiving isotonic solution required rapid volume expansion,whichwascarriedoutusingsalinesolution(0.9% NaCl).
Discussion
In this double-blind, randomized study involving children submittedtoappendectomy,it wasobservedthat: (a)the administrationof hypotonic maintenancesolution did not increasethechanceofhyponatremiawhencomparedtothe isotonicsolution;(b)theinfusionofisotonicsolutiondidnot preventtheonsetofhyponatremiainthePOperiodanddid notincreasetheoccurrenceofhypernatremiainthisperiod; (c)mostofthegroupwhohadhyponatremiaatadmission(24 patients)hadsodiumlevelsnormalized(n=15)irrespective ofthetypeofadministeredsolution;(d) fluidretentionin thepreoperativeperiodwashigherinpatientsthatreceived thehypotonicsolution.
These findings donot supportthe results ofthe inves-tigationbyChoongetal.,wheremostofthepatientswere surgical,demonstratingsignificantlyhigherhyponatremiain the group receiving hypotonic solution.8 It is noteworthy thatinthepresentstudythepatientsusedthesamevolume inthePOperiod(2,000mL/m2/day),withtheexceptionof fourchildren that requiredvolume expansion:threefrom theisotonicgroupandonefromthehypotonicgroup.The small numberof patients and the lack of standardization offluidinfusioninthepre-hospitalizationperiodmayhave preventedtheappearanceoffinalhyponatremiarelatedto hypotonicsolutioninfusion.
Hyponatremia was observed even in the group that received isotonic solution daily, which may be explained by the possible increase of ADH in all patients undergo-ingsurgery,aspreviouslysuggestedinthestudybyChoong et al., through serum measurement of this hormone and urinaryelectrolytes.8Severalrandomized,controlledtrials, blindedornot,haveshownevidenceofisotonicsolution pro-tectionin relation tohyponatremiain theperiodcloseto surgery(beforeandaftertheprocedure).Mostofthemhad heterogeneousgroups ofpatients, includingclinical situa-tionsof varying severityand/or majoror minorsurgeries, makingcomparisonsdifficultwiththepresentstudy.3---5,13,17 AfterthepublicationbyHoornetal.in2004,severalauthors havequestionedthevalidityofevidencedemonstratingthe superiorityofisotonicsolutiontopreventhyponatremia.In arecentmeta-analysisconductedwithtenrandomized con-trolledtrials,theuseofisotonicsalinesolutionwasshown tobesaferthanthehypotonicsolution,inrelationtosodium levels.16
The presentstudydemonstratedthatpatientswithlow sodium had received a larger solution volume and that hyponatremiacouldhavebeenduetothisfactor.3,15Greater fluidbalancepriortosurgerywasalsodemonstratedinthe
groupreceivinghypotonicsolution,whereasgreaterdiuresis wasobservedintheisotonicsolutiongroup.Hyponatremia canbe explainedby theincrease in extracellular content andconsequentsolutedilution.
The infused volume also plays an important role in the occurrence of hyponatremia; many studies, although focusing on the sodium content, also offer patients a highervolumethanwhatisusuallyrecommended.17,18 The cross-sectional study by Armon et al. evaluated hospital-izedchildrenthatwerereceivingintravenousmaintenance solutionandreportedthathypotonicsolutionswere adminis-teredinmostcases(77/99),with38%receivingmaintenance that was higher than 105% of the recommended vol-ume. Twenty-one of 86 patients had hyponatremia (< 135mmol/L).19 Thesolutionproposed byHolliday& Segar for fluidmaintenancein hospitalized children resultsin a hypotonicsolutionandshouldbereconsidered.20
The present study was designed toanalyze the impor-tance of hyponatremia prevention using an isotonic maintenance solution in a group of patients with similar characteristicsandsubmittedtothesametypeofsurgery. However,thisgroupofpatientsshowedadifferenceonlyin fluidretention(higherfluidbalanceinthehypotonicgroup and higher diuresis in the isotonic group), demonstrating possible interference of ADH action in these patients or lowerexpandingcapacityofhypotonicsolutions,requiringa higheroffertoattainthesameeffectasanisotonicinfusion. Themainlimitationofthepresentstudyreferstosample size,withinsufficientpowertotestwhethertheoccurrence of hyponatremia was associated withthe type of infused solution. Additionally, a large proportion of patients had complicatedappendicitis(30/50),withprolongedevolution andprolongedfastingtime,whichcouldnotbecontrolled. ADHandurinaryelectrolyteswerenotmeasured,which pre-cludedinferences about thepresence of hypertonic urine andfluidretentionattributedtothehormone.
Even considering themethodologicallimitations,based ontheseresultsitcanbesuggestedthatfluidmaintenance witheitherhypotonicorisotonicsolutionforashortperiod oftime (less than48h) in patients undergoing appendec-tomy does not increase the incidence of hyponatremia. However,theuseofhypotonicsolutions isassociatedwith higherfluidretentionthanthatobservedwithisotonic solu-tions. In this respect, it should be noted that positive cumulativefluidbalancein critically-ill patientshas been associatedwithhighermortality.21Studiesincludingahigher numberofpatientsarerequiredtoassessbothhyponatremia relatedtohypotonicsolutioninfusion andtheunfavorable evolutionofpatientsreceivingahigherfluidintake.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Adrogué HJ, Madias NE. Hyponatremia. N Engl J Med. 2000;342:1581---9.
3.Hoorn EJ, Geary D, Robb M, Halperin ML, Bohn D. Acute hyponatremia related to intravenous fluid administration in hospitalized children: an observational study. Pediatrics. 2004;113:1279---84.
4.Shafiee MA, Bohn D, Hoorn EJ, Halperin ML. How to select optimal maintenance intravenous fluid therapy. QJM. 2003;96:601---10.
5.EulmesekianPG,PérezA,MincesPG,BohnD.Hospital-acquired hyponatremia in postoperative pediatric patients: prospec-tive observational study. Pediatr Crit Care Med. 2010;11: 479---83.
6.MoritzML,AyusJC.Hospital-acquiredhyponatremia:whyare therestilldeaths?Pediatrics.2004;113:1395---6.
7.HollidayMA, Segar WE. Themaintenance need for water in parenteralfluidtherapy.Pediatrics.1957;19:823---32.
8.ChoongK,AroraS,ChengJ,FarrokhyarF,ReddyD,Thabane L, et al. Hypotonic versusisotonic maintenance fluids after surgeryforchildren:arandomizedcontrolledtrial.Pediatrics. 2011;128:857---66.
9.AuAK,Ray PE, McBrydeKD,NewmanKD,WeinsteinSL, Bell MJ.Incidenceofpostoperativehyponatremiaandcomplications incritically-illchildrentreatedwithhypotonicandnormotonic solutions.JPediatr.2008;152:33---8.
10.Moritz ML, Ayus JC. Intravenous fluid management for the acutelyillchild.CurrOpinPediatr.2011;23:186---93.
11.DukeT,MolyneuxEM.Intravenousfluidsforseriouslyillchildren: timetoreconsider.Lancet.2003;362:1320---3.
12.NevilleKA,VergeCF,O’MearaMW,WalkerJL.Highantidiuretic hormonelevelsandhyponatremiainchildrenwith gastroenteri-tis.Pediatrics.2005;116:1401---7.
13.NevilleKA, Sandeman DJ, RubinsteinA, Henry GM, McGlynn M,WalkerJL.Preventionofhyponatremiaduringmaintenance intravenous fluid administration: a prospective randomized studyoffluidtypeversusfluidrate.JPediatr.2010;156, 313-9.e1-2.
14.YungM,Keeley S.Randomisedcontrolledtrialofintravenous maintenancefluids.JPaediatrChildHealth.2009;45:9---14. 15.Hatherill M, Waggie Z, Salie S, Argent A. Hospital-acquired
hyponatremia is associated with excessive administration of intravenousmaintenancefluid.Pediatrics.2004;114:1368---9. 16.WangJ,Xu E,XiaoY. Isotonicversushypotonicmaintenance
IVfluidsinhospitalizedchildren:ameta-analysis.Pediatrics. 2014;133:105---13.
17.Hatherill M. Rubbing salt in the wound. Arch Dis Child. 2004;89:414---8.
18.HalberthalM,HalperinML,BohnD.Lessonoftheweek:acute hyponatraemiainchildrenadmittedtohospital:retrospective analysisoffactorscontributingtoitsdevelopmentand resolu-tion.BMJ.2001;322:780---2.
19.ArmonK,Riordan A, PlayforS, MillmanG, KhaderA, Paedi-atricResearchSociety.Hyponatraemiaandhypokalaemiaduring intravenousfluidadministration.ArchDisChild.2008;93:285---7. 20.AlvesJT, Troster EJ, Oliveira CA. Isotonicsaline solution as maintenance intravenous fluid therapy to prevent acquired hyponatremia in hospitalized children. J Pediatr (RioJ). 2011;87:478---86.