www.jped.com.br
ORIGINAL
ARTICLE
Breastfeeding
duration
and
associated
factors
between
1960
and
2000
夽
,
夽夽
Danielle
Soares
de
Oliveira
a,
Cristiano
S.
Boccolini
b,
Eduardo
Faerstein
a,
Eliseu
Verly-Jr
a,∗aUniversidadedoEstadodoRiodeJaneiro(UERJ),InstitutodeMedicinaSocial(IMS),RiodeJaneiro,RJ,Brazil bFundac¸ãoOswaldoCruz(Fiocruz),RiodeJaneiro,RJ,Brazil
Received14December2015;accepted25May2016 Availableonline21July2016
KEYWORDS
Breastfeeding; Survivalanalysis; Childhealth; Timeseries
Abstract
Objective: Todescribeahistoricalseriesonthemediandurationofbreastfeedingina popula-tionofmotherswhosechildrenwerebornfromthe1960sonwards,identifyingfactorsassociated withtheinterruptionofbreastfeedingineachdecade.
Methods: DatawereanalyzedfromthePró-SaúdeStudy,alongitudinalepidemiological inves-tigationstartedin1999amongtechnicalandadministrativeemployeesofauniversityinthe stateofRiode Janeiro.Breastfeedingduration wascollected intwo study phases:Phase1 (1999),andphase4(2011---2012).Ofthese,thosewhohadatleastonechildandreportedthe durationofbreastfeedingforthefirstchildwereselected(n=1539).Toanalyzethedurationof breastfeeding,survivalcurveswereconstructedusingtheKaplan---Meiermethodandtheeffect ofcovariatesonthedurationofbreastfeedingwasestimatedbyCoxregressionmodel. Results: Itwasfoundthatthemediandurationofbreastfeedingwashigherinthe1990sand 2000sandlowerinthe1970s, comparedtothe1960s.Inaddition,therewasanassociation betweenhigherincomeandmaternalagewithbreastfeedinginterruption,whichwasfocused inthe1970s.
Conclusion: Therewasshorterdurationofbreastfeedinginthe1970scomparedtothe1960s. Increaseddurationandprevalenceofbreastfeedingfromthe1970sonwardscoincidedwiththe nationaltrendandthepromotionofthispracticesince1980.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
夽
Pleasecitethisarticleas:OliveiraDS,BoccoliniCS,FaersteinE,Verly-JrE.Breastfeedingdurationandassociatedfactorsbetween1960 and2000.JPediatr(RioJ).2017;93:130---5.
夽夽
StudyconductedatUniversidadedoEstadodoRiodeJaneiro(UERJ),RiodeJaneiro,RJ,Brazil. ∗Correspondingauthor.
E-mail:[email protected](E.Verly-Jr).
http://dx.doi.org/10.1016/j.jped.2016.05.005
PALAVRAS-CHAVE
Aleitamentomaterno; Análisedesobrevida; Saúdedacrianc¸a; Sériestemporais
Durac¸ãodoaleitamentomaternoefatoresassociadosentre1960e2000
Resumo
Objetivo: Descrever uma série histórica sobre a durac¸ão mediana da amamentac¸ão em populac¸ão demãescomcrianc¸asnascidasapartir dadécadade1960, identificandofatores associadosàsuainterrupc¸ãoemcadadécada.
Métodos: Foram analisados dados de 1539 participantes do Estudo Pró-Saúde (EPS), uma investigac¸ão epidemiológica longitudinal iniciada em 1999 entre trabalhadores técnico-administrativosdeumauniversidadelocalizadanoEstadodoRiodeJaneiro.Foramutilizadas informac¸õessobredurac¸ãodoaleitamentomaternodoprimeirofilhocoletadasemduasfasesdo EPS(1999e2011-12).Paraanálisedadurac¸ãodoaleitamentomaternoforamconstruídascurvas desobrevidapelométododeKaplan---Meier,esuaassociac¸ãocomcovariáveisfoiestimadapelo modeloderegressãodeCox.
Resultados: Verificou-sequeadurac¸ãomedianadoaleitamentomaternofoimaiornasdécadas de1990e2000,emenornadécadade1970,emcomparac¸ãocomadécadade1960.Alémdisso, houveassociac¸ãoentremaiorrendaefaixaetáriamaternascominterrupc¸ãodoaleitamento materno,queseconcentrounadécadade1970.
Conclusão: Observou-semenordurac¸ãodoaleitamentomaternonadécadade1970emrelac¸ão àdécadade1960.Oaumentodadurac¸ãoedasprevalênciasdeamamentac¸ãoapartirdadécada de1970coincidiucomatendêncianacionalecomapromoc¸ãodessapráticaapartirde1980. ©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Breastfeedingisconsideredoneofthestrategiesthatmost contributestothepreventionofchilddeath,withthe poten-tialtosavemorethan800,000childrenunder5yearsofage per year worldwide1,2 and to reduce neonatal mortality,3
which is recommended as an exclusive practice until 6 monthsofageandasasupplementupto2yearsofageor older.4Inspiteofitsrelevance,socialandeconomic
circum-stancesmayhave aprofound influence ontheprevalence anddurationofbreastfeeding.5,6
In the mid-1960s, massive marketing campaigns were started to encourage the substitution of breastmilk with infant formula without any kind of regulation, reaching mothersfromallsocialstrata,which,togetherwithcultural changesregardingtheroleofbreastfeedinginsociety and theincreasingintegrationofwomenintothelabormarket, ledtothedeclineofbreastfeedingduration.6---9Inresponse
to that, global pro-breastfeeding movements, especially fromtheend ofthe 1970sonwards,ledtothecreation a setofstandardsbasedonethicalprinciplestoregulatethe commercialpromotionofproductsthatcouldinterferewith maternalbreastfeeding.10,11
Since the beginning of the 1980s, several laws, stan-dards, and programs have been adopted by the Ministry of Health in Brazil to promote and support breastfeed-ing, which are considered responsible for the consistent increaseintheprevalenceandmediandurationof breast-feedingsincetheendofthatdecade,5,6,9,10asdemonstrated
bynationalsurveys,12,13withsuchincrementsbeing
associ-atedwithreducedmorbidityandreductioninhospitalization rates.14,15
However,ahistoricalseriesisnotavailablewithregard tothemediandurationofbreastfeedingpriortothe1980s,
as the only national survey carried out in the period (1974---1975)obtained onlyindirect informationabout this practice.16Toclarifywhethermaternalbreastfeeding
dura-tioninBrazilshowedanupward,steady,ordownwardtrend beforethe1980s,itisessentialtoemploythedataobtained fromotherstudiesthatarecomparabletothosefrom sub-sequent periods. This study aimsto describe a historical seriesonbreastfeedingdurationinchildrenborn fromthe 1960sonwards and toidentify factors associated with its interruptionineachdecade.
Methods
Studypopulation
Data from the Pro-Saúde Study (PSS), a longitudinal epi-demiologicalinvestigationstartedin1999withapopulation oftechnical andadministrative employees ofa university in the state of Rio de Janeiro, were analyzed. The main objective of the PSS is to elucidate the role of social determinantsofhealth;between1999and2013,fourdata collectionstepswerecarriedout,includingself-completion ofquestionnaires,anthropometricmeasurements,andother tests.
study.WomenwhoparticipatedinthePhase1andPhase4 wereconsideredonlyonce.Detailsofrecruitmentandthe populationstudiedcanbefoundinanotherpublication.17
The present studyuseddataonbreastfeedingduration relatedtothefirstchild,collectedintwophasesofthePSS: Phase1(1999),andphase4(2011---2012).ThePSSincluded 2160womeninitstwophases,ofwhom1727hadatleastone child.Forthisstudy,onlythosewhowereabletoreportthe breastfeedingduration for thefirst childwere considered (n=1539).
Datacollection
Data collection was performed with the aid of field researchers,usingamultidimensional,self-completed ques-tionnaire administered at the work environment. A pilot study, tool reliability testing, and independent double entry18 were performed to ensure the quality of data.
Breastfeeding duration was obtained in months, through specific questions asked to women who had at least one child,includingthemonthandyearofbirth,thepractice(or not)ofbreastfeeding,andinwhichmonthbreastfeedinghad beeninterrupted,allrelatedthefirstbornchild.Thedates ofbirthwerecategorizedintodecadesfrom1960onwards. The per capita monthly family income was obtained throughtheconversionofthehouseholdnetincomedivided bythetotalnumberofpeoplewhodependedonthisincome, and was categorized into per capita income tertiles. As incomedatarelatedtotwodifferentperiodswereused,the incomereportedinphase1wasadjustedforinflationusing theNationalIndexofConsumerPrices(ÍndicedePrec¸osao Consumidor Amplo [IPCA]), tomaximize itscomparability withStage4.Dataonself-reportedrace/ethnicitywere col-lectedaccordingtothecategoriesoftheBrazilianInstitute ofGeographyandStatistics(InstitutoBrasileirodeGeografia eEstatística[IBGE]):African-descendant,mixed-race, Cau-casian,Asian,andIndigenous.Maternalagewasrelatedto the time they had their first child. Additionally, mothers were questioned about the type of delivery (cesarean or vaginal).
Dataanalysis
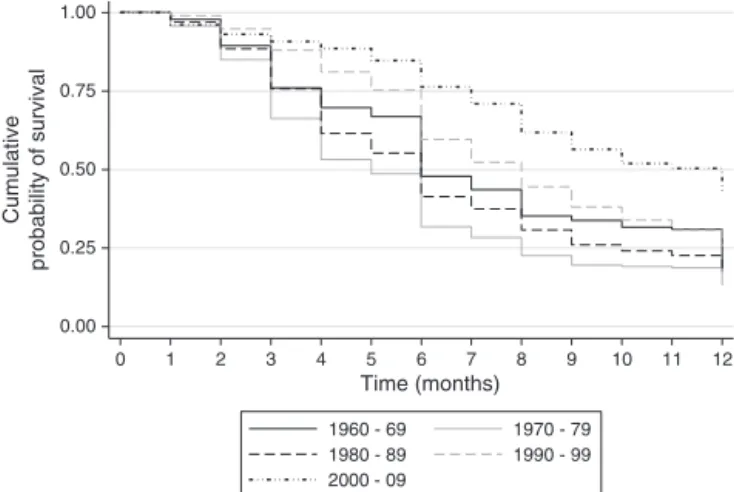
Toanalyzebreastfeedingduration,survivalcurveswere con-structedusingtheKaplan---Meiermethodforeachreported decade,representingthecumulativeprobabilityof breast-feedingover thecourseof months.Timeofbreastfeeding wascensoredat12monthsandtheassociationofcovariates withbreastfeeding durationwasestimatedby Cox regres-sion.
It wasdecidednot toinclude theindividuals classified as Asian and Indigenous regarding skin color/ethnicity in the analysis because of their low frequencies (1.7% and 0.7%,respectively).Theassumptionofproportionalhazards requiredfor Cox regression wastested(including interac-tionsofcovariateswithtime)andbySchoenfeldresiduals (1982);ofthe decadeof birthasan independentvariable wasalsoconducted.Thetestedstatisticalsignificancelevel was5%,andthesoftwareStata(StataCorp.2011.Stata Sta-tisticalSoftware:Release12.CollegeStation,USA)wasused fortheanalysis.
Table1 Tertiles ofmothers’age (inyears) accordingto decade ofbirthof their child. Pró-Saúdestudy, 1999and 2011---2012.
Decade 1sttertile 2ndtertile 3rdtertile
1960---1969 12---19 19---21 22---33 1970---1979 14---20 21---24 24---40 1980---1989 13---24 24---28 28---40 1990---1999 19---28 28---32 32---51 2000---2009 22---32 33---36 37---44
Phase 1 of the PSS was approved in 1999 by the ResearchEthicsCommittee(REC)ofHospital Universitário PedroErnesto(registrationNo.224/1999)andphase4was approvedin2011bytheRECofInstitutodeMedicinaSocial daUERJ(CAAENo.0041.0.259.000-11).
Results
Table 1shows the age in tertilesin each decade studied. This classificationwaschosenbecausethe mothers’mean ageincreasedaccordingtothefirstchild’sdecadeofbirth.
Table2showsthemediandurationofbreastfeedingand the hazardratio(HR),which expressesthe riskof discon-tinuingbreastfeeding ineach decade, takingthe1960sas areference.Anincreasedrisk ofinterruptioninthe1970s (HR=1.36;p<0.001)andalowerriskinthe2000s(HR=0.52;
p<0.001)wereobserved.Survivalcurvesforbreastfeeding areshowninFig.1,whichemphasizesthelowerprobability ofamothertoremainbreastfeedingoverthefirst12months of her child’slife in the 1970s,and a greater increase in breastfeedingdurationinthe2000---2009period.
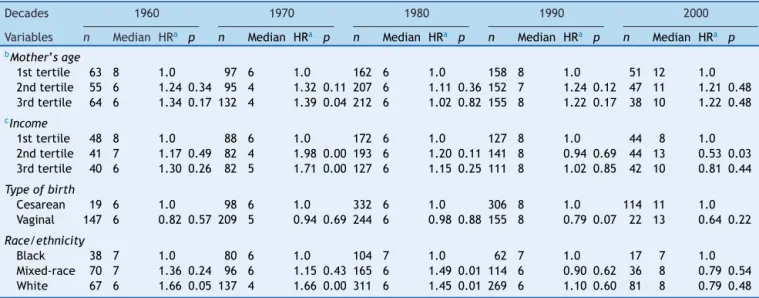
Table3shows theCoxmodelestimates forassociations betweencovariatesandtimeofbreastfeedingforeach stud-ied decade. Statistically significant associations with the mother’s income and age are concentrated in the 1970s. Olderwomen(3rdtertile)showeda39%higherriskof breast-feeding interruptionwhen comparedtoyoungerones (1st tertile). Regarding household income, participants in the secondandthirdtertiles(higherpercapitaincome)showed
0.00 0.25 0.50 0.75 1.00
Cumulative
probability of survival
0 1 2 3 4 5 6 7 8 9 10 11 12
Time (months)
1970 - 79 1960 - 69
1990 - 99 1980 - 89
2000 - 09
Table2 Distributionofwomenwhobreastfed,medianduration,andriskofbreastfeedinginterruptioninthefirstyearoflife perdecadeofbirthofthefirstchild.Pró-Saúdestudy,1999and2011---2012.
Decade na Breastfeeding(n,%)b Medianc p25---p75 HRd
1960---1969 182 168(92%) 6 4---12 1.00
1970---1979 324 292(90%) 5 3---8 1.36(1.08---1.69)
1980---1989 592 549(92%) 6 4---10 1.11(0.90---1.36)
1990---1999 465 431(92%) 8 6---13 0.80(0.65---1.00)
2000---2009 136 131(96%) 12 7---19 0.52(0.39---0.70)
a Totalofwomenthathadtheirfirstchild,perdecade.
b Frequencyandpercentageofwomenwhoreportedhavingbreastfed,perdecade. c Medianbreastfeedingduration,inmonths.
d Hazardratio.Thedecadeofthe1960sisthereferencecategory.
ahigherriskofbreastfeedinginterruptioninthe1970s;in the 2000s, an inverse association wasobserved, in which womenfromthesecondtertileofincomeshowedlowerrisk. Womenwhoself-declaredtheirethnicityasAfrican descen-dantshadalowerrisk ofbreastfeedinginterruption when comparedtoCaucasiansinthe1960sand1970s,aswellas whencomparedtoCaucasiansandmixed-racewomeninthe 1980s.Thetypeofdeliverywasnotassociatedwiththerisk ofbreastfeedinginterruption.
Discussion
Thepresentstudyinvestigatedtheevolutionof breastfeed-ing duration between 1960 and 2009, observing an initial decline in duration in the 1970s when compared to the 1960s,andasubsequentincreaseinthefollowingdecades. Thelowest riskofinterruptionwasobservedintheperiod of 2000---2009. The evolution of duration observed here cannot be compared directly to that observed in other studiesassessingbreastfeedingdurationovertheyearsdue
tothe methods usedfor the analysis, but follows similar patterns.5,6,9,10
The National Survey on Child Mortality and Family Planning(PesquisaNacionaldeMortalidadeInfantile Plane-jamentoFamiliar[PNMIPF])19andtheNationalDemographic
andHealthSurvey(PesquisaNacionaldeDemografiaeSaúde [PNDS])12 showed, respectively, a median breastfeeding
durationof9months(1986)and14months(2006),a simi-larevolutiontothatobservedintheNationalBreastfeeding Prevalence Survey (Pesquisa Nacional de Prevalência do AleitamentoMaterno[PPMA]),13conductedintheBrazilian
capitalcitiesin1999(9.8months)and2008(11.3months). InSãoPaulo,ahospital-basedstudywithinformationrelated totheyears1954---1985showedthatthemedian breastfeed-ingdurationwasapproximately150daysinthe1960sand 100daysinthe1970s,withsubsequentincreasetoover100 daysinthenextdecade.6
Theshortestbreastfeedingdurationwasobservedinthe 1970swhencomparedtothepreviousdecade,whichmaybe associatedwith distinct and complex sociocultural deter-minants,suchastheincreasingparticipationof womenin
Table3 Breastfeedingmediandurationandriskofinterruptioninthefirstyearperdecadeofbirthofthefirstchild.Pró-Saúde study,1999and2011---2012.
Decades 1960 1970 1980 1990 2000
Variables n Median HRa p n Median HRa p n Median HRa p n Median HRa p n Median HRa p bMother’sage
1sttertile 63 8 1.0 97 6 1.0 162 6 1.0 158 8 1.0 51 12 1.0 2ndtertile 55 6 1.24 0.34 95 4 1.32 0.11 207 6 1.11 0.36 152 7 1.24 0.12 47 11 1.21 0.48 3rdtertile 64 6 1.34 0.17 132 4 1.39 0.04 212 6 1.02 0.82 155 8 1.22 0.17 38 10 1.22 0.48 cIncome
1sttertile 48 8 1.0 88 6 1.0 172 6 1.0 127 8 1.0 44 8 1.0 2ndtertile 41 7 1.17 0.49 82 4 1.98 0.00 193 6 1.20 0.11 141 8 0.94 0.69 44 13 0.53 0.03 3rdtertile 40 6 1.30 0.26 82 5 1.71 0.00 127 6 1.15 0.25 111 8 1.02 0.85 42 10 0.81 0.44 Typeofbirth
Cesarean 19 6 1.0 98 6 1.0 332 6 1.0 306 8 1.0 114 11 1.0 Vaginal 147 6 0.82 0.57 209 5 0.94 0.69 244 6 0.98 0.88 155 8 0.79 0.07 22 13 0.64 0.22 Race/ethnicity
Black 38 7 1.0 80 6 1.0 104 7 1.0 62 7 1.0 17 7 1.0 Mixed-race 70 7 1.36 0.24 96 6 1.15 0.43 165 6 1.49 0.01 114 6 0.90 0.62 36 8 0.79 0.54 White 67 6 1.66 0.05 137 4 1.66 0.00 311 6 1.45 0.01 269 6 1.10 0.60 81 8 0.79 0.48
a Hazardratio.
b Tertilesofthemother’sage(asshowninTable1).
thelabor marketand the changesin paradigmsregarding thenatureofbreastfeeding,8constructsthataredifficultto
measurewiththeavailabledatafromthestudies.However, itisaconsensusamongtheauthorswhohavestudiedthis periodthatthisdeclinecoincideswiththepeakofmarketing andcommercializationpracticesthatoccurredwithout reg-ulationbythefoodindustryinBrazilandworldwideduring thisperiod,aswellasthecooptationofhealth profession-alswhoencouragedtheuseofinfantformula,theso-called ‘‘breastmilksubstitute.’’7---9,13,20 It is noteworthy that the
declineinbreastfeedingdurationinthedevelopedcountries hadoccurredapreviousperiod(1930s),withbreastfeeding practicealsobeingre-establishedafterthe1970s.21
In the international context, breastfeeding prevalence anddurationislowerindevelopedcountries,andyet,the prevalenceofexclusivebreastfeedingis37%indeveloping countries,withlargedisparitiesbetweenthepoorerandthe richermothers.1Inthisunfavorablescenariofor
breastfeed-ing,Rolinsetal.carriedoutacasestudypublishedinthe LancetBreastfeedingSeries,whichconcludesthatBrazilis oneofthesuccess storiesin improvingbreastfeeding pat-terns due to the involvement of civil society, as well as thegovernment’sstrongsupportandinvestmentregarding the adoption of practices such as the international code monitoring, implementation of paid maternity leave, the creationofahumanmilkbanknetwork,andchild-friendly hospitals.22
When analyzing the factors associated with the risk of breastfeeding interruption, maternal income and age were highlighted. Older mothers showed greater risk of breastfeedinginterruptionwhencomparedtoyoungerones. Similarly,mothersinthehigherincomestratumhadahigher riskofbreastfeedinginterruptionwhencomparedto lower-incomeones, a pattern similar tothat found in different groups and countriesfrom all regions: when analyzing 98 studiescarried outin developing countries,Victora etal. found that, regardless of the country and region of the world,mothers belonging to the poorest strata breastfed forlongerperiodsthanthosefromthericheststrata.1
Inter-estingly,thesedifferenceswereconcentratedinthe1970s, thesameperiodwhen shorterbreastfeeding durationwas observed.Thehigherincomefavoredweaningbyallowing thepurchaseofartificialformula,14 inacontextof
impor-tantinfluencebytheindustryanddeconstructionofnatural breastfeedingbenefits.20However,therewasanoteworthy
reversalintheassociationbetweenincomeand breastfeed-ing interruption observed in the 2000s, in which mothers withthehighestincomehadlowerriskofweaning(although it was statistically significant only for the intermediate stratum). This change can be understood as a reflection of the change in the mothers’ perception regarding the importance of breastfeeding, the resultof the efforts of pro-breastfeedingmovements,andthelegislationthat reg-ulatedtheadvertisingofartificialformula.9,14
Infact,nationalsurveydata(1975/1989)14 hadalready
signaledthistrend.Theassociationbetweenbreastfeeding durationandincomeshowedtobeinverselyassociatedin 1975, being four-fold higher in children of lower income whencomparedtothoseofhigherincome.In1989,this dif-ferencedecreasedtolessthantwo-foldandwasnolonger an inversely linear association, considering all income strata. Moreover, this phenomenon was also identified in
66countriesstudiedsincethe1990s,inwhichwomenfrom the poorest quintiles breastfed longer than women from therichestquintiles.22
Regarding skin color/ethnicity, the present study dis-closed shorter median breastfeeding duration among CaucasianmotherswhencomparedtoAfricandescendants. There may be cultural influences on infant feeding pat-terns in different ethnic groups; however, there is little evidence about how such patterns have been modified, andwhether theyhavebeen influencedby publicpolicies remainsunknown.23
Some limitations of this study should be emphasized. First,dataonhouseholdincomearerelatedtothetimeof the interview and not of the child’s birth; however, such incomewascategorizedinrelativeterms(tertiles)anditis possiblethatthesepositionshaveremainedstable.
Second,thesmallersample sizeinthe1960sand2000s reducedthestatisticalpowertodetectdifferencesbetween thevariablesintheseperiods;itshouldbenoted,however, that the sample size was larger in the 1980s and 1990s, but statistically significant differences were not observed intheseperiodsinrelationtobreastfeeding.Asforpossible recall bias,a test---reteststudy of the self-reported dura-tion of breastfeeding was carried out in a subpopulation of women followed since1999 in thePSS; theshort-term (14 days) andlong-term (13years) reliabilitywas consid-ered adequate, indicatingthat therecallbias maynotbe importantinthestudy(Robainaetal.,inpress).The exter-nal validitycan bequestioned, butthesimilaritywiththe evolutionofbreastfeedingpatternsobservedatthenational level allowsfor raising hypothesesabout the evolution of breastfeedingsincethe1960s.
Theresultsofthisstudydisclosedthedynamicsof breast-feedingdurationevolutionoverthedecades,withashorter durationinthe1970swhencomparedtothepreviousdecade and a subsequent increase in duration in the following decades.Moreover,morenoteworthyindividualdifferences were observed among the population of mothers in the 1970s.The resultingincrease in breastfeedingduration in the following decades suggests that theadoption of poli-cies,standards,andpracticesforthepromotion,protection and,supportofmaternalbreastfeeding,adoptedfromthe 1980sonward,werefavorabletothispractice.
Funding
State of Rio de Janeiro Research Foundation (n. E-26/010.001796/2015), Brazilian National ResearchCouncil (n.484636/2013-8).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
2.Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, EzzatiM,etal.Maternalandchildundernutrition:globaland regionalexposuresandhealthconsequences.Lancet.2008;371: 243---60.
3.Boccolini CS, Carvalho ML, Oliveira MI, Pérez-Escamilla R. Breastfeedingduringthefirst houroflifeandneonatal mor-tality.JPediar(RioJ).2013;89:131---6.
4.Pérez-EscamillaR,MartinezJL,Segura-PérezS.Impactofthe Baby-friendly Hospital Initiative on breastfeeding and child health outcomes: a systematic review. Matern Child Nutr. 2016;12:402---17.
5.VenancioSI,EscuderMM,SaldivaSR,GiuglianiER.Breastfeeding practiceintheBraziliancapitalcitiesandtheFederalDistrict: currentstatusandadvances.JPediatr(RioJ).2010;86:317---24. 6.Zuniga HP, Monteiro CA. Uma nova hipótese para a ascen-sãodamortalidade infantildacidadede SãoPaulo nosanos 60.In: Monteiro CA,editor. Velhos e novos males da saúde noBrasil:a evoluc¸ãodo país edesuas doenc¸as.São Paulo: HUCITEC/ABRASCO/NUPENS-USP;1995.p.157---73.
7.Jellife DB. Commerciogenic malnutrition. Food Technol. 1971;25:55.
8.AlmeidaJA,NovackFR.Amamentac¸ão:umhíbrido natureza-cultura.JPediatr(RioJ).2004;80:119---25.
9.ReaMF.Reflexõessobreaamamentac¸ãonoBrasil:decomo pas-samosa10mesesdedurac¸ão.CadSaudePubl.2003;19:37---45. 10.VenancioSI,SaldivaSR,MonteiroCA.Seculartrendsin
breast-feedinginBrazil.RevSaudePubl.2013;47:1205---8.
11.WorldHealthOrganization.Internationalcodeofmarketingof breast-milk substitutes.Geneva: World Health Organization; 1981.
12.Brasil.MinistériodaSaúdePesquisaNacionaldeDemografiae SaúdedaCrianc¸aedaMulher(PNDS).[cited12Set2015]. Avail-ablefrom:http://bvsms.saude.gov.br/bvs/pnds/index.php
13.Venâncio SI, Monteiro CA. A tendência da prática da amamentac¸ãonoBrasilnasdécadasde70e80.RevBras Epi-demiol.1998;1:40---9.
14.BoccoliniCS,CarvalhoML,OliveiraMI,BoccoliniPdeM. Breast-feeding can prevent hospitalization for pneumonia among childrenunder1yearold.JPediatr(RioJ).2011;87:399---404.
15.BoccoliniCS,BoccoliniPdeM,CarvalhodeML,OliveiradeMI. Exclusivebreastfeedingand diarrheahospitalizationpatterns between1999and2008inBrazilianStateCapitals.CienSaude Colet.2012;17:1857---63.
16.IBGE(Fundac¸ãoInstitutoBrasileirodeGeografiaeEstatística). Estudonacional dedespesa familiar.Rio deJaneiro: ENDEF; 1976.
17.FaersteinE,ChorD,LopesCS,WerneckGL.EstudoPró-Saúde: característicasgeraiseaspectosmetodológicos.RevBras Epi-demiol.2005;8:454---66.
18.FaersteinE,LopesCS,ValenteK,PláMA,FerreiraMB.Pré-testes deumquestionáriomultidimensionalautopreenchível:a exper-iênciadoEstudoPró-SaúdeUERJ.Physis:RevSaudeColetiva. 1999;9:117---30.
19.Brasil.MinistériodaSaúdeInstitutoparaoDesenvolvimentode Recursos.ProgramadePesquisasDemográficasedeSaúde-DHS. PesquisaNacionalsobreSaúdeMaterno-InfantilePlanejamento Familiar[Relatórioresumido].Maio;1989.
20.Bosi ML, Machado MT. Amamentac¸ão: um resgate histórico. CadernosESP.EscoladeSaúdePúblicadoCeará.2005;1:1---9.
21.PopkinBM,BilsborrowRE,AkinJS.Breastfeedingpatternsin low-incomecountries.Science.1982;218:1088---93.
22.RollinsNC,BhandariN,HajeebhoyN,HortonS,LutterCK, Mar-tinesJC,etal.Whyinvest,andwhatitwilltaketoimprove breastfeedingpractices?Lancet.2016;387(10017):491---504.