www.jped.com.br
ORIGINAL
ARTICLE
Rapid
antigen
detection
test
for
respiratory
syncytial
virus
diagnosis
as
a
diagnostic
tool
夽
,
夽夽
Flávio
da
Silva
Mesquita
a,
Danielle
Bruna
Leal
de
Oliveira
a,∗,
Daniela
Crema
b,
Célia
Miranda
Nunes
Pinez
b,
Thaís
Cristina
Colmanetti
a,
Luciano
Matsumia
Thomazelli
a,
Alfredo
Elias
Gilio
c,
Sandra
Elisabeth
Vieira
c,
Marina
Baquerizo
Martinez
b,d,
Viviane
Fongaro
Botosso
e,
Edison
Luiz
Durigon
aaUniversidadedeSãoPaulo,InstitutodeCiênciasBiomédicas,DepartamentodeMicrobiologia,SãoPaulo,SP,Brazil bUniversidadedeSãoPaulo,HospitalUniversitário,LaboratórioClínico,SãoPaulo,SP,Brazil
cUniversidadedeSãoPaulo,HospitalUniversitário,DivisãodePediatria,SãoPaulo,SP,Brazil dUniversidadedeSãoPaulo,EscoladeCiênciasFarmacêuticas,SãoPaulo,SP,Brazil
eInstitutoButantan,LaboratóriodeVirologia,DivisãodeDesenvolvimentoCientífico,SãoPaulo,SP,Brazil
Received26October2015;accepted19June2016 Availableonline25November2016
KEYWORDS Respiratoryviruses; Respiratorysyncytial virus---RSV;
Rapidantigen detectiontest---RADT
Abstract
Objective: TheaimofthisstudywastoevaluatetheQuickVue®
RSVTestKit(QUIDELCorp,CA,
USA)asascreeningtoolforrespiratorysyncytialvirusinchildrenwithacuterespiratorydisease
incomparisonwith theindirect immunofluorescenceassayasgoldstandard.In Brazil,rapid
antigendetectiontestsforrespiratorysyncytialvirusarenotroutinelyutilizedasadiagnostic
tool,exceptforthediagnosisofdengueandinfluenza.
Methods: Theauthorsretrospectivelyanalyzed486nasopharyngealaspiratesamplesfrom
chil-drenunderage5withacuterespiratoryinfection,betweenDecember2013andAugust2014,
thesampleswereanalyzedbyindirectimmunofluorescenceassayandQuickVue®
RSVTestkit.
SampleswithdiscordantresultswereanalyzedbyrealtimePCRandnucleotidesequencing.
Results: From313positivesamplesbyimmunofluorescenceassays,282(90%)werealsopositive
bytherapidantigendetectiontest,twowerepositiveonlybyrapidantigendetectiontest,33
werepositiveonlybyimmunofluorescenceassays,and171werepositivebybothmethods.The
35sampleswithdiscordantresultswereanalyzedbyrealtimePCR;thetwosamplespositive
onlybyrapidantigendetectiontestandthefivepositiveonlybyimmunofluorescenceassays
werealsopositivebyrealtimePCR.TherewasnorelationbetweenthenegativitybyQuickVue®
夽
Pleasecitethisarticleas:MesquitaFS,OliveiraDB,CremaD,PinezCM,ColmanettiTC,ThomazelliLM,etal.Rapidantigendetection testforrespiratorysyncytialvirusdiagnosisasadiagnostictool.JPediatr(RioJ).2017;93:246---52.
夽夽
StudyconductedatUniversidadedeSãoPaulo,InstitutodeCiênciasBiomédicasII,DepartamentodeMicrobiologia,Laboratóriode VirologiaClínicaeMolecular,SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](D.B.Oliveira).
http://dx.doi.org/10.1016/j.jped.2016.06.013
0021-7557/©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND
RSVTestandviralloadorspecificstrain.TheQuickVue® RSVTestshowedsensitivityof90%,
specificityof98.8%,predictivepositivevalueof99.3%,andnegativepredictivevalueof94.6%,
withaccuracyof93.2%andagreementindexof0.85incomparisontoimmunofluorescence
assay.
Conclusions: ThisstudydemonstratedthattheQuickVue®
RSVTestKitcanbeeffectiveinearly
detectionofRespiratorysyncytialvirusinnasopharyngealaspirateandisreliableforuseasa
diagnostictoolinpediatrics.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
PALAVRAS-CHAVE VirosesRespiratórias; VirusSincicial Respiratório---VSR; TesteRápidode Detecc¸ãodeAntígeno ---TRDA
Testerápidodedetecc¸ãodeantígenosparaodiagnósticodoVírusSincicial Respiratóriocomoferramentadediagnóstico
Resumo
Objetivo: AvaliarotesteQuickVue®
RSVTestKit(QUIDELCorp,CA,EUA)paraodiagnóstico
rápidodovírussincicialrespiratórioemcrianc¸ascomdoenc¸arespiratóriaaguda,
comparando-ocomaimunofluorescênciaindiretacomopadrãoouro.Vistoque,noBrasil,testesrápidospara
detecc¸ãodeantígenosparavírussincicialrespiratórionãosãorotineiramenteutilizadoscomo
ferramentadediagnóstico,excetoparaDengueeInfluenza.
Métodos: Umtotalde486amostrasdeaspiradodenasofaringedecrianc¸asmenoresde5anos
comdoenc¸arespiratóriaaguda,coletadasentredezembrode2013eagostode2014,foram
anal-isadasporimunofluorescênciaepelotesteQuickVue®
.Amostrascomresultadosdiscordantes
entreosmétodosforamsubmetidasaPCRemtemporealesequenciamento.
Resultados: Das313 amostras positivas por IFI, 282foram positivas no teste rápido (90%),
2amostrasforampositivas apenas notesterápido(0.6%),33 apenas naimunofluorescência
(10.5%)e171foramnegativasemambososmétodos.As35amostrascomresultados
discor-dantesforamtestadasporPCRemtemporeal,sendoqueduasqueforampositivasapenasno
teste rápidoe5apenasnaimunofluorescênciaconfirmaram-se positivas.Nãohouverelac¸ão
entreaausênciadepositividadenotesteQuickVue®
comacargaoucomacepaviral.Oteste
QuickVue®mostrousensibilidadede90.1%,especificidade98.9%,valorpreditivopositivo99.3%,
valorpreditivonegativode94.6%,acuráciade93.2%eíndicedeconcordânciade0.85em
comparac¸ãoàimunofluorescência.
Conclusões: NossoestudodemonstrouqueotesteQuickVue® RSVpodeserefetivonadetecc¸ão
precoce dovírussincicialrespiratórioemamostrasdeaspiradodenasofaringeeéconfiável
comoumaferramentadediagnósticosempediatria.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo
OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Respiratory syncytial virus (RSV) is known as a major infectious agentof respiratorytractinfections inchildren worldwide.1 Mostchildrenareinfectedinthefirstyearof
life, but virtually all will be exposed by age 2.2
Reinfec-tionsarecommonthroughout life,depending onthelevel ofneutralizingantibodies intheserum, butcomplications in lowerrespiratory tract infections aremore commonin primaryinfection.3RSVisprimarilyreplicatedinsuperficial
portions of the respiratory tract, untilit spreads through the epithelium,forming asyncytia-like cytopathiceffect. RSVhastwoknownsub-groups:AandB,anditcancausea rangeofclinicalconditions,fromthecommoncoldto bron-chiolitis and pneumonia, which are caused by necrosisof the bronchi and bronchioles. The World Health Organiza-tion(WHO)estimatesthatRSVinfects64millionpeopleand causes160,000deathsperyearworldwide.4Theseasonality
ofthevirusvaries,anditisoftendetectedthroughoutthe year.However,itisknownthatthehighestincidenceoccurs inthewinterseason.
TheviraldiagnosisofRSVcanbeaccomplishedbya num-berofmethods,including:cellculture,immunofluorescence assays (IFA), immune chromatographic assays (rapid anti-gendetectiontests:RADTs),andpolymerasechainreaction (PCR),includingconventionalandreal-timePCRassays.In the last decade, the molecular methods have been used asthegoldstandard,becauseoftheirspecificityand abil-ity to simultaneously detect different viruses.5 In Brazil,
although there are at least four RADTs available for RSV detection (BD-DirectigenTMEZ-RSV [Becton, Dickinson and
Company®,NJ,USA];SASTMRSValert[Medivax®,RJ,Brazil]; AlereTMBinaxNow®
immunodeficiencyvirus(HIV)anddenguetests,6,7whichare
widelyused.
Therapidtest tobeevaluatedinthisstudy(QuickVue® RSVTestKit,Quidel®)providesaresultin15min,compared to approximately 90min for a conventional IFA test and 2---3hforenzyme(ELISA).8Quicklyidentifyingtheetiologic
agentofrespiratorydiseases, suchasbronchitisand bron-chiolitis, isan important steptoward reducing theuse of antimicrobials,especiallyinhospitalizedchildren,9andcan
alsoindicatethemostappropriatemethodofisolationand treatment.
TheQuickVue® RSVtestisadipstickimmunoassay,which allows for the rapid, qualitative detection of RSV anti-gen (viral fusion protein) directly from nasopharyngeal swab, nasopharyngeal aspirate, or nasal/nasopharyngeal washspecimensfromsymptomaticpediatric patients.The testisintendedfor useasanaidinthediagnosisof acute respiratorysyncytialviralinfections.
Theaimofthisstudyistoevaluatesensitivity,specificity, andimportanceoftheQuickVue® RSVTestKitasaRADTfor screeningandimprovementofRSVdiagnosisinthe nasopha-ryngealaspirateofchildrenwithacuterespiratorydisease comparedwithindirectIFA,foruseinhospitalsandpediatric clinicalpractices.
Materials
and
methods
Theauthorsretrospectivelyanalyzednasopharyngeal aspi-rate(NPA)samplesfrom486children---274boys(56.4%)and 212girls (43.6%)--- underfiveyears oldwithsymptomsof acuterespiratoryinfection(ARI),includingupperandlower respiratorytractdisease,intheperiodbetweenDecember 2013 and August 2014, who had ARI and were cared for inthe emergencyroom,asoutpatients,or hospitalizedin thePediatrics Department,University Hospital, University ofSãoPaulo(HU-USP).
ClinicalsampleswerecollectedduringtheRSVoutbreak of2014usingmucustrap.Immediatelyfollowingcollection, thesamplesweresenttotheUniversityofSãoPauloHospital LaboratoryandscreenedbyindirectIFAusingacommercial KitLightDiagnosticsTMRespiratoryPanelViralScreeningand Identification (IFA Chemicon®, Merk Millipore Corp., USA) following the manufacturer’s instructions. These samples werethensenttotheClinicalandMolecularVirology Labora-toryattheInstituteofBiomedicalSciencesoftheUniversity of SãoPaulo, where they werefrozen by cryogenics,and storedat−80◦Cuntilthetimeoftesting.Allthesamples
were registered at the Virology Laboratory Biorepository, andallethics guidelinesforhuman experimentationwere strictlyobservedandapprovedbytheEthicsCommitteeon ResearchwithHumanBeingsattheUniversityofSãoPaulo (USP).
Based on the IFA results, 486 NPA samples distributed duringallthemonths oftheseasonwere selected, corre-spondingto50.4% ofallthe samplesanalyzed.Theywere classifiedintothreedistinct groupsasshown in Fig.1.To reduceoreliminateanybias,theQuickVue® RSVassaywas performed andanalyzed ina blind trial,and resultswere comparedwiththeoriginalresultsfromtheIFAKit.
Inordertoconfirmtheresults,sampleswithdiscrepant resultsweresubsequentlytestedbyreal-timequantitative
NPA samples 486
RSV positive 313
RSV negative 100
RSV-/Other virus+
73
Figure 1 Work flowchart. Nasopharyngeal aspirate samples
were dividedinto threedistinctgroupsscreenedby
immuno-fluorescenceassayandcomparedwithrapidantigendetection
test for respiratory syncytial virus.RSV, respiratory syncytial
virus;NPA,nasopharyngealaspirate;+,positive;−,negative.
reverse transcription PCR (F proteinregion) andby tradi-tionalPCR(GandFproteinregions).
Samples were extracted on the NUCLISENS® easyMag® platform (bioMérieux®, MA, USA) and real-time PCR per-formedonABI7300instrumentationutilizingtheAgPath-ID One-StepRT-PCRmastermixkit(Ambion®,TX,USA) follow-ingthemanufacturer’sinstructions.
For traditional PCR, the authors used a reaction mix-turecontaining10LofcDNA,5LofPCRbufferreaction 10×concentration(50mMTris---HCl[pH9.0],1.0LofMgCl2 (50mM KCl, 20mM [NH4)2SO4]), 2.5mM of each dNTPs, 10pmolofeachprimerforRSV(Table1),0.6UofTaqDNA Polymerase(platinumtaqDNApolymerase,Invitrogen,CA, USA)andwater,resultinginafinalvolumeof50L.
Ampli-fication of protein Gand F wasperformed in a GeneAmp PCRSystem9700(AppliedBiosystems,Inc.,CA,EUA) ther-mocycleraccordingtothefollowingprogram:95◦Cforfive
min,followed by40cyclesof95◦Cfor30s,54◦Cfor30s,
72◦Cfor90s,andonelastsevenmincycleat72◦C.
Approxi-mately1894bpproductsofGgene10---12and1685bpproducts
of F gene13 were purifiedwith a commercial kit (Exosap,
GE®Tech,CA,USA),accordingtothemanufacturer’s instruc-tions. Sequence reactions of the G gene10---13 and the F
gene13,14 weresubjectedtoelectrophoreticseparationfor
primarydatacollectionin a3130DNA sequencer(Applied Biosystems,Inc.,CA,EUA),usingafluorescentdye termina-torkit(AppliedBiosystems,Inc.).Sequencesobtainedwere edited with the Sequence Navigator program version 1.0 (Applied Biosystems, Inc.,CA, EUA)andaligned usingthe programMegalign(Lacergene,DNASTAR,Inc.,WI,USA).A maximumlikelihoodphylogenyofGproteinwasestimated usingMEGA615,16withgammadistribution(TN93+G)forthe
RSVAdatasetandmodelwithgammadistribution(HKY+G) forHRSVB.17 Thephylogenetictreethatresultedwas
mid-pointrooted.
Table1 Primersusedfortraditionalpolymerasechain reaction(PCR)andsequencingofGandFrespiratorysyncytialvirus
(RSV)proteins.
Primername Targetprotein Genomeposition Reaction Sequence5′-3′ Reference
FV-aAB G 186---163/GeneF PCR GTTATGACACTGGTATACCAACC Zhengetal.10
SH+AB G 3924---3948/GeneM PCR CAGCTACACGTTTTTCAATCAAACC Limaetal.11
OG1+21a G 1---21/GeneG SANGER GGGGCAAATGCAACCATGTCC Trentoetal.12
GAB+a,b G/F 504---524/GeneG PCR YCAYTTTGAAGTGTTCAACTT Peretetal.13
BO2---ABb F 1216---1199/GeneF PCR ATCTGTTTTTGAAGTCAT ArbizaJ.c
F1AB+b F 3---22/GeneF SANGER GGTTGGTATACCAGTGTCATAAC Modif.Peretetal.14
FP2+ ABb F 573---595/GeneF SANGER TTAACCAGCAAAGTGTTAGACC InHouse
G,glycoprotein;F,fusionprotein;M,matrixprotein. a PrimerusedinGgenesequencing.
b PrimerusedinFgenesequencing.
c CourtesyofDr.JuanArbiza,LaboratoryofVirology,FacultyofSciences,UniversityoftheRepublic,Montevideo,Uruguay.
diagnosticlikelihood ratios (DLRs).18,19 IFA wasconsidered
asthe gold standard for these analyses. Samples positive by IFA were considered tobe true positives, and samples thatwerenegativebyIFAwereconsideredtobetrue neg-atives.Foraccurateevaluationoftheagreementbetween themethods,thekappaindex()wasalsoassessed.
Results
RADT
Ofthe313 NPAsamplespositive forRSV byIFA,282 (90%) werealsopositivebythe rapidtest(QuickVue® RSVtest), thus the RADTtest revealed 31 falsenegativeresults. All the100NPAsamplesnegativeforRSVbyIFAwerealso neg-ativebytherapidtest(100%).Of73NPAsamplesthatwere negativeforRSVbutpositiveforotherrespiratoryvirus(AdV orPIV1,2,3orFluAandFluB)byIFA,71(97.26%)were confirmedbytherapidtest,andtwo(2.74%)haddivergent results,revealingtwofalsepositiveresults(Table2A).
Discrepantresultstestedbyreal-timePCR
The 33 samples with discordant results between the two methodswereanalyzedbyreal-timePCR(Table2B).
Twenty-sixNPAsamplesthatwerepreviouslyconsidered positiveby IFAand negativebyrapidtest wereconfirmed aspositiveforRSVbyreal-timePCR.ThetwoNPAsamples considered negative by IFA andpositive by the rapid test wereactually positiveby qPCR.Andthe fiveNPAsamples considered positive by IFA and negativeby the rapid test werenegativebyqPCR.Thereal-timePCRthresholdcycle (Ct)valuesofthe26positivesamplesrangedfrom14to37 cycles.
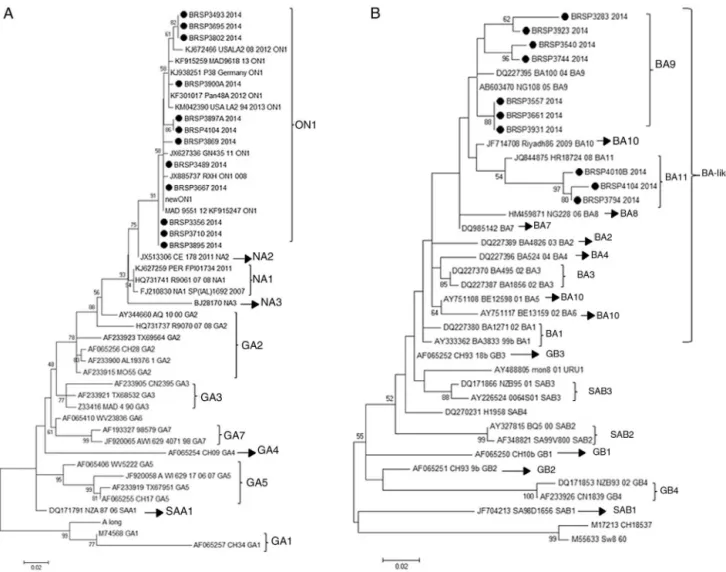
In order tounderstand if the differencesbetween the testswererelatedtoaspecific genotype(RSVAorRSVB) or a genetic variability in the F protein of the virus, the G protein of all 26 samples with divergent results were sequencedandtherewere22consensusesforfurther anal-ysis. Aftersequencing, theresults showed thatall the 12 RSVAsequenceswerefromthenovelgenotypeON1andall tenRSVBsequenceswerefromthenewBA11(three) and BA9(seven)genotypes(Fig.2).
Table 2 Results ofrespiratory syncytial virus(RSV)
pos-itive and negative by indirect immunofluorescence assay
(IFA) and rapid antigen detection test (RADT) and the
totality of divergent samples tested in this study. (A)
Rapid-antigendetectiontestresultscomparedwithIFA.(B)
Discrepant results. (C) Comparison of rapid test
evalua-tionparametersincludingsensitivity,specificity,predictive
positive value (PPV), negative predictive value (NPV),
andpositive/negativediagnosticlikelihoodratio(DLR),for
QuickVue®
RSV test compared to IFA, used as the gold
standard.
RADT(test) Numberofsamples
IFA(goldstandard) Total
Positive Negative
Positive 282 2 284
Negative 31 171 202
Total 313 173 486
Results Numberofsamples
IFA+,RADT−,qPCR+ 26
IFA−,RADT+,qPCR+ 2
IFA+,RADT−,qPCR− 5
IFA−,RADT+,qPCR− 0
Parameter 95%CI
Sensitivity(%) 90.1(86.8---93.4%)
Specificity(%) 98.8(97.2---100)
PPV(%) 99.3(98.3---100%)
NPV(%) 94.6(79.6---89.6)
PositiveDLR 77.9(19.6---309.26)
NegativeDLR 0.1(0.071---0.14)
Figure2 Humanrespiratorysyncytialvirus(HRSV)maximumlikelihoodphylogenetictreebasedonnucleotidesequencesofthe
Gproteinofthediscrepantsamplesfromthiswork,indicatedasBRSP,andworldwidedistributedstrainsobtainedfromGenBank.
GenBankaccessionnumbers aregiven ineach taxonfollowed by thecorrespondent nameofthe strain.Initial tree(s) for the
heuristicsearch wereobtained byapplyingthe neighbor-joiningmethod toamatrix ofpairwise distancesestimated usingthe
maximumcompositelikelihood(MCL)approach.Thetreesweredrawntoscale,withbranchlengthsmeasuredinthenumberof
substitutionspersite.Numbersattheinternalnodesrepresentthebootstrapprobabilities(5000replicates).Onlybootstrapvalues
>50areshown.(A)HRSVA.TheevolutionaryhistorywasinferredbyusingthemaximumlikelihoodmethodbasedontheTamura---Nei
model.15,16 Thetreewiththehighestloglikelihood(
−1303.6711)isshown.(B)HRSVB.Theevolutionaryhistorywasinferredby
usingthemaximum likelihoodmethod basedontheHasegawa---Kishino---Yano model.17 The treewiththehighest loglikelihood
(−1207.4096)isshown.TheanalyseswereconductedinMEGA6.15
Statisticalanalysis
TheperformanceoftheQuickVue®RSVtestcomparedtoIFA arerepresentedinTable2.Theaccuracywas93.2%(95%CI: 91.0---95.4%)andtheagreementindexbetweenthe
meth-odswas0.85 (95% CI:0.945---0.769), which wasranked as almostperfect,20withp<0.001.
The analysis of the discordant and concordant results between the methodologies showed no significance (p=0.62,p=0.065inthechi-squaredtest,respectively).
Discussion
The aim of this study wastoprove that the rapid test is efficientforRSVdetectionandtoencourageitsuseinBrazil, asitiscurrentlydonefordengue,influenza,andHIV.
ThehallmarkofRSV infectionisbronchiolitis,21 andits
diagnosisisgenerallymadebyclinicalcondition.22Although
notrecommended,theprescriptionofantibioticsfor bron-chiolitis is an extremely common practice in hospitalized children,9,23 andtheiruseisassociatedwithanincreasein
the cost and time of hospitalization24 and an increase of
therisk ofdevelopmentof resistantbacterial strains.25 In
severecases,especiallyinintensivecareunits,antibiotics are commonly used to avoid a potential bacterial infec-tion, although the risk in healthy infants is uncommon.26
A systematic review that analyzed four studies involving childrenattendingtheemergencyroomsuggestedthat diag-nostictestscouldreduce theprescription ofantibiotics,24
of antibiotics.27 If the diagnostic test is positive, it can
contribute to prevent the use of antibiotics. In doubtful cases that are not severe, the patient should stay under observation.
Sincetheresultusingarapidtest isavailablein15min anditisperformedbythedoctorwithouttheneedof lab-oratory equipment,the rapid test would be usedfor this screening,asapointofcareassay.
In this context, the authors’ work showed that the QuickVue® RSVTestisreliableforthistask,ascanbeseen by the results of the performance in comparisonto indi-rectimmunofluorescenceassay(IFA)usedasgoldstandard inthisstudy.Alltheparametersanalyzedwerehigh(greater than 90% --- sensitivity of 90%, specificity of 98.8%, PPV of 99.3%, and NPV of 94.6%) and were similar to those ofother studies thatcomparedRADTwithIFA asthegold standard,whichrangedfrom73%to93%sensitivityand84% to100%specificity.28 Incontrast,in2015Leonardi etal.29
evaluated four RSV direct antigen detection assays and theirresultspresentedonly57.5%sensitivityforQuickVue®, although this difference may be due to the comparison withRT-qPCR,whichhasahighersensitivityandspecificity thanIFA.
In addition, the overall agreement (kappa index) and accuracy between the two tests were considered good, andthenegativeandpositivepercentagreement(173/202 and 284/313 respectively) showed no significant differ-ence(p>0.05). Only33 samplesshowed divergent results betweenthetests;theywereanalyzedbyRT-qPCRinorder toconfirmtheresultsandtocorrelatethesensitivityofthe testwithalowviralload,asitwasobservedbyTuttleetal.30
Twenty-sixsamplescontinuetobeunsolvedafterthis anal-ysis,andtheauthorsalsocouldnotexplainthedifferences by the load viral, sincethe qPCR threshold cycle ranged from 14 to 37. Maybe these false negative results could berelatedtothestorageoffrozen specimensbeforetheir analysis.
Next, inorder tounderstand ifthesedifferences were relatedtoaspecificgenotype(RSVAorRSVB)oragenetic variabilityintheFproteinofthevirus,theGandFgenes were sequenced. The G sequences analysis showed that theybelongedtogenotypesON1andBA-likeinsertion (vari-antsBA11and BA9). However,other samples inthisstudy that showed positive results by QuickVue® RSV Test were sequenced (data not shown) and belonged to the same genotypes, proving that the negativity is not related to thesegenotypes.This studydidnot identifyanymutation intheFgenethatcouldberesponsiblefortheresults.The final approachwastolookfor inhibition caused by chem-icalelementsin thesamplesasan inhibition,nonetheless falsenegativespecimenswerediluted(1:5and1:10),but remainednegative.
Inconclusion,theQuickVue® RSVTestKitdisplayedhigh predictivevaluesandlikelihoodratios,anditprovedtobe effectiveinearlydetectionofRSV.Nevertheless,depending onthepatient’simprovement,itisrecommendedthatthe testmustberepeatedincaseofnegativity.Therefore,this studydemonstratedthattheQuickVue® RSVTestKitcanbe effectiveinearlydetectionofRSVinfrozennasopharyngeal aspiratespecimens and is suitablefor use asa diagnostic toolinpediatrics.
Funding
UniversidadedeSãoPaulo(USP).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
The authors would like tothank QUIDEL Corp.for donat-ingtherapidantigendetectiontestskits,essentialforthe developmentof this work, Gustavo Rezende Melo for the statisticalanalysis,andMr.José MariaLopesfor technical support.
References
1.Domachowske JB, Rosenberg HF. Respiratory syncytial virus infection:immuneresponse,immunopathogenesis,and treat-ment.ClinMicrobiolRev.1999;12:298---309.
2.MohapatraSS,BoyapalleS.Epidemiologic,experimental,and clinicallinksbetweenrespiratorysyncytialvirusinfectionand asthma.ClinMicrobiolRev.2008;21:495---504.
3.GlezenWP,TaberLH,FrankAL,KaselJA.Riskofprimary infec-tionandreinfectionwithrespiratorysyncytialvirus.AmJDis Child.1986;140:543---6.
4.Openshaw PJ. Potential therapeutic implications of new insights into respiratory syncytial virus disease. Respir Res. 2002;3:S15---20.
5.PecchiniR,BerezinEN,FelícioMC,PassosSD,SouzaMC,Lima LR,etal.Incidenceandclinicalcharacteristicsoftheinfection bytherespiratorysyncytialvirusinchildrenadmittedinSanta CasadeSãoPauloHospital.BrazJInfectDis.2008;12:476---9.
6.FerreiraJuniorOC,FerreiraC,RiedelM,WidolinMR, Barbosa-JúniorA,HIVRapidTestStudyGroup.Evaluationofrapidtests foranti-HIVdetectioninBrazil.AIDS.2005;19:S70---5.
7.LimaMdaR,NogueiraRM,SchatzmayrHG,dosSantosFB. Com-parison ofthree commerciallyavailable dengue NS1antigen captureassaysforacutediagnosisofdengueinBrazil.PLoSNegl TropDis.2010;4:e738.
8.RayCG,MinnichLL.Efficiencyofimmunofluorescenceforrapid detection of common respiratory viruses. J Clin Microbiol. 1987;25:355---7.
9.American Academy of PediatricsSubcommittee on Diagnosis and ManagementofBronchiolitis.Diagnosisand management ofbronchiolitis.Pediatrics.2006;118:1774---93.
10.Zheng H, PeretTC, RandolphVB, Crowley JC, Anderson LJ. Strain-specificreversetranscriptasePCRassay:meansto dis-tinguishcandidatevaccinefromwild-typestrainsofrespiratory syncytialvirus.JClinMicrobiol.1996;34:334---7.
11.LimaHN,BotossoVF,OliveiraDB,Campos AC,Leal AL,Silva TS,etal.MolecularepidemiologyoftheSH(small hydropho-bic)geneofhumanrespiratorysyncytialvirus(HRSV),over2 consecutiveyears.VirusRes.2012;163:82---6.
12.TrentoA,ÁbregoL,Rodriguez-FernandezR,González-Sánchez MI,González-MartínezF,DelfraroA, etal.Conservationof g-proteinepitopesinrespiratorysyncytialvirus(groupA)despite broadgeneticdiversity:isantibodyselectioninvolvedinvirus evolution?JVirol.2015;89:7776---85.
14.PeretTC,HallCB,SchnabelKC,GolubJA,AndersonLJ. Circu-lationpatternsofgeneticallydistinctgroupAandBstrainsof humanrespiratorysyncytialvirusinacommunity.JGenVirol. 1998;79:2221---9.
15.TamuraK,StecherG,PetersonD,FilipskiA,KumarS.MEGA6: molecularevolutionarygeneticsanalysisversion6.0.MolBiol Evol.2013;30:2725---9.
16.NeiM,KumarS.Molecularevolutionandphylogenetics.New York,USA:OxfordUniversityPress;2000.
17.HasegawaM,KishinoH,YanoT.Datingofthehuman-ape split-tingbya molecular clockofmitochondrial DNA. JMol Evol. 1985;22:160---74.
18.MacKinnon DP, Krull JL, Lockwood CM. Equivalence of the mediation, confounding and suppression effect. Prev Sci. 2000;1:173---81.
19.AltmanDG,BlandJM.Quartiles,quintiles,centiles,andother quantiles.BMJ.1994;309:996.
20.LandisJR,KochGG.Themeasurementofobserveragreement forcategoricaldata.Biometrics.1977;33:159---74.
21.ShayDK,HolmanRC,NewmanRD,LiuLL,StoutJW,Anderson LJ.Bronchiolitis-associatedhospitalizationsamongUSchildren, 1980---1996.JAMA.1999;282:1440---6.
22.ZorcJJ,HallCB.Bronchiolitis:recentevidenceondiagnosisand management.Pediatrics.2010;125:342---9.
23.ChristakisDA,CowanCA,GarrisonMM,MolteniR,MarcuseE, ZerrDM.Variationininpatientdiagnostictestingand manage-mentofbronchiolitis.Pediatrics.2005;115:878---84.
24.DoanQ,EnarsonP,KissoonN,KlassenTP,JohnsonDW.Rapid viraldiagnosisfor acutefebrilerespiratoryillnessinchildren in theEmergency Department. Cochrane Database Syst Rev. 2012;5:CD006452.
25.Wang EE, Einarson TR, Kellner JD, Conly JM. Antibiotic prescribingforCanadianpreschoolchildren:evidenceof over-prescribing for viral respiratory infections. Clin Infect Dis. 1999;29:155---60.
26.RandolphAG,RederL,EnglundJA.Riskofbacterialinfection inpreviouslyhealthyrespiratorysyncytialvirus-infectedyoung childrenadmittedtotheintensivecareunit.PediatrInfectDis J.2004;23:990---4.
27.FerronatoÂE,GilioAE,FerraroAA,PaulisMD,VieiraSE. Etio-logicaldiagnosisreducestheuseofantibioticsininfantswith bronchiolitis.Clinics(SaoPaulo).2012;67:1001---6.
28.ChartrandC,TremblayN,RenaudC,PapenburgJ.Diagnostic accuracyofrapidantigendetectiontestsforrespiratory syncy-tialvirusinfection:systematicreviewandmeta-analysis.JClin Microbiol.2015;53:3738---49.
29.LeonardiGP,WilsonAM,DauzM,ZurettiAR.Evaluationof respi-ratorysyncytialvirus(RSV)directantigendetectionassaysfor useinpoint-of-caretesting.JVirolMethods.2015;213:131---4.