SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Polypropylene
prosthesis
for
the
treatment
of
fingertip
injuries.
Description
of
surgical
technique
and
results
夽
Leandro
Azevedo
de
Figueiredo,
Rafael
de
Souza
Ribeiro,
Antonio
Leão
Bandeira
de
Melo,
André
Luiz
Lima,
Bernardo
Barcellos
Terra
∗,
Fernando
Carvalho
Ventim
SantaCasadeMisericórdiadeVitória,DepartamentodeOrtopediaeTraumatologia,Vitória,ES,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received18August2016 Accepted3October2016 Availableonline26October2017
Keywords:
Fingerphalanges Fingersinjuries Adults
a
b
s
t
r
a
c
t
Objective:Reporttheresultsoftreatmentoffingertipinjuriesanddescribethisreproducible andlowcostsurgicaltechnique,whichutilizesapolypropyleneprosthesisthattemporarily replacesthenailandisplacedontheareaofinjury,providingprotectionandencouragement forhealingbysecondaryintention.
Method:Thisstudyevaluated22patientswithtraumaticinjuriesofthefingertipsinthe periodfromJanuary2012toDecember2015.Allprocedureswereperformedbythesame surgeon.Themeanpostoperativefollow-upwas13months,withaminimumfollow-upof sixmonths.Forallstatisticalinferences,ap-valueof0.05wasconsidered.Thesoftwareused wasSPSSversion21.0forWindows.
Results:Therewerenocasesofcomplicationsrelatedtothepolypropylenedevice.There wasnosignificantdifferencebetweenstatictwo-pointdiscriminationandage,between discriminationandtimebetweeninjuryandsurgery,orbetweendiscriminationandtime tofollow-up.Theauthorsusedatableofscoresthatincludesthreefactorsproposedby Jeffersonforabetterevaluationoftheresults.72.7%(16cases)ofpatientshadgoodresults, 22.7%(fivecases)fairresults,andonly4.5%(onecase)poorresult.
Conclusion: Thisstudypresentedanewtechniqueforfingertiplesions,simpleandeasily reproducible,withsatisfactoryresultsandlowcomplicationrates.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheSantaCasadeMisericórdiadeVitória,DepartamentodeOrtopediaeTraumatologia,Vitória,ES,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](B.B.Terra). http://dx.doi.org/10.1016/j.rboe.2016.10.017
Uso
da
prótese
de
polipropileno
para
o
tratamento
das
lesões
em
ponta
de
dedo.
Descric¸ão
de
técnica
cirúrgica
e
resultados
Palavras-chave:
Falangesdosdedosdamão Traumatismosdosdedos Adulto
r
e
s
u
m
o
Objetivo:Relatarosresultadosdotratamentodaslesõesdepontadededo,bemcomo descr-everatécnicacirúrgica,reprodutíveledebaixocusto,queusaumaprótesedepolipropileno quesubstituitemporariamenteaunhaeécolocadasobreaáreadalesão,promoveprotec¸ão eestímuloparaasuacicatrizac¸ãoporsegundaintenc¸ão.
Método: Foramavaliados22pacientesportadoresdelesõestraumáticasdapolpadigital dejaneirode2012adezembrode2015.Todososprocedimentosforamfeitospelomesmo cirurgião.Otempomédiodeseguimentopós-operatóriofoide13meses,comum segui-mentomínimodeseismeses.Paratodaainferênciaestatística,considerou-seumvalorde pde0,05.OsoftwareusadofoioSPSSforWindows,versão21.0.
Resultados:Nãofoiobservadocasodecomplicac¸ãoreferenteaodispositivodepolipropileno. Nãofoiobservadadiferenc¸aestatísticasignificanteentresensibilidadeestáticaentredois pontos(DE2P)eidade,entresensibilidadeetempoentrelesãoedatadacirurgianementre sensibilidadeetempodeseguimento.Adotou-seumatabeladeescoresqueincluiutrês fatorespropostosporJeffersonparamelhoravaliac¸ãodosresultados;72,7%(16casos)dos pacientestiveramresultadosbons,22,7%(cinco)regulareseapenas4,5%(um)apresentou resultadoruim.
Conclusão: Opresenteestudoapresentouumanovatécnica,simplesefacilmente repro-dutível,paraaslesõesdaspontasdededoscomresultadossatisfatóriosebaixataxade complicac¸ões.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Injuriestothefingertips,definedasthedistalportionofthe fingerwheretheflexorandextensortendonsareinserted,are responsibleforoneofthemaincausesofemergencyroom visitsinpublicandprivatehospitals.1
Theseinjuries,whenuntreatedorpoorlymanaged,often leadtoirreparablesequelaeandlimitations,causingagreat losstotheeconomicallyactivepopulation,especiallywhen theyinvolvethethumband/orindexfinger.2
Intheliterature,numeroustechniqueshavebeendescribed forthetreatmentoffingertipinjuries,inordertomaintain maximumlength,withfunctionalcoverageandadequate sen-sitivity.Differentfactorsshouldbeconsideredwhenchoosing one surgical technique over another, especially the type of injury and factors related to the patient, surgeon, and institution.2–5However,manytechniquesarenotreproducible
elsewhere,duetotheircostandthepopulationstudied. Thisarticleisaimedatreportingtheresultsofthe treat-mentoffingertipinjuries,aswellastodescribeareproducible, low-costsurgicaltechniquethatusesapolypropylene pros-thesisthattemporarilyreplacesthenailandisplacedoverthe areaoftheinjury,byprotectingandstimulatingitshealingby secondintention.
Material
and
methods
Twenty-two patients with traumatic injuries of the digital pulpwerestudiedfromJanuary2012toDecember2015.All
procedureswereperformedbythesamesurgeon.Thestudy wasapprovedbytheEthicsCommitteeoftheinstitutionand thepatientssignedtheInformedConsentFormtoparticipate. Initially, a descriptive analysis of the studied variables wasperformed.Duetothenon-normalityofthedata, non-parametric tests were used for inferential analyses. The Mann–Whitney ortheKruskal–Wallis testwasusedforthe evaluationbetweenscoreandage,timebetweeninjuryand surgery,andfollow-uptime.Fortheanalysisbetween subjec-tiveevaluationandage,timebetweeninjuryandsurgery,and follow-uptime,theMann–Whitneytestwasused.Spearman’s correlationtestwasusedtoevaluatecorrelationbetween sen-sitivity andage,time frominjurytosurgery,and follow-up time.
The inclusion criteria were patients with acute trauma (compression,avulsion)inanyfingerofthehand.Exclusion criteriawereinfections;priorsurgeriesontheinjuredfinger; tumors;severeosteoarthritisofthejoint;systemicdiseases, suchas psoriasis, lupuserythematosus,Raynaud’s disease, irondeficiencyanemia,andhemochromatosis,andheartor lungdisease.
Patients’ age ranged from 16 to 67 years (mean of 40); 20 (90.9%) patients were male. The extent of pulpal loss was determined immediately after adequate debridement inall injuries;itwas measuredinsquarecentimeterswith the aid ofa sterile ruler. Table 1 presents the descriptive analysis of all the numerical variables contained in the database.
Table1–Descriptiveanalysisofnumericalvariables.
N Mean SD Median Min Max
Age(years) 22 40.27 14.7 39 16 67
2PD(mm) 22 2.86 0.68 3 2 4
Timefrominjurytosurgery(days) 22 5.38 7.17 2 0.5 28
Follow-up(months) 22 13.05 7.14 12 6 36
2PD,dynamicsensitivitybetweentwopoints.
andtheSemmes–Weinsteinmonofilamenttestingwereused tochecksensitivity.
Themean postoperativefollow-up time was 13 months (minimumofsixmonths).
Forallstatisticalinference,ap-valueof0.05wasconsidered significant.SPSS forWindowsversion 21.0wasusedforall analyses.
Description
of
the
technique
Adigitalblockadewithlidocainewasinitiallymade.Intrauma withinjuriestothenailbed,thebed wasrepairedwith6.0 absorbablesutureor7.0or8.0microsurgicalnonabsorbable suture;thebedwasthenprotectedwithapolypropylene pros-thesisobtainedthrough asmall portionofflexiblesilicone (polypropylene) cut away from a saline plastic bag, which
temporarily replacesthenail.Thismaterialiseasilyobtainable inoperatingrooms.
Afterthematerialwascutintheexactshapeoftheopen areaofthewound,itwasfixedunderthenailfoldandsutured atthehealthyedgesofthelesion.Forthat, aU-suturewas madewithagooddistancebetweentheentranceandexitsites ofthesuturetoavoidskinischemia.Thissamesuturecanbe usedtoattachtheplasticprosthesistothelateralnailfold. Simplesuturesaresufficienttoattachtheplastictotheentire skinborder,sothattheprosthesisisperfectlyaccommodated withoutpressingontothewound.
The dressing ismade withsterile gauze and micropore papertape. Thefirst dressing ischangedonlyafterfive or sevendays. During thisfirst periodoftime,liquid exudate forms,discretelymoisteningthedressing.Afterthefirstweek, thereisnomoreexudate,butratherfibrintissueformation thatwillbegraduallyreplacedbygranulationtissue,which willfilltheentirelostareaandrestoretheoriginalshapeof
Fig.2–Clinicalcase2:femalepatient,34yearsold.Traumabycrushingthemiddlefinger;(a)aspectofthedorsumofthe fingerwithcomplexnailbedlesion;(b)obliquevolarinjury(difficultflapuse);(c)plastictrimmedintoaU-shape;(d) intraoperativeaspect;(eandf):latepostoperativeaspect.Presenceofaviablenail.
thedigitalpulp.Thusitisobservedthatthegreaterthebone lossofthephalanx,thesmallerthefinallengthofthefinger. However,theshapeandappearanceoftheresidualsegment areveryclosetotheoriginal.Figs.1–3illustrateclinicalcases inwhichthedescribedtechniquewasused.
Afterthefirstweek,thedressingsarechangeddaily;only 70%alcoholisused, and thewoundiscoveredwithgauze andmicroporepapertape.Theprosthesisisremovedaftersix weeks.
Results
No complications were observed regarding the use of a polypropylenedeviceobtainedfromasalineplasticbag.
Thevariable timebetweeninjuryandsurgerypresented valueswithdifferentmeasurementunits,someindaysand othersinhours(<24h).Thus,inordertoanalyzethisvariable, itwasconvertedfrom<24hto12h.
Thescore table proposed byJefferson,6 which included
three factors (Table 2), was used for better evaluation of
the results. The following variables were considered: nail growth (0=no growth; 1=partial growth with plate arrest; and 2=normal growth),nail size(0≤50%;1=between 50% and75%;and2≥75%ofthesizeofthenailontheopposite side); andthe shapeofthenail (0=significant deformation in the verticalplane; 1=minor deformation inthe vertical
Table2–Estheticandfunctionalclassificationaccording tothesumoftheresults.
Nailgrowth 0=nogrowth;1=partialgrowthwith arrest;2=normalgrowth
Nailsize 0≤50%;1=between50%and75%; 2=75%ofthesizeofthenailonthe oppositeside
Nailshape 0=significantdeformityinthevertical plane;1=smalldeformityinthe verticalplane;2=nodeformity Totalscore6 Theresultswereobtainedbyadditing
Fig.3–Clinicalcase3:malepatient,38yearsold.Injurytotheradialborderofthethumb;(aandb)thumbwithextensive obliquelesionfromitsradialborder(difficultflapplanning);(candd)aspectofplasticcoveringlargeopenarea;(eandf): epithelizationaspect,oneweekafterremovaloftheplastic.Thethumbacquiresaroundedshape.
plane; and 2=no deformity), compared with the opposite side.Theresultswereobtainedbyaddingupthescores,and they were classified as good (5–6), regular (3–4), and poor (<3);72.7%(16cases)ofthepatientspresentedgoodresults, 22.7% (five) regular, and only 4.5% (one) presented a poor result.
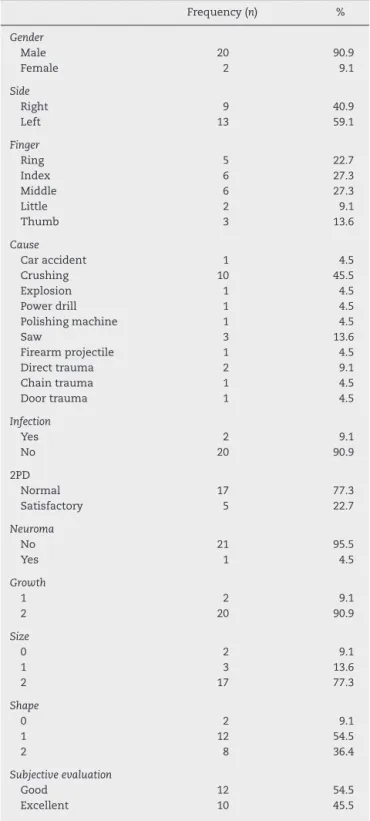
Table3presentsthedescriptiveinformationofthe quali-tative/categoricalvariables.
Table4presentstheresultsofinferentialanalysisbythe Kruskal–Wallismethod to assess whether therewas a dif-ference between scoreand age, time betweensurgery and injury, and follow-up time. No significant differences were observed between score and age, between score and time betweeninjuryandsurgery,norbetweenscoreandfollow-up time.Thevariablesage,timebetweeninjuryandsurgery,and follow-uptimedonotseemtohaveanyinfluenceonthescore obtained.
Table5presentsananalysisbetweenthesubjective eval-uation with age, time between surgery and injury, and follow-up time. No significant differences were observed between subjective evaluation and age, between subjec-tive evaluation and time between injury and surgery, nor betweensubjectiveevaluationandfollow-uptime.The vari-ablesage,timebetweeninjury,andsurgeryandfollow-uptime appearedtohavenoinfluenceonthesubjectiveevaluation result.
Table3–Descriptiveanalysisofqualitativevariables.
Frequency(n) %
Gender
Male 20 90.9
Female 2 9.1
Side
Right 9 40.9
Left 13 59.1
Finger
Ring 5 22.7
Index 6 27.3
Middle 6 27.3
Little 2 9.1
Thumb 3 13.6
Cause
Caraccident 1 4.5
Crushing 10 45.5
Explosion 1 4.5
Powerdrill 1 4.5
Polishingmachine 1 4.5
Saw 3 13.6
Firearmprojectile 1 4.5
Directtrauma 2 9.1
Chaintrauma 1 4.5
Doortrauma 1 4.5
Infection
Yes 2 9.1
No 20 90.9
2PD
Normal 17 77.3
Satisfactory 5 22.7
Neuroma
No 21 95.5
Yes 1 4.5
Growth
1 2 9.1
2 20 90.9
Size
0 2 9.1
1 3 13.6
2 17 77.3
Shape
0 2 9.1
1 12 54.5
2 8 36.4
Subjectiveevaluation
Good 12 54.5
Excellent 10 45.5
and follow-up time donotseem to haveany influenceon sensitivity.
Table7presentstheresultsbetweensensitivity(2PD)and age, time betweeninjury and surgery, and follow-up time. Nosignificant correlationwasobservedbetweensensitivity (2PD)andage,timebetweeninjuryandsurgeryand follow-uptime. Anegativecorrelationwas observedbetween2PD andtimebetweeninjuryandsurgery,i.e.,thehigherthe2PD value,the shorterthe time between injuryand surgeryor viceversa.
Discussion
Intraumaticfingertipinjuries,thenailmaybeavulsedor dam-agedinawaythatitspreservationisrenderedimpossiblein reconstructionprocedures.Inthesecases,atemporary substi-tutecanbeusedtoprotectthenailbedandthematrixuntila newnailgrows.Anidealreplacementshouldbesterile, inex-pensive,easilyaccessible,andsturdyenoughtoprotectthe fingertipfrompainfulstimuli.
Inrecentdecades,numerousdeviceshavebeenusedfor this purpose.7 A nail-shaped silicone blade was described
by Zook.8,9 However, due to the weakness ofthe blade, a
displacementofthefoldmayoccurifthesutureis improp-erlypositioned.Specificsplints(INROnailsplint)havebeen describedbyOgunro10forthetreatmentofnailinjuries,but
theircosthinderstheapplicabilityinothermedicalcenters. Simplersubstitutes,suchasaportionofanX-rayfilmorthe suture-kitenvelopeitself,havebeenused(Cohen,Dumontier). Other authors reported the use of silicone-based nasogas-trictubematerialsorplasticsyringes.5,7Thesematerialsare
readilyavailableandcanbemoldedintosplintsforthenail bed.However,thematerialofthenasogastrictubeisnotas resistantasacrylicormetal;itsdurabilityandabilityto pro-tectthenailbedagainstexternalforcesarealsolower.Inturn, metaloracrylicsplintscancauseadditionalinjuriesdueto theirrigidity.Inthepresentstudy,apolypropyleneprosthesis wasused;ithadfeaturesthatprotectedthenailbedagainst painfulstimuliandexternalforces,andatthesametimewas notsorigidastocauseresidualdeformities.
Transverseinjuriesofthedistalthirdofthedistalphalanx are usuallytreatedwithKutlerorAtasoyV-Yadvancement flaps.6,11,12Thegreatchallengeisvolarobliqueinjuries,which
affectalargeextensionofthedigitalpulpand,unlike trans-verse injuries, do not allow local skin advance. For more complexcases,countlessflaptechniqueshavebeendescribed in the literature; however, there is no consensus on what would bethe bestforeach typeofinjury. Theseflap tech-niquesaretechnicallydifficult,andrequirespecificskillsand training.Furthermore,alltechniquesrequireadonorareaof cutaneoustissue,whichmaycomefromanontraumatized regionoftheinjuredfingeroranotherlessimportantfinger, asintherenownedLittler’sflap.4Otherareasofthehand,both
volaranddorsal,mayalsofunctionasdonorsforpedicledor randomflaps.Microsurgicalflapshavealsobeenmentioned intheliterature,andrequireevenmoreskillandtrainingby thespecialist;moreover,theyarepoorlyreproduciblebymost surgeons.Thetechniquedescribedinthepresentstudyis indi-catedtocoverdifferenttypesoffingertipinjuries,engagingor notthenailbed.
Table4–Analysisbetweenscoreandage,timebetweeninjuryandsurgery,andfollow-uptime.
Score p-Value
≤3 4 5 6
M(±SD) M(±SD) M(±SD) M(±SD)
Age(years) 58.5(±9.19) 28.5(±3.82) 40.2(±14.0) 41.8(±14.2) 0.1
Timefrominjurytosurgery(days) 10.7(±14.42) 3.5(±3.71) 6.0(±9.00) 4.0(±3.78) 0.97
Follow-up(months) 6.5(±0.7) 19.4(±11.3) 12.4(±5.51) 12.0(±5.38) 0.16
Kruskal–Wallistest.
Table5–Analysisbetweensubjectiveevaluationandage,timebetweeninjuryandsurgery,andfollow-uptime.
Evaluation Subjective p-Value
Good Excellent
M(±SD) M(±SD)
Age(years) 44.8(±13.4) 34.4(±13.4) 0.09
Timefrominjurytosurgery(days) 4.2(±7.6) 6.7(±6.6) 0.22
Follow-up(months) 13.4(±5.5) 12.6(±9.0) 0.49
Mann–Whitneytest.
Table6–Analysisbetweensensitivityandage,timebetweeninjuryandsurgery,andfollow-uptime.
Sensitivity p-Value
Normal Satisfactory
M(±SD) M(±SD)
Age(years) 41.88(±13.4) 34.81(±16.3) 0.35
Timefrominjurytosurgery(days) 6.35(±9.92) 2.00(±1.0) 0.64
Follow-up(months) 12.24(±7.7) 15.8(±3.4) 0.12
Mann–Whitneytest.
Table7–Correlationbetweensensitivityandage,time betweeninjuryandsurgery,andfollow-uptime.
r p-Value
2PDvs.age 0.23 0.98
2PDvs.timebetweeninjuryandsurgery −0.006 0.3
2PDvs.follow-uptime 0.21 0.32
r,Spearman’scorrelationcoefficient.
whethertransverseoroblique.Duringthe45daysofuseof theprosthesis,thebodyappearstoreacttothepresenceof polypropylene,producinggranulationtissueinanaccelerated andcoordinatedway,quicklyre-establishingtheanatomical shapeofthefinger.Moreover,theprosthesisprotectstheopen areaofthelesionandavoidsadherenceofthedressingand bleedingduringthe changeofdressings.Theauthors have evenobservedthereturnofthefingerprintontheremaining digitalsegment.
Infections are well-described complications after finger surgery, especially in contaminated lesions or those asso-ciated with compound fractures.2 The risk of infection
increases by 13% in contaminated wounds and 40% in thoseseverelycontaminated.Themostfrequentlyobserved infectiousagentsareStaphylococcusaureus,Streptococcus,and pseudomonas.2 In the present study, no cases of
infec-tionwereobserved.Theauthorsbelievethisfactmay have
improvedpatients’satisfactionregardingestheticappearance orresidualfingerdeformity.
Conclusion
Thepresentstudypresentedanew,simple,andeasily repro-ducible technique for fingertip injuries, with satisfactory resultsandalowrateofcomplications.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BrownRE.Acutenailbedinjuries.HandClin. 2002;18(4):561–75.
2.MangramAJ.Abriefoverviewofthe1999CDCguidelinefor thepreventionofsurgicalsiteinfection,CentersforDisease ControlandPrevention.JChemother.2001;13(1):35–9. 3.OetgenME,DoddsSD.Non-operativetreatmentofcommon
5. BayraktarA,OzcanM.Anasogastriccathetersplintfora nailbed.AnnPlastSurg.2006;57(1):120.
6. SilvaJB,GerhardtS.Traumatothenailcomplex.RevBras Ortop.2014;49(2):111–5.
7. EtözA,KahramanA,OzgenelY.Nailbedsecuredwitha syringesplint.PlastReconstrSurg.2004;114(6): 1682–3.
8. ZookEG.Understandingtheperionychium.JHandTher. 2000;13(4):269–75.
9.ZookEG.Theperionychium:anatomy,physiology,andcareof injuries.ClinPlastSurg.1981;8(1):21–31.
10.OgunroEO.ExternalfixationofinjurednailbedwiththeINRO surgicalnailsplint.JHandSurgAm.1989;142Pt1:
236–41.
11.HendersonJ.Shiny-sidedownisbestforfoilsplintsafter nailbedrepairs.JPlastReconstrAesthetSurg.2009;62(4):479. 12.ZookEG.Anatomyandphysiologyoftheperionychium.Hand