SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
What
is
the
best
fixation
technique
for
the
treatment
of
supracondylar
humerus
fractures
in
children?
夽
Gyoguevara
Sol
Queiroz
Andrade
Patriota
a,∗,
Carlos
Alberto
Assunc¸ão
Filho
b,
Carlos
Alberto
Assunc¸ão
baHospitalManoelVictorino,Servic¸odeOrtopediaeTraumatologia,Salvador,BA,Brazil
bHospitalRegionaldeSantoAntoniodeJesus,Servic¸odeOrtopediaeTraumatologia,SantoAntôniodeJesus,BA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received31May2016 Accepted5August2016 Availableonline7June2017
Keywords:
Humeralfractures Fractureinternalfixation Child
Bonewires
a
b
s
t
r
a
c
t
Objective:Todefinethebesttechniqueforthesurgicaltreatmentofsupracondylarfracture ofthehumerus(SFH)inchildren,evaluatingpercutaneouspinningwithsidewiresvs. cross-pinning.
Methods:RandomizedcontrolledtrialsusingtheMedline,CAPES,andBIREME.Thecriteria forinclusionofarticlescriteriawere:(1)randomizedcontrolledtrials(RCTs)comparing percutaneouswirefixationtechniques,(2)SFHGartlandIIB,III,andIV,and(3)children aged1–14years.Thefollowingwereusedasmainvariables:incidenceofiatrogenicinjury totheulnarnerveandlossreduction.
Results:Eightstudieswereselected(521patients)comparingsurgicaltreatmentwith pin-ningin supracondylarfracture ofthehumerusinchildrenGartlandII typeB,IIIor IV. Iatrogenicinjurytotheulnarnervewasgreaterwiththecross-pinningtechnique,withRR 0.28andp=0.03,whilethemini-opentechniquepresentedRR0.14andp=0.2.Astatistically significantgreaterlossofreductioninthelateralpinningwasobservedinFSUGartlandIII andIV(p=0.04).
Conclusion:Basedupon thismeta-analysisofprospectiverandomized clinicaltrials, the followingisrecommended:(1)percutaneouspinningwithlateralwiresinsupracondylar fracturesofthehumerusinchildrenclassifiedasGartlandIItypeB;(2)useofcrossedwires forGartlandtypeIIIorIV,usingthemini-opentechniqueforthemedialwire.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatHospitalManoelVictorinoandHospitalRegionaldeSantoAntoniodeJesus,Salvador,BA,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](G.S.Patriota).
http://dx.doi.org/10.1016/j.rboe.2017.05.013
Qual
a
melhor
técnica
para
fixac¸ão
no
tratamento
de
fratura
supracondilar
do
úmero
em
crianc¸as?
Palavras-chave:
Fraturasdoúmero Fixac¸ãointernadefraturas Crianc¸as
Fiosortopédicos
r
e
s
u
m
o
Objetivo: Definiramelhortécnicaparaotratamentocirúrgicodafraturasupracondilardo úmero(FSU)nascrianc¸aseavaliarapinagempercutâneacomfioslateraisvs.cruzados.
Métodos: RevisãodeensaiosclínicosrandomizadosnasbasesdedadosMedline,Capes, Bireme.Oscritériosdeinclusãodosartigosforam:(1)Ensaiosclínicosrandomizadosque comparamtécnicasdefixac¸ãopercutâneacomfios,(2)FSUGartlandII tipoB,IIIeIVe (3) Crianc¸ascomuma 14anos. Usamoscomoprincipaisvariáveis:incidênciadelesão iatrogênicadonervoulnareperdadareduc¸ão.
Resultados: Foramselecionadosoitoestudos(521pacientes)quecomparamtratamento cirúrgicocompinagememfraturasupracondilardoúmeroemcrianc¸asclassificadascomo GartlandIItipoB,IIIouIV.Alesão iatrogênicadonervoulnarfoimaiorcomatécnica depinagemcruzada,apresentouRR0,28ep=0,03,enquantoquenatécnicademini-open
encontraram-seRR0,14ep=0,2.EmcasosdeFSUGartlandIIIeIV,evidenciou-semaior perdadareduc¸ãonapinagemlateral,comsignificânciaestatística(p=0,04).
Conclusão: Embasadoemnossametanálisecomensaiosclínicosrandomizados prospec-tivos,recomendamos:(1)pinagempercutâneacomfioslateraisemfraturassupracondilar doúmeroemcrianc¸asclassificadascomoGartlandIItipoB(2)Usodefioscruzadospara fraturasGartlandtipoIIIouIV,comatécnicademini-openparaofiomedial.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Supracondylarfractureofthehumerus(SFH)isfrequentinthe immatureskeleton.1 Thereispredominanceintheleftside orthenon-dominantside,2andfracturesinelbowextension withposteriordeviationrepresent97%ofcases.2,3
Themostwidelyusedclassificationisthatdescribed by Gartland,4whichwasproposedforfractureswithelbow exten-sionmechanismandbasedondeviationsinthecoronalplane inelbowradiographs.TypeI:undisplacedorminimally dis-placed,withtheanteriorhumerallineintact.TypeII:small deviation,fragmentsincontact(intactposteriorcortex),Type III:completedisplacementofthefragments(posteriorcortex injury).In1996,WilkinsproposedtheB-typesubdivisionfor SFHinchildrenwithrotationaldeviation.5–7 In2006,Leitch etal.8addedtypeIV,whichdescribesmultidirectional insta-bility.
SurgicaltreatmentisindicatedintypesIIB,III,andIV frac-tures.Closedreductionandpinningstabilizationisthemost commonlyusedtechnique.9,10Fixationcanbeperformedwith crossedpins8 orlateral pins.4 Amini-opentechniqueisan optionformedialpassage.11Themostcommoncomplication iscubitusvarus(3–57%ofcases),11andismainlyduetopoor reductionorlossofreductionduringtreatment.Themost fre-quentiatrogenicnerveinjuryisthatoftheulnarnerve,with anincidenceof0–6%.12
This study aimed to define the best technique recom-mendedbythecontemporaryliteratureforsurgicaltreatment ofsupracondylarfractureofthehumerusinchildrenandto evaluatepercutaneouspinningwithlateralwiresvs.crossed wires.
Materials
and
methods
A systematicreview ofrandomized clinical trials was per-formed through literature search of PubMed, CAPES, and BIREMEdatabases.Theterms“supracondylarfractures,” “per-cutaneousfixation,”“k-wire,”“children,”“crosspinning,”and “lateralpinningfixation”wereusedindifferentcombinations. Adirectsearchofstudieslistedinthereferencesofthe arti-clesretrievedwasalsoperformed.Therewasnorestriction regardinglanguageofpublication.Titlesandabstractsof stud-iesretrievedintheelectronicsearchwereevaluated,andfull textsofselectedarticleswereobtained.
Inclusion criteria were: (1) randomized controlled trials (RCTs) comparing percutaneous fixation techniques using wires,(2)SFHGartlandIItypesB,III,andIV,and(3)children aged1–14years.Exclusioncriteriawere:repeatedstudyor sur-gical techniquedifferentfromthatadvocatedinthisstudy. Thetwoauthors(GSQAPandCAAF)independentlyassessed themethodologicalqualityofincludedstudiesusingthe Det-skyQualityIndexscore(maximumof21points).13
Main variables considered were incidence of iatrogenic injuryoftheulnarnerveandlossofreduction.Recommended secondaryfindingswereradiographicresults(Baumannangle, loadingangle,humero-capitellarangle,Baumannangle varia-tion,lossofloadingangle).Lossofreductionwasdetermined based on Baumannangle change according to the criteria reportedbySkaggsetal.14:(1)nodisplacement(losssmaller than6◦),(2)moderatedisplacement(6◦–12◦),and(3)large dis-placement(largerthan12◦).
Clinical trials (CT) (n=85)
Potential CTs (n=32) CT Included – title/abstract
(n=50)
Randomized CT3,4,5,6,7,8,9,10 (n=8)/521 Patients
Excluded (n=35): Non-randomized CT
Excluded (n=18): Duplication
Excluded (n=24) Surgical technique (n=7) Repeated publication (n=5) Compared pins vs. different technique (n=3)
Compared open vs. closed (n=5) Patient triage (n=4)
Identification
Rastreio
Elegibilidade
Included
Fig.1–Studydesign.
chi-squaredtest(I2),consideredstatisticallysignificantwith
p>0.05,and aI2 greater than 50% were considered signifi-cantheterogeneity.Forgroupsthatpresentedheterogeneity, randomeffectswereappliedtoselecteddata.
Relativerisks(RR)andriskdifferenceswerecalculatedfor dichotomousoutcomes.Forcontinuousoutcomes,mean dif-ferencesand95%confidenceintervals(CI)werecalculated.
Results
Initially, 85 clinical trials comparing percutaneous pinning inSFHinchildrenwereretrieved.Ofthesestudies,35were excluded for not being randomized. Of the 50 RCTs, 42 wereexcludedforduplicationand/orsurgicaltechniqueused.
Finally,thisstudyincludedeightprospectiveRCTs,comprising 521patients(Fig.1).Regardingassessmentofmethodological quality,theDetskyQualityIndexscorerangedfrom13to20 points(averageof15.7).15–22
Iatrogeniculnar nerveinjuryinthetreatmentofSFHin children wasmorecommonly observedinpatients treated withcross-pinningwhencomparedwithlateral-onlypinning (RR 0.28;95%CI 0.09–0.87;p=0.03).Heterogeneitywas non-significant,withI2=0%.AmongtheeightRCTsincludedinthe study,12patients(4.46%)presentediatrogenicinjuryofthe ulnarnerveinthecross-pinninggroup,vs.onlytwopatients intheothergroup(0.78%;Fig.2).
When RCTs that used mini-open technique for cross-pinningwereanalyzed,nostatisticallysignificantdifferences were observed(RR0.14;95% CI0.01–2.79;p=0.20)regarding
Study or subgroup
Laterais Cruzados
Weight Total
Odds ratio Odds ratio
M-H, Fixed,95% CI M-H, Fixed,95% CI
Events Total
Total (95% CI) 252 269 1.00.0% 0.28 [0.09, 0.87]
Total events
Heterogeneity: Chi2 = 0.34, df = 4 (p = 0.99);I2 = 0%
Test for overall effect: Z = 2.20 (p = 0.03)
Events
Anwar 2011 Foead 2004 Gaston 2010 Kocher 2007 Maity 2012 Mazda 2001 Tripuraneni 2009 Vaidya. 2009
2 0 0 0 0 0 0 2 0
29 20 0 80 24 47 27 25
31 25.5% 11.2% 11.3% 34.8% 17.2%
20 0 80 28 57 28
25 0.32 [0.01, 8.25] 0.37 [0.06, 2.09] 0.23 [0.01, 4.99]
0.32 [0.01, 8.26] 0.14 [0.01, 2.79] Not estimable Not estimable Not estimable
3
0.1 1 10 200 0.005
Favours [experimental] Favours [control]
1 0 0 0 2 5 1
12
Study or subgroup
Laterais Cruzados
Weight Total
Odds ratio Odds ratio M-H, Fixed,95% CI M-H, Fixed,95% CI
Events Total Events
0.1 1 10 100
0.01
Favours [experimental] Favours [control] Total (95% CI)
Total events
Heterogeneity: Not applicable Test for overall effect: Z = 1.29 (p = 0.20) Kocher 2007
Maity 2012 Vaidya 2009
0 0 0
0
0 0 3
3 31
135
137 1.00.0%
1.00.0% 28
80 80 29
24
0.14 [0.01, 2.79]
0.14 [0.01, 2.79]
Not estimable Not estimable
Fig.3–Comparativeanalysistoassessiatrogenicinjuryoftheulnarnervein272patientswhounderwentpercutaneous pinningwithexclusivelylateralorcrossedKirschnerwires(withmini-opentechniqueformedialaccess)forthetreatment ofsupracondylarhumeralfracture.
Study or subgroup
Laterais Cruzados
Weight Total
Risk ratio Risk ratio
M-H, Fixed,95% CI M-H, Fixed,95% CI
Events Total Events
0.1 1 10 100 0.01
Favours [experimental] Favours [control] Total (95% CI)
Total events Gaston 2010 Kocher 2007 Maity 2012
Mazda 2011 Vaidya. 2009
Test for overall effect: Z = 0.94 (p = 0.35) 32 26
202
202 1.00.0% 1.26 [0.78, 2.02]
3.21 [0.35, 29.11] 0.49 [0.13, 1.85] 0.86 [0.35, 2.10] 5.14 [0.66, 39.77] 1.46 [0.69, 3.07]
Heterogeneity: Chi2 = 5.29, df = 4 (p = 0.26);I2 = 24%
3 3 8 12 6
29 32 66 28 47
1 5 9 1
31 26 64 24 10 57
3.8% 21.4% 35.5% 4.2% 35.1%
Fig.4–Comparativeanalysistoassesslossofreductionamong404patientswhounderwentpercutaneouspinningwith exclusivelylateralorcrossedKirschnerwiresfortreatingsupracondylarhumeralfractureinchildren.
Study or subgroup
Laterais Cruzados
WeightM-H, Fixed,95% CI Total
Risk ratio Risk ratio
M-H, Fixed,95% CI Events
Total Events
Total (95% CI) 104 112 1.00.0% 1.97 [1.02, 3.81]
Total events
Heterogeneity: Chi2 = 1.66, df = 2 (p = 0.44);I2 = 0%
Test for overall effect: Z = 2.00 (p = 0.04) Gaston 2010
Kocher 2007
Maity 2012
Mazda 2001
Vaidya. 2009
21 3 3 8 6 12
29 32 66 28 47
31 8.7% 81.6%
9.7%
0.0%
0.0% 26 64 24
57 1.46 [0.69, 3.07]
5.14 [0.66, 39.77]
0.86 [0.35, 2.10]
0.49 [0.13, 1.85]
3.21 [0.35, 29.11] 1
0.1 1 10 100 0.01
Favours [experimental] Favours [control]
5 9 1 10
12
Kocher 2007 Maity 2012 Tripuraneni 2009
Study or subgroup
Laterais Cruzados
Total
Mean difference
SD
Mean Mean SD TotalWeight IV, Fixed, 95%CI
Mean difference
IV, Fixed, 95%CI
Total (95% CI) 114
76.2 70.7 73.7 3.51 6.3 8.4 66 20 28 77.2 70.7 75.8 80.7% 11.3% 8.0% 67 20 24 4.35 5.2 7.3
111 –0.97 [–2.18, .23]
–0.00 [–3.58, 3.58] –1.00 [–2.34, 0.34] –2.10 [–6.37, 2.17]
1.00.0%
Heterogeneity: Chi2 = 0.55, df = 2 (p = 0.76);I2 = 0% Test for overall effect: Z = 1.58 (p = 0.11)
–5 0 5 10 –10
Favours [experimental] Favours [control]
Fig.6–Baumannangle.
Study or subgroup
Laterais Cruzados
Total
Mean difference
SD
Mean Mean SD TotalWeight IV, Fixed, 95%CI
Mean difference
IV, Fixed, 95%CI
Total (95% CI) 222
5.3 3.7 5.16 5 4.5 2.64 27 47 25 5.96 2.9 5.56 3.9% 12.0% 19.7% 28 57 25 5.6 3.7 1.8
229 0.07[–0.48, 0.63]
0.80 [–.81, 2.41] –0.66 [–3.46, 2.14] –0.40 [–1.65, 0.85]
3.71 5.3 5.8 2.1 5 3.5 66 29 28 3.57 5.96 5.4 50.5% 4.3% 9.6% 64 31 24 2.43 5.6 3.1
–0.66 [–3.34, 2.02] 0.14 [–0.64, 0.92] 0.40 [–1.39, 2.19]
1.00.0%
Heterogeneity: Chi2 = 2.04, df = 5 (p = 0.84);I2 = 0% Test for overall effect: Z = 0.25 (p = 0.80) Anwar 2011 Foead 2004 Gaston 2010 Kocher 2007 Maity 2012 Vaidya. 2009
–2 0 2 4 –4
Favours [experimental] Favours [control]
Fig.7–VariationofBaumannangle.
ulnar nerve injury when compared with lateral pinning (Fig.3).
Patients submittedto lateral percutaneous pinning pre-sented greater loss of reduction (32 cases; 15.84%) when compared with those who underwent cross-pinning (26 cases;12.87%);thedifferencewasnotstatisticallysignificant (p=0.35;Fig.4).
WhenanalyzingpatientswithSFHGartlandIIIandIV,a statisticallysignificant(p=0.04)greaterlossofreductionwas observedinpatientssubmittedtolateralpinning(21cases– 20.19%).Lossofreductionwasobservedin12patients(10.71%) inthecross-pinninggroup(Fig.5).
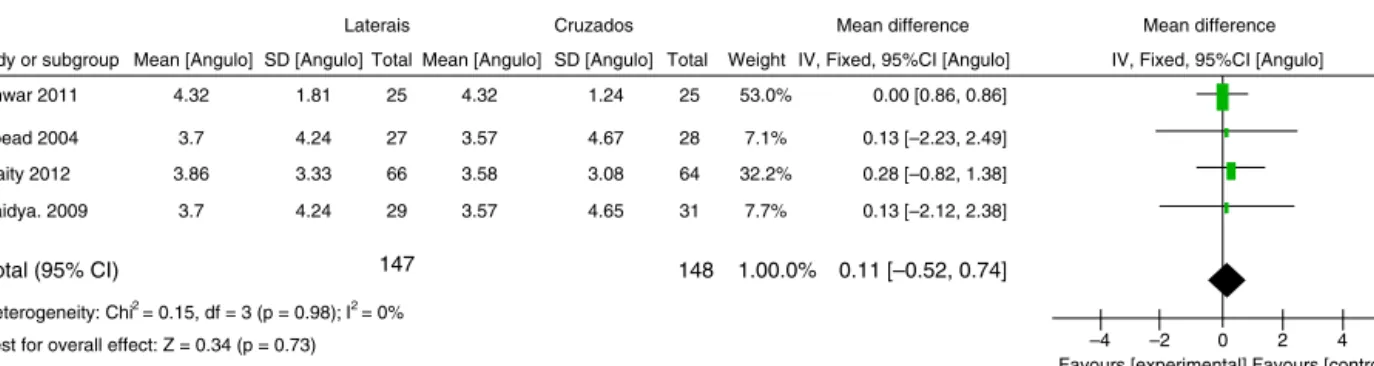
No statistically significant difference was observed betweenthetwotechniquesregardingtheBaumannangle, Baumann angle variation, loading angle, loading angle
variation, humero-capitellar angle, and humero-capitellar anglevariation(Figs.6–9).
Discussion
Iatrogenicinjuryoftheulnarnerveisanimportantfactorto beanalyzedwhentreatingSFHusingpercutaneouspinning withKirschnerwiresinchildren.Theincidenceofulnarnerve injuryobservedinthepresentstudy(4.46%)isinagreement withtheresultspreviouslyfoundintheliterature.15–22Babal etal.23concludedthatmedialpinningistheleadingcauseof iatrogeniculnarnerveinjury.Braueretal.24demonstratedthat useofmedialpinincreasedtheincidenceofneurologicinjury by1.84times.
–1 0 1 2 –2
Favours [experimental] Favours [control] Study or subgroup
Laterais Cruzados Total
Mean difference SD
Mean Mean SD Total Weight IV, Fixed, 95%CI
Mean difference IV, Fixed, 95%CI
Kocher 2007 Maity 2012
Total (95% CI) 94
5.56 7.3 4.62 1.7 66 28 5.52 7.2 31.7% 68.3% 64 24 3.77 1.9
88 0.08 [–0.73, 0.90]
0.04 [–1.41, 1.49] 0.10 [–0.89, 1.09]
1.00.0%
Heterogeneity: Chi2 = 0.00, df = 1 (p = 0.95); I2 = 0%
Test for overall effect: Z = 0.19 (p = 0.85)
Study or subgroup
Laterais Cruzados Total
Mean difference SD [Angulo]
Mean [Angulo] Mean [Angulo] SD [Angulo] Total Weight IV, Fixed, 95%CI [Angulo]
Mean difference IV, Fixed, 95%CI [Angulo] Anwar 2011
Foead 2004 Maity 2012 Vaidya. 2009
Total (95% CI) 147 148 1.00.0% 0.11 [–0.52, 0.74]
Heterogeneity: Chi2 = 0.15, df = 3 (p = 0.98); I2 = 0% Test for overall effect: Z = 0.34 (p = 0.73)
3.86 3.7 4.32
3.33 4.24
1.81 53.0%
7.1% 32.2% 3.58
3.57
4.32 0.00 [0.86, 0.86]
0.13 [–2.23, 2.49] 0.28 [–0.82, 1.38] 66
3.7 4.24 3.57 7.7% 3.08
4.67 1.24
4.65 64 28 25
31 0.13 [–2.12, 2.38] 29
27 25
–2 0 2 4 –4
Favours [experimental] Favours [control]
Fig.9– Variationofloadingangle.
Inthismeta-analysis,astatisticallysignificantdifference wasobservedintheincidenceofiatrogenicinjuryoftheulnar nervewhencomparingtechniquesoflateralpinsvs.crossed pins(p=0.03),whichconfirmedtherelationshipofiatrogenic injuryoftheulnar nervewiththe passageofamedialpin. Neuralrecoveryusuallyoccursafter2–2.5monthsof observa-tion,butitcantakeupto6months.11Inthestudiesincludedin thisreview,allpatientsrecoveredfromtheneurologicaldeficit duringfollow-up.
Previousstudieshaveshownthatmini-opentechniquefor medialpinpresentsalowincidenceofulnarnerveinjury.11In thisstudy,nostatisticallysignificantdifferencewasobserved intheanalysisofulnarnerveinjurywhenusingmedialpin withmini-opentechnique.
Regarding loss ofreduction, the literaturestill presents inconsistent results.18,23,24 In a retrospective study of 345 children with SFH, Skaggs et al.25 observed no difference inrelationship tomaintenanceoffracture reductionwhen comparingbothsurgicaltechniques.Inaclinicaland biome-chanical study, Omid et al.26 found similar stability using divergent,spacedlateralwireswhencomparedwith cross-pinning. In a systematic review, Brauer et al.24 observed residualdeformity(secondarytolossofreduction)in3.4%of patientstreatedwithcross-pinningandin5.9%ofpatients treatedonlywithlateralpin,astatisticallysignificantresult. They concluded that cross-pinning provides greater sta-bility in the wire configuration (they should cross above fracture) and that the probability of deformity or loss of reductionwas58% lower whencomparedwithlateral pin-ning.
Thepresent meta-analysisdidnot finda statistical sig-nificantdifferenceforlossofreductionwhenevaluatingthe totalityofpatients involvedin thestudies included. When groupswithfracturestypeIIIorIVofGartlandwereassessed, incidenceoflossofreductionwasapproximately10%higher inthegroupwithlateralwires,astatisticallysignificant dif-ference(p=0.04).
Conclusion
Based on this meta-analysis with prospective randomized clinicaltrials,theauthorsrecommend:(1)percutaneous pin-ningwithlateralwiresforSFHinchildrenwithGartlandIItype Bfractures;(2)crossedwiresinGartlandtypeIIIorIVfractures, withamini-opentechniqueforthemedialwire.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.DavisRT,GorczycaJT,PughK.Supracondylarhumerus fracturesinchildren.Comparisonofoperativetreatment methods.ClinOrthopRelatRes.2000;(376):49–55.
2.WilkinsKE.Fracturesanddislocationsoftheelbowregion.In: RockwoodCA,KingRE,WilkinsKE,editors.Fracturesin children.3rded.NewYork:JBLippincott;1991.p.526–617.
3.ChengJC,LamTP,MaffulliN.Epidemiologicalfeaturesof supracondylarfracturesofthehumerusinChinesechildren.J PediatrOrthopB.2001;10(1):63–7.
4.GartlandJJ.Managementofsupracondylarfracturesofthe humerusinchildren.SurgGynecolObstet.1959;109(2):145–54.
5.WilkinsKE.Fracturesanddislocationsoftheelbowregion.In: RockwoodCAJr,WilkinsKE,KingRE,editors.Fracturesin children.4thed.Philadelphia:Lippincott–RavenPublishers; 1996.p.680.
6.O’HaraLJ,BarlowJW,ClarkeNM.Displacedsupracondylar fracturesofthehumerusinchildren.Auditchangespractice. JBoneJtSurgBr.2000;82(2):204–10.
7.SkaggsDL,MirzayanR.Theposteriorfatpadsignin associationwithoccultfractureoftheelbowinchildren.J BoneJtSurgAm.1999;81(10):1429–33.
8.LeitchKK,KayRM,FeminoJD,ToloVT,StorerSK,SkaggsDL. Treatmentofmultidirectionallyunstablesupracondylar humeralfracturesinchildren.AmodifiedGartlandtype-IV fracture.JBoneJtSurgAm.2006;88(5):980–5.
9.ButurovicS.Komparacijarezultatalijeèenjapreloma distralnoghumerusakoddjecepremaindikacijiza konzervativnoilioperativnorjeˇsenje:doktorskadisertacija. Sarajevo:UniverzitetuSarajevu,Medicinskifakultet;2006.
10.Madjar-SimicI,Talic-TanovicA,HadziahmetovicZ, Sarac-HadzihalilovicA.Radiographicassessmentinthe treatmentofsupracondylarhumerusfracturesinchildren. ActaInformMed.2012;20(3):154–9.
11.GreenDW,WidmannRF,FrankJS,GardnerMJ.Lowincidence ofulnarnerveinjurywithcrossedpinplacementforpediatric supracondylarhumerusfracturesusingamini-open
technique.JOrthopTrauma.2005;19:158–63.
12.Krusche-MandlI,AldrianS,KöttstorferJ,SeisA,Thalhammer G,EgkherA.Crossedpinninginpaediatricsupracondylar humerusfractures:aretrospectivecohortanalysis.Int Orthop.2012;36(9):1893–8.
randomizedtrialsintometa-analysis.JClinEpidemiol. 1992;45(3):255–65.
14.SkaggsDL,CluckMW,MostofiA,FlynnJM,KayRM. Lateral-entrypinfixationinthemanagementof supracondylarfracturesinchildren.JBoneJtSurgAm. 2004;86(4):702–7.
15.AnwarW,RahmanN,IqbalMJ,KhanMA.Comparisonoftwo methodsofpercutaneousK-wirefixationindisplaced supracondylarfractureofhumerusinchildren.JPostgrad MedInst.2011;25:356–61.
16.FoeadA,PenafortR,SawA,SenguptaS.Comparisonoftwo methodsofpercutaneouspinfixationindisplaced
supracondylarfracturesofthehumerusinchildren.JOrthop Surg(HongKong).2004;12(1):76–82.
17.GastonRG,CatesTB,DevitoD,SchmitzM,SchraderT,Busch M,etal.Medialandlateralpinversuslateral-entrypin fixationforType3supracondylarfracturesinchildren:a prospective,surgeon-randomizedstudy.JPediatrOrthop. 2010;30(8):799–806.
18.KocherMS,KasserJR,WatersPM,BaeD,SnyderBD,Hresko MT,etal.Lateralentrycomparedwithmedialandlateral entrypinfixationforcompletelydisplacedsupracondylar humeralfracturesinchildren.Arandomizedclinicaltrial.J BoneJtSurgAm.2007;89(4):706–12.
19.MaityA,SahaD,RoyDS.Aprospectiverandomised, controlledclinicaltrialcomparingmedialandlateralentry pinningwithlateralentrypinningforpercutaneousfixation ofdisplacedextensiontypesupracondylarfracturesofthe humerusinchildren.JOrthopSurgRes.2012;7:6.
20.TripuraneniKR,BoschPP,SchwendRM,YasteJJ.Prospective, surgeon-randomizedevaluationofcrossedpinsversuslateral pinsforunstablesupracondylarhumerusfracturesin children.JPediatrOrthopB.2009;18(2):93–8.
21.MazdaK,BoggioneC,FitoussiF,Pennec¸otGF.Systematic pinningofdisplacedextension-typesupracondylarfractures ofthehumerusinchildren.Aprospectivestudyof116 consecutivepatients.JBoneJtSurgBr.2001;83(6): 888–93.
22.VaidyaSM.Percutaneousfixationofdisplacedsupracondylar fractureinchildrencomparinglateralwithmedialandlateral pin[thesis].UniversityofSeychelles:AmericanInstituteof Medicine;2009.Availablefrom:http://www.mch-orth.com/ pdf/Thesis%20by%20Dr.Sudeep%20Vaidya.
23.BabalJC,MehlmanCT,KleinG.Nerveinjuriesassociatedwith pediatricsupracondylarhumeralfractures:ameta-analysis.J PediatrOrthop.2010;30(3):253–63.
24.BrauerCA,LeeBM,BaeDS,WatersPM,KocherMS.A systematicreviewofmedialandlateralentrypinningversus lateralentrypinningforsupracondylarfracturesofthe humerus.JPediatrOrthop.2007;27(2):181–6.
25.SkaggsDL,HaleJM,BassettJ,KaminskyC,KayRM,ToloVT. Operativetreatmentofsupracondylarfracturesofthe humerusinchildren.Theconsequencesofpinplacement.J BoneJtSurgAm.2001;83(5):735–40.