www.jped.com.br
ORIGINAL
ARTICLE
Prevalence
and
factors
associated
with
smoking
among
adolescents
夽
,
夽夽
Marilyn
Urrutia-Pereira
a,b,
Vinicius
J.
Oliano
c,
Carolina
S.
Aranda
d,
Javier
Mallol
e,
Dirceu
Solé
d,∗aUniversidadeFederaldoPampa(UNIPAMPA),Uruguaiana,RS,Brazil
bPontifíciaUniversidadeCatólicadoRioGrandedoSul(PUC-RS),PortoAlegre,RS,Brazil cUniversidadedaRegiãodaCampanha(URCAMP),Alegrete,RS,Brazil
dUniversidadeFederaldeSãoPaulo(UNIFESP),EscolaPaulistadeMedicina(EPM),DepartamentodePediatria,SãoPaulo,RS,
Brazil
eUniversidadedeSantiagodoChile(USACH),HospitalCRSElPino,DepartamentodeMedicinaRespiratóriaPediátrica,Santiago,
Chile
Received12April2016;accepted13July2016 Availableonline22November2016
KEYWORDS
Tobacco; Adolescent;
Riskfactors;
Cigarette
Abstract
Objective: Despite anti-smoking prevention programs, many adolescents start smoking at schoolage.Themainobjectivesofthisstudyweretodeterminetheprevalenceandriskfactors associatedwithsmokinginadolescentslivinginUruguaiana,RS,Brazil.
Methods: Aprospectivestudywasconductedinadolescents(12---19years),enrolledin munic-ipalschools,whoansweredaself-administeredquestionnaireonsmoking.
Results: 798adolescentswereenrolledinthestudy,withequaldistributionbetweengenders. Thetobaccoexperimentation frequency(evertriedacigarette, evenoneortwo puffs)was 29.3%; 14.5% started smokingbefore 12 years ofage and13.0% reportedsmoking atleast onecigarette/daylastmonth.Havingasmokingfriend(OR:5.67,95%CI:2.06---7.09),having cigarettesofferedbyfriends(OR:4.21,95%CI:2.46---5.76)andhavingeasyaccesstocigarettes (OR:3.82,95%CI:1.22---5.41)wasidentifiedasfactorsassociatedwithsmoking.Havingparental guidanceonsmoking(OR:0.67,95%CI:0.45---0.77),havingnocontactwithcigarettesathome inthelastweek(OR: 0.51,95%CI:0.11---0.79)andknowingaboutthedangersofelectronic cigarettes(OR:0.88,95%CI:0.21---0.92)wereidentifiedasprotectionfactors.
夽 Pleasecitethisarticleas:Urrutia-PereiraM,OlianoVJ,ArandaCS,MallolJ,SoléD.Prevalenceandfactorsassociatedwithsmoking
amongadolescents.JPediatr(RioJ).2017;93:230---7.
夽夽StudycarriedoutatEscolaPaulistadeMedicina(EPM),UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](D.Solé). http://dx.doi.org/10.1016/j.jped.2016.07.003
Conclusion: TheprevalenceofsmokingamongadolescentsinUruguaianaishigh.The imple-mentationofmeasurestoreduce/stoptobaccouseanditsnewformsofconsumption,suchas electroniccigarettesandhookah,areurgentandimperativeinschools.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
PALAVRAS-CHAVE
Tabaco; Adolescente;
Fatoresderisco;
Cigarro
Prevalênciaefatoresassociadosaotabagismoentreadolescentes
Resumo
Objetivo: Apesardosprogramasdeprevenc¸ãoantitabagista,muitosadolescentescomec¸ama fumarnaidadeescolar.Foramobjetivosdoestudodeterminaraprevalênciaeosfatoresde riscoassociadosaoconsumodetabacoemadolescentesmoradoresdomunicípiodeUruguaiana RS,Brasil.
Métodos: Estudotransversal, realizado em adolescentes de12 a 19 anos, matriculados em escolasdomunicípio,queresponderamquestionárioautoaplicávelsobretabagismo.
Resultados: Participaram798adolescentescomigualdistribuic¸ãoentreosgêneros.A frequên-ciadeexperimentac¸ãodetabaco(Algumaveztentoufumarumcigarro,mesmoqueumaou duastragadas)foi29,3%,sendoque14,5%comec¸aramfumarantesdos12anosdevidae13,0% delesafirmaramterem fumadopelomenosumcigarro/dianoúltimomês. Foram identifica-doscomoassociadosaotabagismo:teramigotabagista(OR:5,67,IC95%:2,06-7,09),teroferta decigarropeloamigo(OR:4,21,IC95%:2,46-5,76)efacilidadedeconseguircigarros(OR:3,82, IC95%:1,22-5,41).Terorientac¸õesdospaissobretabagismo(OR:0,67,IC95%:0,45-0,77),nãoter contatocomcigarroemcasanaúltimasemana(OR:0,51,IC95%:0,11-0,79)esaberosmalefícios docigarroeletrônico(OR:0,88,IC95%:0,21-0,92)foramidentificadoscomodeprotec¸ão. Conclusões: A prevalência de tabagismo entre os adolescentes de Uruguaiana é alta. A implantac¸ãode medidasnasescolaspara reduzirouacabaroconsumo detabacoedesuas novasmodalidades,comooscigarroseletrônicoseonarguilééurgenteeimperiosa.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Tobaccouseistheleadingpreventablecauseofdeathand
diseases worldwide and it is estimated that in the 21st
century, one billion people will die becauseof smoking.1
Approximately80%ofsmokersintheworldliveincountries with low and/or medium income, where the burden of tobacco-relateddiseaseshasagreatimpact.2
Atotalof11%ofdeathsfromischemicheartdiseaseand 70%ofdeathsfromlung,bronchial,andtrachealcancerare attributedtotobaccouse.Itisbelievedthattheincreased prevalenceofsmokingobservedindevelopingcountriesover the years will be responsible for a two-fold increase in theoverloadofhealthcarefornon-communicablediseases.3
Therefore,itisnecessarytoestablishanefficientand sys-tematicsurveillancemechanismtomonitorthetrendsofuse oftobaccoanditsderivatives.4
An international collaborative study of schoolchildren from131countriesshowedthatadolescentsarethegroup with the highest risk for smoking initiation, since the overallprevalence ofschoolchildrenwhoareactive smok-ers was 8.9%, being higher in the Americas (17.5%) and Europe (17.9%), and less than 10% in other assessed regions.5
In Brazil, the National School-Based Health Sur-vey (Pesquisa Nacional de Saúde do Escolar [PeNSE])
documented that 30% of young individuals aged between 13and15 startedsmokingbefore12yearsof age.6 Ithas
beenreportedthathabitsacquiredatthisstageoflifeare usuallykeptatadulthoodandaredifficulttomodify,7and
thatalthoughadolescentshaveknowledgeoftherisksthat areinvolvedintheconsumption oftobaccoandits deriva-tives, theirhabits seem tobedivergent.8 Itis during the
transitionyears,duringhighschoolandcollege/university, thattobaccouse starts,aswell asgreater stabilizationof smokingbehavior.9
Forthisreason,overthepastdecades,theschool envi-ronmenthasbeenthefocusofspecificeffortstoinfluence thebehaviorofadolescents,byusingappropriate interven-tionstohelpthemavoidtobaccouseatsuchanearlystage intheirlives.10,11
Thus,consideringtheconsumptionofcigarettesby ado-lescentsasariskbehaviortotheirhealthandthatalthough arecentBrazilianstudy12showedareductioninthe
preva-lenceofsmokingamongyoungindividuals,particularlythose ina vulnerable socio-economiccondition, smoking among adolescentsitisstillamajorchallengeinthecityof Urugua-iana,stateofRioGrandedoSul,Brazil.
Methods
Studydesign
ProspectivestudycarriedoutbetweenMarchandJune2015
inthecityofUruguaiana,RS,whosepopulationisestimated
at125,435inhabitants,ofwhich6%areattheagerangeof
thestudy,i.e.,12---19years.13
Ofthe66 schoolsinthe municipality(31municipal,32 state, and three private schools) 51 were excluded (31 municipaland20stateschools)asthestudentsenrolledin these schools were not at the age range assessed in the study.Of the 15 remaining schools, eight were randomly selectedforthestudy.Duringthesecondphase,classes con-tainingstudentsattheagegroupassessedinthestudywere randomly selected in each school and the students were invitedtoparticipate.
Samplesizecalculation
The sample size calculation was performed using these
parameters: prevalence of 10% for tobacco consumption
withaconfidencelevelof95%andalphaerrorof5%,
result-ing in 750 students, plus 20% for eventual losses, which
resultedinafinalsampleof900students.
ThestudywasapprovedbytheEthicsCommitteeof
Hos-pitalSantaCasadeCaridadeofUruguaianaandwasgranted
permissiontocarryouttheresearchbytheDepartmentof
StateEducation andrespectiveprivateschools in
Urugua-iana.
All adolescents signed the free and informed consent
form,andthoseyounger than18 yearsalso hadthe form
signedbytheirparents/guardians.
Datacollection
The adolescents allowed to participate in the study
answeredtheself-administeredquestionnaireinthe
class-room,andduetoconfidentialityissues,wereidentifiedonly
byageandgender.Thequestionnaireswerefilledoutwith
thehelpofatrainedinvestigator(VJO,physicaleducation
teacher)presentintheclassroomatthattime.
The self-administered questionnaire used in the study
was the California Tobacco Survey,14 translated into
Por-tugueseandadaptedtotheBrazilian cultureaccording to international recommendations.15 The questionnaire was
independentlytranslatedintoPortuguese bytwoBrazilian physiciansspecializedinallergies(forwardtranslation).The two translations were compared by two other physicians and disagreements were eliminated after consensus. The productwasthentranslatedintoEnglishbyanative English-speaking translator (backward translation) and compared totheoriginalquestionnaire,withnorelevantdifferences found betweenthem. The final versionin Portuguese was administeredtoagroupofadolescentstoassesstheir under-standinganddifficultiesinansweringit,andafewlinguistic adaptationswereperformed(patienttesting).Afew adjust-mentsweremadeandthefinalversionofthequestionnaire wascompleted(Tables1and2).
The questionnaire consists of questions related to tobacco andsmoking, aswell as thoughts and knowledge on tobacco(Table 1) and exposure tosmoke from others (Table2),thesmokingstatusoffamilymembersandfriends, andknowledgeofhazardoussmokinghabits.
Theadolescentsthatsmokedcigarettesatsomepointin their lives(have youever tried smokingacigarette,even oneortwopuffs?)wereconsideredexperimentalsmokers. Adolescents whosmoked cigaretteson‘‘oneormoredays in thelastthirtydays’’wereconsidered currentsmokers, asrecommendedbytheCentersforDiseasePreventionand Control(CDC)andtheWorldHealthOrganization(WHO).15
Statisticalanalysis
Afterreviewingthereturnedquestionnaires,102were
dis-carded due to questionnaire completion errors and the
remaining 798 were analyzed. The obtained data were
transferred toan Excel spreadsheetfor further statistical
analysis. Considering smoking as the dependent variable,
the resultswereshown in relationtothe exposureor not
tosmoke,usingthechi-squaredorFisher’sexacttest.The
variablesidentifiedassignificant(p<0.05)wereusedinthe
logistic regression model (stepwise backward) and
signifi-cantdifferenceswereidentified.
Results
A total of 798 questionnaireswere adequately filled out,
withequaldistributionbygender,astheyweredistributed
inequalnumberstobothgendersineachclassroom.
According to the affirmative answer to the question
‘‘Haveyouevertriedacigarette,evenoneortwopuffs?’’
adolescents were characterized as ‘‘has tried smoking’’
(n=234), and the ones that answered no, as ‘‘never
smoked’’(n=564).
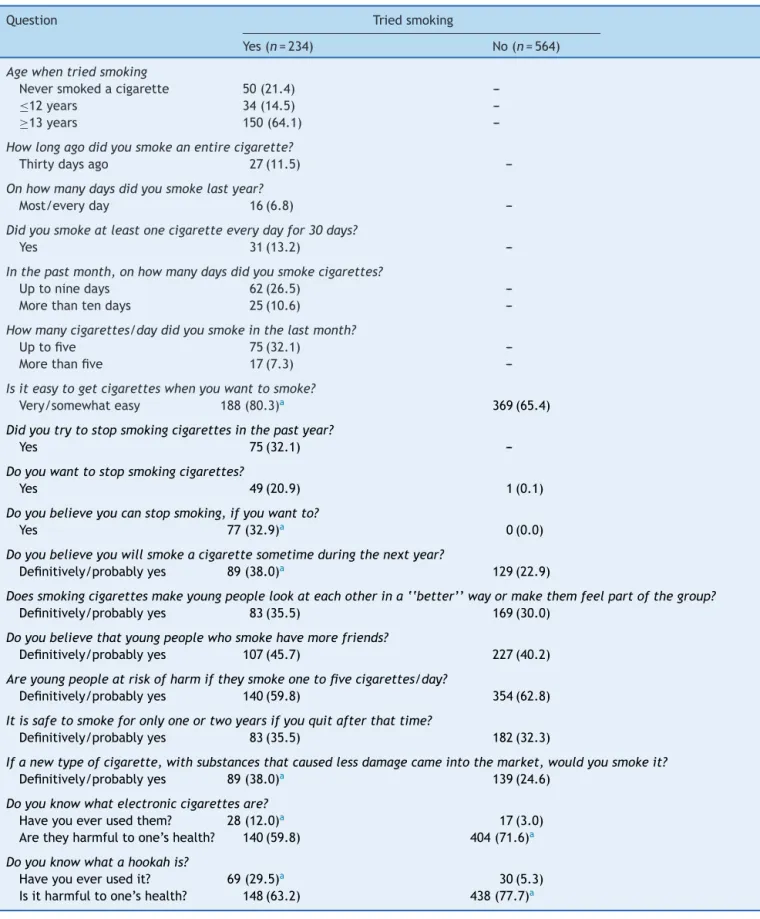
Table1summarizestheadolescents’answersregarding smoking. A total of 29.3% reported having tried smoking (234/798), whereas21.4% (50/234)reported neverhaving smoked an entirecigarette,14.5% startedsmokingbefore age12,and64.1%after13yearsold.
When asked about how long ago they had smoked an entire cigarette, 11.5% reported smoking in the last month(Table1).Although6.8%(16/234)oftheadolescents reportedhavingsmoked onmost daysor everyday inlast month, 13.2%(31/234) hadsmoked at least onecigarette every day and 32.1% (75/234) had smoked at least five cigarettesinthelast30days(Table1).Additionally,32.1% (75/234) reportedhavingtriedtoquitsmokingin thelast yearand32.9%(77/234)believed theycouldstopsmoking iftheywantedto(Table1).
Thecomparativeanalysisbetweenthetwogroups signif-icantlyshowedthat80.3%ofthosewhotriedsmokingsaid they thoughtit was very/somewhateasy tostop smoking iftheywantedto, 32.9%(77/234) believedtheywouldbe abletoquitsmokingiftheywantedto,and20.9%(49/234) reportedtheywantedtoquitsmoking.
Table1 Adolescents’answersregardingtobaccouseandthoughtsaboutit.
Question Triedsmoking
Yes(n=234) No(n=564)
Agewhentriedsmoking
Neversmokedacigarette 50(21.4)
---≤12years 34(14.5)
---≥13years 150(64.1)
---Howlongagodidyousmokeanentirecigarette?
Thirtydaysago 27(11.5)
---Onhowmanydaysdidyousmokelastyear?
Most/everyday 16(6.8)
---Didyousmokeatleastonecigaretteeverydayfor30days?
Yes 31(13.2)
---Inthepastmonth,onhowmanydaysdidyousmokecigarettes?
Uptoninedays 62(26.5)
---Morethantendays 25(10.6)
---Howmanycigarettes/daydidyousmokeinthelastmonth?
Uptofive 75(32.1)
---Morethanfive 17(7.3)
---Isiteasytogetcigaretteswhenyouwanttosmoke?
Very/somewhateasy 188(80.3)a 369(65.4)
Didyoutrytostopsmokingcigarettesinthepastyear?
Yes 75(32.1)
---Doyouwanttostopsmokingcigarettes?
Yes 49(20.9) 1(0.1)
Doyoubelieveyoucanstopsmoking,ifyouwantto?
Yes 77(32.9)a 0(0.0)
Doyoubelieveyouwillsmokeacigarettesometimeduringthenextyear?
Definitively/probablyyes 89(38.0)a 129(22.9)
Doessmokingcigarettesmakeyoungpeoplelookateachotherina‘‘better’’wayormakethemfeelpartofthegroup? Definitively/probablyyes 83(35.5) 169(30.0)
Doyoubelievethatyoungpeoplewhosmokehavemorefriends?
Definitively/probablyyes 107(45.7) 227(40.2)
Areyoungpeopleatriskofharmiftheysmokeonetofivecigarettes/day?
Definitively/probablyyes 140(59.8) 354(62.8)
Itissafetosmokeforonlyoneortwoyearsifyouquitafterthattime?
Definitively/probablyyes 83(35.5) 182(32.3)
Ifanewtypeofcigarette,withsubstancesthatcausedlessdamagecameintothemarket,wouldyousmokeit? Definitively/probablyyes 89(38.0)a 139(24.6)
Doyouknowwhatelectroniccigarettesare?
Haveyoueverusedthem? 28(12.0)a 17(3.0) Aretheyharmfultoone’shealth? 140(59.8) 404(71.6)a
Doyouknowwhatahookahis?
Haveyoueverusedit? 69(29.5)a 30(5.3) Isitharmfultoone’shealth? 148(63.2) 438(77.7)a
Chi-squared/Fisher’sexacttest.
a Significantlyhigherthantheothergroup.
cigarettesmadetheirpeerslookatthemina‘‘better’’way
ormadethemfeelpartofthegroupandthatsmokershad
more friends,although theyfeltthat smokingone tofive
cigarettesadaydidnotputthematriskandthatsmoking
forone totwoyearswould besafe,iftheystoppedafter
thisperiod(Table1).
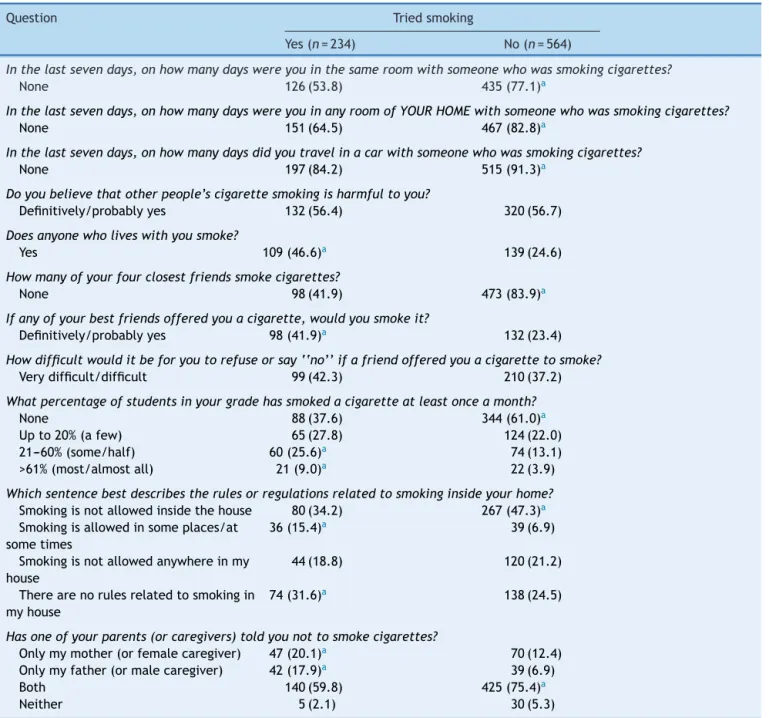
Table2 Adolescents’answersrelatedtoexposuretootherpeople’ssmoking.
Question Triedsmoking
Yes(n=234) No(n=564)
Inthelastsevendays,onhowmanydayswereyouinthesameroomwithsomeonewhowassmokingcigarettes?
None 126(53.8) 435(77.1)a
Inthelastsevendays,onhowmanydayswereyouinanyroomofYOURHOMEwithsomeonewhowassmokingcigarettes?
None 151(64.5) 467(82.8)a
Inthelastsevendays,onhowmanydaysdidyoutravelinacarwithsomeonewhowassmokingcigarettes?
None 197(84.2) 515(91.3)a
Doyoubelievethatotherpeople’scigarettesmokingisharmfultoyou?
Definitively/probablyyes 132(56.4) 320(56.7)
Doesanyonewholiveswithyousmoke?
Yes 109(46.6)a 139(24.6)
Howmanyofyourfourclosestfriendssmokecigarettes?
None 98(41.9) 473(83.9)a
Ifanyofyourbestfriendsofferedyouacigarette,wouldyousmokeit?
Definitively/probablyyes 98(41.9)a 132(23.4)
Howdifficultwoulditbeforyoutorefuseorsay‘‘no’’ifafriendofferedyouacigarettetosmoke? Verydifficult/difficult 99(42.3) 210(37.2)
Whatpercentageofstudentsinyourgradehassmokedacigaretteatleastonceamonth?
None 88(37.6) 344(61.0)a
Upto20%(afew) 65(27.8) 124(22.0)
21---60%(some/half) 60(25.6)a 74(13.1)
>61%(most/almostall) 21(9.0)a 22(3.9)
Whichsentencebestdescribestherulesorregulationsrelatedtosmokinginsideyourhome? Smokingisnotallowedinsidethehouse 80(34.2) 267(47.3)a Smokingisallowedinsomeplaces/at
sometimes
36(15.4)a 39(6.9)
Smokingisnotallowedanywhereinmy house
44(18.8) 120(21.2)
Therearenorulesrelatedtosmokingin myhouse
74(31.6)a 138(24.5)
Hasoneofyourparents(orcaregivers)toldyounottosmokecigarettes?
Onlymymother(orfemalecaregiver) 47(20.1)a 70(12.4) Onlymyfather(ormalecaregiver) 42(17.9)a 39(6.9)
Both 140(59.8) 425(75.4)a
Neither 5(2.1) 30(5.3)
Chi-squared/Fisher’sexacttest.
ap<0.05---significantlyhigherthantheothergroup.
triedsmokingand 24.6%of thosewhodid notsmokesaid
theywouldusethem(Table1).Amongtheadolescentswho
triedsmoking,therewasasignificantlygreateraccountof knowledgeofelectroniccigarettesandhookahswhen com-pared tothose who never smoked; the use of electronic cigarettes and hookahs wasalso higher amongthose who hadtriedsmoking(Table1).Incontrast,amongthosewho hadneversmoked,therewasagreaterknowledgeofboth (electroniccigarettesandhookahs)beingharmfultohealth (Table1).
Regardingexposuretosmokefromotherpeople,itwas observed that those whotried smokingwere significantly moreexposedtootherpeople’stobaccosmokeathome,in thebedroom,orinthecar(Table2).Nevertheless,therewas
nosignificantdifferencebetweenthetwogroupsregarding thethoughtthatthesmokefromotherswouldcause dam-age:56.4% forthosewhohadtried smokingand56.7%for thosewhohadneversmoked(Table2).
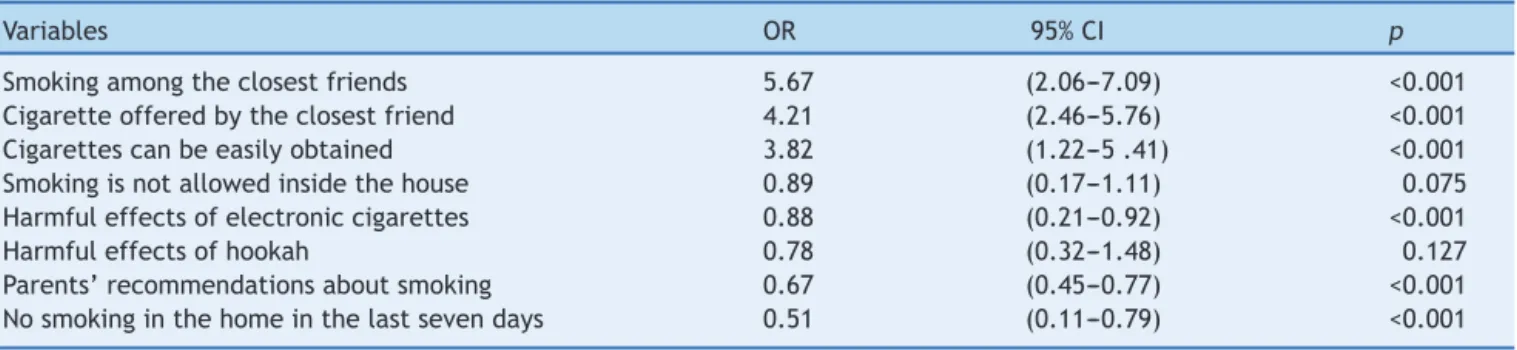
Table3 Factorsidentifiedasrelatedtosmokinginadolescenceafterlogisticregressionanalysis.
Variables OR 95%CI p
Smokingamongtheclosestfriends 5.67 (2.06---7.09) <0.001 Cigaretteofferedbytheclosestfriend 4.21 (2.46---5.76) <0.001 Cigarettescanbeeasilyobtained 3.82 (1.22---5.41) <0.001 Smokingisnotallowedinsidethehouse 0.89 (0.17---1.11) 0.075 Harmfuleffectsofelectroniccigarettes 0.88 (0.21---0.92) <0.001
Harmfuleffectsofhookah 0.78 (0.32---1.48) 0.127
Parents’recommendationsaboutsmoking 0.67 (0.45---0.77) <0.001 Nosmokinginthehomeinthelastsevendays 0.51 (0.11---0.79) <0.001
OR,oddsratio;95%CI,95%confidenceinterval.
insidethehouse.Inbothgroups,thiscontrolisexercisedby
themotherand/orfather(Table2).
The variables identifiedassignificantlyassociatedwith smoking after the logistic regression analysis are shown in Table 3. The following were identified as risk factors forsmoking: havingfriendswhosmokes,havingcigarettes offeredbyfriends,andeasyaccesstocigarettes(Table3). Having parental guidance on smoking, not being exposed to smokingat home in the last week, and knowledge on theharmfuleffectsofelectroniccigaretteswereidentified asprotectivefactors(Table3).Thefactthat smokingwas not allowedinside thehome showed borderline value for significance.
Discussion
Adolescence is an important stage in life, when because
of thediscoveries, the concerns,the need toexplore the
unknown and venture without worrying about the
conse-quences,adolescentsoftenadoptriskybehaviors,including
cigarettesmoking.8However,although notalladolescents
whotrycigarettesbecomesmokers,experimentationisthe firststeptowardfutureadherencetoregularconsumption oftobaccoproducts.7
Thedefinitionofasmokerusedinthepresentstudywas theonerecommendedbytheWHO15andtheprevalenceof
smokingamongtheevaluatedadolescentswas37.2%,with 13.2%ofthemsmokingeveryday,higherthantherate pre-viouslyobservedinotherlocations.5Theserateswerelower
thanthoseamongthegeneralpopulationinseverallocations in Brazil(22.3---29.3%).16 However,theyweremuchhigher
thanthoseobservedinPortoAlegre:7.4%formenand9.1% inwomen.11
It is noteworthythat amongtheadolescentsevaluated here, 14.5% started cigarettesmoking before 12 yearsof ageand64.1%didsoaftertheageof13,similarlytowhat waspreviouslyobservedamongstudentsofthepublicschool system in ten Brazilian city capitals, showing that 11.6% ofstudentshadtriedsmokingbetween10and12yearsof age,17aswellasStudyofCardiovascularRisksinAdolescents
(ERICA)11where30%ofyoungindividualshadtriedsmoking
before12yearsandearlierthantheageobservedbyother authors.18
Earlyinitiationof tobaccouseis animportant prognos-tic factor for disease and should be avoided. The delay of afew yearsin thestart of consumption can reduceby
almosttwo-fold the risk of damagecaused by tobacco to health.6Ontheotherhand,itisshownthatwithincreasing
age,adolescentswhotrytobaccoanddonotinterruptthe habitbecometobaccousers,thusconsolidatingthehabitof smoking.7
The main factors associatedwithcigarette smokingby adolescentsevaluatedherewere:havingfriendswhosmoke and having cigarettes offered by friends, in addition to easyaccesstocigarettes(Table3).AlthoughinBrazilthere arelawsthat hindercigaretteaccessandconsumption by children and adolescents, such as the Child and Adoles-centStatute thatprohibitsthesale,supply,ordelivery of cigarettes to children or adolescents,19 the present data
confirmedthatthispracticehasnotbeenrespectedandit hasbeenidentifiedasariskfactorforsmoking,as80.3%of adolescentsmokersreportedeasyaccesstocigaretteswhen theywantedtosmoke(Table1).
However,onecannotblame exclusivelythelegal prod-ucttrade, asoneshouldconsidertheclandestinesales of cigarettes,such asthosethat arethe resultof smuggling andevenobtainingthemfromfriendsand/orrelativeswho smoke.Moreover,theroleofsocialnetworksininfluencing andstrengtheningsmokinghabitsis clear,which hasbeen increasinglystudiedandhasshownthathavingfriendswho smokeincreasesthe tolerance tothese habits, aswell as thepossibility of adoptingthem,20 identifiedas the main
risk factor for smoking among adolescents assessed here (Table3).ThesedataarecorroboratedbyaNorth-American study,which observed that non-smoking adolescents with friendswho smoked were morelikely tostart smokingin thefuturethanthosewhosefriendsdidnotsmoke.21
It is noteworthy that, although parental smoking was morefrequentamongadolescentsmokers(Table2),itwas not identified as a risk factor for current smoking. This is in contrast withthe observations of other studies that showthecriticalinfluenceofparentsonadolescent smok-ingbehavior. It is known that children aremore likely to reproducethebehaviorsandattitudesoftheirparents,who areconsidered by themas rolemodels;additionally, par-entswhosmokearemorelikelytoallowsmokinginsidethe house.22
Although there has been a reduction in smoking rates among parents, the same has not occurred among adolescents.23 Thissuggeststhattobaccocontrol
interven-tionsshouldbemorecomprehensiveandtargetedtoother influences, such as friends,20 school,9 visual media,24 or
toward the acquisition of new habits, such as the use of hookahs25orelectroniccigarettes,26withthelatterbeingan
importantinitiatingagentofsmoking,aswellasincreased taxrates.2
Thus, comparing the results observed in the ERICA11
and PeNSE-201227 studies, the prevalence of
experimen-tation was 18.5% vs. 19.6%, respectively, lower than the present result of 29.3%, and for current smoking, 5.7%
vs. 5.1%, against 13% among the present study’s adoles-cents.Nevertheless,onecannotruleoutthepossibilityof underreporting by the adolescents themselves, identified ascommonpracticein studies onsmoking. The low rates observedin thesenational studies11,27 possiblyreflectthe
country’spioneeringcomprehensivepolicies,whichhavea majorimpactonreducingtobaccouseamongyoung individ-uals,suchasthelegislationthatbannedsmokinginindoor public environments, the ban onadvertising in all media except at sales points, and the prohibition of misleading descriptors,suchas‘‘light’’or ‘‘ultra-light’’oncigarette packs.28
InthecityofUruguaiana(SouthBrazil),theresultswere different. The finding of higher prevalence rates in the Southcouldbe possiblydue tothe regioncultivationand production of tobacco, as well as a greater influence of Europeanmigrationthattraditionallyentails ahigh preva-lenceofsmokinghabits,whichcanbeperpetuatedthrough generations.11Toallthesefacts,onemustbeaddtheeasy
accesstocigarettes, suchasin the case of smuggling, as recentlyidentifiedinthecityofUruguaiana.29
It is importantthat anti-smokingeducational programs beencouragedinschools,sothatstudentsreceiveguidance andprofessionalhelp,especiallyforthosewhowanttoquit smoking.9,30Thedemandforspecializedhealthservices
out-sidetheschoolenvironmentcanresultinincreasedschool absenteeismand evenhindertheadolescents’accessand adherencetotheprograms.
These results reinforce theneed tostrengthen,at the municipalor statelevel,publicpoliciesaimedatreducing oreliminatingcontactofchildrenand/oradolescentswith cigarettes.Compliancewiththelawsrestrictingthesaleand consumptionofcigarettes,increasingthelegalageof pur-chase,promotinghealthy lifestyles,familyinvolvementin thepreventionofsmokinghabitprograms,priceincreases, implementationofanti-smokingprogramsinschools,aswell asappropriateguaranteedtreatmentsforsmokers,aresome ofthemeasuresthatcouldbeundertaken.
Pediatricians,beingthefirstprofessionalstocareforthe children,know theirenvironmentalexposure, followtheir development, and have a primary role as educators and promotersofhealthyhabits.
Although theconsequences ofsmokingareobserved in adulthood,itshouldbenotedthatthereductionor restric-tionof tobacco consumption in adolescence will have an educational impact on health and can reduce the possi-bilityof contactwithother restrictionsor illicit drugs, so it is essential for the physician to be attentive and well informed, and to participate in the development of new
approaches tofight againstsmoking, in anintegrated and interdisciplinarymanner.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.JhaP,PetoR. Globaleffects ofsmoking,ofquitting,and of takingtobacco.NEnglJMed.2014;370:60---8.
2.WorldHealthOrganizationWHOReportontheglobaltobacco epidemic. Geneva, Switzerland:WHO; 2015. Available from: http://www.who.int/tobacco/globalreport/2015/en/ [cited 31.01.16].
3.BoutayebA,BoutayebS.Theburdenofnoncommunicable dis-easesindevelopingcountries.IntJEquityHealth.2005;4:2. 4.VigitelVigilânciadefatoresderiscoeprotec¸ãoparadoenc¸as
crônicasporinquéritotelefônico:percentualdefumantesno Brasil. Available from: http://www2.inca.gov.br/wps/wcm/ connect/agencianoticias/site/home/noticias/2014/percentual
fumantesbrasilcaimaisumavezvigitel[cited26.01.16]. 5.Warren CW, Jones NR, Eriksen MP, Asma S, Global Tobacco
Surveillance System (GTSS) collaborative group. Patterns of globaltobaccouseinyoungpeopleandimplicationsforchronic diseaseburdeninadults.Lancet.2006;367:749---53.
6.BarretoSM,GiattiL,Oliveira-CamposM,AndreazziMA,Malta DC.Experimentationanduse ofcigaretteandothertobacco products among adolescents in the Brazilian state capitals (PeNSE2012).RevBrasEpidemiol.2014;17:S62---76.
7.BorraciRA,MulassiAH. Tobaccouseduringadolescencemay predictsmokingduringadulthood:simulation-basedresearch. ArchArgentPediatr.2015;113:106---12.
8.SmalleySE,WittlerRR,OliversonRH.Adolescentassessmentof cardiovascularheartdiseasesriskfactorattitudesandhabits.J AdolescHealth.2004;35:374---9.
9.ThomasRE,McLellanJ,PereraR.Effectivenessofschool-based smoking preventioncurricular: systematic review and meta-analysis.BMJOpen.2015;5:e006976.
10.Vigescola --- Vigilância de tabagismo em escolares. Dados e fatosde 12capitaisbrasileiras. Rio de Janeiro:INCA;2004. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/ vigescolavol1.pdf[cited20.06.15].
11.FigueredoVC,SzkloAS,CostaLC,KuschnirMC,SilvaTL,Bloch KV,etal.ERICA:smokingprevalenceinBrazilianadolescentes. RevSaudePubl.2016;50:12.
12.IBGE-CIDADES. Available from: http://www.cidades.ibge.gov. br/xtras/home.php[cited16.08.16].
13.Californiastudenttobaccosurvey;2011---2012.Availablefrom: https://www.cdph.ca.gov/programs/tobacco/Documents/ CDPH%20CTCP%20Refresh/Research%20and%20Evaluation/ Survey%20Instrument/2011-12%20California%20Student% 20Tobacco%20Survey%20(CSTS)%20Questionnaire–CTCP.pdf [cited16.08.15].
14.GroveA, MartinM,EremencoS,McElroy S,Verjee-LorenzA, Erikson P, et al. Principles of good practice for the trans-lation and cultural adaptation process for Patient-Reported Outcomes (PRO) measures: report of the ISPOR Task Force forTranslationandCulturalAdaptation.ValueHeart. 2005;8: 94---104.
16.INCA.Asituac¸ão do tabagismono Brasil:dados dos inquéri-tos do Sistema Internacional de Vigilância, da Organizac¸¯ao MundialdaSaúde,realizadosnoBrasil,ente2002e2009.Rio deJaneiro:InstitutoNacionaldeCâncerJoséAlencarGomesda Silva(INCA);2011.Availablefrom:http://bvsms.saude.gov.br/ bvs/publicacoes/inca/PDFfinalsituacaotabagismo.pdf [cited 20.06.15].
17.CentroBrasileiro de Informac¸o˜essobre DrogasPsicotro´picas. V levantamento nacional sobre o consumo de drogas entre estudantesdoensinofundamentalemédiodaredepu´blicade ensinonas27capitaisbrasileiras;2004.Availablefrom:http:// www.cebrid.epm.br/levantamento brasil2/000-Iniciais.pdf [cited20.06.15].
18.DemirM,KaradenizG,DemirF,KaradenizC,KayaH,Yenibertiz D,etal.Theimpactofanti-smokinglawsonhighschoolstudents inAnkara,Turkey.JBrasPneumol.2015;41:523---9.
19.Brasil,PresidênciadaRepública.LeiFederaln.8.069de13de julhode1990.Dispõe sobreoEstatutodaCrianc¸a edo Ado-lescenteedáoutrasprovidências.Brasília:DiárioOficial(da) RepúblicaFederativadoBrasil;1990.Availablefrom:http:// www.planalto.gov.br/ccivil03/LEIS/L8069.htmSec.1:1.[cited 20.06.15].
20.SchaeferDR,HaasSA,BishopNJ.AdynamicmodelofUS ado-lescents’smokingandfriendshipnetworks.AmJPublicHealth. 2012;102:e12---8.
21.Bricker JB, Peterson AV Jr, Andersen MR, Rajan KB, Leroux BG,SarasonIG.Childhoodfriendswhosmoke: dothey influ-enceadolescentstomakesmokingtransitions?Addict Behav. 2006;31:889---900.
22.ScraggR,LaugesenM,RobinsonE.Parentalsmokingandrelated behaviorsinfluenceadolescenttobaccosmoking:resultsfrom the2001NewZealandnationalsurveyof4thformstudents.N ZMedJ.2003;116:U707.
23.INCA. Número de fumantes no Brasil cai 20,5% em cinco anos. Available from: http://www2.inca.gov.br/wps/wcm/ connect/agencianoticias/site/home/noticias/2014/numero defumantesnobrasilcai20porcentoemcincoanos [cited 20.06.15].
24.MorgensternM,SargentJD, EngelsRC,Scholte RH,FlorekE, HuntK,etal.Smokinginmoviesandadolescentsmoking initi-ation:longitudinalstudyinsixEuropeancountries.AmJPrev Med.2013;44:339---44.
25.WardKD.Thewaterpipe:anemergingglobalepidemicinneed ofaction.TobControl.2015;24:i1---2.
26.LeventhalAM,StrongDR,KirkpatrickMG,Unger JB,Sussman S,RiggsNR,etal.Associationofelectroniccigaretteusewith initiationofcombustibletobaccoproductsmokinginearly ado-lescence.JAmMedAssoc.2015;314:700---7.
27.InstitutoBrasileirodeGeografiaeEstatística.PesquisaNacional deSaúdedo Escolar(PeNSE):2012.Riode Janeiro:Instituto Brasileiro de Geografia e Estatística; 2013. Available from: http://www.ibge.gov.br/home/estatistica/populacao/pense/ 2012/[cited30.06.15].
28.LevyD,deAlmeidaLM,SzkloA.TheBrazilSimSmokepolicy sim-ulationmodel:theeffectofstrongtobaccocontrolpolicieson smokingprevalenceandsmoking-attributabledeathsinmiddle incomenation.PLoSMed.2012;9:e1001336.
29.GarciaP.CaminhosdoContrabando.Argentinaonovo corre-dor para o RS. Diario da Fronteira; 2015. Available from: www.facebook.com/diariodafronteira[cited21.06.15]. 30.Thomas RE,McLellan J,Perera R. School-basedprogrammes