www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Preoperative
vestibular
assessment
protocol
of
cochlear
implant
surgery:
an
analytical
descriptive
study
夽
Roseli
Saraiva
Moreira
Bittar,
Eduardo
Setsuo
Sato
∗,
Douglas
Jósimo
Silva
Ribeiro,
Robinson
Koji
Tsuji
UniversidadedeSãoPaulo(USP),EscoladeMedicina,DepartamentodeOtorrinolaringologia,SãoPaulo,SP,Brazil
Received2July2015;accepted20June2016 Availableonline31July2016
KEYWORDS
Cochlearimplant; Vestibularfunction; Preoperative diagnosis
Abstract
Introduction:Cochlearimplantsareundeniablyaneffectivemethodfortherecoveryofhearing functioninpatientswithhearingloss.
Objective:Todescribethepreoperativevestibularassessmentprotocolinsubjectswhowillbe submittedtocochlearimplants.
Methods:Ourinstitutionalprotocolprovidesthevestibulardiagnosisthroughsixsimpletests: RombergandFukudatests,assessmentforspontaneousnystagmus,HeadImpulseTest, evalu-ationforHeadShakingNystagmusandcalorictest.
Results:21patientswereevaluatedwithameanageof42.75±14.38years.Only28%ofthe samplehad allnormaltest results.Thepresence ofasymmetricvestibular informationwas documentedthroughthecalorictestin32%ofthesampleandspontaneousnystagmuswasan importantclueforthediagnosis. Bilateralvestibular areflexiawas presentinfoursubjects, unilateralarreflexiainthreeandbilateral hyporeflexiaintwo.TheHeadImpulseTestwasa significantindicatorforthediagnosisofareflexiainthetestedear(p=0.0001).Thesensitized Rombergtestusingafoampadwasable todiagnoseseverevestibular functionimpairment (p=0.003).
Conclusion:Thesixclinicaltestswereabletoidentifythepresenceorabsenceofvestibular functionandfunctionasymmetrybetweentheearsofthesameindividual.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:BittarRS,SatoES,RibeiroDJ, TsujiRK.Preoperativevestibularassessmentprotocolofcochlearimplant
surgery:ananalyticaldescriptivestudy.BrazJOtorhinolaryngol.2017;83:530---5.
∗Correspondingauthor.
E-mail:[email protected](E.S.Sato).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.06.014
PALAVRAS-CHAVE
Implantecoclear; Func¸ãovestibular; Diagnóstico pré-operatório
Protocolodeavaliac¸ãovestibularpré-operatóriadacirurgiadeimplantecoclear: estudodescritivoanalítico
Resumo
Introduc¸ão: Osimplantescocleares(IC)sãoindiscutivelmenteummétodoeficazderecuperac¸ão dafunc¸ãoauditivadepacientessurdos.
Objetivo: Descreveroprotocolodeavaliac¸ãovestibularpré-operatóriaemsujeitosqueserão submetidosaoIC.
Método: Nossoprotocoloinstitucionalprevêodiagnósticovestibularpormeiodeseistestes simples:testesdeRombergeFukuda,nistagmoespontâneo,HeadImpulseTest,HeadShaking Nistagmus,provacalórica.
Resultados: Foramavaliados21pacientescomidademédiade42,75±14,38anos.Apenas28% daamostraapresentoutodosostestesnormais.Apresenc¸adeinformac¸ãovestibularassimétrica foidocumentadapelaprovacalóricaem32%daamostraeonistagmoespontâneomostrou-se pistaimportanteparaseudiagnóstico.Aarreflexiavestibularbilateralfoidiagnosticadaem qua-trosujeitos;arreflexiaunilateralemtrêsehiporreflexiabilateralemdois.OHeadImpulseTest
mostrou-seindicadorsignificante(p=0,0001)paradiagnosticararreflexiadaorelhatestada.O testedeRombergsensibilizadoemalmofadafoicapazdediagnosticaroscomprometimentos severosdafunc¸ãovestibular(p=0,003).
Conclusão:Osseistestesclínicosforamcapazesdeidentificarapresenc¸aounãodefunc¸ão vestibulareassimetriadafunc¸ãoentreasorelhasdeummesmoindivíduo.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Cochlearimplants(CI)arehighlyeffectivedevicesfor recov-eryofhearingfunctioninindividualswithhearinglossand have facilitated integration into social life. The success ofpost-implantrehabilitationhasraisednewchallengesin boththeselectionandtheplanningofthehearing progno-sis of subjects undergoing surgery. Although the cochlear system is distinct from the vestibular system, both have identical neural transmission.The benefits of the electri-calstimulationoftheCIgobeyondtheauditorypathways andalsobenefitthevestibularsystemandposturalcontrol.1
Nonetheless, the CI is not without risk to the semicircu-lar canaland otolithfunction andmayimpairor suppress vestibular function, especially if there is pre-existing pathology.
The prevalenceofpostoperativedizzinessvarieswidely intheliteratureandis around20% inourcases.Itusually resolvesinapproximately30 days.Someof thesepatients developbilateralvestibularareflexia(BVA),whichseverely reducespatientqualityoflife.2Knowledgeofvestibular
sys-temfunction beforeand after CIsurgery is importantfor thesatisfactory managementofeach case.Therefore,we have added vestibular assessment to our outpatient rou-tine prior to CI surgery. Our main goal is to document the existence of vestibular function and possible asym-metriesbetweentheearsbeforesurgery.Thisinformation canhelp intheselection ofwhich eartoimplantand can assistin the management of any postoperative vestibular symptoms.
In adults, preoperative vestibular assessment was designedtobebriefandeasy toperform,usingresources
availableatanyotorhinolaryngologyoutpatientclinic.The testsusedareable toidentifyboth vestibularasymmetry fromunilaterallesionsaswellasbilateralinvolvement.The protocolwasdesignedtobeaccessibletoservicesthat per-formCI surgery but do not always have a neurotological departmentandresearchequipment.
It is not our intention to speak at length about each vestibular test used, but to provide the reader a quick andconvenientmethodtoidentifyvestibularimpairment. Knowledgeofvestibularfunctioncanindicatetheadequate managementandpreventundesirablesideeffects.3,4
Ourgoalistodescribethepreoperativevestibular assess-mentofadultpatientswhoarecochlearimplantcandidates inourinstitution,demonstrateitseffectivenessanddiscuss itsimportanceinthepostoperativeoutcome.
Methods
Thisisadescriptiveandanalyticalcross-sectionalstudythat followed the ethical standards approved by the CAEPesq number0983.07. All participants arefrom the Institution OtorhinolaryngologyClinic.
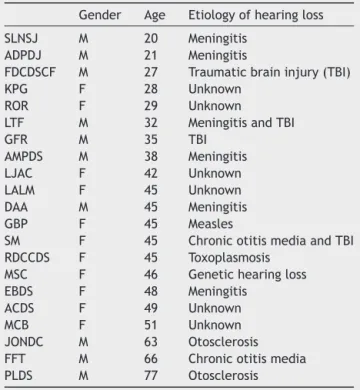
Table1 Listofassessedpatientsregardinggender,ageand etiologyofhearingloss.
Gender Age Etiologyofhearingloss
SLNSJ M 20 Meningitis ADPDJ M 21 Meningitis
FDCDSCF M 27 Traumaticbraininjury(TBI)
KPG F 28 Unknown
ROR F 29 Unknown
LTF M 32 MeningitisandTBI
GFR M 35 TBI
AMPDS M 38 Meningitis LJAC F 42 Unknown LALM F 45 Unknown DAA M 45 Meningitis
GBP F 45 Measles
SM F 45 ChronicotitismediaandTBI RDCCDS F 45 Toxoplasmosis
MSC F 46 Genetichearingloss EBDS F 48 Meningitis
ACDS F 49 Unknown
MCB F 51 Unknown
JONDC M 63 Otosclerosis FFT M 66 Chronicotitismedia PLDS M 77 Otosclerosis
completeabsenceofvestibularfunction.Thestudysample includingtheiragesandetiologiesareshowninTable1.
VORandvestibularasymmetryassessment5
Spontaneousnystagmus6
Spontaneousnystagmus(SN)is ocularmovement observed withthepatientinthesittingpositionwiththeeyesfixed straight ahead. The presence of SN indicates vestibular asymmetryandis theresults of asymmetryin oculomotor tonethatoriginatedfromthevestibularsystem.Itconsistsin aslowgazedeviation,followedbyaquickmovementofthe eyeballtothecenterposition(correctivesaccades).When ithasaperipheralorigin,spontaneousnystagmusdecreases witheyefixation and intensifieswhen theeye is diverted 30◦ toward the fast component (Alexander’s Law).6 The
directionof the nystagmusis the direction ofthe correc-tivesaccadewhichiseasiertovisualize.Butitistheslow gazedeviationthatdeterminesthesidewith hypofunction-inglabyrinth.
HeadImpulseTest(HIT)7
TheHeadImpulseTestisasimpleclinicalmaneuverto iden-tifyanimpairedvestibulo-ocularreflexinthetestedearby observingtheocularresponsethatoccursafteraquickhead movement.Whilefacingtheexaminer,thepatientfocuses onatargetontheexaminer’sface.Theexaminerholdsthe patient’sfaceinhis/herhandsandsuddenlyturnshis/her head,andobservestheocularresponse.Anormalindividual willkeephis/hereyesonthetarget,butwhenthe vestibulo-ocular reflex (VOR) is impaired, the eyes will follow the movementoftheheadandthen performasaccadeinthe
oppositedirectiontothecorrectiveheadmovementto re-fixateonthevisualtarget.
HeadShakingNystagmus8,9
TheHeadShakingNystagmus(HSN)examinationinvestigates asymmetryofmuscletoneathighfrequenciesofhead rota-tion.The patientsitsface-to-face withtheexaminer and looksatatargetontheexaminer’sface.Thenthepatient performs20lateralheadturnsathighspeed.Attheendof thetest,thepatientinterruptstherotations,stabilizesthe headandremainsfacingthefrontdirection.The presence ofnystagmusindicatesasymmetryofvestibularinformation. Inperipherallabyrinthinedisorders,theslowgazedeviation indicatesahypofunctioninglabyrinth.
Calorictesting5
Calorictestingisperformedinthesupinepositionwiththe headflexed30◦.Waterat 30◦ and44◦ isthestimulusused
for thetest.Irrigations areperformed inboth earswitha five-minute interval between them. The resulting nystag-musis recordedusingnystagmography equipment.Normal angular velocities of nystagmus are between 7◦ and 52◦.
Whentheangularvelocityofthemovementsexceedsthese limits,it is called hyperreflexia andwhen it is below the minimum,hyporeflexia. The equipmentusedin this study wasthevector-electronystagmographySCEContronic®.
Labyrinthine predominance (LP) designates asymmetry betweenthevestibularresponses.Avalueof18%waschosen for LP.The presenceofLP meansasymmetryofvestibular informationofperipheralorcentraloriginandalways indi-catesthesidewithbetterfunction.
Posturaltestassessment
Alterations of the Romberg’s and Fukuda’s tests are not pathognomonicofvestibularpathology,althoughtheyhelp with the diagnosis. The tests can be influenced by pro-prioceptive or neurological lesions and should be used in conjunctionwithothervestibulartests.
Romberg’stest10
The patientis instructedtostandwithheelstogetherand toesapartatapproximately30◦
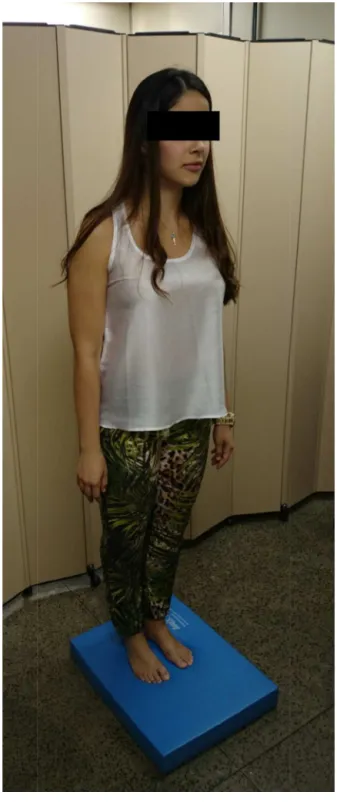
Figure1 Testusingafoampad.
Fukuda’stest12
Fukuda’stestisusedtoidentifytoneasymmetriesinthe dis-tallower-limbmuscles.Witharmsoutstretched,thepatient isaskedtomarch60stepswiththeeyesclosedandwithout moving.The subject’sanglesof deviationandshiftingare evaluated.Attheendofthetest,anangulardeviationofup to30◦
andthelineardisplacementofupto50cmare consid-erednormal.Theposteriordisplacementinrelationtothe startingpointisnotcommon.Rotationshigherthan45◦are
consideredabnormal.Asymmetricallesionsofthevestibular
Table 2 Significance of the incidence of falls at the Rombergtestusingafoampadinrelationtotheabsenceof vestibular functioninoneearinsubjectswithasymmetric post-caloricfunction(Fisher’sexacttest).
Falls Nofalls Total
Asymmetricwithoutareflexia 0 7 7 Unilateralvestibularareflexia 3 0 3
Total 3 7 10
Fisher’stest,p=0.008.
systemresultin bodyrotationinthedirectionof theslow nystagmuscomponent---thehypofunctioninglabyrinth.
Testresults werequantifiedaspercentagesand associ-atedusingFisher’sexacttestandp-values≤0.05fora95% confidenceintervalwereconsideredstatisticallysignificant.
Results
Themeantimetakentoperformallthetestswas approx-imately 1h. Of the 21 patients, only 6 (28%) had normal resultsin all tests. Therefore,72% of the sample showed sometypeofalterationduringvestibularassessment.
Regardinginformationasymmetry,weidentified10(32%) subjectswiththepresenceofpost-calorictestasymmetry. Ofthese,2(20%)hadspontaneousnystagmus---onecasewas associatedwiththepresenceoflabyrinthinepredominance, whilethe other wasnot.Three subjectswithpost-caloric asymmetryshowed complete lack of response in oneear. Amongtheselastthree,twofellandshowedgreatinstability attheRombergtestusingafoampadandwitheyesclosed (p=0.008)(Table2).
Still considering the caloric test, 1 subject(4.5%) had bilateral hyporeflexia and 4 (18%) bilateral areflexia. All patients(100%)fell duringthe Romberg testusinga foam padwithclosedeyes.Fisher’sexacttest shows an associ-ationbetween the fallat Romberg test usinga foam pad withclosedeyesandareflexiaorseverevestibularfunction impairment(p=0.003)(Table3).
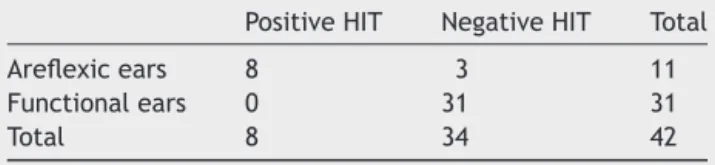
When individuallyanalyzing vestibularfunctionin each ear,thefoursubjectswhohadbilateralareflexia(8ears)and threewithunilateral arreflexia(three ears)at the caloric test,hadapositiveHITresultin6(54%)ears.HITwas consid-eredhighlysignificanttoidentifyareflexicears(p=0.0001) (Table4).
The HSNtest didnotshowanyabnormalresults inthe assessedpatients.
Table 3 Significance of the incidence of falls at the Rombergtestusingafoampadinrelationtothepresenceor absenceofresidualvestibularfunction(Fisher’sexacttest).
Falls Nofalls Total
Presentvestibularfunction 3 13 16 Absentvestibularfunction 5 0 5
Total 8 13 21
Table4 SignificanceofapositiveHeadImpulseTest(HIT) and absence of function (areflexia) of the assessed ears (Fisher’sexacttest).
PositiveHIT NegativeHIT Total
Areflexicears 8 3 11
Functionalears 0 31 31
Total 8 34 42
Fisher’stest,p=0.0001.
Discussion
Balance is a vital condition for the preservation of our species.Toadequatelyperceivetheenvironmentaroundus andtoreacttoposturalchallengesarenecessaryforbody safety.The structuraland functional integrityof the ves-tibular system is necessary for maintenanceof the entire complexpostural system, adaptationto theenvironment, andthefight-or-flightresponse.The absenceof vestibular functionisaccompaniedbypoorprognosisandsevere lim-itations in the activities of daily life, suchas ambulating inlow-lightenvironmentsoronunevenground,swimming, drivingfast,etc.Afrequentcomplaintisoscillopsiaduring headmovements,especiallyin thedark.13 The benefitsof
theCIareprovenanditspositiveimpactondeafpatients’ auditoryperceptionandqualityarenolongerdebated. How-ever,thesurgicalimplantprocedurerequirestheopeningof thelabyrinthandthereareriskswhenthevestibular func-tionispresent.Priorknowledgeofthevestibularcondition increasesthediagnosticindexandhelpsthemanagementof possiblepostoperativevestibularcomplications. Thereare twoquestionsthatshouldberaised whenweconsiderthe vestibularfunctionofapatientwhowillbesubmittedtoCI: (1)Isvestibularfunction present? (2)Isthe function sym-metric?To answer thesequestionswe developed asimple preoperativeassessmentthatdoesnotrequiresophisticated equipment.
The importanceof thepreoperative assessmentcanbe understoodwhen weobserveour results,whichidentified 72%ofthesamplewithsometypeofvestibularalteration. Incase of normalfunction,when oneearis implanted,it ispossibletoreversethedizzinesssymptom,evenifthere is complete loss of vestibular function on the operated side.Theadequateuseof neuroplasticitymechanismscan restorebodybalancethroughvestibularrehabilitation tech-niques.Thecasesthatoffergreaterriskofpermanentlesion arethosewithvestibularfunctionasymmetrybetweenthe ears.Adequatevestibularassessmentpreventsbilateral ves-tibular areflexia, as it provides data on the presence or absenceofvestibularfunctionandallowschoosingtheear thatofferslowersurgicalrisk.
We identified 10 (32%) subjects with post-caloric test asymmetry. In these cases, spontaneous nystagmus was presentin20%,indicatingthepresenceofvestibular func-tionasymmetryatthecalorictest.
Anotherimportanttesttodetectvestibulartone asym-metry is the HSN test. However, there is difficulty in observingthe head-shakingnystagmus, especiallybecause patientsfixtheirgazeontheexaminer’sfaceattheendof theprocedure.Itisaknownfactthatocularfixationinhibits
nystagmus of peripheral origin. None of our patients had apositive HSNtest, butwhetherthe nystagmusinhibition causedbyocularfixationwouldnothavepreventedthe visu-alizationofthefinalnystagmusisyettobeclarified.Theuse ofFrenzelglasses decreasesthebiasby preventingocular fixation.
Thepatientsevaluatedinthissamplewerenotsubmitted toFukudatest, subsequentlyaddedtothediagnostic rou-tine.Thetestisusefultoassessdeviationssecondarytotone asymmetry and it is routinely usedtoevaluate vestibular compensation during treatment. We decidedtoinclude it subsequentlytoobservetheassociationbetweenvestibular tone asymmetrydiagnosed byspontaneousnystagmusand post-caloricasymmetries--- importantforchoosingtheear tobeimplanted.Insuchcases,boththespontaneous nystag-musandtheFukudatestcontributeimportantinformation whensearchingforunilaterallesions.
Theworstpost-operativesituationisbilateralvestibular areflexia(BVA),asvestibularrehabilitationislimited,only improvingbalanceby50%inthesecases.2BVAcanbe
pre-vented when there is prior knowledge of the vestibular function of the earto be implanted. Classically, BVA can beeasilydiagnosedbyfallincondition5ofthe computer-izeddynamic posturography,whichsubjectstheindividual tooscillationoffootsupportwithclosedeyes.Condition5 canbeperfectlymimickedbytheRombergtestusingafoam pad.Inthissituation,withoutthevisionandwithconflicting proprioceptive information, the only determinant of pos-tureisthevestibularfunctionand,initsabsence,thefall occurs.14,15
Patientswithpost-caloricasymmetryduetoabsenceof vestibular responses on one side also showed a low per-formanceonthe Romberg testusinga foam pad:66% fell and33%showedsevereinstability.Statisticalanalysisofthe sampleshowsthattheRombergtestusingafoam padwas sensitivetodiagnoseseverevestibularfunctionimpairment (p=0.003).Ourdataareconsistentwiththeliteraturethat attributes79%ofsensitivityand80%ofspecificitytothetest whendetectingunilateralorbilateralarreflexia.16
Inthosepatientswhohadnovestibularresponsetothe caloric test, the HIT wasvaluable (p=0.0001). A positive test resultis highlysuggestive of failureof the vestibulo-ocular reflex,withtheadditionaladvantageofidentifying theaffectedside.7 Thediagnosis ofvestibularareflexiain
theeartobeimplantedmakesthesurgeonmoreconfident, asthereisnofunctiontobecompromised.Inbilateralcases, thereisnoriskofpostoperativedizziness.
Finally,itisimportanttorememberthattheknowledge of the vestibular function prior tothe surgery allows the physicianto assesswhat occurred duringsurgery.17 It will
bepossibletosaywhethertherewasalesioninthe oper-ated side or if a pre-existingsituation wasaggravated. A simple,six-stepevaluationbeforesurgeryoffersthe possi-bilityof identifyinglesionsand beingpreparedtomanage anyvestibularimpairments.
Conclusion
severeimpairmentofthevestibularfunction,confirmedby thecalorictest.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Ito J. Influence of the multichannel cochlear implant on vestibular function. Otolaryngol Head Neck Surg. 1998;118: 900---2.
2.Bittar RSM, Bottino MA, Pedalini MEB, Ramalho JRO, CarneiroCG.Arreflexia pós calórica bilateral:aplicabilidade clínica da reabilitac¸ão vestibular. Rev Bras Otorrinolaringol. 2004;70:188---93.
3.Vankatova L, Cao Van H, Perez Fornos A, Guinarnd N. Cochlearimplantation---bettersafethansorry.RevMedSuisse. 2014;10:1820---3.
4.JacotE,AbbeeleTVD,DebreHR,Wiener-VacherR.Vestibular impairmentspreand post-cochlearimplantinchildren.IntJ PedOtorhinolaryngol.2009;73:209---17.
5.MezzaliraR,BittarRSM,AlbertinoS.OtoneurologiaClínica.Rio deJaneiro:Revinter;2014.
6.BalohRW,HonrubiaV.Neurophysiologyofthevestibularsystem. NewYork:Oxford;2011.
7.HalmagyiGM,CurthoisIS.Aclinicalsignalofcanalparesis.Arch Neurol.1988;45:737---9.
8.GuidettiG,MonzaniD,CivieroN.Headshakingnystagmusinthe follow-upofpatientswithvestibulardiseases.ClinOtolaryngol. 2002;27:124---8.
9.KimMB,HuhSH,BanJH.Diversityofheadshakingnystagmus inperipheralvestibulardisease.OtolNeurotol.2012;33:634---9. 10.Rogers JH. Rombergand his test. JLaryngol Otol. 1980;94:
1401---4.
11.HongSK,ParkJH,KnonSY,KimJS,KooJW.Clinicalefficacyof theRombergtestusingafoampadtoidentifybalanceproblems: acomparativestudywiththesensoryorganizationtest.EurArch Otorhinolaryngol.2015;272:2741---7.
12.Fukuda T. Thestepping test: two phasesofthelabyrinthine reflex.ActaOtolaryngol.1959;50:95---108.
13.VibertD,LiardP,HäuslerR.Bilateralidiopathiclossof periph-eralvestibularfunctionwithnormalhearing.ActaOtolaryngol (Stockh).1995;115:611---5.
14.LanskaD,GoetzC.Romberg’ssign:development,adoption,and adaptationinthe19thcentury.Neurology.2000;55:1201---6. 15.Shumway-CookA, HorakF.Assessingtheinfluenceofsensory
interactionof balance.Suggestionfrom thefield.Phys Ther. 1986;66:1548---50.
16.FujimotoC,MurofushiT,ChiharaY,UshioM,SugasawaK, Yam-aguchi T, et al. Assessment of diagnostic accuracy of foam posturography forperipheral vestibulardisorders:analysisof parametersrelatedtovisual andsomatosensorydependence. ClinNeurophysiol.2009;120:1408---14.