SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Total
hip
arthroplasty
complications
in
patients
with
or
without
controlled
diabetes
mellitus
during
hospitalization
夽
Fernanda
Rezende
Campos
Falcão
a,∗,
Bruno
Anderson
Gomes
Dias
a,
Liz
Araujo
Wolfovitch
a,
David
Sadigursky
a,baFaculdadedeTecnologiaeCiências(FTC),Salvador,BA,Brazil bClínicaOrtopédicaTraumatológica(COT),Salvador,BA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15January2016 Accepted28February2016 Availableonline31August2016
Keywords:
Totalhiparthroplasty Postoperativecomplications
Diabetesmellitus
a
b
s
t
r
a
c
t
Introduction:Totalhiparthroplasty(THA)isaprocedurethataimstorestorethefunction ofthehipjoint.Diabetesmellitus(DM)isoneofthemostprevalentcomorbiditiesamong patientsundergoingTHA.DMinvolvesvariousimmunologicalandmetabolicaspects,which leadtolimitationsandsurgicalcomplications.
Objective:ToevaluatetheassociationbetweenTHAcomplicationsandcontrolledDMduring hospitalizationperiod.
Methods:Cross-sectionalresearchthroughtheanalysisofretrospectiverecordsofa pri-vatehospitalinSalvador,Bahia.Thechi-squaredandFisher’sexacttestswereusedinSAS statisticalprogram.
Results:Mostpatientswereelderlyfemales.Themostprevalentcomorbiditiesinthesample werehypertensionanddiabetes.Themostfrequentunderlyingpathologyinthesamplewas coxarthrosis;amongpatientswithDM,itwasfemoralneckfracture.Themostcommon complicationswerechangesinthehemolymphopoieticsystem,amongwhichanemiawas themostfrequentcomplication.Cardiovascular,nervous,andbloodglucosecomplications werepositivelyassociatedwithcontrolledDM.Inturn,hemolymphopoietic,genitourinary, digestive,electrolyte,andinfectiouscomplicationswerenotassociatedwithDM.Having DMwasaprotectivefactorforthermalcomplications.Therewasnostatisticallysignificant differencebetweenpatientsthathadordidnothaveDMineachcomplicationgroupstudied.
Conclusion: PatientswithcontrolledDMdidnotpresentmorecomplicationsthanthose withoutDMduringhospitalizationinthepostTHA.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatClínicaOrtopédicaTraumatológica(COT),Salvador,BA,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.R.Falcão). http://dx.doi.org/10.1016/j.rboe.2016.08.016
Complicac¸ões
pós-artroplastia
total
de
quadril
em
portadores
e
não
portadores
de
diabetes
mellitus
controlado
durante
a
internac¸ão
Palavras-chave:
Artroplastiatotaldequadril Complicac¸õespós-operatórias
Diabetesmellitus
r
e
s
u
m
o
Objetivo: Avaliaraassociac¸ãoentreascomplicac¸õespós-ATQeDMcontroladonoperíodo dainternac¸ão.
Métodos: Pesquisadecortetransversalpormeiodaanálisedeprontuáriosretrospectivos deumhospitalparticularemSalvador(BA).Usaram-seostestesqui-quadradoeexatode FishernoprogramaestatísticoSAS.
Resultados: Amaioriadospacienteseradosexofemininoeidosa.Ascomorbidadesmais prevalentesdaamostraforamhipertensãoarterialsistêmicaeDM.Apatologiadebase maisfrequentenaamostrafoicoxartrose;jáentreospacientescomDM,foifraturadocolo dofêmur.Ascomplicac¸õesmaiscomunsforamalterac¸õesdosistemahemolinfopoiético. Dentreessasanemiafoiacomplicac¸ãomaisfrequente.Ascomplicac¸õesdoaparelho car-diovascular,dosistemanervosoe asglicêmicastiveramassociac¸ãopositiva comoDM controlado.Jáascomplicac¸õeshemolinfopoiéticas,geniturinárias,digestórias, eletrolíti-caseinfecciosasnãoapresentaramassociac¸ãocomDM.SerportadordeDMfoiumfator protetordecomplicac¸õestérmicas.Nãohouvediferenc¸aestatisticamentesignificanteentre ospacientesportadoresenãoportadoresdeDMemnenhumdosgruposdecomplicac¸ões estudados.
Conclusão:OspacientesportadoresdeDMcontroladonãoapresentarammaiscomplicac¸ões dosqueospacientesnãoportadoresdeDMduranteainternac¸ãonopós-operatóriodaATQ. ©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Totalhiparthroplasty(THA),aprocedureofreplacementof thehipjointwithaprosthesis,isarelativelysafe interven-tion.Theincreasedlifeexpectancyhaselevatedthenumberof procedures.1–3 IntheUnitedStates,morethan168,000THAs
and30,000implantsubstitutionsareperformedperyear.In Brazil,therearefewepidemiologicaldata.4,5
Coxarthrosis is the most common indication for THA. Other common indications are rheumatoid arthritis, frac-tures, and necrosis of the femoral head.6–8 THA aims to
relievepainandimprovefunctionalcapacity.1,9Complications
involve surgeryinfections, thromboembolism, and anemia, amongothers.Infectionsarethemostfeared,prevalent,and studiedcomplications.9Diabetesmellitus(DM),hypertension
(SAH),andheartdiseasesarethemostprevalentcomorbidities amongTHApatients.10,11
DM prevalence inBrazil is7.6%,12 and isinitially
char-acterizedbyhyperglycemia.Itistheresultofanomaliesin theinsulinsecretionand/oraction.Itinvolvesimmuneand metabolicaspects,whichfacilitateinfectionsandreducethe repairandhealingability.Chroniccomplicationsconferahigh degreeofmorbidityandmortality.Naturally,alterationsvary withtheintensityandlevelofcontrolofthedisease. There-fore,itisimportanttoassessthehealthconditionofthese patientsandtheneedforsurgicalintervention,andtoanalyze thecost–benefitofsurgeriessuchasTHA.13,14
There is a considerable lack of information about THA complicationsinpatients withDM.13 Thus, the analysisof
theprofileofpatientsandtheirpost-THAcomplicationscan contributetothedevelopmentofprotocols,pointto associ-ations,and assist theorthopedistin theindicationofTHA for diabetic patients. Therefore, this study aimed to eval-uate theassociation betweenpost-THAcomplicationswith andwithoutcontrolledDMduringtheperiodof hospitaliza-tion.
Materials
and
methods
Thiswasacross-sectionalstudythroughretrospective anal-ysisofmedicalrecordsofaprivatehospitalthatspecializes in the treatment of orthopedic patients, primarily from middle-andupper-class,whichbelongstotheprivate health-care network.In this hospital,two surgicalteams perform THA.
Thestudypopulationcomprisedhospitalpatients under-going THA. The calculated sample size, witha confidence interval of95% andasampleerror of5%, was84 patients. Permutedrandomizationwasdoneinblocksofpatients,so thatsamplewascomposedofthesamenumberofpatients operatedbyeachsurgicalteam,42each.Thestudyincluded patientswhounderwentTHAfromJanuary2013toDecember 2014andweredrawn.Patientswithincompleteorlostrecords inthehospitaldatabasewereexcluded.
areasofsclerosisandosteophyteformationand/orproximal femurfracture),andclinicalexamination(intensepainthat impairsfunctionandgait).
Collectedvariableswere:gender,age,smoking,alcoholuse, illicitdruguse,pre-existingchronicdiseases(DM,SAH, dys-lipidemia,and obesity),criteria forTHAindication, typeof surgery(primaryTHAorrevisionTHA),operatedside,useof cement,deathduringhospitalization,andclinical postopera-tivecomplicationsduringhospitalization.
Complicationswereclassifiedintogroups:cardiovascular system,respiratory system,digestive system,genitourinary tract,nervoussystem,oftheextremities,hemolymphopoietic system,electrolyte,infectious,thermal,glucose,sleep disor-ders,skindisorders,andpain.Themostprevalentgroupswere usedforstatisticalanalysis.
AmemberoftheInformationTechnology(IT)department ofthe hospitalconducted an active search for patients in themedicalrecordssystemwhohadundergoneTHAsurgery between2013and2014.Thissearchledtotherecord num-bers of patients who underwent this surgery within this period.
Later,threemedicalstudentsresearchersinvolvedinthis project were trained by a member of the IT department’s medicalrecordssystem.Theseresearcherstookturnsto col-lect data. Patient records and variables were inserted into Microsoft®Excel®2011forMac,version14.5.7,therefore cre-atingthedatabaseforthisresearch.
Inthedescriptivestatistics,absoluteandrelative frequen-cieswere used fornominal variables.Numerical variables, whetherdiscreteorcontinuous,wereanalyzedaccordingto measures of central tendency (mean or median) and dis-persion (standarddeviation and quartiles), consideringthe dependenceofthesampledistribution.
Intheanalytical statistics,theprevalenceratiowas cal-culatedwitha95%confidenceinterval(CI).Anerrorof5%˛ wasadopted(statisticalsignificance:p<0.05).Asthevariables werenominal,thechi-squaredandFisher’sexacttestswere used.Thelatterwasusedwhen50%ofthe2×2tablecellshad countslowerthanfive,asinthatcasethechi-squaredtestis notvalid.
TheprogramusedforthisanalysiswastheStatistical Anal-ysisSystem®(SAS)version9.4,asoftwaredevelopedbythe SAS Institute for advanced analysis, multivariate analysis, businessintelligence,datamanagement,andpredictive ana-lytics.
This study was approved by the Research Ethics Com-mittee of the Instituto Mantenedor de Ensino Superior da Bahia(IMES),CAAENo.49260815.0.0000.5032,inorderto com-ply withResolution No.466/2012 of the Brazilian National HealthCouncil.Itwasnotnecessarytoelaborateandsignan informedconsentform,asthiswasastudyofsecondarydata (medicalcharts).
Results
Out of the 84 patients, one was excluded due to incom-pletemedicalchart.Thus,thefinalsamplehad83patients. Ofthese,24(28.9%)hadDM; 66.3%ofthetotalsampleand 75% of the DM patients were female. SAH was present in
Table1–Categoricalepidemiologicalvariablesof patientsundergoingTHA,withandwithoutDMduring hospitalizationinahospitalinSalvador,BA,Brazil,from January2013toDecember2014.
Characteristics DM Total p-Value
Yes No
24(28.9%) 59(71.1%)
Sex 0.28a
Female 18(75%) 37(62.7%) 55(66.3%)
Male 6(25%) 22(37.3%) 28(33.7)
Smoking 3(12.5%) 3(5.1%) 6(7.2%) 0.35b
Alcohol consumption
3(12.5%) 6(10.3%) 9(10.8%) 0.72b
Useofillicitdrugs 0 1(1.7%) 1(1.2%) >0.9b
Obesity 4(16.7%) 2(3.4%) 6(7.2%) 0.055b
Dyslipidemia 9(37.5%) 8(13.6%) 17(20.5%) 0.032b
SAH 21(87.5%) 32(54.2%) 53(63.9%) 0.004a
THAindication 0.019b
Coxarthrosis 8(34.8%) 38(64.4%) 46(55.4%) Femurfracture 14(60.9%) 18(30.5%) 32(38.6%) Otherarthrosis 0 2(3.4%) 2(2.4%)
Osteonecrosis 0 1(1.7%) 1(1.2%)
Osteomyelitis 1(4.4%) 0
Surgery 0.35b
Primary 23(27.7%) 50(60.2%) 73(88%) Secondary 1(4.2%) 9(15.3%) 10(12%)
Side 0.82a
Right 14(58.3%) 36(61%) 50(60.2%)
Left 10(41.7%) 23(39%) 33(39.8%)
Useofcement 8(33.3%) 23(39%) 31(37.4%) 0.63a
Death 1(1.2%) 2(2.4%) 3(3.6%) 1b
a Peason’schi-squaredtest.
b Fisher’sexacttest.
63.9%ofthesampleandin87.5%ofpatientswithDM.The preoperative diagnosis of coxarthrosis was made in 55.4% ofthe sample;amongdiabetics,femoralneckfracture was the indication of the THA in 60.9% of patients (p=0.019; Table1).
Meanagewas66.8years(±15.73,range:33–95);themean ageofDMpatientswas72.8(±1.85,range:41–89)andthatof non-DMpatientswas64.3(±16.32,range:33–95).
Allpatientsreceivedprophylaxisfordeepvenous thrombo-sisandantibioticprophylaxisinaccordancewiththecurrent literature.14,15
In the sample,79.5% of patientshad at leastone clini-calcomplicationduringthehospitalizationperiod,whether or not related tothe surgicalprocedure, fora total of229 complications. Fig. 1 shows the frequencies of complica-tions, which were grouped and are described below. Some patients had more than one complication from the same group.
22%
20%
19% 11%
5% 4% 4%
4% 3%
3% 3% 1% 1% 0%
HLP
GUT
CVS
DS
Infectious
Electrolytic
RS
NS
Thermal
Glycemic
Skin
Sleep
Pain
Extremities
Fig.1–Frequenciesofhemolymphopoietic(HLP),genitourinary(GUT),cardiovascular(CVS),digestive(DS),electrolytic, respiratory(RS),nervoussystem(NS),infectious,thermal,glycemic,skin,sleep,pain,andextremitiescomplicationsin patientsundergoingTHA(229complications)duringinahospitalinSalvador,BA,BrazilfromJanuary2013toDecember 2014.
andretrovesicalfistula(2%).Thecardiovascularsystemhad 18.3%ofcomplications(42):hypotension(43%),hypertensive peak(17%),hypovolemicshock(14%),tachycardia(7%),cardiac arrest(5%),septicshock(2%),acutemyocardialinfarction(2%), atrialfibrillation(2%),tachyarrhythmia(2%),bradycardia(2%), andhemodynamicinstability(2%).
The digestive tract presented 10.9% of the complica-tions(25):constipation(84%),epigastricpain(4%),dysphagia (4%), vomiting (4%), and diarrhea (4%). Infections hap-pened ten times (4.5%); among these, the following were observed:postoperativewoundinfection(40%),catheter infec-tion (20%), osteomyelitis (20%), oropharyngeal infections (10%), and sepsis (10%). Electrolyte changes occurred nine times (3.9%), as hyponatremia(78%) and hypomagnesemia (22%). Inthe respiratory system, nine complications(3.9%) were observed: desaturation (11%), dyspnea (11%), acute respiratoryfailure(11%),bronchialaspiration(11%), pneumo-nia(11%),pleural thickening(11%), atelectasis(11%),apical nodules (11%), and bilateral pleural effusion (11%). In the nervous system, eight complications(3.5%) were observed: decreasedlevelofconsciousness(38%),ischemic encephalo-vascular disease (12.5%), delirium (12.5%), encephalopathy (12.5%),hypothymia(12.5%),andhypoactivity(12.5%). Ther-malcomplicationswere observed seventimes(3.1%): fever (86%) and hypothermia (14%). Glucose complications were observedsixtimes: hyperglycemia(83%)and hypoglycemia (17%).
Skindisorderswereobservedsixtimes(2.6%):eschar(17%), ecchymoses (17%), fistula (17%), hematic collection (17%), bleedingfromthesurgicalwound(17%),andlesioninthe scro-tum(17%).Insomniawastheonlysleepdisturbancereported,
having occurred in two cases (0.9%). Pain was also only describedinthemedicalrecordstwice(0.9%),bothinthe oper-atedlimb.Amongthecomplicationsoftheextremities,there wasasinglecaseoflowerlimbedema(0.4%).
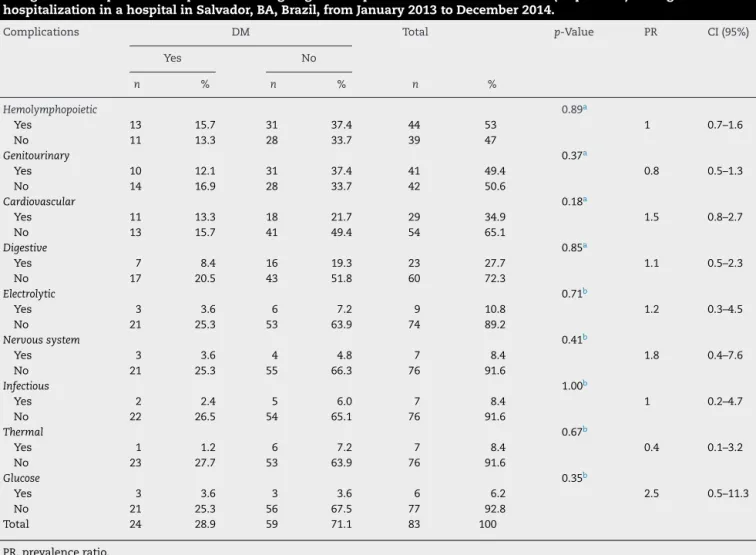
Table 2 presents analytical statistics. For this, the nine mostprevalentgroupsofcomplicationsinthepatientsofthe sample(83)wereused.Apositiveassociationwasobserved betweenthe groupsofcardiovascularsystem, nervous sys-tem,andglycemiccomplications.Therewasnoassociation betweengroupsofhemolymphopoietic,genitourinary, diges-tive, electrolytic, and infectious complications. There was aninverseassociationinthermalcomplications.Therewas no statisticallysignificant differencebetweenpatientswith and without DM in any of the groups of complications studied.
Discussion
Table2–Hemolymphopoietic,genitourinary,cardiovascular,digestive,electrolytic,nervoussystem,infectious,thermal, andglucosecomplicationsinpatientsundergoingTHAinpatientswithandwithoutDM(83patients)during
hospitalizationinahospitalinSalvador,BA,Brazil,fromJanuary2013toDecember2014.
Complications DM Total p-Value PR CI(95%)
Yes No
n % n % n %
Hemolymphopoietic 0.89a
Yes 13 15.7 31 37.4 44 53 1 0.7–1.6
No 11 13.3 28 33.7 39 47
Genitourinary 0.37a
Yes 10 12.1 31 37.4 41 49.4 0.8 0.5–1.3
No 14 16.9 28 33.7 42 50.6
Cardiovascular 0.18a
Yes 11 13.3 18 21.7 29 34.9 1.5 0.8–2.7
No 13 15.7 41 49.4 54 65.1
Digestive 0.85a
Yes 7 8.4 16 19.3 23 27.7 1.1 0.5–2.3
No 17 20.5 43 51.8 60 72.3
Electrolytic 0.71b
Yes 3 3.6 6 7.2 9 10.8 1.2 0.3–4.5
No 21 25.3 53 63.9 74 89.2
Nervoussystem 0.41b
Yes 3 3.6 4 4.8 7 8.4 1.8 0.4–7.6
No 21 25.3 55 66.3 76 91.6
Infectious 1.00b
Yes 2 2.4 5 6.0 7 8.4 1 0.2–4.7
No 22 26.5 54 65.1 76 91.6
Thermal 0.67b
Yes 1 1.2 6 7.2 7 8.4 0.4 0.1–3.2
No 23 27.7 53 63.9 76 91.6
Glucose 0.35b
Yes 3 3.6 3 3.6 6 6.2 2.5 0.5–11.3
No 21 25.3 56 67.5 77 92.8
Total 24 28.9 59 71.1 83 100
PR,prevalenceratio.
a Peason’schi-squaredtest.
b Fisher’sexacttest.
Theresultsshowsimilarepidemiologicalcharacteristicsto thoseofpreviouslypublishedstudies;thatis,mostpatients wereagedover65years,theprevalenceoffemale osteoarthri-tiswasthemostcommonindicationforsurgery,andSAHwas mostfrequentclinicalcomorbidity.1,10,16–18
Ofthepatients,28.9%hadadiagnosisofDM.Theliterature variesregardingtheprevalenceofDM:from34.2%to9.2%.10,11
ThehighestmeanageofpatientswithDM(sixyearsolder) isjustifiedbythefact that theincidenceofthis pathology intensifieswithincreasingage.19Aliteraturereviewshowed
reductionin the surgicalsite infection rate, mortality, and lengthof hospitalization in patients with controlled blood glucose.14
In the present study, the prevalence of SAH was 64%; similarstudiesreported50.4%10 and45.9%.11Therewasno
statisticallysignificantdifferencebetweenDMand comorbidi-ties:SAH(p=0.004)anddyslipidemia(p=0.03).Inturn,obesity hadap-valuethat wasveryclosetostatisticalsignificance (p=0.06).Therefore,anassociationofDMwithSAHand dys-lipidemiawasobservedinthispopulation;probablymanyof
thepatientshadadiagnosisofmetabolicsyndrome,butthis diagnosiswasnotdocumentedinthemedicalrecordsofany patient.
TheICD-10thatwasmostdeclaredasthemaindiagnosis wasM16.9(unspecifiedcoxarthrosis),in55.42%ofthe sam-ple.Otherstudiesalsoobservedthediagnosisofcoxarthrosis as the primaryindicationofTHA, one with49.1% and the other with 92.4%,respectively, of patients who underwent THA.10,11 In the present study, among patients with DM,
theICD-10 mostcommonlycitedwastheS72.0(fractureof neck offemur) in60.87% ofpatients, astatistically signifi-cantdifference(p=0.02).Nodataonthe baselinediagnosis forTHAindicationinpatientswithDMwereretrievedinthe literature.However,it isknown thatdiabetic patientshave low bonemetabolism, decreasedbone formationand, toa lesserextent,decreasedreabsorption.Thesefactorsleadto anincreasedriskoffracturesinDMpatients.Themechanism isunknownandlikelytobemultifactorial.20,21
studies,secondaryTHArevisionaccountedforaminorityof procedures.Inotherstudies,thefrequencyofprimaryTHA was92.4%and98%,respectively.10,11
Right side was the most operated within total sample (60.24%)andinDMpatients(58.33%).Theliteratureis diver-gentastothemostoperatedsideinTHA;insomestudies,the involvementoftheleftorrightsidewassimilar.22,23Inturn,in
somestudiesthemostoperatedsidewastheright,69.2%and 55.6%respectively.24,25Anothersurveyfoundaslight
predom-inanceoftheleftside,with53.5%.26Bonecementwasusedin
37.35%ofthesample.Pianoetal.11usedcementin48%oftheir
THApatients.
Inthepresent sample,themortalityratewas3.6%,with threedeaths.Onepatientdevelopedosteomyelitis,later pro-gressing with sepsis and then cardiac arrest, having died on the 115th day of hospitalization. One patient had a hypovolemicshock and died inthe first postoperativeday. Thethirdhadasepticshock,followedbyventricular tachycar-diaandcardiacarrest,havingdiedonthe15thpostoperative day. Another study found a mortality rate of 0.1% in a sample of 344 patients undergoing THA.10 There was no
statistically significant difference between the deaths of patients withand without DM (p=1) inthe present study. A hip fracture post-correction mortality survey showed a correlation between higher number of clinical comorbidi-ties, longer hospital stays, and use of general anesthesia insurgerywithhighermortality.22 However,there wereno
data about the mortality of diabetic patients undergoing THA.
AlthoughTHAisreportedintheliteratureasarelatively safeintervention,79.5%ofpatientshadsomecomplication, inatotalof229 clinicalcomplicationsduringhospitalstay of patients (related or unrelated to surgery). This demon-strates that surgeons should be cautious. A study with a sampleof334patientswhounderwentTHAfound76clinical complications.10
Themostprevalentinfectionswere UTIinninepatients (10.8%),followedbywoundinfectioninfour(4.8%).Areview thataddressedthecausesandcontrolofinfectionsinsurgical patientsalsofoundUTIasthemostcommoninfectionin sur-gicalpatients.14Astudyofnosocomialinfectionsinpatients
undergoingTHApresentedincidenceof15.1%;wound infec-tionwasthemostcommon(13%),followedbyUTI(2.1%).27
Authors stated that UTI has lower mortality; that surgical woundinfectionisthesecondinfrequency,butthethirdin costs;andthathematologicinfectionandpneumoniaareless common,butwithhighmortalityandhighcosts.14Although
theliteraturedescribesDMasariskfactorforinfections,28no
statisticallysignificantdifferencewasobservedinthepresent study forpatientswith and withoutDM. A possible expla-nationisbecausepreoperativeglycemiccontrolisassociated withadecreaseininfectiouscomplicationsindifferenttypes ofsurgery.14
AfterUTI, whichwas the mostprevalent,Lenzaet al.10
foundthefollowingascomplications:surgicalsiteinfection (1.5%), respiratory failure (1.5%), and anemia (1.5%). In the presentstudy,respiratoryfailureoccurredinonepatient(1.2%) andanemiawasthemostcommoncomplication,in44(53%). Thisindicatesthatpatientsloseasignificantamountofblood duringsurgery.Findingtheriskfactorsforthiscomplication
isimportantforeffectiveprevention.Thereductionincases ofanemiaduetobleedingalsopreventsotherconditions,e.g., hypovolemicshock,whichwasobservedinfivepatients(6%) inthepresentstudy.
Onestudyfounddeepveinthrombosisasacomplication inTHAin1.2%ofpatients.10Inthepresentstudy,therewere
nocasesofdeepveinthrombosis,whichprobablyindicates thattheprotocolfollowedbytheinstitutionforthispathology isefficient.
Anobservationalstudyof202elderlypatientswho under-wentTHAandtotalkneearthroplastyobservedthatthehigher theage,thehighertheincidenceofcomplications.29This
con-firmsthehighrateofcomplicationsinthepresentstudy,since themeanagewashigh,66.8years(±15.73,range:33–95)inthe totalsampleand72.8years(±11.85,range:41–89)inpatients withDM.
The hemolymphopoietic, genitourinary, digestive, elec-trolytic,andinfectiouscomplicationgroupshadaprevalence ratioofapproximatelyone.Thisindicatesthattheprevalence rate ofcomplications inexposed and unexposed groupsis identical,i.e.,thereisnoassociation.
Thecomplicationsofthecardiovascularsystemand ner-vous system showed a prevalence rate of approximately two, and glycemic complications, of approximately three. Thus, there is a positive association or increased risk among those exposed to the factor studied when com-pared with those unexposed. Therefore, patients with DM had atwo-foldincreasedrisk forcomplicationsofthe car-diovascular system and nervous system, and three times moreglycemiccomplicationswhencomparedwithpatients withoutDM.
Theprevalenceratioofthermalcomplicationswas approx-imatelyzero,i.e.,thereisaninverseassociationoradecreased riskamongthoseexposedtothefactorstudied,whichisthe so-calledprotectionfactor.Thus,havingDMwasaprotective factorforthermalcomplications.
There wasnostatisticallysignificantdifferencebetween patientswithandwithoutDMinanyofthegroupsof compli-cationsstudied.Thismeansthatthechanceofthisdifference betweenmeansbeduetochance(andnotaresultoftheDM) isabove5%(alphaerror).Therefore,thenullhypothesiscould notberejected,astherewasnotstrongenoughevidenceto provethatthenullhypothesiswasfalse.Theconfidence inter-valalsoshowsthatthegroupsaresimilar,provingthatthere isnodifferencebetweenthegroups.Thus,itcanbeinferred thatpatientswithcontrolledDMdidnotpresentmore com-plicationsthanthosewithoutDMinthepost-operativeperiod ofTHA,duringhospitalization.
When describing characteristics of patients undergoing THA in a private hospital, it isessential to compare with other hospitals. Thisanalysis iscomplex duetothe diver-sity of the population, description of the methods, study design,studyperiods,anddifferenthealthcaresystems. How-ever, cross-sectional and qualitative analyses are essential to improve healthcare in each of the populations.10 Data
Thereare limitationstothepresent results.Firstly,data wereanalyzedretrospectivelyfromthedatabase,whichleads to some questions about its collection. Secondly, a cross-sectional study is descriptive, hence causal inferences are impossible.Otherfactorsmayalsohaveinfluencedthe com-plicationsofTHA.Thereisnopresumptionthatthefeatures ofthissamplewillremainthesame.Duetothedesignofthis study andsmall samplesize,the authors recommendthat furtherstudiesinvolvinglargersamplesizesofpatientsfrom severalcentersshouldbeconducted.
Conclusion
Theresultsofthisstudyshowedthattherewasnostatistically significantdifferencebetweenthepost-THAcomplicationsin patientswithand withoutcontrolledDMduringthe period ofhospitalization.Withtheseresults,itcanbeinferredthat theorthopedistmayindicateTHAfortheircontrolleddiabetic patientsaftertakingstandardcaremeasures.Ascontrolled diabeticpatientsdonotpresent morecomplications, a dif-ferentprotocolormorecautiousmeasuresarenotrequired. Patient can be warned that THA does not bring higher risk for individuals with controlled diabetes than for the non-diabetic.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. KeurentjesJC.Predictorsofclinicaloutcomeintotalhipand kneereplacement:amethodologicalappraisalofimplants andpatientfactors[tese].Leiden,Holanda:LeidenUniversity; 2014.Availablefrom:https://openaccess.leidenuniv.nl/ handle/1887/28958[accessed03.11.15].
2. NemesS,GordonM,RogmarkC,RolfsonO.Projectionsof totalhipreplacementinSwedenfrom2013to2030.Acta Orthop.2014;85(3):238–43.
3. SchwartsmannCR,BoschinLC,Gonc¸alvesRZ,YépezAK, SpinelliLF.Novassuperfíciesemartroplastiatotaldoquadril. RevBrasOrtop.2012;47(2):154–9.
4. CohenM.Tratadodeortopedia.Sa˜oPaulo:Roca;2007. 5. GuedesRC,DiasJMD,DiasRC,BorgesVS,LustosaLP,Rosa
NMB.Artroplastiatotaldequadrilemidosos:impactona funcionalidade.RevBrasFisioter.2011;15(2):123–30. 6. PatrizziLJ,Vilac¸aKHC,TakataET,TrigueiroG.Análiseprée
pós-operatóriadacapacidadefuncionalequalidadedevida depacientesportadoresdeosteoartrosedequadril submetidosàartroplastiatotal.RevBrasReumatol. 2004;44(3):185–91.
7. SiddiquiMM,YeoSJ,SivaiahP,ChiaSL,ChinPL,LoNN. Functionandqualityoflifeinpatientswithrecurvatum deformityafterprimarytotalkneearthroplasty:areviewof ourjointregistry.JArthroplasty.2012;27(6):1106–10. 8. SoeverLJ,MackayC,SaryeddineT,DavisAM,FlanneryJF,
JaglalSB,etal.Educationalneedsofpatientsundergoingtotal jointarthroplasty.PhysiotherCan.2010;62(3):206–14. 9. SinghJA.Epidemiologyofkneeandhiparthroplasty:a
systematicreview.OpenOrthopJ.2011;5:80–5.
10.LenzaM,FerrazSB,ViolaDCM,GarciaFilhoRJ,Cendoroglo NetoM,FerrettiM.Epidemiologiadaartroplastiatotalde quadriledejoelho:estudotransversal.Einstein. 2013;11(2):197–202.
11.PianoLPA,GolmiaRP,ScheinbergM.Artroplastiatotalde quadrilejoelho:aspectosclínicosnafaseperioperatória. Einstein.2010;8(3):350–3.
12.MalerbiDA,FrancoLJ.Multicenterstudyoftheprevalenceof diabetesmellitusandimpairedglucosetoleranceinthe urbanBrazilianpopulationaged30–69yr.TheBrazilian CooperativeGroupontheStudyofDiabetesPrevalence. DiabetesCare.1992;15(11):1509–16.
13.FardinAC,Marcondes-AranegaA,Gaetti-JardimEC, Buso-RamosMM,Âmbar-LinsS,Gaetti-JardimJúniorEL. Cuidadosespeciaisnoatentimentocirúrgicodepacientes diabéticos.RevistaATO.2009;(June).Availablefrom:http:// www.actiradentes.com.br/revista/2009/textos/23RevistaATO-Diabetes-2009.pdf[accessed03.10.15].
14.FreitasPS,RomanziniAE,RibeiroJC,BellusseGC,GalvãoCM. Controleglicêmiconoperioperatório:evidênciasparaa prevenc¸ãodeinfecc¸ãodesítiocirúrgico.RevEletrEnf. 2013;15(2):541–50.
15.JørgensenCC,JacobsenMK,SoeballeK,HansenTB,HustedH, Kjærsgaard-AndersenP,etal.Thromboprophylaxisonly duringhospitalisationinfast-trackhipandkneearthroplasty, aprospectivecohortstudy.BMJOpen.2013;3(12):e003965. 16.AbdelSalamH,RestrepoC,TarityTD,SangsterW,ParviziJ.
Predictorsofintensivecareunitadmissionaftertotaljoint arthroplasty.JArthroplasty.2012;27(5):720–5.
17.deBeerJ,PetruccelliD,AdiliA,PiccirilloL,WismerD, WinemakerM.Patientperspectivesurveyoftotalhipvstotal kneearthroplastysurgery.JArthroplasty.2012;27(6):865–9, e1-5.
18.TirkkonenK,HurmeS,RautavaP,VirolainenP.Electronic medicalrecordsforappropriatetimingofarthroplasty.JEval ClinPract.2013;19(1):209–13.
19.Diagnosisandclassificationofdiabetesmellitus.Diabetes Care.2010;33Suppl.1:S62–9.Availablefrom:
http://care.diabetesjournals.org/content/33/Supplement1/ S62.full.pdf[accessed21.10.15].
20.HamannC,KirschnerS,GüntherKP,HofbauerLC.Bone, sweetbone–osteoporoticfracturesindiabetesmellitus.Nat RevEndocrinol.2012;8(5):297–305.
21.SilvaMBG,SkareTL.Manifestac¸õesmusculoesqueléticasem
diabetesmellitus.RevBrasReumatol.2012;52(4):594–609. 22.ArlianiGG,AsturDC,LinharesGK,BalbachevskyD,Fernandes
HJA,ReisFB.Correlac¸ãoentretempoparaotratamento cirúrgicoemortalidadeempacientesidososcomfraturada extremidadeproximaldofêmur.RevBrasOrtop.
2011;46(2):189–94.
23.VicenteJRN,MiyaharaHS,LuzoCM,GurgelHM,CrociAT. Artroplastiatotaldoquadrilfeitaporviaposterior
minimamenteinvasiva–Resultadosapósseisanos.RevBras Ortop.2015;50(1):77–82.
24.GuimaraesRP,SouzaGS,ReginaldoSS,OnoNK,HondaEK,Ci PoleselloG,etal.Estudodotratamentodasfraturasdacabec¸a dofêmur.RevBrasOrtop.2010;45(4):355–62.
25.QueirozRD,PenaLF,BorgerRA,MoreteRA,TakanoMI,Franco RS.Aacuráciadacirurgiaassistidapornavegadorna artroplastiatotaldoquadril.RBMRevBrasMed.
2010;67(esp.7).Availablefrom:http://www.moreirajr.com.br/ revistas.asp?fase=r003&idmateria=4428[accessed07.11.15]. 26.RicciG,LongarayMP,Gonc¸alvesRZ,UngarettiNetoAS,
ManenteM,BarbosaLBH.Avaliac¸ãodataxademortalidade emumanoapósfraturadoquadrilefatoresrelacionadosà diminuic¸ãodesobrevidanoidoso.RevBrasOrtop.
27.LimaALL,BaroneAA.Infecc¸õeshospitalaresem46pacientes submetidosaartroplastiatotaldequadril.ActaOrtopBras. 2001;9(1):36–41.
28.DuarteGMH,AlbertiLR.Artroplastiatotalcimentadado quadril.RevMedRes.2013;15(1):36–49.