www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Accuracy
of
peripheral
arterial
tonometry
in
the
diagnosis
of
obstructive
sleep
apnea
夽
,
夽夽
José
Antonio
Pinto
a,b,∗,
Luciana
Balester
Mello
de
Godoy
a,b,
Renata
Coutinho
Ribeiro
a,
Elcio
Izumi
Mizoguchi
a,
Lina
Ana
Medeiros
Hirsch
a,b,
Leonardo
Marques
Gomes
a,baDepartmentofOtorhinolaryngology,HospitalSãoCamilo,Pompéia,SãoPaulo,SP,Brazil
bOtorhinolaryngologyandHeadandNeckSurgeryandSleepMedicineCenterofSãoPaulo(NOSP),SãoPaulo,SP,Brazil
Received30January2014;accepted8October2014 Availableonline21July2015
KEYWORDS Polysomnography; Obstructivesleep apneasyndrome; Diagnosis
Abstract
Introduction:The use of handheld devices that assess peripheral arterial tonometry has
emergedasanauxiliarymethodforassessmentanddiagnosisofobstructivesleepapnea
syn-drome.
Objective: Toevaluatetheaccuracyofperipheralarterialtonometryinthediagnosisof
obstruc-tivesleepapnea.
Methods:Contemporary cohort cross-sectional study. Thirty patients with suspected
obstructive sleep apnea underwent peripheral arterial tonometry and assisted nocturnal
polysomnographyconcomitantly.
Results:The meanapnea/hypopneaindexbyperipheralarterialtonometrywassignificantly
higherthanthatby polysomnography (p<0.001),but thevaluesofbothsleepstudieswere
significantlycorrelated(r=0.762).Therewasahighcorrelationbetweenvariables:minimum
oxygensaturation(r=0.842,p<0.001),oxygensaturation<90%(r=0.799,p<0.001),andmean
heart rate(r=0.951,p<0.001).Sensitivityandspecificitywere 60%and96.2% (AUC:0.727;
p=0.113),respectively,whenatathresholdvalueof5events/h.Inseverecases(≥30events/h),
theresultwasasensitivityof77.8%andaspecificityof86.4%(AUC:0.846,p=0.003).
Conclusion: Peripheral arterial tonometry is a useful portable device for the diagnosis of
obstructivesleepapnea;itsaccuracyishigherinmoderateandseverecases.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby
ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:PintoJA,deGodoyLBM,RibeiroRC,MizoguchiEI,HirschLAM,GomesLM.Accuracyofperipheralarterial
tonometryinthediagnosisofobstructivesleepapnea.BrazJOtorhinolaryngol.2015;81:473---8.
夽夽Institution:Otorhinolaryngology,HeadandNeckSurgeryandSleepMedicineCenterofSãoPaulo(NOSP),SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](J.A.Pinto).
http://dx.doi.org/10.1016/j.bjorl.2015.07.005
PALAVRAS-CHAVE Polissonografia; Síndromesdaapneia dosono;
Diagnóstico
Acuráciadatonometriaarterialperiféricanodiagnósticodaapneiaobstrutivado sono
Resumo
Introduc¸ão:Autilizac¸ãodedispositivosportáteis,queavaliamatonometriaarterialperiférica,
surgecomométodoadjuvanteparaavaliac¸ãoediagnósticodasíndromedaapneiaobstrutiva
dosono.
Objetivo:Avaliaraacuráciadatonometriaarterialperiféricanodiagnósticodaapneia
obstru-tivadosono.
Método: Estudodecoortecontemporâneacom cortetransversal.Trinta pacientescom
sus-peita de apneia obstrutiva do sono foram submetidos a tonometria arterialperiférica e a
polissonografianoturnaassistidasimultaneamente.
Resultados: A média do índice de apneia/hipopneia pela tonometria arterial periférica
foi significativamente maior do que a da polissonografia (p<0,001), porém os valores de
ambos os estudos do sono foramsignificativamente correlacionados (r=0,762). Houve alta
correlac¸ãoentreasvariáveis:saturac¸ãomínima deoxigênio(r=0,842,p<0,001),saturac¸ão
deoxigênio<90%(r=0,799,p<0,001)e médiadefrequência cardíaca (r=0,951,p<0,001).
Asensibilidadeeespecificidadeforam96,2%e60%(AUC:0,727,p=0,113),respectivamente,
quandolimiarde5eventos/hora.Noscasosgraves(≥30eventos/hora),oresultadofoiuma
sensibilidadede77,8%eumaespecificidadede86,4%(AUC:0,846,p=0,003).
Conclusão::Atonometriaarterialperiféricaéumdispositivoportátilútilnodiagnósticoda
apneiaobstrutivadosonoesuaacuráciaémaiornoscasosmoderadosegraves.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor
ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Obstructive sleep apnea syndrome (OSAS) is a form of sleep-disordered breathing (SDB) characterized by recur-rent episodes of partial or complete obstruction of the upper airways during sleep, which lead to intermittent hypoxemia, transient hypercapnia, and frequent awaken-ingsassociated withclinical signsand/or symptoms.1It is
estimated that the prevalence of OSAS in the adult pop-ulationis2---4%.2 Arecentepidemiologicalstudyshoweda
highprevalenceofOSASintheadultpopulationofSãoPaulo (32.8%).3
ThemostcommonsignsandsymptomsofOSASare snor-ing, excessive daytime sleepiness, and breathing pauses during sleep,in addition to cardiovascular disorderssuch ashypertension,ischemicheartdisease,stroke,heart fail-ure, arrhythmias, and sudden death.4 Early diagnosis is
paramount.Lossofcognitivefunctions(suchas concentra-tion,attention,andmemory),andofexecutivefunctionare oftenobserved,aswellasmoodswings,irritability, depres-sion,andanxiety.5Properdiagnosisandcorrecttreatment
ofOSASleadstosignificantimprovementinsymptoms, redu-cingtherisksassociatedwiththisdisease.6,7
Polysomnography(PSG)is consideredthegold-standard fordiagnosis ofOSAS,whichcombines theovernight mon-itoring of sleep stages with a continuous register of airflow,chestandabdominalventilatorymovements,heart rate, oxygen saturation, snoring, muscle tone, and leg movement.3,8Thenumberofevents(apneasorhypopneas)
persleephourisknownastheapnea---hypopneaindex(AHI), whichis widely used inthe assessment of severityof the syndrome.9
Thereareseveral portabledevices usedfor evaluation anddiagnosisofOSAS.Someofthesedevicesassess periph-eralarterialtonometry(PAT),aphysiologicalsignofchanges intheautonomicnervoussystemthatoccurduringsleep.In additiontoPAT,thesehandheldmonitorsassessheartrate, oxygensaturation,andactigraphy.Anautomaticalgorithm analyzes the amplitude of PAT signal that, in association withvariationsinheartrateandoxygensaturation,identify respiratoryevents.Theresultofthisalgorithmdetermines apnea/hypopnea index (AHI) and respiratory disturbance index(RDI),usingspecificsignalpatterns.10,11
SleepstudieswithPSGarecostly,becausetheyrequire afull sleeplaboratory andaspecializedteam.Therefore, alternative diagnostic methods arebeingdeveloped, such asperipheralarterialtonometry,enablingitsrealizationin patient’sownhomeinordertoreduce costsandmaintain thesame efficiencyin thediagnosis ofsleepdisorders.3,10
The meancostofthesetwodiagnosticmethodswas signi-ficantlydifferent(PSG, US$2252.73; SD,US$877.40; PAT, US$895.74,SDUS$975.00;p<0.001).12
TheaimofthisstudywastoevaluatetheaccuracyofPAT inthediagnosisofobstructivesleepapnea.
Methods
This was a historical, single-blind, cross-sectional cohort study conducted at a private hospital in São Paulo. Whole-night polysomnography was performed in a hos-pital environment concomitantly with peripheral arterial tonometryrecordingswithaWatch-PAT-200®device(Itamar
OSAS(symptomssuchassnoring,excessivedaytime sleepi-ness, and apnea witnessed during sleep by the spouse). Thirty-three patients were subjected to monitoring from October to November of 2013. Of these, three patients were excluded for operational problems in which there wasnotechnicalinterference.Patientswerecarefully pre-clinicallyevaluatedtoexcludethosewithcentralormixed apnea,moderate-to-severelungdisease,neuromuscular dis-ease, and congestive heart failure. Parameters of sleep architectureandrespiratorymeasureswereevaluatedand compared through analysis by polysomnography and with theuseofaWatch-PAT-200®device.Testinterpretationwas
carriedoutbytwophysiciansexperiencedinsleepmedicine. Polysomnography procedures werestaged according to the rules established in the American Academy of Sleep Medicine(AASM)manual(2007);apneaisdefinedasan air-flow reduction>90%for at least90% oftheepisode, for a minimumof10s,andmeasured byathermalsensor.13 For
hypopnea,an‘‘alternative’’rulewasused,whichconsists inanairflowreduction>50%,accompaniedbyoxygen desat-uration>3%and/orawakening,1whichis bestobservedby
nasalcannula.
Watch-PAT®consistsofadeviceplacedonthewristofthe
patient’snon-dominanthand,connectedtoaprobeapplied ontheipsilateralindexfinger.The devicehasasnoreand positionsensorfixedwithadhesiveonthechestandsternal notch,aswellasanoximeterplacedontheringfingeralso of thepatient’s non-dominanthand. The device’sspecific software(zzzPat®)readstheexam.ThezzzPAT® algorithm
is basedon 14features fromtwoseries of PAT amplitude andfrominter-pulseperiods(IPP).Inassociationwith actig-raphy,thesedataallow stagingof patient’ssleepintothe followingstages:wakefulness,lightsleep,deepsleep,and rapideyemovement(REM)sleep.
In statistical analysis, means and standard deviations for continuous variables from assisted nocturnal PSG and Watch-PAT® weredescribedusingSpearmancorrelationand
Bland---Altmanplots.TheaccuracywasanalyzedusingROC curves.ThestatisticalprogramusedwasSPSSv.18.Thep -valuewasconsideredsignificantwhen<0.05.Thisstudywas approvedbytheEthicsinResearchCommitteeofthis insti-tution,underNo.437912.
Results
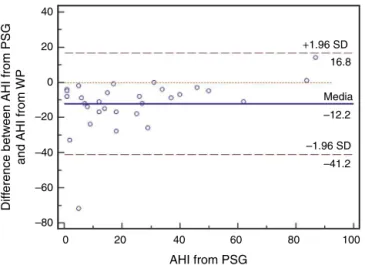
Atotalof30adultpatientswithsuspectedOSAS,20(66.7%) male and 10 (33.3%) female subjects with mean age of 42.8±12.32 years (range 24---71 years) were evaluated. A high correlation among values of the following varia-bles from assisted nocturnal PSG and peripheral arterial tonometry was found: AHI (r=0.762, p<0.0001), min-imum oxygen saturation (r=0.842, p<0.0001), oxygen saturation<90%(r=0.799,p<0.001),andmeanheart rate (r=0.951, p<0.0001) (Table 1 and Fig. 1). With the use ofBland---Altman plots forAHI obtainedfromPAT (WP)vs.
AHI fromPSG,agoodagreement betweenAHI valueswas observed(Fig.2).
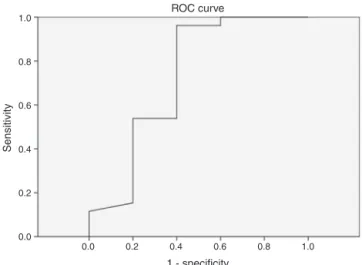
DifferentcutoffvaluesforAHIwereestablishedinorder to evaluate sensitivity and specificity rates of peripheral arterialtonometrytests.ForAHI≥5events/h,the sensitiv-itywas96.2%andthespecificity,60%(AUC0.727,p=0.113)
Table1 Spearmancorrelationamongvaluesoflaboratory
polysomnography(PSGlab)andperipheralarterial
tonome-try(PAT)parameters.
Parameters PSGlabvs.PAT
Spearman
correlation(r)
p-value
RDI 0.688 <0.001
AHI 0.762 <0.001
N1andN2(lightsleep) 0.459 0.014
N3(deepsleep) 0.264 <0.001
REM 0.543 <0.001
MinimumO2saturation 0.842 <0.001
MeanO2saturation 0.683 <0.001
O2saturation>90% 0.799 <0.001
Minimumheartrate 0.668 <0.001
Meanheartrate 0.951 <0.001
RDI,breathingdisturbanceindex;AHI,apnea/hypopneaindex; REM,rapideyemovement.
0 0 20 40 60 80 100
20 40 60
WP
PSG lab
80 100
Mean heart rate NV Mean heart rate WP Total AHI NV Total AHI WP
Figure1 SpearmancorrelationamongAHI,minimumoxygen
saturation,andmeanheartrateofPSGlabandperipheral
arte-rialtonometry(WP).
0 –80 –60 –40 –20 20 40
0
20 40 60
AHI from PSG
Diff
erence betw
een AHI from PSG
and AHI from
WP
80 100 –41.2 –12.2 Media
16.8
–1.96 SD
+1.96 SD
Figure 2 Bland---Altman plot of difference between AHI
fromPSG andAHI fromPAT (WP) withrespect tolaboratory
0.0 0.0
0.2 0.4 0.6 0.8 1.0
0.2 0.4 0.6
1 - specificity ROC curve
Sensitivity
0.8 1.0
Figure 3 ROC curve with cutoff score of AHI≥5events/h
(AUC:0.727).
0.0 0.0
0.2 0.4 0.6 0.8 1.0
0.2 0.4 0.6
1 - specificity ROC curve
Sensitivity
0.8 1.0
Figure4 ROCcurvewith cutoff scoreofAHI≥15events/h
(AUC:0.805).
(Fig.3).ForAHI≥10events/h,thesensitivitywas70%and the specificity 73.7% (AUC 0.761, p=0.018). For AHI≥15 events/h,thesensitivitywas82.4%andthespecificity78.6% (AUC0.805,0.004)(Fig.4).ForAHI≥20events/h,the sen-sitivity was 84.6% and the specificity 83.3% (AUC 0.861,
p=0.001)(Fig.5).ForAHI≥30events/h,thesensitivitywas 77.8% and the specificity 86.4% (AUC 0.846, p=0.003). It worthnotingthataccuracyofPATishigherwhenthevalue ofAHIisgreaterthan20events/hcomparedtolowercutoff scores.
Discussion
The method used to assess peripheral arterial tonometry distinguishes REM sleep from NREM sleep. In REM sleep, thereis anattenuationofPATsignal amplitudeinrelation toNREMsleep.14 As indeepsleep,PAT signalvariabilityis
lowerthan inREMsleep;andsuperficialsleephasgreater variabilitythaninREM,andtherecordingmayalso distin-guishbetweendeepNREMsleepvs.superficialNREMsleep.15
Hedneretal.showedthatPATsignalisusefultodistinguish wakefulnessfromsleep,andforstratificationinlightsleep,
0.0 0.0
0.2 0.4 0.6 0.8 1.0
0.2 0.4 0.6
1 - specificity ROC curve
Sensitivity
0.8 1.0
Figure5 ROCcurve withcutoff score ofAHI≥20 events/h (AUC:0.861).
deep sleep,and REMstages. There was statistical signifi-cancebetweenN3andREMsleepinthisstudy.16Sleeptime
iscriticaltodeterminetrueDRI.Arterialtonometrydetects thestateofsleep/wakefulnessandREMsleepstagethrough the‘‘totalsleeptime’’;thisprovidesanaccurateestimate ofsleeparchitecture.Thedetectionofautomaticsleeptime bythisdiagnosticmethodisdeterminedfromtotalrecording time --- (waking time+invalid sign times). Several valida-tion studies of PAT as a diagnostic method of OSAS have been published.Schnallet al.reporteda highcorrelation betweenAHIvaluesinlaboratorypolysomnographyandPAT (r=0.92,p<0.0001).17Severalotherauthorsalsofoundhigh
correlation between AHI values fromPAT and laboratorial polysomnography.5,8---11,14---16Pangetal.foundagood
correla-tionbetweenAHI(r=0.9288,p<0.0001)andminimaloxygen saturation (r=0.9891, p<0.0001), and between PSG and theportablemonitorthatevaluatesPAT18;O’Donnelletal.
experimentally induced an obstruction of upper airways andconcludedthattheairflowobstructioncharacteristicof OSASpatientsresultsinattenuationofthePATsignal.19
Themajordifferencebetweenthisportablemonitorand other existingdevicesis thattheidentification of respira-toryevents,suchashypopneaandapnea,isperformed by meansofchangesinperipheralarterialtonesignal,without theneedforconventionalmeasuresofairflowand respira-toryeffort.8---11However,peripheralarterialtonometrydoes
notdistinguishbetweenapneasandhypopneas.Choietal. foundhighcorrelationwiththeseverityofAHI(Kendalltau
---b=0.897,p<0.001)andPSG.5WhiletheseverityofOSASis
definedasthesumofthetwoeventsinrelationtototalsleep time,this non-distinctionis hardlyrelevant, sinceapneas andhypopneasleadtosimilarclinicalconsequences.
andspecificityof 88.2and 80.0%,respectively. Therewas a high correlation between PSG and PAT with respect to AHI,respiratorydisturbanceindex,andoxygendesaturation index.20
Thedeviceforperipheralarterialtonometryevaluation tended to overestimate AHI values in mild cases of OSAS (Figs. 3 and 4). In the present study, there was a higher sensitivitytoresaturationrate.Sometimes,thedecreasein saturation level is quite slow andalmost imperceptible ---which couldjustify thepresence ofRERAs, especiallyif a resaturationoccursattheendofalgorithm’smeasurement. Itis alsopossiblethat PAT andheartrate responsevalues ofapatientwithsevereOSASaredifferentthanthose val-uesof apatientwithmild OSASduringan apnea episode. Furthermore,itcanbeobservedthattheresaturationrate canvarysignificantlyin thesamepatientduring different timesegments.21 This fact doesnot diminishtheportable
device usefulness,asclinical data associatedwitha prior screeningprocedureresultinhighsensitivityinthe diagno-sisof OSAS,obviating the exclusionof potential patients. Itcanbeinferredthattheaccuracyof thisportable mon-itor is better for patients withhigh probabilityof having moderateorsevereOSAS.However,inthecaseofpatients undersuspicionofadifferentsleepdisorderthanDRS, lab-oratorypolysomnographymustbeindicatedasadiagnostic method.22,23
According toa recentmeta-analysispublished by Yala-manchalietal.,ahighcorrelationofRDIandAHI(r=0.889 [95%CI,0.862---0.911],p<0.001)wasdemonstrated.Studies comparingRDIbetweenPATandPSGhadacombined correla-tionof0.879(95%CI,0.849---0.904,p<0.001),whileinthose comparing AHI, this correlation was 0.893 (0.857---0.920,
p<0.001). On the other hand, in those studies that com-pared the oxygen desaturation index (ODI), a correlation of0.942(0.894---0.969,p<0.001)wasfound.24 Anstudyon
children showed that PAT sign was significantly higher in thosesubjectswithOSAScomparedwithcontrols,indicating increasedsympathetic toneduring wakefulness.25 Arterial
stiffnessalsocorrelatedwithsleepdisorders(arousalindex) and mean O2 saturation; this variable better reflects the
cardiovascularimpactofOSASvs.AHIinconventionalPSG. Increased arterial stiffness (AS) is widely recognized as a determinantfactorofcardiovascularriskandhasalsobeen linkedtoOSAS.26
Therearesomelimitationstothisstudy.Theevaluation ofarterialtonometrywasperformedinasleeplaboratory, and not in the patient’s home. The use of this portable deviceissuitableforhomemonitoring;thus,furtherstudies shouldbeconductedinordertoevaluatethe reproducibil-ityoftheseresultsoutsidethe sleeplaboratory.However, ascheme of carryingoutboth tests simultaneously would exclude the possible variationof results that could occur fromonenighttothenext.Anotherlimitationisthesmall sample,andtherewasnocontrolgroupwithout signsand symptomsofobstructivesleepapnea.Morestudies should beconductedwithalargernumberofindividuals.
Conclusion
Respiratory parameters derived from arterial tonometry showed a good correlation and accuracy when compared
withpolysomnography; andAHI>20/h showed better sen-sitivity and specificity. Peripheral arterial tonometry is a veryvaluableoption for the diagnosis of OSAS,especially in cases of patients withhigh probabilityof moderate or severeOSAS.Becausethisisaneasy-to-useportabledevice, theresultsarereadilyprovidedandinterpreted;thus,this wouldserveasan optiontooptimizetheidentification of patientswithsuspectedOSAS.Inthismanner,itsusewould allowamoreprompttreatmentofthisdisease.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.International classification of sleep disorders, second edi-tion:diagnosticandcodingmanual.Westchester,IL:American AcademyofSleepMedicine;2005.
2.YoungT,PaltaM,DempseyJ,SkatrudJ,WeberS,BadrS.The occurrenceofsleep-disorderedbreathing amongmiddle-aged adults.NEnglJMed.1993;328:1230---5.
3.TufikS,Santos-SilvaR,TaddeiJA,BittencourtLR.Obstructive sleep apnea syndrome inthe São Pauloepidemiologic sleep study.SleepMed.2010;11:441---6.
4.KimJ,InK,KimJ, YouS,KangK,ShimJ,etal. Prevalence ofsleep-disorderedbreathinginmiddle-agedKoreanmenand women.AmJRespirCritCareMed.2004;170:1108---13. 5.ChoiJH,KimEJ,KimYS,ChoiJ,KimTH,KwonSY,etal.
Vali-dationstudyofportabledeviceforthediagnosisofobstructive sleepapneaaccordingtothenewAASMscoringcriteria: watch-PAT100.ActaOtolaryngol.2010;130:838---43.
6.ShaharE,WhitneyCW,RedlineS,LeeET,NewmanAB,NietoFJ, etal.Sleep-disordered breathingand cardiovasculardisease: cross-sectionalresultsoftheSleepHeartHealthStudy. AmJ RespirCritCareMed.2001;163:19---25.
7.KushidaCA,LittnerMR,MorgenthalerT, Alessi CA,BaileyD, ColemanJJr,etal.Practiceparametersfortheindicationsfor polysomnographyandrelatedprocedures:anupdatefor2005. Sleep.2005;28:499---521.
8.HednerJ,PillarG,PittmanSD,ZouD,GroteL,WhiteDP.Anovel adaptivewristactigraphyalgorithmforsleep---wakeassessment insleepapneapatients.Sleep.2004;27:1560---6.
9.AyasNT,PittmanS,MacDonaldM,White DP.Assessmentofa wrist-worndeviceinthedetectionofobstructivesleepapnea. SleepMed.2003;4:435---42.
10.BaroneD.TheWatch-Patinthesleeplaboratory.ItamarMedical Ltd.;2005.
11.BarA, Pillar G, Dvir I,SheffyJ,Schnall RP,Lavie P. Evalua-tionofaportabledevicebasedonperipheralarterialtonefor unattendedhomesleepstudies.Chest.2003;123:695---703. 12.Townsend D, Sharma A, Brauer E, Scattarelli D, McEiver J,
EikenT,et al.Assessingefficacy,outcomes,andcostsavings forpatientswithobstructivesleepapneausingtwodiagnostic andtreatmentstrategies.SleepDiagnTherapy.2007;7:1---8. 13.IberC,Ancoli-IsraelS,ChessonALJr,QuanSF.TheAASMmanual
for the scoring of sleep and associated events: rules, ter-minologyandtechnicalspecifications.Westchester:American AcademyofSleepMedicine;2007.
14.HerscoviciS,Pe’erA,PapyanS,LavieP.DetectingREMsleep from thefinger:anautomaticREMsleepalgorithm basedon peripheral arterial tone (PAT) and actigraphy. Physiol Meas. 2007;28:129---40.
devicebased onperipheralarterial tonometry.PhysiolMeas. 2008;29:571---84.
16.HednerJ,WhiteDP,MalhotraA,HerscoviciS,PittmanSD,ZouD, etal.Sleepstagingbasedonautonomicsignals:amulti-center validationstudy.JClinSleepMed.2011;15:301---6.
17.SchnallRP,ShlitnerA,SheffyJ,KedarR,LavieP.Periodic, pro-foundperipheralvasoconstriction---anewmarkerofobstructive sleepapnea.Sleep.1999;22:939---46.
18.PangKP,GourinCG,TerrisDJ.Acomparisonofpolysomnography andtheWatchPATinthediagnosisofobstructivesleepapnea. OtolaryngolHeadNeckSurg.2007;137:665---8.
19.O’DonnelC,AllanL,AtkinsonP,SchwartzA.Theeffectofupper airway obstructionandarousalonperipheral arterial tonom-etryin obstructive sleepapnea.Am JRespirCritCareMed. 2002;166:965---71.
20.CeylanT,FıratH,Kuran G,Ardıc¸S,BilginE,C¸elenkF.Quick diagnosisinobstructivesleepapneasyndrome:WatchPAT-200. IranRedCrescentMedJ.2012;14:475---8.
21.BetitoM[dissertac¸ão]DiagnosisofOSAsyndromefromPATand oximetryrecordingsusingfuzzydecisiontrees.TelAviv Univer-sity;2004.
22.Pittman SD, Ayas NT, MacDonald MM, Malhotra A, Fogel RB, White DP. Using a wrist-worn device based on periph-eralarterialtonometry todiagnoseobstructive sleepapnea: in-laboratory and ambulatory validation. Sleep. 2004;27: 923---33.
23.Berry RB, Hill G, Thompson L, McLaurin V. Portable mon-itoring and auto-titration versus polysomnography for the diagnosis and treatment of sleep apnea. Sleep. 2008;31: 1423---31.
24.YalamanchaliS,FarajianV,HamiltonC,PottTR,SamuelsonCG, FriedmanM.Diagnosisofobstructivesleepapneabyperipheral arterialtonometry:meta-analysis.JAMAOtolaryngolHeadNeck Surg.2013;139:1343---50.
25.NisbetLC,YiallourouSR,WalterLM,HorneRS.Bloodpressure regulation,autonomiccontrolandsleepdisorderedbreathing inchildren.SleepMedRev.2014;18:179---89.