SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Total
ruptures
of
the
extensor
apparatus
of
the
knee
夽
Diogo
Moura
∗,
Fernando
Fonseca
CentroHospitalareUniversitáriodeCoimbra,DepartamentodeOrtopedia,Coimbra,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12February2016 Accepted18March2016 Availableonline25October2016
Keywords:
Rupture Knee
Rangeofmotion,articular Patella
Tendons
a
b
s
t
r
a
c
t
Objective:Thiswasaretrospectivecase-controlstudyontotalrupturesoftheextensor appa-ratusoftheknee,aimedtocomparepatellafractureswithtendinousruptures.
Methods:Thesampleincluded190patientsand198totalrupturesofthekneeextensor apparatus.Allpatientswereevaluatedbythesameexaminerafteraminimumone-year follow-up.
Results:Tendinousrupturesoccurredmostfrequentlyinmen,inyoungerpatients,andhad betterclinicalandfunctionaloutcomeswhencomparedwithpatellafractures;however,the formerpresentedhigherlevelsofthighatrophy.Patellafracturesoccurredmostfrequently inwomenandinolderpatientsandcausedmostfrequentlycausedresidualpain,muscle weakness,andlimitationsindailyactivities.Comminutedfractureswererelatedto high-energytrauma,lowerclinicalandfunctionaloutcomes,andhigherlevelsofresidualpain andosteosynthesisfailure.Earlyremovalofosteosynthesismaterialwasrelatedtobetter outcomes.Regardingthetendinousruptures,overhalfofthepatientspresentedrisk con-ditionsfortendinousdegeneration;alongerdelayuntilsurgerywasrelatedtolowerKujala scores.
Conclusion:Thesurgicalrepairofbilateralrupturesofthekneeextensorapparatusresulted insatisfactoryclinicalandfunctionaloutcomes,whichwerebetterfortendinousruptures whencomparedwithpatellafractures.However,theselesionsareassociatedwith non-negligiblelevelsofresidualpain,muscleweakness,atrophy,andothercomplications.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Roturas
totais
do
aparelho
extensor
do
joelho
Palavras-chave:
Rotura Joelho
Amplitudedemovimentoarticular
r
e
s
u
m
o
Objetivo:Estudoretrospectivosobreroturastotaisdoaparelhoextensordojoelhoque com-paraasfraturasdapatelacomasroturastendinosas.
Métodos:Amostracom190pacientese198roturastotaisdoaparelhoextensordojoelho. Otempomínimodeseguimentoapósacirurgiafoideumanoetodosospacientesforam avaliadosclínicaeradiologicamentepelomesmomédico.
夽
StudyconductedattheDepartmentofOrthopedy,CentroHospitalareUniversitáriodeCoimbra,Coimbra,Portugal.
∗ Correspondingauthor.
E-mail:[email protected](D.Moura).
http://dx.doi.org/10.1016/j.rboe.2016.10.012
Patela Tendões
Resultados: Asroturastendinosasocorremmaisfrequentementeemhomens,empacientes maisnovoseestãoassociadasaníveisclínico-funcionaissuperioresemrelac¸ãoàsfraturas dapatela.Noentanto,comatrofiadacoxamaisfrequente.Asfraturaspatelaresocorrem maisfrequentementeemmulherescomidademaisavanc¸adaeprovocammais frequente-mentedorresidual,déficitdeforc¸amuscularelimitac¸ãodasatividadesdavidadiária.A maiorcominuic¸ãodasfraturasdapatelaesteveassociadaaresultadosclínico-funcionais maisdesfavoráveis,aníveismaiselevadosdedorresidualededesmontagemdomaterial deosteossíntese.Aextrac¸ãoprecocedomaterialdeosteossínteseesteveassociadaa mel-horesresultados.Nogrupodasroturastendinosas,maisdemetadeapresentavadoenc¸as consideradasderiscoparadegenerac¸ãotendinosaeumtempodeesperamaisprolongado atéacirurgiademonstrouvaloresdeescoredeKujalasignificativamenteinferiores.
Conclusão: Otratamentocirúrgicodasroturastotaisdoaparelhoextensordojoelhogarante bonsresultadosfuncionais,quesãosuperioresparaasroturastendinosasemcomparac¸ão comasfraturasdapatela.Noentanto,estãoassociadasaníveisimportantesdedorresidual, fraquezamuscular,atrofiamusculareoutrascomplicac¸ões.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Theextensorapparatusoftheknee consistsofthreebasic structures:twotendons,thequadricepsandpatellar;andone bone,thepatella.Thetotalruptureofthisapparatuscanoccur throughtheboneortendon,leadingtoaninabilitytoactively extendtheleg.Patellarfracturesaremorefrequentthan tendi-nousruptures,inratios rangingfrom17:1to43:1;ruptures ofthe quadricepstendonare more frequentthan those of thepatellartendon.1,2Theseinjuriesrequiresurgical
recon-structionofthe extensorapparatusinorder torecoverthe extensionfunction.3Todate,onlyonestudyhasdirectly
com-paredclinicalandfunctionalresultsofpatellarfracturesand tendinousruptureoftheextensorapparatusoftheknee.3
Material
and
methods
This was a retrospective study, comprising a mean of 5.1 years(range1–10);190patientswere retrieved, correspond-ingto198totalrupturesoftheextensorapparatusoftheknee thatweresurgicallytreated.Allpatientswithotherassociated traumaticinjuriesandthose whocould notbefollowed-up foraminimumofoneyearaftersurgerywereexcluded.The clinicalevaluationincludedfunctionalassessment, measure-mentofrangeofmotion,andtheapplicationofavalidated score for patellofemoral pathology, the Kujala score.4 The
degreeof patientsatisfaction was also assessedina scale from 0to5, were 0–dissatisfied,and 5 –totally satisfied. Radiologically,patientswereassessedforfracture classifica-tion(AOclassification)5;presenceorabsenceofconsolidation;
patellofemoralarthrosis;patellarheight,usingtheInsalland Salvatiindex6;andwhetherornottheosteosynthesis
mate-rial was extracted. The variables were treated statistically using SPSSv23, and a 0.05 significance level was adopted.
Quantitativevalueswerepresentedasmean±standard devia-tion(minimum–maximum),andqualitativevaluesasnumber (n)or percentage(%).For comparisonsbetweentwogroups
with quantitative variables, Student’s t-test was used; the Mann–Whitney test was used when the values were very low. Tocompareamongthreeormoregroups,ANOVA was used.Forcomparisonsbetweentwogroupswithnominal vari-ables, the chi-squared test wasused; for ordinalvariables, the Mann–Whitney test. To study the association between quantitativevariables,Pearson’scorrelationwasused;forthe multivariate study,the generallinearmodel(GLM)analysis wasadopted.ThestudywasapprovedbytheEthics Commit-teeoftheCentroHospitalareUniversitáriodeCoimbraand all patientsortheir respectivefamilies signedaninformed consentform.
Results
Thesampleconsistedof190patientsor198ruptures,aseight werebilateral.Themeanagewas58.82±17.86years(range 18–90)and56.6%weremale.Ofthetotal,67.17%(n=133)was patellarfractures;tendinousrupturesoftheextensor appara-tusaccountedfortheremaining32.82%(n=65),whichwere dividedbetweenquadricepstendonruptures(56.9%)and rup-tureofthepatellartendon(43.1%;Table1).
In the analysisofthe groupwith patellarfractures, the mostcommonmechanismofinjurywaslowenergy(87.1%) direct trauma (86.4%). The predominant types of patellar fracturewereC1,C3,andA1consideringtheAOclassification (Fig. 1). Comminuted type C patellar fractures (C1 to C3)
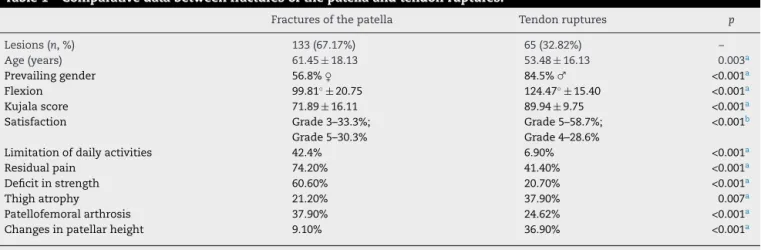
Table1–Comparativedatabetweenfracturesofthepatellaandtendonruptures.
Fracturesofthepatella Tendonruptures p
Lesions(n,%) 133(67.17%) 65(32.82%) –
Age(years) 61.45±18.13 53.48±16.13 0.003a
Prevailinggender 56.8%♀ 84.5%♂ <0.001a
Flexion 99.81◦±20.75 124.47◦±15.40 <0.001a
Kujalascore 71.89±16.11 89.94±9.75 <0.001a
Satisfaction Grade3–33.3%;
Grade5–30.3%
Grade5–58.7%;
Grade4–28.6%
<0.001b
Limitationofdailyactivities 42.4% 6.90% <0.001a
Residualpain 74.20% 41.40% <0.001a
Deficitinstrength 60.60% 20.70% <0.001a
Thighatrophy 21.20% 37.90% 0.007a
Patellofemoralarthrosis 37.90% 24.62% <0.001a
Changesinpatellarheight 9.10% 36.90% <0.001a
a Chi-squaredtest.
b Mann–Whitneytest.
vs. 63.88±16.44; p=0.016) and flexion (104.32±17.45 vs.
90.61±23.31; p=0.001). An extension deficit from 1◦ to 5◦
wasobservedin6.06%ofcases,andadeficitfrom5◦ to10◦,
in 2.27%. Signs of patellofemoral arthrosis were observed in37.90%ofcases,andallchangesinpatellarheight corre-spondedtolowpatellae.Complicationsdirectlyrelatedtothe surgicaltreatmentoccurredin23.7%ofcasesandconsisted of painful material (19.7%), osteosynthesis removal (8.3%), infection(3%),non-consolidationofthe fracture(1.5%),and othersurgicalwoundproblems(3.8%).Comparedwithtype C1 fractures, type C3 comminuted patellar fractures pre-sentedhigherlevelsofosteosynthesisremoval(11.8%vs.3%) andresidualpain(84.8%vs. 71%).Regardingosteosynthesis techniques,screwsledtocomplicationsin75%ofcaseswhile circular tension band, 38.5%. These techniques presented thehighestratesofcomplications,aswellashigherratesof osteosynthesisremoval,particularlyinthe25%ofthepatients whoreceivedscrewsandin15.4%ofthoseinwhomacircular tensionband wasperformed. Regarding theosteosynthesis material,screwswerethemostsymptomatic(50%ofcases), followedbycirculartension band(in 23.1%ofcases).Older individualshad asignificantlylower Kujalascore(r=−0.60;
p<.001),lowermeanflexion(r=−0.51;p<0.001),andalower degreeofsatisfaction (p<0.001; rho=−0.42). Moreover,they
AO classification
14.4%
0.8%
0.8%
50% 8.3%
25.8%
A1
A2
B1
C1
C2
C3
Fig.1–Prevalenceoftypesofpatellarfracturesaccordingto theAOclassification.
presentedhigherlevelsofresidualpain(p<0.001)andmore muscularstrengthdeficit(p<0.001).Inturn,younger individu-alspresentedsignificantlymoretightatrophy(p<0.001)anda trendforhigherratesofosteosynthesisremoval.Theremoval oftheosteosynthesismaterialoccurredin50.8%ofpatients withpatellarfractures;thesepatients,whencomparedwith thoseinwhomtheosteosynthesismaterialwasnotremoved, presentedasignificantlyhigherKujalascore(74.79±15.21vs. 64.84±15.49)(p=0.002)and meanflexion (104.66±19.40vs. 93.03±20.72)(p=0.006).Patients who underwentextraction ofosteosynthesismaterialpresentedlowerlevelsofresidual painwhencomparedwiththoseinwhomthematerialwas notremoved(69%vs.84.2%).
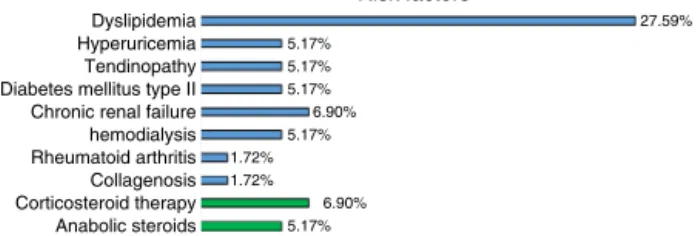
Regarding the group oftendon ruptures, falls were the causeofinjuryin70.69%ofcases,andindirecttraumawas themostfrequent(91.38%).Thepredominantmechanismsof injury wereknee torsion(67.92%),hyperflexion ofthe knee (15.1%), and counter-resistance with the knee in semiflex-ion(9.43%).Fivetendonrupturesoccurredbydirecttrauma andconsistedoffragmentswithdirecttendoncut.The col-lapseoccurredmorefrequentlyatthemidpointofthetendon (43.10%), followed bypatellar insertion (39.66%), myotendi-nous transition (13.79%), and insertion at the level of the anteriortibialtuberosity(3.45%).Recurrenceoftendon rup-turewasobservedin3.45%,rupturesinthecontextoftotal kneereplacementin3.45%,andbilateralrupturesin12.07%of casesoftendinousrupture.Halfofthepatientswithtendinous rupture wereconsidered tobeatriskfordegeneration and tendinousruptureoftheextensorapparatus,and2.07% pre-sentedriskdrugintakes(Fig.2).7–9Only12.07%ofthepatients
Dyslipidemia Risk factors 5.17% 27.59% 5.17% 5.17% 6.90% 5.17% 1.72% 1.72% 6.90% 5.17% Hyperuricemia Tendinopathy Diabetes mellitus type II Chronic renal failure hemodialysis Rheumatoid arthritis Collagenosis Corticosteroid therapy Anabolic steroids
Fig.2–Prevalenceofriskfactorsinthegroupoftendinous ruptures.
followedbytenorrhaphywithtrans-bonepoints(24.14%), ten-odesiswithanchors(17.24%),andotherreconstructivegraft optionsforcircumstantialcases(6.90%).Protectivewiringwas usedin64%ofcasesofpatellartendonrupture;themeantime foritsremovalwas6.38months.Themeandurationof postop-erativeimmobilizationwas45.43days(range41–66days).The functionaloutcomesandcomplicationsofsurgicaltreatment oftendinousruptures oftheextensorapparatusareshown inTable1.Oftheindividualsinthisgroup,13.85%presented extensiondeficit,alwaysless than 5◦. Radiologicalsigns of
patellofemoral arthrosis were identified in 36.90% of the knees;highpatella,in15.81%;andlowpatella,in21.09%.The waitingtimeuntilsurgerypresentedastatisticallysignificant inversecorrelation(r=−0.03;p=0.008)withtheKujalascore. Thebest resultswere observedin repairs withtrans-bone points,whichshowedastatisticallysignificantdifferencein themeanrangeofflexion(126.14±13.88;p=0.031)andmean Kujalascore(88.46±9.33;p=0.006)whencomparedwiththe results of reconstruction with tendon grafts (respectively, 107.50±22.17 and 77. 25±10.50). Recurrent ruptures and thosethatoccurredinthecontextoftotalkneereplacement presented a significantly lower Kujala score (respectively, 80.25±8.62and 91.08±9.83;p=0.031)whencomparedwith otherdisruptions.Residualpainwas1.75times(oddsratio) morepresentinrupturesofthepatellartendonwhen com-paredwiththoseofthequadricepstendon(50%inpatellar tendonrupturevs.36.1%intheruptureofthequadriceps ten-don)andwasassociatedwithmorerupturesatthelevelof thesiteoftendoninsertioninthebones(100%intheanterior tibialtuberosityand 44.1%inthe patellarinsert, compared to36.7%inthetendinousbody).Patientswithresidualpain hadsignificantlylowerflexionamplitudes(119.46±17.60vs. 128.16±12.54;p=0.031)andlower Kujalascore(83.43±9.32
vs. 95±6.62;p<0.001)when comparedwiththose who did
nothaveresidualpain.Othercomplications,observedless fre-quently,includedre-ruptureofthetendon(3.08%),knee stiff-ness(3.08%),andwounddehiscence(3.08%),amongothers.
Discussion
Thepresentstudydemonstratedthatthegradeof comminu-tionofpatellarfractureswasassociatedwithhigher-energy traumaandwithlessfavorableclinicalandfunctionalresults. The comminution, a difficulty to achieve anatomic reduc-tion andstability ofosteosynthesis,aswell astheneed to use circular and doubletension bands,likelycontribute to thefactthatC3fracturesandthesetypesofosteosynthesis
present higher levels of osteosynthesis removaland resid-ualpain,whichleadstoaworseprognosisofthesefractures. Althoughconsolidationisachievedinmostcases,allowing forreasonableclinicalandfunctional outcome,thesurgical treatmentofpatellarfracturesleadstohighlevelsofresidual pain, atrophy,muscle strength deficit,and other complica-tions,whichisinagreementwiththe literature.10–13 Inthe
present study,osteosynthesisremovalandthighatrophyin patellarfracturesweremorecommoninyoungerindividuals, probablyduetothehigherfunctionallevelofthisagegroup and moreintensive demandonthe extensorapparatus.As thisisanosteosynthesisofaprominentbone,whichisvery mobileandsubjecttohighandrepeatedforces,togetherwith theneedforearlyjointmobilization,impliesthatthe mate-rialoftendesintegrates,migrates,orbecomesprolapsedand painful,delayingfunctionalrecovery.13Earlyextractionofthe
osteosynthesismaterialshouldbeperformedwhenever pos-sible,asthisprocedureisassociatedwithsuperiorclinicaland functionalresults.
Tendonrupturesoccurredmorefrequentlyatthe midsec-tionofthetendonandpatellarinsertion.Thisisinagreement with the fact that almost all tendon ruptures ofthe knee extensor apparatus occur after adegenerative and inflam-matoryprocess,whichismorepronouncedinthetendinous midsection and in osteotendinous junction in which the tendonresistanceissignificantlyreducedandtheriskof rup-ture,increased.7–9 Theolderagerangeobservedinpatients
with rupture of the quadriceps tendon is consistent with theliterature.3Alongerwaitingtimeuntilsurgerypresented
significantly lower Kujala scores, which is consistent with results obtained by other authors.2,14–16 Clinical and
func-tionalresultsinthetendontearswerealsosatisfactory,with near normalmobility and Kujala score; nonetheless,these were less favorable inrecurrent ruptures, inpatients with knee prostheses,and whentherewas aneedforatendon graft, probably due to the weakening and changes in the patellofemoralbiomechanics.14–16Furthermore,nearlyhalfof
patients with tendon ruptures had residual pain; this was morepresentinpatellartendonrupturesandinthoseatthe levelofboneinserts.
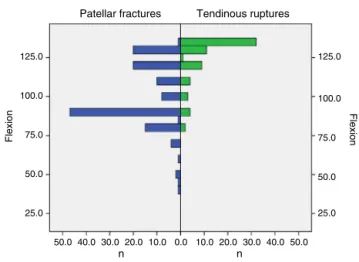
Patellar fractures
125.0
100.0
75.0
Flexion
50.0
25.0
125.0
100.0
75.0
Flexion
50.0
25.0
50.0 40.0 30.0
n n
20.0 10.0 0.0 10.0 20.0 30.0 40.0 50.0
Tendinous ruptures
Fig.3–Amplitudesofflexion:comparisonofpatellar fractureswithtendinousruptures.
predictablyhigherinpatellarfractures,notonlyduetothe advanced age, but also because these fractures have joint involvement.Inamultivariateanalysis,whencomparing flex-ionandKujalascorebetweenpatellarfracturesandtendinous ruptures,adjustingforageandthepresenceofpatellofemoral arthrosis,theseparameterswerestillfoundtobesignificantly higherintendinousruptures;theestimatedmeanflexionwas 98.92◦ in fractures and 116.62◦ in tendinous ruptures, and
the Kujalascorewas 70.86in fractures and82.59 in tendi-nousruptures.Theonlypreviousstudythatdirectlycompared resultsofsurgicaltreatmentofpatellarfractures(n=50)with rupture ofthe quadriceps tendon (n=36) and patellar ten-don(n=13) didnotidentifysignificant differencesinrange ofmotion,radiographicsignsofarthrosis,andfunctional Teg-ner,Lysholm,andSF-36scoresamongthedifferenttypesof rupture.3
Limitations of this study are related to the fact that it was anobservationalretrospective study with asubjective clinical assessment and tothe difficulty ofcontrolling the variablesthatdetermineclinicalandfunctionalresults,and complications.Thestrengthsofthepresentstudyincludethe largenumberofpatientsineachgroup,aswellastheuseof
Tendinous ruptures Patellar fractures
120
100
80
60
Kujala score
40
20
120
100
80
60
Kujala score
40
20
20.0 15.0 10.0
n n
5.0 0.0 5.0 10.0 15.0 20.0
Fig.4–Kujalascore:comparisonofpatellarfractureswith
tendonruptures.
objectiveandvalidatedmeasuresforclinicalandfunctional assessmentofrangeofmotionandtheKujalascore.
Conclusion
Surgicaltreatmentoftotalrupturesoftheextensor appara-tusofthekneeprovidedgoodfunctionalresults,whichwere superior fortendonruptureswhen comparedwithpatellar fractures,probablyduetohigherage ofthe latterpatients. Nonetheless,ruptureoftheextensorapparatusisassociated withhighlevelsofresidualpain,muscleweakness,muscle atrophy,andothercomplications,whichisprobablyduetoa lossofdynamicbalanceofthepatellofemoraljoint.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
ToDr.MargaridaMarques,fromtheStatisticsDepartmentof theHospitalandUniversityofCoimbra,forhercollaboration.
r
e
f
e
r
e
n
c
e
s
1.KellersmannR,BlattertTR,WeckbachA.Bilateralpatellar tendonrupturewithoutpredisposingsystemicdiseaseor steroiduse:acasereportandreviewoftheliterature.Arch OrthopTraumaSurg.2005;125(2):127–33.
2.SiwekCW,RaoJP.Rupturesoftheextensormechanismofthe kneejoint.JBoneJointSurgAm.1981;63(6):932–7.
3.TejwaniNC,LekicN,BechtelC,MonteroN,EgolKA. Outcomesafterkneejointextensormechanismdisruptions: isitbettertofracturethepatellaorrupturethetendon?J OrthopTrauma.2012;26(11):648–51.
4.KujalaUM,JaakkolaLH,KoskinenSK,TaimelaS,HurmeM, NelimarkkaO.Scoringofpatellofemoraldisorders. Arthroscopy.1993;9(2):159–63.
5.Classificac¸ãoAOdaPatela;2016.Disponívelem:
https://www2.aofoundation.org/wps/portal/surgery? showPage=diagnosis&bone=Knee&segment=Patella[acesso em07jan2016].
6.InsallJ,SalvatiE.Patellapositioninthenormalkneejoint. Radiology.1971;101(1):101–4.
7.KellyDW,CarterVS,JobeFW,KerlanRK.Patellarand quadricepstendonruptures–Jumper’sknee.AmJSports Med.1984;12(5):375–80.
8.ZernickeRF,GarhammerJ,JobeFW.Humanpatellartendon rupture:akineticanalysis.JBoneJointSurgAm.
1977;59(2):179–83.
9.KannusP,JozsaL.Histopathologicalchangespreceding spontaneousruptureofatendon.Acontrolledstudyof891 patients.JBoneJointSurgAm.1991;73(10):1507–25.
10.LazaroLE,WellmanDS,SauroG,PardeeNC,BerkesMB,Little MT,etal.Outcomesafteroperativefixationofcomplete articularpatellarfractures:assessmentoffunctional impairment.JBoneJointSurgAm.2013;95(14):e961–8.
12.KumarG,MereddyPK,HakkalamaniS,DonnachieNJ.Implant removalfollowingsurgicalstabilizationofpatellafracture. Orthopedics.2010;33(5):301.
13.DyCJ,LittleMT,BerkesMB,MaY,RobertsTR,HelfetDL,etal. Meta-analysisofre-operation,nonunion,andinfection afteropenreductionandinternalfixationofpatella fractures.JTraumaAcuteCareSurg.2012;73(4):928–32.
14.KovacevN,Anti´cJ,Gvozdenovi´cN,Obradovi´cM,VranjeˇsM, MilankovM.Patellartendonrupture–treatmentresults.Med Pregl.2015;68(1–2):22–8.
15.BoudissaM,RoudetA,Rubens-DuvalB,ChaussardC, SaragagliaD.Acutequadricepstendonruptures:aseriesof50 kneeswithanaveragefollow-upofmorethan6years.Orthop TraumatolSurgRes.2014;100(2):213–6.