SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Total
bilateral
ruptures
of
the
knee
extensor
apparatus
夽
Diogo
Lino
Moura
a,∗,
José
Pedro
Marques
b,
João
Páscoa
Pinheiro
c,
Fernando
Fonseca
aaCoimbraUniversityHospital,OrthopedicsDepartment,Coimbra,Portugal bCoimbraUniversityHospital,SportsMedicineDepartment,Coimbra,Portugal
cCoimbraUniversityHospital,PhysicalRehabilitationMedicineDepartment,Coimbra,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13September2016 Accepted3November2016 Availableonline30December2016
Keywords:
Kneejoint Tendoninjuries
Patellarligament/injuries Rupture
a
b
s
t
r
a
c
t
Objective:Bilateralextensortendonrupturesofthekneearerareandhaveonlybeen pub-lishedintheformofcasereportsorsmallseries.
Methods:Sevenpatientscorrespondingto14extensortendonrupturesofthekneewere evaluatedbythesameexaminerafteraminimumoneyearpost-surgery.Clinicaland radio-graphicevaluationswereperformed;forstatisticalanalysis,thelevelofsignificancewasset at0.05.
Results:Themostcommoninjurywaspatellartendonrupture(n=9;64.29%)followedby quadricepstendonrupture(n=5,35.71%).Theintrasubstancewasthemostaffectedlocation (57.15%),followedbythemyotendinousjunction(21.43%)andthepatellarboneinsertions (21.43%).Quadricepstendonrupturesweremoreprevalentinpatientsolderthan50years, whilepatellartendonrupturestendedtooccurinyoungerindividuals.Allbutonepatient hadrecognizedriskfactorsfortendinousdegenerationandrupture:75%ofthecases suf-feredfromdiseases,50%hadhistoryofdruguseand/orabuse,and37.5%hadbothdisease anddrugusehistory.MeanattainedvaluesforflexionROMwere124.64◦±9.43(110–140◦)
and89.57±6.02(78–94)forKujalascore.Morethanhalfofthepatientscomplainedof resid-ualpainandquadricepsmuscularweakness.Meanagewasyoungerintheindividualswho complainedofresidualpain.
Conclusion: Bilateraltendonrupturesofthekneeextensorapparatusrupturesarerareand seriousinjuries,mostlyassociatedwithriskfactors.Earlysurgical repairandintensive rehabilitationprogramforbilateralextensortendonrupturesofthekneemaywarrant sat-isfactoryfunctionaloutcomesinthemediumtolongterm,despitenon-negligiblelevelsof residualpain,quadricepsmuscleweakness,andatrophy.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheCoimbraUniversityHospital,Coimbra,Portugal.
∗ Correspondingauthor.
E-mail:[email protected](D.L.Moura). http://dx.doi.org/10.1016/j.rboe.2016.11.009
Ruptura
bilateral
total
do
aparelho
extensor
do
joelho
Palavras-chave:
Articulac¸ãodojoelho Lesõesdotendão Ligamentopatelar/lesões Ruptura
r
e
s
u
m
o
Objetivo:Asrupturasbilateraisdotendãoextensordojoelhosãorarasesóforampublicadas naformaderelatosdecasosoudepequenasséries.
Métodos: Setepacientes(14rupturasdotendãoextensordojoelho)foramavaliadospelo mesmoexaminadorapósumperíodomínimodeumanodepós-operatório.Foram real-izadasavaliac¸õesclínicaseradiográficas.Paraaanáliseestatística,oníveldesignificância foifixadoem0,05.
Resultados: Alesãomaiscomumfoirupturadotendãopatelar(n=9;64,29%)seguidade rupturadotendãodoquadríceps(n=5,35,71%).Aintrasubstânciafoialocalizac¸ãomais acometida(57,15%),seguidapelajunc¸ãomiotendinosa(21,43%)einserc¸ãoósseapatelar (21,43%).Asrupturasdotendãodoquadrícepsforammaisprevalentesempacientescom maisde50anos;poroutrolado,asrupturasdotendãopatelartenderamaocorrerem indiví-duosmaisjovens.Àexcec¸ãodeumpaciente,todososdemaisapresentavamreconhecidos fatoresderiscoparadegenerac¸ãoerupturatendínea:75%doscasossofriamdedoenc¸as, 50%tinhamhistóricodeusoe/ouabusodedrogase37,5%apresentavamsimultaneamente históricodedoenc¸aeusodedrogas.OsvaloresmédiosobtidosparaaADMdeflexãoforam de124,6◦±9,43(110-140◦);noescoredeKujala,osvaloresmédiosforam89,57±6,02(78-94).
Maisdametadedospacientessequeixoudedorresidualefraquezamuscularnoquadríceps. Aidademédiadosindivíduosquesequeixaramdedorresidualeramenor.
Conclusão: Asrupturasbilateraisdotendãonasrupturasdoaparelhoextensordojoelho sãolesõesrarasegravese namaioriadoscasosestão associadasafatoresderisco.O reparocirúrgicoprecoceeainstaurac¸ãodeumprogramadereabilitac¸ãointensivapara rupturasbilateraisdotendãoextensordojoelhopodemlevarresultadosfuncionais sat-isfatóriosamédioelongoprazo,apesardosníveisnãonegligenciáveisdedor residual, fraquezamuscularnoquadrícepseatrofia.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The knee extensor apparatus encompasses two tendons, quadricepsandpatelar,andthepatellarbone.Unilateral rup-turesarequitecommon,asopposedtotherarebilateralknee extensorruptures.Thisishighlightedbythefactthatthelatter haveonlybeenpublishedintheformofcasereportsorsmall series.Bilateralkneetendonextensorapparatusrupturesare seriousanddisablinginjuries,mostlyassociatedwithrisk fac-tors.Theyarefrequentlyreportedasdifficulttotreatinjuries, demandinglong recoveryperiods.1–10 Thispaperreportson ourcentre’sexperiencetreatingpatientswithbilateralknee tendonextensor ruptures andrepresents thelargest series publishedtodate.Theaimofthisstudy istoprovide infor-mationregardingprognosisonvarious clinicaloutcomesof thesepatients,increasingourunderstandingofthe natural historyofthis rare clinicalpresentation. Alsowehope our resultsmayhelpcliniciansidentifyingpatientsatrisk,leading totheintroductionofpreventivemeasures.
Methods
Medicalrecordswereretrospectivelyreviewedand7patients were identified and included in our study. They had all been previouslysubmitted tosurgery dueto totalbilateral knee tendon extensor rupture (time between surgery and
clinical evaluation – average: 5.29 years; range 1–8 years). All patients were summoned and evaluated by the same examiner after aminimum of1-year post-surgery. Clinical examination included range of motion (ROM) assessment andtheapplicationofKujalascore.11Additionallya satisfac-tion index(scale0–5:0–insatisfiedto5–totally satisfied), thepresenceofresidualsymptomsanditscharacterization were assessed. Radiographicevaluation aimedatdetecting thepresenceofpatellofemoralarthritisusingMerchant patel-lar view and measuring patellar height with Insall–Salvati ratio.12,13ForstatisticalanalysisweusedSPSS(version23,IBM Corp,Armonk,NewYork)withthelevelofsignificancesetat 0.05.Quantitativemeasuresarepresentedasmean±standard deviation (SD; minimumvalue–maximum value) and qual-itative measures with total number (n) or percent (%).We usedMann–Whitneytestforcomparingquantitativeand Chi-square test for qualitative data. To study the association betweenquantitativeoutcomesweusedSpearman correla-tiontest.
Results
Demographicandinjurycharacterizationdata
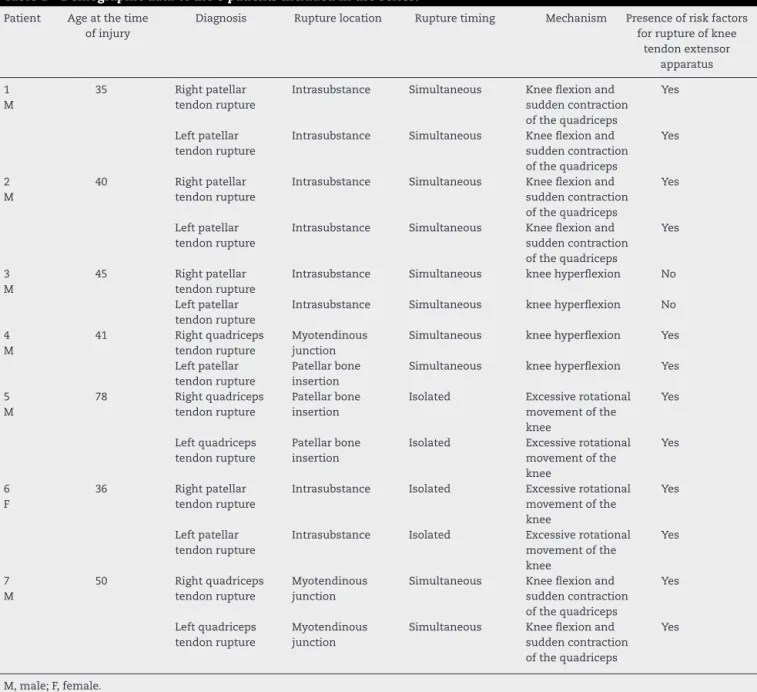
Table1–Demographicdataofthe8patientsincludedintheseries.
Patient Ageatthetime ofinjury
Diagnosis Rupturelocation Rupturetiming Mechanism Presenceofriskfactors forruptureofknee
tendonextensor apparatus
1 M
35 Rightpatellar tendonrupture
Intrasubstance Simultaneous Kneeflexionand suddencontraction ofthequadriceps
Yes
Leftpatellar tendonrupture
Intrasubstance Simultaneous Kneeflexionand suddencontraction ofthequadriceps
Yes
2 M
40 Rightpatellar tendonrupture
Intrasubstance Simultaneous Kneeflexionand suddencontraction ofthequadriceps
Yes
Leftpatellar tendonrupture
Intrasubstance Simultaneous Kneeflexionand suddencontraction ofthequadriceps
Yes
3 M
45 Rightpatellar tendonrupture
Intrasubstance Simultaneous kneehyperflexion No
Leftpatellar tendonrupture
Intrasubstance Simultaneous kneehyperflexion No
4 M
41 Rightquadriceps tendonrupture
Myotendinous junction
Simultaneous kneehyperflexion Yes
Leftpatellar tendonrupture
Patellarbone insertion
Simultaneous kneehyperflexion Yes
5 M
78 Rightquadriceps tendonrupture
Patellarbone insertion
Isolated Excessiverotational movementofthe knee Yes Leftquadriceps tendonrupture Patellarbone insertion
Isolated Excessiverotational movementofthe knee
Yes
6 F
36 Rightpatellar tendonrupture
Intrasubstance Isolated Excessiverotational movementofthe knee
Yes
Leftpatellar tendonrupture
Intrasubstance Isolated Excessiverotational movementofthe knee
Yes
7 M
50 Rightquadriceps tendonrupture
Myotendinous junction
Simultaneous Kneeflexionand suddencontraction ofthequadriceps
Yes
Leftquadriceps tendonrupture
Myotendinous junction
Simultaneous Kneeflexionand suddencontraction ofthequadriceps
Yes
M,male;F,female.
(35–78y)and85.71%weremale.Themostcommoninjurywas patellartendonrupture(n=9;64.29%),followedbyquadriceps tendonrupture(n=5;35.71%)(Fig.1).Withthesoleexception ofanindividualwithrightpatellartendonandleftquadriceps
9 ([VALUE]) 5 ([VALUE]) 0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00%
Patellar tendon ruptures Quadricipital tendon ruptures
Level of rupture at knee extensor apparatus
Fig.1–Levelofruptureatkneeextensorapparatus.
42.86% 28.57%
28.57% 28.57% 14.29%
14.29% 14.29% 14.29%
Reported risk factors
Fig.2–Reportedriskfactorsofacaseseriesofbilateral rupturesofthekneetendonextensorapparatus.
profileevaluationrevealedthat85.71%ofthesamplesuffered fromdiseasesthatarerecognizedriskfactorsfortendinous degeneration and rupture, 57.14% had history of drug use and/orabuse,42.86%hadbothdiseaseanddrugusehistory. Therewasonly1healthypatientwithoutknownriskfactors. Corticotheraphy (42.86%) and anabolic steroid use (28.57%) were the main recognized consumptions. Chronic kidney injuryundergoing haemodialysis(28.57%), hypercholestero-laemia(28.57%),hyperuricemia(14.29%),rheumatoidarthritis (14.29%),systemiclupuserythematosus(14.29%)and osteo-genesisimperfecta(14.29%)weretheidentifiedpredisposing diseases(Fig.2).Allquadricepstendonrupturesoccurredin patientswithknowndisease.Ontheotherhand,patellar ten-donrupturesweremorecloselyrelatedtodruguse(66.7%of druguseand/orabuseversusonly40%inquadricepstendon ruptures).
Treatmentperformed
Meanwaitingtimeforsurgerywas51.3hours(5–120h). Surgi-calrepairwasthetreatmentofchoiceinallpatients(Table2).
Employed techniques were end-to-end suture (50%), tran-sosseoussuture(28.57%)andtenodesiswithsutureanchors (21.43%). Cerclage protection wire was used in 3 patellar tendon ruptures with7.3 months being the mean time to removal. Meanimmobilizationtime post-surgerywas48.43 days(42–70),followedbyrehabilitationprogramunder physio-therapistsupport,whichincludedinitiallyisometricmuscle strengtheningandprogressivekneeflexionandstrengthening exercises.
Outcomes
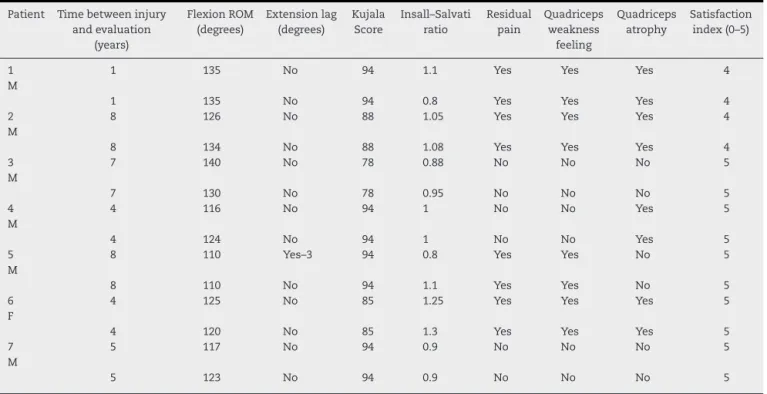
Mean attained values for flexion ROM (Table 3) were 124.64◦±9.43 (110–140◦) and 89.57±6.02 (78–94) in Kujala score.FullextensionROMwasobservedinallexceptoneofthe knees,whiletheremainingdisplayeda5◦deficitorless. Con-cerningthesatisfactionindex28.57%chosegrade4and71.43% grade5.Signsofpatellofemoralarthritiswerenotidentified inthissample,andtherewere2kneeswithpatellabajain thesamepatientwithpatellartendonruptures(Insall–Salvati ratio=1.25and 1.3).Age demonstratedasignificant inverse correlationwithkneeflexionROM(rho=−0.60;p=0.022).
Whencomparingquadricepswithpatellartendonruptures wenoticedlowerflexionROM(116◦±5.5vs129.4◦±6.8)and superior Kujalascores (94±0vs87.1±6.3) inpatients who sufferedfromquadricepstendonruptures,althoughthe dif-ferenceswerenon-significant.Rupturesattheintrasubstance level were associated with lower Kujala score (86.3±6,2;
p=0.039) when compared with ruptures at the myotendi-nousjunction(94±0) orattheboneinsertionlevel(94±0). However,theypresentedasignificantlysuperiorflexionROM (130.6◦±6.2;p=0.006)whencomparedwithrupturesatthe myotendinousjunction(113.3◦±5.8).Thosewhohadno pre-disposing diseaseattainedsuperior flexionROM(135◦±4.1;
p=0.002)comparedwiththeoneswhodid(115.4◦±13.4).We
Table2–Specificitiesofthetreatmentperformedtoeachofthe8patientsincludedintheseries.
Patient Surgicalrepair Cerclage protectionwire
Immobilization time(days)
Timebetweeninjury andsurgery(hours)
1 M
End-to-endsuture Yes 45 5
End-to-endsuture Yes 45 5
2 M
End-to-endsuture No 42 72
End-to-endsuture No 42 72
3 M
End-to-endsuture Yes 56 96
End-to-endsuture Yes 56 96
4 M
End-to-endsuture No 42 120
Tenodesiswithsutureanchors Yes 42 120
5 M
Tenodesiswithsutureanchors No 70 120
Tenodesiswithsutureanchors No 70 120
6 F
End-to-endsuture No 42 96
End-to-endsuture No 42 96
7 M
End-to-endsuture No 42 6
Table3–Outcomesofeachofthe7patientsincludedintheseries.
Patient Timebetweeninjury andevaluation
(years)
FlexionROM (degrees)
Extensionlag (degrees)
Kujala Score
Insall–Salvati ratio
Residual pain
Quadriceps weakness
feeling
Quadriceps atrophy
Satisfaction index(0–5)
1 M
1 135 No 94 1.1 Yes Yes Yes 4
1 135 No 94 0.8 Yes Yes Yes 4
2 M
8 126 No 88 1.05 Yes Yes Yes 4
8 134 No 88 1.08 Yes Yes Yes 4
3 M
7 140 No 78 0.88 No No No 5
7 130 No 78 0.95 No No No 5
4 M
4 116 No 94 1 No No Yes 5
4 124 No 94 1 No No Yes 5
5 M
8 110 Yes–3 94 0.8 Yes Yes No 5
8 110 No 94 1.1 Yes Yes No 5
6 F
4 125 No 85 1.25 Yes Yes Yes 5
4 120 No 85 1.3 Yes Yes Yes 5
7 M
5 117 No 94 0.9 No No No 5
5 123 No 94 0.9 No No No 5
foundnodifferencesinthefunctionalresultsachievedwith different surgical techniques and different immobilization periods.
Complications
Morethanhalfofthepatients(57.14%)complainedof resid-ualpainandquadricepsweakness,symptomselicitedmainly
bylong periodsofstanding or walking,climbing and
des-cendingstairsandsquatting.Nonethelessallpatientsdenied
important functional impairment in daily activities. The
prevalenceofresidualpainwasfoundtobesuperiorin patel-lartendonruptures (66.7%), rupturesatthe intrasubstance (75%)andmyotendinousjunction(66.6%)levels,althoughnot reachingstatisticalsignificantdifferences.Meanagewas sig-nificantlyinferior (47.3±19.1 vs54.5±17.3;p=0.038)inthe individualswhocomplainedofresidualpain.Thighatrophy
auto-perception was claimed in 8 ruptures, corresponding
to 7 patellar tendon ruptures and 1 quadriceps tendon
rupture.
Discussion
Ittakes a strength that is 17.5 times superior to our own bodyweight tocauserupture ofahealthy patellartendon. Howeverthemajorityoftherupturesfollowminortraumaor happenspontaneously.14,15KannusandJozsa16reportedtheir findings on 891 patients withspontaneous tendinous rup-tureemphasizingthatallofthemhaddegenerativechanges on histopathological examination. Accordingly, most knee extensor apparatus ruptures follow an inflammatory and degenerativeprocesswherebytendon’smechanicalproperties becomeseverelyimpaired.Thisoccursinsystemicdiseases
(rheumatologic diseases, diabetes, chronic kidney injury, hyperparathyroidism, gout, obesity), local diseases (patel-lar tendinopathy) and drug use (corticotheraphy, anabolic steroids).1,2,10,14,17–21 Ourseriesdemonstratesastrong asso-ciationbetweentendinousrupturesandpersonalhistoryof diseaseand/ordrugconsumption,findingsthatareconsistent withtheliterature.3–6
Most injuries were due to falls. As reported by other authors, knee flexion coinciding with sudden contrac-tion of the quadriceps was the most common injury mechanism.17,21–23Higherprevalenceofrupturesatthe intra-substance tendon level have been reported previously and attributedtoitstendencytodegenerationundertheinfluence ofdiseasestatesordruguse.Instead,healthytendonstendto tear atmyotendinousjunctionorboneinsertionlevel.9,20,23 Quadriceps tendon ruptures are more frequentin patients older than 50years whilepatellartendonruptures tendto occur inyoungerindividuals.Ourfindingsare corroborated byotherresearchers.1,2,14,21,24
Early diagnosis and surgical repair are needed to re-establishkneeextensormechanism.Tendonrepair,followed by immobilization and rehabilitation have shown good outcomes.1,2,19Cerclageprotectionwireuseinthiscontextis controversial.1,9,14,23,24Althoughitallowsearlymobilizationit alsorequiresasecondsurgeryforremoval.
tendonruptures.Provelegiosetal.4 publishedtheresultsof aseriesof5patientwithspontaneousbilateral quadriceps ruptures.AllsufferedfromCKIandhyperparathyroidismand hadexcellentfunctionaloutcomes.
Siweketal.25statedthatkneeextensormechanism rup-tures must be repaired as soon as possible in order to maximize functional outcomes.Theyclaimthat adelay of morethantwoweekscanseriouslycompromiseprimary ten-donrepairduetoretraction.Inourserieswecouldnotfind differencesin functionaloutcomes attributabletodifferent waitingtimesforsurgery.Despitetheabsence ofahealthy contralateraltendontocompare,weonlyhad14.29%of patel-larheightabnormalvaluesinthe14operatedknees,assuming Insall–Salvati13rationormalvaluesbetween0.8and1.2.
A significant percentage of our patients complained of residual pain and quadriceps weakness. The comparison between patellar and quadriceps tendon ruptures showed thatpatellartendonrupturesaremorecommoninyounger patients, tend to occur at the intrasubstance level, have superior residual pain and flexion ROM. Pain and quadri-cepsweaknessandatrophyweremorecommoninyounger patientswithpatellartendonrupture. Noteworthythis isa subsetpatientswhohavehigherphysicaldemandsand supe-riorauto-perceptionofpainandfunctionalimpairment(when comparedwiththeiroldercounterparts).Quadricepstendon ruptures are more frequent in older patients, which may explainwhytheyhavelowerflexionROMbuthigherKujala scores(possiblyduetolowerresidualpain).
Presentstudylimitationsincludeitsretrospectivedesign, thesmallsizeofthesampleandasubjectiveclinicaland func-tionalevaluation.
Conclusions
Bilateralknee extensortendonapparatus rupturesare rare andseriousinjuries,mostlyassociatedwithriskfactors. Nev-ertheless,weandotherauthorshavedemonstratedthatan earlysurgicalrepairandintensiverehabilitationprogrammay warrantsatisfactory functionaloutcomesonmediumterm, despitenon-negligiblelevelsofresidualpain,quadriceps mus-cleweaknessandatrophy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
WethankDr.MargaridaMarques,DepartmentofStatistics, CoimbraHospitalandUniversityCenterforthesupportgiven tothisarticle.
r
e
f
e
r
e
n
c
e
s
1. KellersmannR,BlattertTR,WeckbachA.Bilateralpatellar tendonrupturewithoutpredisposingsystemicdiseaseor
steroiduse:acasereportandreviewoftheliterature.Arch OrthopTraumaSurg.2005;125(2):127–33.
2.MorettiB,NotarnicolaA,MorettiL,GarofaloR,PatellaV. Spontaneousbilateralpatellartendonrupture:acasereport andreviewoftheliterature.ChirOrganiMov.2008;91(1): 51–5.
3.ChangES,DodsonCC,TjoumakarisF,CohenSB.Functional resultsfollowingsurgicalrepairofsimultaneousbilateral quadricepstendonruptures.PhysSportsmed.
2014;42(2):114–8.
4.ProvelegiosS,MarkakisP,CambouroglouG,ChoumisG, DounisE.Bilateral,spontaneousandsimultaneousruptureof thequadricepstendoninchronicrenalfailureandsecondary hyperparathyroidism.Reportoffivecases.ArchAnatCytol Pathol.1991;39(5–6):228–32.
5.GoldsteinZH,YiPH,HaughomBD,HellmanMD,LevineBR. Bilateralextensormechanismdisruptionaftertotalknee arthroplastyintwomorbidlyobesepatients.Orthopedics. 2015;38(5):e443–6.
6.SengC,LimYJ,PangHN.Spontaneousdisruptionofthe bilateralkneeextensormechanism:areportoftwocases.J OrthopSurg(HongKong).2015;23(2):262–6.
7.FormigaF,MogaI,PacM,ValverdeJ,FiterJ,PalomX. Spontaneoustendinousruptureinsystemiclupus erythematosus.Presentationof2cases.RevClinEsp. 1993;192(4):175–7.
8.LauermanWC,SmithBG,KenmorePI.Spontaneousbilateral ruptureoftheextensormechanismofthekneeintwo patientsonchronicambulatoryperitonealdialysis. Orthopedics.1987;10(4):589–91.
9.GiblinP,SmallA,NicholR.Bilateralruptureofthe ligamentumpatellae:twocasereportsandareviewofthe literature.AustNZJSurg.1982;52(2):145–8.
10.VanGlabbeekF,DeGroofE,BoghemansJ.Bilateralpatellar tendonrupture:casereportandliteraturereview.JTrauma. 1992;33(5):790–2.
11.KujalaUM,JaakkolaLH,KoskinenSK,TaimelaS,HurmeM, NelimarkkaO.Scoringofpatellofemoraldisorders. Arthroscopy.1993;9(2):159–63.
12.MerchantAC,MercerRL,JacobsenRH,CoolCR.
Roentgenographicanalysisofpatellofemoralcongruence.J BoneJointSurgAm.1974;56(7):1391–6.
13.InsallJ,SalvatiE.Patellapositioninthenormalkneejoint. Radiology.1971;101(1):101–4.
14.KuoRS,SonnabendDH.Simultaneousruptureofthepatellar tendonsbilaterally:casereportandreviewoftheliterature.J Trauma.1993;34(3):458–60.
15.ZernickeRF,GarhammerJ,JobeFW.Humanpatellartendon rupture:akineticanalysis.JBoneJointSurgAm.
1977;59(2):179–83.
16.KannusP,JozsaL.Histopathologicalchangespreceding spontaneousruptureofatendon.Acontrolledstudyof891 patients.JBoneJointSurgAm.1991;73(10):1507–25. 17.MaffulliN,WongJ.RupturesoftheAchillesandpatellar
tendons.ClinSportsMed.2003;22(4):761–76.
18.McMasterP.Tendonandmusclerupture.Clinicaland experimentalstudiesonthecausesandlocationsof subcutaneousruptures.JBoneJointSurg.1933;15:705. 19.AlpantakiK,PapadokostakisG,KatonisP,HadjpavlouA.
Spontaneousandsimultaneousbilateralruptureofthe quadricepstendon.Acasereport.ActaOrthopBelg. 2004;70(1):76–9.
20.KellyD,CarterV,JobeF,KerlanR.Patellarandquadriceps tendonruptures–jumper’sknee.AmJSportsMed. 1984;12(5):375–80.
22.SochartDH,ShravatBP.Bilateralpatellartendon disruption—aprofessionalpredisposition?JAccidEmerg Med.1994;11(4):255–6.
23.HoHM,LeeWK.Traumaticbilateralconcurrentpatellar tendonrupture:analternativefixationmethod.KneeSurg SportsTraumatolArthrosc.2003;11(2):105–11.
24.WebbLX,TobyEB.Bilateralruptureofthepatellatendonin anotherwisehealthymalepatientfollowingminortrauma.J Trauma.1986;26(11):1045–8.