www.jped.com.br
ORIGINAL
ARTICLE
Early
amplitude-integrated
electroencephalography
for
monitoring
neonates
at
high
risk
for
brain
injury
夽
Gabriel
Fernando
Todeschi
Variane
a,∗,
Maurício
Magalhães
a,
Renato
Gasperine
a,
Heitor
Castelo
Branco
Rodrigues
Alves
b,
Thiago
Luiz
Pereira
Donoso
Scoppetta
b,
Rodrigo
de
Jesus
Gonc
¸alves
Figueredo
a,
Francisco
Paulo
Martins
Rodrigues
a,
Alexandre
Netto
a,
Marcelo
Jenne
Mimica
a,c,
Clery
Bernardi
Gallacci
aaFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,DepartamentodePediatria,SãoPaulo,SP,Brazil bFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,DepartamentodeRadiologia,SãoPaulo,SP,Brazil cFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,DepartamentodePatologia,SãoPaulo,SP,Brazil
Received16June2016;accepted18November2016 Availableonline23February2017
KEYWORDS Newborn; Braininjury;
Amplitude-integrated EEG;
Earlyoutcome
Abstract
Objective: Thisstudyaimedtocorrelateamplitude-integratedelectroencephalographyfindings withearlyoutcomes,measuredbymortalityandneuroimagingfindings,inaprospectivecohort ofinfantsathighriskforbraininjuryinthiscenterinBrazil.
Methods: Thisblindedprospectivecohortstudyevaluated23preterminfantsbelow31weeks ofgestationalageand17infantsdiagnosedwithhypoxic-ischemicencephalopathysecondary toperinatalasphyxia,withgestationalagegreaterthan36weeks,monitoredwith amplitude-integratedelectroencephalographyinapublictertiarycenterfromFebruary2014toJanuary 2015.Backgroundactivity(classifiedascontinuous,discontinuoushigh-voltage,discontinuous low-voltage,burst-suppression,continuouslow-voltage,orflattrace),presenceofsleep-wake cycling,andpresenceofseizureswereevaluated.Cranialultrasonographyinpreterminfants andcranialmagneticresonanceimagingininfantswithhypoxic-ischemicencephalopathywere performed.
Results: In the preterm group, pathological trace or discontinuous low-voltage pattern (p=0.03)andabsenceofsleep-wakecycling(p=0.019)wereassociatedwithmortalityandbrain injuryassessedbycranialultrasonography.Inpatientswithhypoxic-ischemicencephalopathy, seizurepatternsonamplitude-integratedelectroencephalographytraceswereassociatedwith mortalityorbrainlesionincranialmagneticresonanceimaging(p=0.005).
夽
Pleasecitethisarticleas:VarianeGF,MagalhãesM,GasperineR,AlvesHC,ScoppettaTL,FigueredoRJ,etal.Earlyamplitude-integrated electroencephalographyformonitoringneonatesathighriskforbraininjury.JPediatr(RioJ).2017;93:460---6.
∗Correspondingauthor.
E-mail:[email protected](G.F.Variane).
http://dx.doi.org/10.1016/j.jped.2016.12.003
Conclusion: This studysupports previousresultsand demonstratestheutility of amplitude-integratedelectroencephalographyformonitoringbrainfunctionandpredictingearlyoutcome inthestudiedgroupsofinfantsathighriskforbraininjury.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradePediatria.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
PALAVRAS-CHAVE Recém-nascido; Lesãocerebral; EEGdeamplitude integrada; Resultadoprecoce
Eletroencefalogramadeamplitudeintegradaprecocenomonitoramentodeneonatos comriscoelevadodelesãocerebral
Resumo
Objetivo: Este estudovisou correlacionarosachados doeletroencefalogramade amplitude integrada (aEEG)comresultadosprecoces,medidospormortalidadeeachadosde neuroim-agem,emumacoorteprospectivadeneonatoscomriscoelevadodelesãocerebralemnosso centronoBrasil.
Métodos: Oestudoprospectivodecoortecegoavaliou23neonatosprematurosabaixode31 semanasdeidadegestacional(IG)e17neonatosdiagnosticadoscomEncefalopatia Hipóxico-Isquêmica(EHI)secundáriaàasfixiaperinatal,comIGsuperiora36semanas,monitoradoscom aEEGemumcentroterciáriopúblicodefevereirode2014ajaneirode2015.Foramavaliadas aatividadedebase(classificadacomopadrãocontínuo,descontínuodealtavoltagem, descon-tínuodebaixavoltagem,supressãodeexplosão,contínuodebaixavoltagemoutrac¸oplano), apresenc¸adeciclodosono-vigíliaeapresenc¸adeconvulsões.Foramfeitasaultrassonografia cranianaemprematurosearessonânciamagnética(RM)cranianaemneonatoscomEHI. Resultados: Nogrupodeprematuros,otrac¸opatológicooupadrãodescontínuodebaixa volt-agem(p=0,03)eaausênciadeciclodosono-vigília(p=0,019)foramassociadosamortalidadee lesãocerebralavaliadaporultrassonografiacraniana.EmpacientescomEHI,ospadrõesde con-vulsãonostrac¸adosdoaEEGforamassociadosamortalidadeoulesãocerebralnaRMcraniana (p=0,005).
Conclusão: EsteestudocorroboraosresultadosanterioresedemonstraautilidadedoaEEGno monitoramentodafunc¸ãocerebralenapredic¸ãodealterac¸õesprecocesnosgruposdeneonatos estudadoscomriscoelevadodelesãocerebral.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileiradePediatria.Este ´
eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
Introduction
The incidence of neurodevelopmental impairment in extremelypreterminfantsandthosewithhypoxic-ischemic encephalopathy (HIE) secondary to perinatal asphyxia remains high inspite of advancesin perinatalcare. Stud-ieshaveestimatedaglobalincidenceof345,000premature infantsand233,000infantswithHIEperyearwith moder-ate/severeneurologicalimpairment.1,2Bothpopulationsare
consideredathighriskforbraininjury.
Differentimagingmethodscanevaluatebraininjuryand assess neurological prognosis.3---5 Acute
electroencephalo-graphicabnormalitiesresultfromneuronaldisorganization and correlate with cognitive impairment.6,7
Amplitude-integratedelectroencephalography(aEEG) providesa clin-ically accessible method for continuous observation of cerebral background activity in illinfants at thebedside. Thus, the utility of early aEEG for the assessment of the severityofcerebralinjuryandadverseoutcomesin prema-ture infants hasbeen investigated asa tool for assessing initialneonatalrisk.8---10
The aEEGpattern is well correlated withconventional EEG,andresultsintermnewbornswithperinatalasphyxia
showedgoodpredictivevalueofshort-andlong-term neuro-logicalprognosis.11---13Otherstudieshaveshownthatsevere
electroencephalographicabnormalitiesinpretermneonates evaluatedduringthefirst72hoflifearerelatedto neurode-velopmentalimpairment.14,15
Giventheseverityofbraininjury,aswell itshigh mor-bidityand mortality rate,the identification of prognostic factors with appropriate timing to provide early future interventions is relevant. Therefore, this study aimed to correlateaEEGfindingswithearlyoutcomes,measuredby mortalityandneuroimagingfindings,inaprospectivecohort ofinfantsathighriskforbraininjuryinthiscenterinBrazil.
Methods
incompatiblewithlife wereexcluded, asthese conditions couldaffecttheresults.
The criteria for perinatal hypoxic-ischemic events included the presence of at least two of the following: (a)Apgar scorebelow5 at 5min; (b)need for ventilation up to10min of life (intubation or ventilation under con-tinuouspositive airway pressure);(c)gas analysis of cord blood in the first hour of life with pH<7.10 or BE>−12. ThemodifiedclinicalSarnatscorewasusedtogradeHIE.16
The aEEG was recorded for 72h as a two-channel EEG frombiparietalsurfacediskelectrodesusinganEEGdevice (Neuron-Spectrum-4 and 5 systems with Neurospectrum softwaremoduleforaEEGandtrending---Neurosoft,Russia). NewbornswithHIEwhoweretreatedwiththeinstitutional hypothermia protocol were evaluated for an additional 24h in order to monitor the rewarming phase. In brief, theobtained signalwasfiltered, rectified,smoothed, and amplitude-integratedbeforeitwasprintedoutordigitally availableonthemonitorataslowspeed(6cm/h),directly atthebedside.
Therecordingswereanalyzedbytwoindependent read-ersandregisteredasshownbelow17:
1) Backgroundactivity:
- Continuous voltage pattern (CVP): continuous activ-itywithminimumamplitudeabove5Vandmaximum amplitudeabove10V.
- Discontinuous voltage pattern (DC): discontinuous activitywithminimumamplitudebelow5Vand max-imumamplitudeabove10V.Forpretermevaluation this study also used the sub-classification proposed byOlischaretal.18 andthispatternwasfurther
sub-divided into: (a) discontinuous high voltage pattern (DHVP) --- minimum range between 3 and 5V; (b) discontinuouslow voltagepattern(DLVP) ---minimum rangebelow3V.
- Burst suppression: discontinuous activity with mini-mum amplitude without variability at 0---1/2V,and burstswithamplitude>25V.
- Inactive, flat trace(FT):mainly inactive background (electrocerebral inactivity) with amplitude always below5V.
2) Sleep-wake cycling (SWC): characterized by sinusoidal smoothcyclicvariations,mainlyoftheminimum ampli-tude. It was further categorized as developed SWC, immatureSWC,andnoSWC.
3) Seizures:characterizedasanabruptriseinminimumand maximum amplitude,categorizedassingleseizures(no morethanoneseizurepereachperiodof30minof anal-ysis),repetitiveseizures(morethanoneelectrographic seizurepereach 30min periodof analysisbut nomore than oneelectrographic seizure over a 10min period), or statusepilepticus (ongoing seizure activity >30min, presentas‘‘sawtoothpattern’’orascontinuousincrease oftheloweranduppermargins,ormorethanone elec-trographicseizureovera10minperiod).19
4) NewbornswithHIEwerefurtherassessedbytimeto nor-maltrace(TTNT):calculatedbythenumberofhoursof life toregainnormalaEEGactivity (continuousvoltage pattern).
Tocharacterizebackgroundactivity,4-hperiodsof ade-quate monitoring were evaluateddaily on days1, 2, and 3 of life. BothaEEG readers were blinded tothe clinical history. Cranial ultrasound (cUS) was performed at least oncea week in the neonatalperiodand cranialmagnetic resonanceimaging(MRI)wasperformed inallinfantswith HIEbetweendaysfourandtenoflife.Clinicalandimaging datawerecollectedincludingwithpre-establishedinterest variables,suchasdemographic(sex, maternalage, race), clinical(birthweight,gestationalage,Apgarscores, diagno-sisofearly-onsetsepsis,presenceofclinicalseizure,need forventilatorysupport,surfactants,andvasoactivedrugs), andimagingdata.TheMRIexaminationswereassessedby two independent neuroradiologists without knowledge of the clinical data or aEEG findings. Since the interpreta-tionagreementamongdifferentMRIratersmayaffectthe reliabilityofresults,theinterobserveragreementwasalso evaluatedinthisstudy.MRIwasperformedwithT1spinecho sequences;T1MTC;T2FSE;diffusion;andT2gradient-echo. Four radiographic findings were evaluated: lesions in the posterior limb of the internal capsule (PLIC) --- labeledas presentorabsent;lesionsinthebasalgangliaandthalamus (BGT), white matter, and corticalgray matter, labeledas normal,mild,moderate,orsevere.
In the premature group, good early outcome was defined assurvivalto 28days without severe periventric-ular/intraventricular hemorrhage(PIVH), definedasgrade IIIorIV,orperi-ventricularleukomalacia(PVL),whilepoor early outcome wasconsidered as neonataldeathor pres-enceofseverePIVHorPVL.InnewbornsfromtheHIEgroup, goodearlyoutcomewasdefinedassurvivalwithout moder-ate/severelesionassessedbycranialMRI,whilepoorearly outcomewasconsideredasdeathormoderate/severelesion assessed by cranial MRI. Presence of PIVH was evaluated according to Papile classification.The HIE cohort pattern ofbraininjurywasclassifiedaccordingtoabnormalitiesin brainregionsknowntobesusceptibleinHIE,basedon crite-riapublishedbyRutherfordetal.20
Statisticalanalysis
Adescriptiveanalysiswasperformedusingpercentageand number of validcases for categorical variablesaswell as mean, standard deviation, and number of valid cases for continuous variablesinordertoidentifythemain charac-teristicsofpatientswithhighriskforbraininjurymonitored with aEEG. Fisher’s exact test was used for analysis of categoricalvariablesandthet-testforcomparisonsof con-tinuous variables using Stata software (Stata Corp. 2013, Stata Statistical Software,version13,USA), considering a 5%significancelevelforalltests.Positive predictivevalue (PPV),negativepredictivevalue (NPV),andrisk ratio(RR) were evaluated. For inter-rater agreement analysis, the kappa coefficient () was applied,using the SPSS v. 19.0
software.
Results
Patients
Table1 Baselinecharacteristicsofmonitoredgroups.
Extremelypretermgroup Total(n=23) Goodearlyoutcome(n=10) Poorearlyoutcome(n=13) pvalue
Gestationalage(wk)(mean±SD) 28±1.7 28.3±1.3 27.6±1.6 NS
Weight(g)(mean±SD) 917±243 965±261 880±185 NS
Male(n) 12 6 6 NS
Apgar1(mean±SD) 5.2±2.5 5.9±2.8 4.7±2.1 NS
Apgar5(mean±SD) 7.9±2.6 8.9±1.2 7.1±3.2 NS
HIEgroup Total(n=17) Goodearlyoutcome(n=11) Poorearlyoutcome(n=6) pvalue
Gestationalage(wk)(mean±SD) 39±1.5 39.3±1 38.6±2.2 NS
Weight(g)(mean±SD) 3100±422 3139±217 3029±680 NS
Male(n) 14 8 6 NS
Apgar1(mean±SD) 2.2±1 2.2±0.9 2.3±1.3 NS
Apgar5(mean±SD) 4.7±1.3 4.8±1 4.7±1.8 NS
Sarnatscore(n)
Mildencephalopathy 0 0 0 NS
Moderateencephalopathy 10 6 4 NS
Severeencephalopathy 7 5 2 NS
Therapeutichypothermia(n) 17 11 6 NS
HIE,hypoxic-ischemicencephalopathy;wk,weeks;SD,standarddeviation.
the group of extremely preterm infants, gestational age ranged from26to30.4 weeks,withamean of28 weeks; birth weight ranged from 610g to 1310g, with a mean of 938g.Eight infantsin this groupdied during thestudy period.In the HIE group, gestational age ranged from 36 to 40.6 weeks, with a mean of 39 weeks; birth weight ranged from2280gto3940g,withamean of3100g,and oneinfantdied.The baselinecharacteristicsareshownin Table1.
aEEGfindings
Allpatients started monitoring withinthe firstday of life (mean 6.2h of life, range 2---16h of life) andwere moni-toredfor72---96hafterbirth.Pathological aEEGtracewas defined asflat tracing, burst-suppression, and continuous low-voltagepattern.
Extremelypretermnewborns
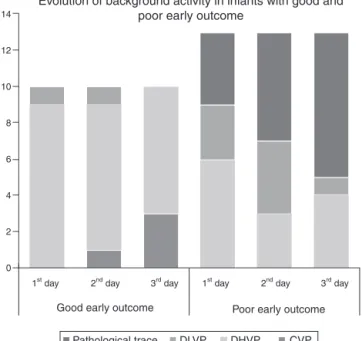
Inthepretermgroup,meantimetoinitiateaEEGmonitoring was5.2(±1.2)hoflife,andpathologicaltraceorDLVPwere associatedwithhigherratesofpoorearlyoutcome(p=0.03, PPV90.9%,NPV75%,RR=3.63).AbsenceofSWCwas asso-ciated withpoor early outcome (p=0.019, PPV 75%, NPV 87.5%,RR=1.53).TheresultsareshowninTable2.The back-groundactivityofpatientswithpoorearlyoutcomechanged fromnormal topathologicalaEEGpattern infivepatients (38.4%),whileinone(7.6%)itchangedfrompathologicalto normalaEEGpattern.Noneofthepatientswithgoodearly outcome developed pathological aEEGpattern during the periodofmonitoring.EvolutionofaEEGbackgroundactivity inpatientswithpoorearlyoutcomeandgoodearlyoutcome isshowninFig.1.
NewbornswithHIE
PatientswithHIEwereassessedforbackground activityin thefirsthoursoflife,TTNT,presenceofSWC,andseizures. SeizurepatternsonaEEGtraces(p=0.005,PPV83.3%,NPV 90.9%,RR=5.45)and longerTTNT(p=0.015)were associ-ated with poor early outcome. All the patients with HIE underwenttherapeutichypothermia.Theresultsareshown inTable2.
14
12
10
8
6
4
2
0
1st day 2nd day
Good early outcome
3rd day 1st day 2nd day
Poor early outcome
Evolution of background activity in infants with good and poor early outcome
3rd day
Pathological trace DLVP DHVP CVP
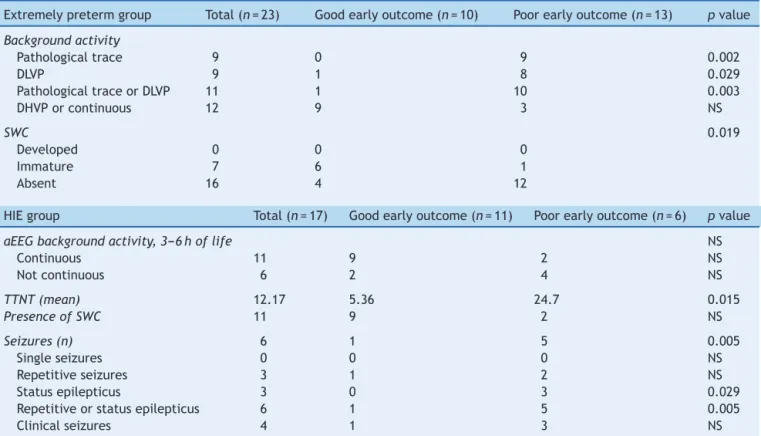
Table2 aEEGfindingsrelatedtooutcomeinextremelypretermandHIEgroups.
Extremelypretermgroup Total(n=23) Goodearlyoutcome(n=10) Poorearlyoutcome(n=13) pvalue
Backgroundactivity
Pathologicaltrace 9 0 9 0.002
DLVP 9 1 8 0.029
PathologicaltraceorDLVP 11 1 10 0.003
DHVPorcontinuous 12 9 3 NS
SWC 0.019
Developed 0 0 0
Immature 7 6 1
Absent 16 4 12
HIEgroup Total(n=17) Goodearlyoutcome(n=11) Poorearlyoutcome(n=6) pvalue
aEEGbackgroundactivity,3---6hoflife NS
Continuous 11 9 2 NS
Notcontinuous 6 2 4 NS
TTNT(mean) 12.17 5.36 24.7 0.015
PresenceofSWC 11 9 2 NS
Seizures(n) 6 1 5 0.005
Singleseizures 0 0 0 NS
Repetitiveseizures 3 1 2 NS
Statusepilepticus 3 0 3 0.029
Repetitiveorstatusepilepticus 6 1 5 0.005
Clinicalseizures 4 1 3 NS
aEEG,amplitude-integratedelectroencephalography;HIE,hypoxic-ischemicencephalopathy;DLVP,discontinuouslow-voltagepattern; DHVP,discontinuoushigh-voltagepattern;SWC,sleep-wakecycling;TTNT,timetonormaltrace.
Imagingfindings
Cranialultrasoundfindingsintheextremelypretermgroup wereasfollows:nine(39%)hadnormalcranialultrasound, one(4.3%)hadPIVHgradeI,four(17.3%)hadPIVHgradeII, four(17.3%)hadPIVH gradeIII,and three(13%)hadPIVH grade IV. Three (13%) infants developed PVL and cranial ultrasoundwasnotperformed in twodue toearly prema-ture death. MRI findings in infants withHIE are shown in Table3.MRIwasnotperformedinoneofthepatientsdue toprematuredeath.
Interobserveragreementsbetweenradiologistsregarding injury ofthe BGT, whitematter, and cortical graymatter were:75%(=0.636;p<0.001);56.3%(=0.321;p=0.029), and81.3%(=0.586;p<0.001),respectively.Theobserved agreement between radiologists regarding the PLIC was 100%(=1.0;p<0.001). Analyses of thenormal/mild and moderate/severe injury groups of the BGT, white matter, and cortical gray matter were: 100% (=1.0; p<0.001); 87.5%(=0.589;p=0.009),and93.8%(=0.764;p<0.001), respectively.
Discussion
This study was performed to evaluate the correlation betweenelectroencephalicdisordersandearlyoutcomein aprospectivecohortofinfantsathighriskforbraininjury inasampleoftheBrazilianpopulation.TheabsenceofSWC in the first 72h of life and the presence of pathological traceorDLVPactivitywereassociatedwithseverePIVHor
Table3 MRIfindingsininfantswithHIE.
Total n(%)
Poorearly outcome n(%)
Goodearly outcome n(%)
LesioninPLIC
Present 14(87.5%) 2(12.5%) 12(75%)
Absent 2(12.5%) 2(12.5%) 0(0%)
LesioninBGT
Absent 6(37.5%) 0(0%) 6(37.5%)
Mild 6(37.5%) 1(6.25%) 5(31.25%)
Moderate 2(12.5%) 2(12.5%) 0(0%)
Severe 2(12.5%) 2(12.5%) 0(0%)
Lesioninwhitematter
Absent 6(37.5%) 0(0%) 6(37.5%)
Mild 7(43.75%) 2(12.5%) 5(31.25%)
Moderate 1(6.25%) 1(6.25%) 0(0%)
Severe 2(12.5%) 2(12.5%) 0(0%)
Lesionincorticalgraymatter
Absent 2(12.5%) 0(0%) 2(12.5%)
Mild 11(68.75%) 2(12.5%) 9(56.25%)
Moderate 1(6.25%) 1(6.25%) 0(0%)
Severe 2(12.5%) 2(12.5%) 0(0%)
deathintheneonatalperiod.Infantswithpoorearly out-comemorecommonlychangedfromnormaltopathological aEEGpatternthantheopposite.Thesefindingssupportthe findingsofSoubasietal.,10whichshowedasensitivityof89%
and70%, andspecificity of 80%and 80.7%for background activity (pathologicaltraceor DLVP)andabsenceof SWC, respectively,fortheoccurrenceofadverseoutcomes(PIVH grade III/IV, PVL, or death). A recent prospective cohort studydemonstratedthatpreterminfantswithsevere cere-bral lesionsalready manifest a maturational delay in the aEEGcyclicactivitysoonafterbirth.21 Othersstudieshave
alsoreportedasignificantpositivecorrelationbetweenthe degreeofabnormalityoftheaEEGandbothUSG abnormal-itiesandpoorneurodevelopmentalprognosis.22,23
InnewbornswithHIE,thepresenceofseizures(repetitive seizuresorstatusepilepticus)patternsonaEEG/EEGtraces andlongerTTNTwereassociatedwithmoderatetosevere lesionsobservedonMRIanddeath.Earlierstudiesalsofound anassociationbetweenelectrographicseizuresandseverity offindingsoncranialMRI.24,25Aretrospectivereviewof
con-tinuousaEEGdatafromencephalopathicnewbornstreated with whole-body hypothermia found association between delayof aEEGbackground recoveryasincreasingly predic-tiveofadverseearlyoutcomeovertimeinnewbornsbeing treated with therapeutic hypothermia.26 Thoresen et al.
havedescribedthattherecoverytimetonormalbackground patternwasthebestpredictorofpooroutcomebytheage at2yearsinneonateswithbirthasphyxia.27Arecent
meta-analysis showedthat aEEGcan be usedas predictive and prognostictoolinpreterminfants,withaspecificityof93% andsensitivityof84%.28
The present study showeda goodinterobserver agree-mentinMRIevaluations;however,shouldthisbeinterpreted withcautionduetothesmallsamplesize.
Strengths of this study included an independent and blinded radiographic review and the use of two-channel montage associated with the interpretation of raw EEG technique(aEEG/EEG),asit isknowntoincrease the sen-sitivity and specificity of the method.29,30 Limitations of
the study were the relatively smallsample size, the lack ofstratificationbytheuseofantiepilepticdrugs,sedation orothermedicationswhichmightpotentiallyinfluencethe aEEGtrace,andlackofknowledgeregardingtimingofbrain injury,especiallyinthepretermgroup,inwhichinjurycould occuraftertheperiodofaEEGmonitoring.
In conclusion, this study confirmsthat previous results areapplicabletothestudiedpopulation,andthusaEEGisa justifiedtoolintheneonatalintensivecareunittomonitor thisgroupofneonatesathighriskforbraininjury.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BlencoweH,LeeAC,CousensS,BahalimA,NarwalR, Zhong N,etal.Pretermbirth-associatedneurodevelopmental impair-mentestimatesatregionalandgloballevelsfor2010.Pediatr Res.2013;74:17---34.
2.LeeAC,KozukiN, BlencoweH,VosT, BahalimA, Darmstadt GL,etal.Intrapartum-relatedneonatalencephalopathy inci-denceand impairmentatregional andglobal levelsfor 2010 withtrendsfrom1990.PediatrRes.2013;74:50---72.
3.LeijserLM,deBruïneFT,SteggerdaSJ,vanderGrondJ,Walther FJ,vanWezel-MeijlerG.Brainimagingfindingsinverypreterm infantsthroughouttheneonatalperiod:partI.Incidencesand evolutionoflesions,comparisonbetweenultrasoundandMRI. EarlyHumDev.2009;85:101---9.
4.ShankaranS,SlovisTL,BedardMP,PolandRL.Sonographic clas-sification of intracranial hemorrhage. A prognostic indicator ofmortality,morbidity,andshort-termneurologicoutcome.J Pediatr.1982;100:469---75.
5.WatanabeK,HayakawaF,OkumuraA.NeonatalEEG:apowerful toolintheassessmentofbraindamageinpreterminfants.Brain Dev.1999;21:361---72.
6.LeBihannicA,BeauvaisK,BusnelA,deBaraceC,FurbyA. Prog-nosticvalueofEEGinveryprematurenewborns.ArchDisChild FetalNeonatalEd.2012;97:F106---9.
7.OkumuraA,HayakawaF,KatoT,KunoK,WatanabeK. Develop-mentaloutcomeandtypesofchronic-stageEEGabnormalities inpreterminfants.DevMedChildNeurol.2002;44:729---34. 8.BowenJR,ParadisisM,ShahD.DecreasedaEEGcontinuityand
baselinevariabilityinthefirst48hoursoflifeassociatedwith poor short-term outcome in neonates born before 29weeks gestation.PediatrRes.2010;67:538---44.
9.ChalakLF,SikesNC,MasonMJ,KaiserJR.Low-voltageaEEGas predictorofintracranialhemorrhageinpreterminfants.Pediatr Neurol.2011;44:364---9.
10.SoubasiV,MitsakisK,SarafidisK,GrivaM,NakasCT,Drossou V.Earlyabnormal amplitude-integrated electroencephalogra-phy(aEEG)isassociatedwithadverse short-termoutcomein prematureinfants.EurJPaediatrNeurol.2012;16:625---30. 11.TosoPA,GonzálezAJ,PérezME,KattanJ,FabresJG,TapiaJL,
etal.ClinicalutilityofearlyamplitudeintegratedEEGin mon-itoringtermnewbornsatriskofneurologicalinjury.JPediatr (RioJ).2014;90:143---8.
12.alNaqeebN,EdwardsAD,CowanFM,AzzopardiD.Assessment ofneonatalencephalopathybyamplitude-integrated electroen-cephalography.Pediatrics.1999;103:1263---71.
13.ToetMC,Hellström-WestasL,GroenendaalF,EkenP,deVries LS.AmplitudeintegratedEEG3and6hoursafterbirthinfull termneonateswithhypoxic-ischaemicencephalopathy.ArchDis ChildFetalNeonatalEd.1999;81:F19---23.
14.Klebermass K, Olischar M, Waldhoer T, Fuiko R, Pollak A, WeningerM.Amplitude-integratedEEGpatternpredictsfurther outcomeinpreterminfants.PediatrRes.2011;70:102---8. 15.Wikström S,Pupp IH,RosénI,Norman E, FellmanV,Ley D,
etal.Earlysingle-channelaEEG/EEGpredictsoutcomeinvery preterminfants.ActaPaediatr.2012;101:719---26.
16.SarnatHB,SarnatMS.Neonatalencephalopathyfollowingfetal distress. A clinical and electroencephalographic study. Arch Neurol.1976;33:696---705.
17.Hellström-WestasL,RosénI.Continuousbrain-function moni-toring:stateoftheartinclinicalpractice.SeminFetalNeonatal Med.2006;11:503---11.
18.Olischar M, Klebermass K, Kuhle S, Hulek M, Kohlhauser C, RücklingerE,etal.Referencevaluesforamplitude-integrated electroencephalographic activity in preterm infants younger than30weeks’gestationalage.Pediatrics.2004;113:e61---6. 19.Mizrahi EM. Acute and chronic effects of seizures in the
developingbrain:lessonsfromclinicalexperience.Epilepsia. 1999;40:S42---50,discussionS64---6.
21.NatalucciG,RoussonV,BucherHU,BernetV,HagmannC,Latal B. Delayed cyclic activity development on early amplitude-integrated EEG in the preterm infant with brain lesions. Neonatology.2013;103:134---40.
22.Song J, Zhu C, Xu F, Guo J, Zhang Y. Predictive value of early amplitude-integrated electroencephalography for later diagnosed cerebralwhite matterdamageinpreterminfants. Neuropediatrics.2014;45:314---20.
23.Benavente-Fernández I, Lubián-López SP, Jiménez-Gómez G, Lechuga-SanchoAM,Garcia-AllozaM.Low-voltagepatternand absenceofsleep-wakecyclesareassociatedwithsevere hem-orrhage and death in very preterm infants. Eur J Pediatr. 2015;174:85---90.
24.ShahDK,WusthoffCJ,ClarkeP,WyattJS,RamaiahSM,DiasRJ, etal.Electrographicseizuresareassociatedwithbraininjuryin newbornsundergoingtherapeutichypothermia.ArchDisChild FetalNeonatalEd.2014;99:F219---24.
25.GlassHC, Nash KB,BonifacioSL, BarkovichAJ, FerrieroDM, Sullivan JE,et al.Seizuresand magneticresonance imaging-detectedbraininjuryinnewbornscooledforhypoxic-ischemic encephalopathy.JPediatr.2011;159:731---5.e1.
26.MassaroAN, Tsuchida T, Kadom N, El-DibM, GlassP, Baum-gartS,etal.aEEGevolutionduringtherapeutichypothermia andpredictionofNICUoutcomeinencephalopathicneonates. Neonatology.2012;102:197---202.
27.ThoresenM,Hellström-WestasL,LiuX,deVriesLS.Effectof hypothermiaonamplitude-integratedelectroencephalogramin infantswithasphyxia.Pediatrics.2010;126:e131---9.
28.LinB, Zhang P,Cheng G, Zhou W, Wang L. Meta-analysis of prognostictestsinneonatesover35-weekgestationalagewith hypoxic-ischemic encephalopathy. Zhonghua Yi Xue Za Zhi. 2014;94:115---21.
29.Lavery S, Shah DK,Hunt RW,Filan PM,Doyle LW, InderTE. Single versus bihemispheric amplitude-integrated electroen-cephalographyin relationto cerebralinjury and outcome in the term encephalopathic infant. J Paediatr Child Health. 2008;44:285---90.