www.jped.com.br
ORIGINAL
ARTICLE
Infection
with
multidrug-resistant
gram-negative
bacteria
in
a
pediatric
oncology
intensive
care
unit:
risk
factors
and
outcomes
夽
Patrícia
de
Oliveira
Costa
a,∗,
Elias
Hallack
Atta
a,
André
Ricardo
Araújo
da
Silva
baCenterofHematopoieticStemCellTransplantation,InstitutoNacionaldoCâncer(INCA),RiodeJaneiro,RJ,Brazil bUniversidadeFederalFluminense(UFF),Niterói,RJ,Brazil
Received23June2014;accepted12November2014 Availableonline6June2015
KEYWORDS
Cancer;
Pediatricintensive careunit;
Infection;
Multidrug-resistant gram-negative; Riskfactor; Outcome
Abstract
Objective: This study aimed at evaluating the predictors and outcomes associated with multidrug-resistant gram-negative bacterial (MDR-GNB) infections in an oncology pediatric intensivecareunit(PICU).
Methods: Data were collected relating toall episodes ofGNB infection thatoccurred in a PICUbetweenJanuary of2009andDecemberof2012.GNBinfectionsweredividedintotwo groupsfor comparison:(1)infectionsattributedtoMDR-GNBand(2)infectionsattributed to non-MDR-GNB.Variablesofinterestincludedage,gender,presenceofsolidtumoror hemato-logicdisease, cancerstatus,centralvenouscatheteruse,previousPseudomonasaeruginosa
infection,healthcare-associatedinfection,neutropeniainthepreceding7days,durationof neutropenia,lengthofhospitalstaybeforeICUadmission,lengthofICUstay,andtheuseof anyofthefollowingintheprevious30days:antimicrobialagents,corticosteroids, chemother-apy,orradiationtherapy.Othervariablesincludedinitialappropriateantimicrobialtreatment, definitiveinadequateantimicrobialtreatment,durationofappropriateantibioticuse,timeto initiateadequateantibiotictherapy,andthe7-and30-daymortality.
Results: Multivariate logistic regression analyses showed significant relationships between MDR-GNBandhematologicdiseases(oddsratio [OR]5.262;95%confidenceinterval[95%CI] 1.282---21.594;p=0.021)andhealthcare-associatedinfection(OR18.360;95%CI1.778---189.560;
p=0.015).There were significantdifferences betweenMDR-GNBandnon-MDR-GNB patients for thefollowing variables: inadequateinitial empirical antibiotic therapy,time to initiate adequateantibiotictreatment,andinappropriateantibiotictherapy.
Conclusions: Hematologic malignancyand healthcare-associatedinfection weresignificantly associatedwithMDR-GNBinfectioninthissampleofpediatriconcologypatients.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:deOliveiraCosta P,AttaEH,daSilvaAR. Infectionwithmultidrug-resistantgram-negativebacteriaina
pediatriconcologyintensivecareunit:riskfactorsandoutcomes.JPediatr(RioJ).2015;91:435---41. ∗Correspondingauthor.
E-mail:[email protected](P.deOliveiraCosta).
http://dx.doi.org/10.1016/j.jped.2014.11.009
PALAVRAS-CHAVE
Câncer;
Unidadedeterapia intensivapediátrica; Infecc¸ão;
Bactérias gram-negativas multirresistentes; Fatorderisco; Resultado
Infecc¸ãoporbactériasgram-negativasmultirresistentesemumaunidadedeterapia intensivapediátricaoncológica:fatoresderiscoeresultados
Resumo
Objetivo: Este estudo visou avaliaros preditores e resultados associados às infecc¸ões por bactérias gram-negativas multirresistentes (BGN-MR) em uma unidade de terapia intensiva pediátricaoncológica(UTIP).
Métodos: Foramcoletadosdadoscomrelac¸ãoatodososepisódios deinfecc¸ãoporBGNque ocorreramemumaUTIPentrejaneirode2009edezembrode2012.Asinfecc¸õesporBGNforam divididasem doisgruposparacomparac¸ão:1)infecc¸õesatribuídasaBGN-MRe2)infecc¸ões atribuídasaBGNnãomultirresistente.Asvariáveisdeinteresseincluíramidade,sexo,presenc¸a detumorsólidooumalignidadehematológica,câncer,usodecatetervenosocentral,infecc¸ão anteriorporPseudomonasaeruginosa,infecc¸ãohospitalar,neutropenianos7diasanteriores, durac¸ãodaneutropenia,tempodeinternac¸ãoantesdaUTI,durac¸ãodainternac¸ãonaUTIeuso dequaisquerdosseguintesnos30diasanteriores:agentesantimicrobianos,corticosteroides, quimioterapiaouradioterapia.Outrasvariáveisincluíram:tratamentoantimicrobianoinicial adequado,tratamentoantimicrobianodefinitivoinadequado,durac¸ãodousodeantibióticos adequados,tempodeiníciodaterapiaantibióticaadequada,mortalidadeem7diase mortali-dadeem30dias.
Resultados: Asanálisesderegressãologísticamultivariadamostraramrelac¸õessignificativas entreasBGN-MReasdoenc¸ashematológicas(razãodechance(RC)5,262;intervalodeconfianc¸a de95% (ICde95%)1,282---21,594;p=0,021)einfecc¸õeshospitalares(RC18,360;IC de95% 1,778---189,560;p=0,015).Houvediferenc¸as significativasentreospacientescomBGN-MRe BGNnãoMRcomrelac¸ãoàsseguintesvariáveis:recebimentodeterapiaantibióticaempírica inicialinadequada,tempopara iníciodotratamentoantibióticoadequadoerecebimentode terapiaantibióticainadequada.
Conclusões: Amalignidadehematológicaeainfecc¸ãohospitalarforamsignificativamente asso-ciadasàinfecc¸ãoporBGN-MRnessaamostradepacientespediátricosoncológicos.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Patients with cancer and hematologic malignancy are at high risk of infections. Anumber of factors contribute to thisrisk, including immunosuppressionrelated tothe dis-ease and aggressive treatments, such as chemotherapy, radiationtherapy,steroiduse,andhematopoieticstemcell transplantation.1As aresult,infectionremains afrequent
complicationinpatientswithcancerandisresponsiblefor
intensivecareunit(ICU)admissions.1However,withrecent
advancesincancer treatmentsandimprovements in
criti-calcare,anincreasingnumberofpatientswithhematologic
malignanciesarebeing admittedtothe ICU.2 Despitethe
improvementsinoutcomesassociatedwithimprovedcare,
mortalityremainshighincriticallyillpatientswithcancer
orhematologicmalignancies,particularlyinthepresenceof
ICU-acquirednosocomialinfections.2
Specifically,therateofinfectionsrelatedto
multidrug-resistant gram-negative bacteria (MDR-GNB) in patients
with cancer is increasing globally.3 However, treatment
options for MDR-GNB infections are often limited.
Car-bapenemsarethedrugsofchoiceforinfectionscausedby
extended-spectrum-lactamase(ESBL)-producing
microor-ganisms,buttheirusemaynotbeappropriateininfections
causedbyPseudomonasaeruginosa,Acinetobacter
bauman-nii,orStenotrophomonasmaltophilia,forwhichresistance
to carbapenems is increasing. There are very few new
antimicrobial agents available for the treatment of
MDR-GNB.4 Owing to the lack of novel agents to treat
resistant infections, clinicians must use antibiotics
judi-ciously and appropriately to limit the development of
resistance.5
The presence of cancer, hematologic malignancy, and
a prioror current ICU stay increasestherisk of mortality
in patients withinfections due toMDR-GNB.6 In addition,
GNBinfectionisassociatedwithMDRinfebrileneutropenic
pediatric cancerpatients.7 Previousstudies haveprovided
informationabouttheriskfactorsforcolonizationor
infec-tion withMDR-GNB in select patient populations, suchas
transplant patients and those in intensive or long-term
care.8,9 Studies involving cancer patientshave focused on
bloodstream infections. Limited information is available
regardingthespectrumandmicrobiologyoftheseinfections
inother sites,suchastheurinarytract,respiratorytract,
gastrointestinaltract,andskin.Thisisdespitethefactthat
suchinfectionsarenotrare.10
Littleis known,in particular,regardingtherisk factors
andoutcomesof MDR-GNBinfectionsin anoncology
pedi-atricICU(PICU).Therefore,thisstudyaimedatevaluating
the risk factors and outcomes associated with MDR-GNB
infectionsin childrenwithcancer and/orhematologic
Materials
and
methods
Studydesign
A case---controlstudy wasperformed in the National Can-cerInstitute(InstitutoNacionaldoCâncer[INCA])PICU,Rio deJaneiro,Brazil.INCAisatertiaryoncologypublic hospi-tal, and the six-bed PICU admits only patients with solid tumors and hematologic malignancies. The principal rea-sonsfor admissiontothePICUarepostoperativecare and infectiouscomplicationsinoncologypatients.
Datawerecollectedfromallinfectionepisodesrelatedto GNBthatoccurredbetweenJanuary1,2009andDecember 31,2012inPICU patients,agedbetween 0monthsand18 years,whowerehospitalizedformorethan24h.TheEthics CommitteeofFluminenseFederalUniversity approvedthe study.
Variables included age,gender, thepresence ofa solid tumor or hematologic malignancy, cancer status, and the presence of a central venous catheter. Information prior tothe dateof GNB infectionwasalso collected:previous infectionrelatedtoP.aeruginosa,neutropeniainthe pre-ceding7 days,lengthof neutropenia≥3days,durationof
ICUstay>3days,lengthofhospitalizationbeforeICU admis-sion,andhealthcare-associatedinfection,inadditiontothe useofantimicrobialagents,corticosteroids,and chemother-apyand/orradiationtherapyintheprevious30days.
Infections caused by GNB were divided into 2 groups: (1) infections attributed to MDR-GNB and (2) infections attributedtosusceptibleGNB (non-MDR-GNB).The groups were similar with respect to the infection site. Patients wereincludedmorethanonceintheanalysisforseparate episodesofinfection.Othersvariablesincluded: appropri-ate initial antimicrobial treatment, definitive inadequate antimicrobialtreatment,durationofappropriateantibiotic use,lengthoftimetoinitiateadequateantibiotictherapy, 7-daymortality,and30-daymortality.
Definitionofterms
AnepisodeofinfectionwasdefinedastheisolationofGNB in the presence of compatible clinical signs or symptoms from3daysbeforethedate ofPICUadmissiontothelast day of hospitalization in the PICU. Healthcare-associated infectionsandthosepresentonadmissionwereincluded.
ThediagnosticcriteriaoftheCentersforDiseaseControl andPreventionwereused.GNBwereisolatedfromcultures oftheblood,urine,stool,bronchoalveolarlavage,tracheal aspirate,liquor, orcathetertipduring thistime.The tra-chealaspiratewascollectedfromendotracheal tubesand the tracheostomy of patients who underwent mechanical ventilation.
The diagnostic criteria for pneumonia included puru-lenttracheobronchialsecretionornewpathogenicbacteria isolated from tracheal aspirate and at least two of the following criteria: fever (temperature >38◦C); leukocytes >12,000cells/mLor<4000cells/mLincrease;anewand per-sistent(>48h)infiltratedetectedonachestradiograph;new onsetorworseningcoughordyspneaortachypnea;or wors-eninggasexchange.Thresholdvaluesforculturedspecimens
usedin thepneumonia criteriawere≥104CFU/mL in
tra-chealaspirateorbronchoalveolarlavage.
Cathetercultureswereperformedwhenacatheterwas removedforsuspectedintravascularcatheter-related infec-tion,unexplainedsepsisorerythemaoverlyingthecatheter insertionsite,orpurulenceatthecatheterinsertionsite.At leastoneofthefollowingsignsorsymptomswasrequired for the diagnosis of catheter-associated infection: fever (>38◦C),pain,erythema,heatatthevascularsitewithno otherrecognizedcauseand>15coloniesculturedfroman intravascularcannula tipusing a semiquantitativeculture method,andlackofabloodcultureornoorganismscultured fromblood.
The diagnostic criteria for urinary tract infection included a positive urine culture of ≥105CFU/mL and
withnomore thantwospeciesof microorganisms,andat leastoneof followingsignsor symptomswasrequired for diagnosis: fever (>38◦C); dysuria; suprapubic tenderness; costovertebralanglepainortendernesswithnoother rec-ognizedcause.
Thediagnosticcriteriaforgastroenteritisincludedacute onset of diarrhea (liquid stools for >12h) with or with-out vomiting or fever (>38◦C), no likely non-infectious cause (e.g., diagnostic tests, therapeutic regimen other thanantimicrobialagents,acuteexacerbationofachronic condition,orpsychologicalstress),andanentericpathogen detectedinastoolculture.
MDR-GNB infection was considered in the presence of ESBL-producing Enterobacteriaceae, microorganisms with intrinsicresistancemechanismssuchasS.maltophiliaand
Elizabethkingia meningoseptica, or carbapenem-resistant GNB. Carbapenem-resistant P. aeruginosa and A. bau-manniiwereconsidered MDR-GNB.Polymicrobialinfection involved the isolation of more than one pathogen from a culture sample. Infection was classified as healthcare acquiredwhenonsetoccurred>48hafteradmissiontothe study hospital (ward or PICU). Neutropenia was defined as an absolute neutrophil count <500/mm3 in the blood sample.
Hematologic malignancy included leukemias and lym-phoma.Cancerstatuswasclassifiedintothreecategories: remission/controlled (patients in cancer remission or control who had undergone previous treatments, with-out evidence of recurrence according to the attending oncologist/hematologist), recent diagnosis (patients with active disease diagnosed within the previous three months with need for first-line anticancer treatment), andrelapse/recurrence(patientswithactivedisease with relapseorrecurrence).
Microbiologicalprocedures
Bacterialclassification wasperformed by theINCA micro-biology laboratory using the Vitek automated method (Bio-MerieuxInc.,Marcyl’Etoile,France)andmanually con-firmedforbacterialisolateidentificationandantimicrobial resistance,aspertheClinicalLaboratoryStandardInstitute (CLSI)standards.
Statisticalanalysis
Statistical analysis was conducted using SPSS v.17 (SPSS Inc.,Chicago, Illinois, USA). A value of p<0.05 was con-sideredstatistically significant. Continuous variableswere presentedas medians,andcomparative analysiswas con-ductedusingindependentt-tests.Chi-squaredandFisher’s exacttestswereusedtocomparecategoricalvariables,and oddsratios(OR)with95%confidenceintervals(95%CI)were calculated. Univariate logistic regression analyses identi-fied statistically significant variables (p<0.05) related to MDR-GNBinfectionforinclusioninthemultivariatelogistic regressionanalysis,which wasperformedusingastepwise model.
Results
Therewere765admissionstothePICUbetweenJanuary1, 2009andDecember31,2012.Therewere101episodesof GNBinfectionin76patientsin86admissions,and47(46.5%) oftheseepisodeswererelatedtoMDR-GNBinfection.
The most frequently occurring pathogens among the MDR-GNB were asfollows: A. baumannii, seven (17%); S. maltophilia,seven(15%); Enterobacterspp., seven(15%); and Klebsiella pneumoniae, seven (15%). The most fre-quentlyoccurringpathogensamongthenon-MDR-GNBwere asfollows:P.aeruginosa,22(41%);A.baumannii,14(26%); andK.pneumoniae,eight(15%).Polymicrobialinfectionwas present in one MDR-GNB patient(2.0%, n=1/47) and two non-MDR-GNBpatients(3.8%,n=2/54).
AmongtheGNBinfectionepisodes,MDRwasfoundatthe followingfrequenciesforeachofthebacterialstrains:100% (n=2/2)ofMorganellamorganii,100%(n=1/1)of Citrobac-terspp.,87.5%(n=7/8)ofEnterobacterspp.,50%(n=5/10) ofEscherichiacoli,46.6%(n=7/15)ofK.pneumoniae,36.4% (n=8/22) of A. baumannii,18.5% (n=5/27) ofP. aerugin-osa,and0%(n=0/2)ofProteusmirabilis.Therewereseven episodesof infection by S. maltophilia and four episodes ofinfection by E. meningoseptica,which are microorgan-ismswithintrinsicresistancemechanisms.Therewerethree episodesofpolymicrobialinfection:oneofK.pneumoniae
and non-MDR-GNB E. coli, one of Klebsiella oxytoca and non-MDR-GNBE.coli,andoneofMDRP.aeruginosaandS. maltophilia.
In the MDR-GNB group, bacteria were most frequently isolatedfromthetrachealaspirate(n=17,36.2%),followed by blood culture (n=8, 17%), urine culture (n=4, 8.5%), andcathetertipculture(n=3,6.4%).Inthenon-MDR-GNB group,bacteriaweremostfrequentlyisolatedfromthe tra-chealaspirate(n=22,40.7%),urineculture(n=10,18.5%), blood culture (n=10,18.5%), and a combination of blood culture and catheter tip culture (n=4, 7.4%). There was
concordance between isolate microorganisms, when GNB wereisolatedfromacombinationofdifferentculture.63.8% (30/47) of the MDR-GNB group and 70.3% (38/54) of the non-MDR-GNBgroupweremechanicallyventilatedpatients. The most frequent diseases in the group with MDR-GNB infection were central nervous system tumor (19%), neuroblastoma (15%), non-Hodgkin lymphoma (15%), and acutelymphoblasticleukemia(15%).Inthegroupwith non-MDR-GNB,themostfrequentdiseaseswerecentralnervous system tumor (52%), neuroblastoma (11%), rhabdomyosar-coma(6%),andWilmstumor (6%).Onlyonepatientinthe studygrouphadundergoneabonemarrowtransplant.
Demographicandclinicalcharacteristicsareprovidedin
Table1.
The median neutropenia duration was 0 days in both
groups (MDR-GNB infection, range 0---36; non-MDR-GNB
infection, range 0---6; OR 3.747; 95% CI 1.222---11.488;
p=0.021). The median of length of ICU stay was 8 days
(0---80) in the group with MDR-GNB infection and 2 days
(0---45)inthenon-MDR-GNBinfectiongroup(OR2.296;95%
CI0.001---0.015;p=0.024).
The results of the univariate logistic regression are
describedinTable1.Inthemultivariatelogisticregression
analysis,the presenceof hematologicdiseases (OR5.262;
95% CI1.282---21.594; p=0.021)andhealthcare-associated
infection(OR18.360;95%CI1.778---189.560;p=0.015)were
significantlyassociatedwithMDR-GNBinfection(Table2).
TheothersvariablesassociatedwithMDR-GNBinfection
are detailed in Table 3. Patientswith an MDR-GNB
infec-tionmorefrequentlyreceivedinadequateinitialempirical
antibiotictherapy (74.5%)than thosein thenon-MDR-GNB
group (37.0%, p<0.001), and the time to initiate
ade-quateantibiotictherapywaslongerfortheMDR-GNBgroup
(median:2days)thanforthenon-MDR-GNBgroup(median:
0days,p<0.001).TheMDR-GNBgroupwasalsosignificantly
more likely to receive definitive inappropriate antibiotic
therapy(10.6%vs.0%,p=0.014).
Discussion
Thereis alackofstudies withpediatric oncologypatients hospitalized in the ICU and with MDR-GNB infection. Hematologic malignancy and healthcare-associated infec-tionemergedasimportantfactorsassociatedwithMDR-GNB infectioninthisstudy.
Sepsisincreasesmortalityinchildrenwithmultipleorgan dysfunctionsyndrome.11Therearewideregionalvariations
in the incidence of each resistant pathogen, and these
epidemiologic factors must be considered when making
decisionsaboutempiricantibiotics.5
Recent studies have reported high rates of MDR-GNB
infection in the PICU or pediatric oncology patients. In
children withhematologicalmalignanciesandfebrile
neu-tropenia, 51.6% of bacteremia episodes by K. pneumonia
wereresistanttoceftazidime.12 Moreover,inanotherstudy
in pediatric oncology patients with febrile neutropenia,
50% of Acinetobacter spp., 44.4% of E. coli, 66.7% of
K. pneumoniae, and 100% of P. aeruginosa were MDR.7
MDR cases were present in 57.1% of oncology pediatric
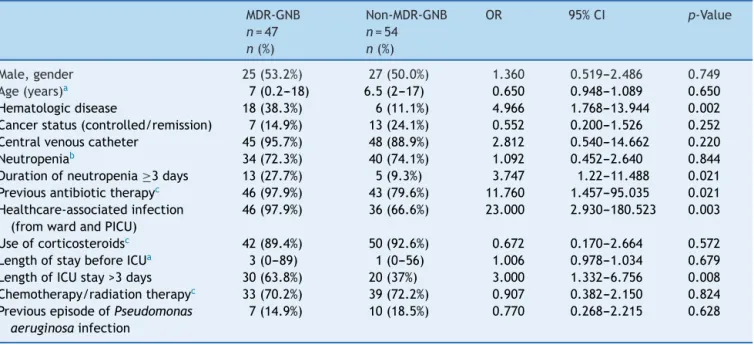
Table1 Demographicandclinicalvariablesrelatingtomultidrug-resistantgram-negativebacterial(MDR-GNB)infectionina pediatricintensivecareunit(PICU),analyzedusingunivariatelogisticregression.
MDR-GNB
n=47
n(%)
Non-MDR-GNB
n=54
n(%)
OR 95%CI p-Value
Male,gender 25(53.2%) 27(50.0%) 1.360 0.519---2.486 0.749
Age(years)a 7(0.2---18) 6.5(2---17) 0.650 0.948---1.089 0.650
Hematologicdisease 18(38.3%) 6(11.1%) 4.966 1.768---13.944 0.002
Cancerstatus(controlled/remission) 7(14.9%) 13(24.1%) 0.552 0.200---1.526 0.252
Centralvenouscatheter 45(95.7%) 48(88.9%) 2.812 0.540---14.662 0.220
Neutropeniab 34(72.3%) 40(74.1%) 1.092 0.452---2.640 0.844
Durationofneutropenia≥3days 13(27.7%) 5(9.3%) 3.747 1.22---11.488 0.021
Previousantibiotictherapyc 46(97.9%) 43(79.6%) 11.760 1.457---95.035 0.021
Healthcare-associatedinfection (fromwardandPICU)
46(97.9%) 36(66.6%) 23.000 2.930---180.523 0.003
Useofcorticosteroidsc 42(89.4%) 50(92.6%) 0.672 0.170---2.664 0.572
LengthofstaybeforeICUa 3(0---89) 1(0---56) 1.006 0.978---1.034 0.679
LengthofICUstay>3days 30(63.8%) 20(37%) 3.000 1.332---6.756 0.008
Chemotherapy/radiationtherapyc 33(70.2%) 39(72.2%) 0.907 0.382---2.150 0.824
PreviousepisodeofPseudomonas aeruginosainfection
7(14.9%) 10(18.5%) 0.770 0.268---2.215 0.628
CI,confidenceinterval;OR,oddsratio;ICU,intensivecareunit.
a Reportedasmedian(range).
b Inthe7dayspriortothepositivecultureforgram-negativebacteria. c Inthe30dayspriortothepositivecultureforgram-negativebacteria.
Table2 Resultsofthemultivariatelogisticregressionanalysisfortheoutcomeofmultidrug-resistantgram-negativebacteria (MDR-GNB),includingthevariablesthatwerestatisticallysignificantintheunivariatelogisticregressionanalysis.
MDR-GNB
n=47
n(%)
Non-MDR-GNB
n=54
n(%)
OR 95%CI p-Value
Healthcare-associated infection
46(97.9%) 36(66.6%) 18.360 1.778---189.560 0.015
Hematologicdiseases 18(38.3%) 6(11.1%) 5.262 1.282---21.594 0.021
Lengthofneutropenia≥3days 13(27.7%) 5(9.3%) 2.802 0.602---13.035 0.189 LengthofICUstay>3days 30(63.8%) 20(37%) 1.680 0.613---4.606 0.313 Previousantibiotictherapya 46(97.9%) 43(79.6%) 3.082 0.296---32.049 0.346
CI,confidenceinterval;OR,oddsratio.
a Inthe30dayspriortothepositivecultureforgram-negativebacteria.
Table3 Outcomesandothersvariablesassociatedwiththepresenceofmultidrug-resistantgram-negativebacteria(MDR-GNB) inpatientsinapediatricintensivecareunit.
MDR-GNB
n=47
n(%)
Non-MDR-GNB
n=54
n(%)
p-Value
Appropriateinitialantibiotictreatment 12(25.5%) 34(63.0%) <0.001
Definitiveinadequateantimicrobialtreatment 5(10.6%) 0(0%) 0.014
Lengthoftimetoinitiateadequateantibiotictherapy(days)a 2(0---10) 0(0---7) <0.001
Durationofappropriateantibioticuse(days)a 10.5(5---22) 10(2---23) 0.608
7-daymortality 5(10.6%) 3(5.6%) 0.345
30-daymortality 12(25.5%) 9(16.7%) 0.273
P.aeruginosabacteremiainchildrenundergoing chemother-apyandhematopoieticstemcelltransplantation.14
In the PICU, 30% of K. pneumonia15 and 23% of
Enterobacteriaceae16 were ESBL-producing strains.
Car-bapenemresistanceinpediatricpatientsintheICUis also
common,withresistanceobservedin62%ofA.baumannii.17
Inthepresentstudy,MDRwasdetectedin50.0%ofE.coli,
46.6%ofK.pneumoniae,36.4%ofA.baumannii,and18.5%
ofP.aeruginosa.
Recentstudiesinneutropenicchildrenwithcancerin
dif-ferenttimeperiodshave indicatedanincreaseintherate
ofinfections relatedtoA. baumannii.7 MDRA.baumannii
arenowconsideredoneofthemostchallengingpathogens
incriticallyillpatients,7especiallypediatricpatients,due
totheabsenceofneweffectiveantimicrobialagents.Inthe
presentstudy,A.baumanniiaccountedfor21.8%(22/101)of
allepisodesofinfectionwithGNBandwerethemost
com-monMDRbacteria(17%,8/47),confirming theimportance
ofthisetiologicagentinthispopulation.
Inthisstudy,themostcommontypesofinfectioninorder
offrequencywerepneumonia,bloodstreaminfections,and
urinarytractinfections. Other studies havedemonstrated
that the main sites of healthcare-associated infections in
PICUarepneumoniaandbloodstreaminfection.18,19
Onco-logicpatients,whensubjectedtoinvasiveproceduressuch
asmechanical ventilation, aremore susceptible to
infec-tiouscomplicationsthanthegeneralpopulation.
In patients with solid tumor, the primary treatment
is often surgical. However, patients with hematological
malignancy often receive more aggressive chemotherapy,
resulting in longer periods of neutropenia, more febrile
neutropenia episodes, and more frequent antibiotic use.
Furthermore,becausehematologicalpatientsoftenpresent
withspecific pathophysiologicalconditions that mayalter
the pharmacokinetic behavior of antimicrobials, differing
administrationschedulesandantimicrobialdosingregimens
fromthestandardschedulesandregimensmayberequired.
Specifically,increaseddoses(e.g.,aminoglycosides,
fluoro-quinolones), prolonged infusion (e.g., beta-lactams), and
therapeuticdrugmonitoringareimportanttooptimizethe
antimicrobialuse. Pharmacokineticand pharmacodynamic
principlesmustbeconsideredwhendesigningantimicrobial
regimens,asithasbecomeincreasinglyclearthat
subopti-malconcentrationsatthesiteofinfectionmaycontribute
toincreasedmicrobialresistance.20
The present results regarding healthcare-associated
infectionsalsosupportthose reportedbyprevious studies
in children with cancer.21 The rates of nosocomial
infec-tionsandantibioticresistancearemuchhigherinthePICU
comparedwithotherhospitalunits.Nosocomial infections
affect up to 30% of patients in the ICU, and they occur
five to ten times more often than in non-ICU patients.5
Inastudyofpediatric patientswithnosocomialinfection,
the overall incidence of nosocomial infection was 2.5%,
rangingfrom1% ingeneralpediatric unitsto23.6% inthe
PICU.18 Severalfactorsmayaccountfor thesedifferences,
includingtheuse of moreinvasive procedures,poor hand
hygiene, lapses in aseptic techniques, selective pressure
for antibiotics duetoinappropriate use, patienttransfers
within the hospital, severe underlying disease,
malnutri-tion, and immunosuppression.5 In the present study, the
lengthofICUstay,previousantibioticuse,andneutropenia
duration were associated with MDR infection in the
uni-variateanalysis,butnotinthemultivariateanalysis,likely
owing to the fact that thesevariables were inter-related
with healthcare-associated infections or hematologic
dis-easesthatwerestronglyassociatedwithMDR-GNBinfection
inthemultivariateanalysis.
Relationshipsbetweenresistantbacterialinfectionsand
pooroutcomeshavebeenreported.5Onedetermining
fac-torintheoutcomeofpatientswithinfectionsisthechoice
of appropriate empirical therapy within the first 48h of
theinitialsymptomsandwithinthefirst24hof apositive
blood culture.4 In thecurrent study,the groupwith
MDR-GNB infectionsreceivedinappropriateempiricalantibiotic
therapy morefrequentlythan thegroupwithoutMDR-GNB
infections, andthetimetoreceive adequate therapywas
longerinthepatientswithMDR-GNBinfections.Therewas
also a trend for greater 7- and 30-day mortality in the
patientswithMDR-GNB;however,thiswasnotstatistically
significant.
A previous study in pediatric cancer patients also
reportednostatisticallysignificantdifferencesin
infection-relatedorall-causemortalityduetoMDR-GNBinfections.21
The relationship between the timeliness of adequate
therapy and prognosis is complex. Physicians tend to
prescribe early extended-spectrum antimicrobial therapy
to patients with severe clinical presentations. In
con-trast, antimicrobial therapy is often delayed in patients
who do not present with organ dysfunction or who have
delayed positivityofblood cultures.Finally, patientswith
a rapid progression to death never receive antimicrobial
therapy.22
Inthisstudy,themediantimetoinitiateadequate
antibi-otictherapywas2daysinchildrenwithMDR-GNBinfection,
withnoimpactonmortality.Studiesregardingtheeffectof
adelaytoinitiateadequateantibioticsonmortalityin
pedi-atricpatientsarelacking.However,instudieswithadults,a
delayof2---3daystoinitiateadequateantibioticshadlittle
effectonpatientmortality.23---26
Thestrengths ofthe current studyinclude the
popula-tion,whichhadacombinationofriskfactorsforMDR-GNB
infections:cancerandanICUstay.Furthermore,the
knowl-edge of risk factors for MDR-GNB might help clinicians
identify patients who require more attention during the
empirical prescription of antimicrobial therapy, special
monitoring,andinfectioncontrolmeasures.
Thisstudyhadcertainlimitations, includingthe
collec-tionofretrospective datainasmallsample. Despitethis,
therewerenomissingdata,andsignificantdifferenceswere
observed.
Conclusion
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Rosolem MM, Rabello LS, Lisboa T, Caruso P, Costa RT, Leal JV,etal.Criticallyillpatientswithcancerandsepsis:clinical courseandprognosticfactors.JCritCare.2012;27:301---7. 2.TurkogluM,MirzaE,Tunc¸canOG,ErdemGU,DizbayM,Ya˘gcı
M,etal.Acinetobacterbaumannii infectioninpatientswith hematologicmalignanciesinintensivecareunit:riskfactorsand impactonmortality.JCritCare.2011;26:460---7.
3.MontassierE,BatardE,GastinneT,PotelG,delaCochetière MF.Recentchangesinbacteremiainpatientswithcancer:a systematicreviewofepidemiology and antibiotic resistance. EurJClinMicrobiolInfectDis.2013;32:841---50.
4.Gudiol C, Tubau F, Calatayud L, Garcia-Vidal C, Cisnal M, Sánchez-Ortega I, et al. Bacteraemia due to multidrug-resistantGram-negativebacilliincancerpatients:riskfactors, antibiotic therapy and outcomes. J Antimicrob Chemother. 2011;66:657---63.
5.VollesDF,BrananTN.Antibioticsintheintensivecareunit:focus onagentsforresistantpathogens.EmergMedClinNorthAm. 2008;26:813---34.
6.VardakasKZ,RafailidisPI,KonstanteliasAA,FalagasME. Predic-torsofmortalityinpatientswithinfectionsduetomulti-drug resistantGramnegativebacteria:thestudy,thepatient,the bugorthedrug.JInfect.2013;66:401---14.
7.El-MahallawyHA, El-WakilM, MoneerMM, ShalabyL. Antibi-oticresistanceisassociatedwithlongerbacteremicepisodes andworseoutcomeinfebrileneutropenicchildrenwithcancer. PediatrBloodCancer.2011;57:283---8.
8.BorerA,Saidel-OdesL,EskiraS,NativR,RiesenbergK, Livshiz-Riven I, et al. Risk factors for developing clinical infection withcarbapenem-resistantKlebsiellapneumoniaeinhospital patientsinitiallyonlycolonizedwithcarbapenem-resistantK. pneumoniae.AmJInfectControl.2012;40:421---5.
9.BlotS,DepuydtP,VogelaersD,DecruyenaereJ,DeWaeleJ, HosteE,etal.Colonizationstatusandappropriateantibiotic therapy for nosocomial bacteremia caused by antibiotic-resistant gram-negative bacteria in an intensive care unit. InfectControlHospEpidemiol.2005;26:575---9.
10.AshourHM,El-SharifA.Speciesdistributionandantimicrobial susceptibilityofgram-negativeaerobicbacteriainhospitalized cancerpatients.JTranslMed.2009;7:14.
11.TantaleánJA,LeónRJ,SantosAA,Sánchez E.Multiple organ dysfunction syndrome in children. Pediatr Crit Care Med. 2003;4:181---5.
12.AriffinH,NavaratnamP,MohamedM,ArasuA,AbdullahWA,Lee CL,etal.Ceftazidime-resistantKlebsiellapneumoniae blood-stream infection in children with febrile neutropenia. Int J InfectDis.2000;4:21---5.
13.Fernandes TA, Pereira CA, Petrili AS, Pignatari AC. Molecu-larcharacterizationofcarbapenem-resistantandmetallo-beta
-lactamase-producing Pseudomonas aeruginosa isolated from bloodculturesfrom childrenand teenagerswithcancer.Rev SocBrasMedTrop.2010;43:372---6.
14.CaselliD,CesaroS,ZiinoO,ZanazzoG,ManiconeR,Livadiotti S,etal.MultidrugresistantPseudomonasaeruginosainfection inchildrenundergoingchemotherapyand hematopoieticstem celltransplantation.Haematologica.2010;95:1612---5. 15.Grisaru-Soen G, Sweed Y, Lerner-Geva L, Hirsh-Yechezkel G,
BoykoV,VardiA,etal.Nosocomialbloodstreaminfectionsin apediatricintensivecare unit:3-yearsurvey.MedSciMonit. 2007;13:CR251---7.
16.MittP,MetsvahtT,AdamsonV,TellingK,NaaberP,LutsarI,etal. Five-yearprospectivesurveillanceofnosocomialbloodstream infectionsinanEstonianpaediatricintensivecareunit.JHosp Infect.2014;86:95---9.
17.Katragkou A, Kotsiou M, Antachopoulos C, Benos A, Sofi-anouD,TamiolakiM,etal.Acquisitionofimipenem-resistant Acinetobacterbaumanniiinapediatricintensivecareunit:a case---controlstudy.IntensiveCareMed.2006;32:1384---91. 18.Raymond J, Aujard Y. Nosocomial infections in pediatric
patients:aEuropean,multicenterprospectivestudy.European StudyGroup.InfectControlHospEpidemiol.2000;21:260---3. 19.AbramczykML,CarvalhoWB,CarvalhoES,MedeirosEA.
Nosoco-mialinfectioninapediatricintensivecareunitinadeveloping country.BrazJInfectDis.2003;7:375---80.
20.Ansari SR, Hanna H, Hachem R, Jiang Y, Rolston K, Raad I. Risk factors for infections with multidrug-resistant Stenotrophomonasmaltophiliainpatientswithcancer.Cancer. 2007;109:2615---22.
21.HaeuslerGM,Mechinaud F,DaleyAJ,Starr M,ShannF, Con-nellTG,etal.Antibiotic-resistantGram-negativebacteremiain pediatriconcologypatients---riskfactorsandoutcomes.Pediatr InfectDisJ.2013;32:723---6.
22.TabahA,KoulentiD,LauplandK,MissetB,VallesJ,Bruzzide CarvalhoF,etal.Characteristicsanddeterminantsofoutcome ofhospital-acquired bloodstreaminfectionsinintensive care units:theEUROBACTInternationalCohortStudy.IntensiveCare Med.2012;38:1930---45.
23.To KK, Lo WU, Chan JF, Tse H, Cheng VC, Ho PL. Clini-caloutcomeofextended-spectrumbeta-lactamase-producing Escherichiacolibacteremiainanareawithhighendemicity.Int JInfectDis.2013;17:e120---4.
24.Anderson DJ,EngemannJJ,Harrell LJ,Carmeli Y,Reller LB, KayeKS.Predictorsofmortalityinpatientswithbloodstream infectionduetoceftazidime-resistantKlebsiellapneumoniae. AntimicrobAgentsChemother.2006;50:1715---20.
25.Kang CI, Kim SH, Kim DM, Park WB, Lee KD, Kim HB, et al. Risk factors for and clinicaloutcomes of bloodstream infections caused by extended-spectrum beta-lactamase-producing Klebsiella pneumoniae. Infect Control Hosp Epi-demiol.2004;25:860---7.