r e v b r a s r e u m a t o l . 2017;57(5):479–482
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
Disseminated
histoplamosis
in
adolescent
mimicking
granulomatosis
with
polyangiitis
Histoplamose
disseminada
em
um
adolescente
mimetizando
uma
granulomatose
com
poliangiíte
Marlon
van
Weelden
a,b,
Gabriela
R.
Viola
c,
Katia
T.
Kozu
d,
Nadia
E.
Aikawa
d,e,
Claudia
M.
Ivo
f,
Clovis
A.
Silva
d,e,∗aVrijeUniversity,MedicalFaculty,Amsterdam,TheNetherlands
bUniversidadedeSãoPaulo,FaculdadedeMedicina,DepartamentodePediatria,SãoPaulo,Brazil
cUniversidadedeSãoPaulo,FaculdadedeMedicina,UnidadedeReumatologia,SãoPaulo,Brazil
dUniversidadedeSãoPaulo,FaculdadedeMedicina,UnidadedeReumatologiaPediátrica,SãoPaulo,Brazil
eUniversidadedeSãoPaulo,FaculdadedeMedicina,DivisãodeReumatologia,SãoPaulo,Brazil
fUniversidadedeSãoPaulo,FaculdadedeMedicina,UnidadedeInfectologiaPediátrica,SãoPaulo,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received5June2014 Accepted20January2015 Availableonline14July2015
Introduction
Systemicinfections are importantdifferential diagnoses to autoimmunepediatricrheumaticdiseases.Disseminated fun-gal infections have been rarelyreported in these patients, especiallyinchildhood-onsetsystemiclupuserythematosus patientsunderdiseaseactivity,lymphopeniaor immunosup-pressortherapy.1–3
In addition, systemic histoplasmosis generally is asso-ciated with immunocompromised patients.4 This inva-sive fungal infection may mimic primary vasculitis with similar clinical manifestations, in particular granulomato-sis with polyangiitis (GPA) or Wegener granulomatosis, which was rarely described in adult patients, but to our
∗ Correspondingauthor.
E-mail:[email protected](C.A.Silva).
knowledgesuchathinghasnotbeen reportedinpediatric population.5
Therefore, we reported herein an immunocompetent patient with disseminated histoplasmosis mimicking GPA thatfulfilledthenewEuropeanLeagueAgainstRheumatism (EULAR), Pediatric Rheumatology International Trials Orga-nization(PRINTO),PediatricRheumatologyEuropeanSociety (PRES) propose validated classificationcriteria forpediatric population.6
Case
report
A 6year-oldboy hadrecurrent acute migratory polyarthri-tis in shoulders, elbows, hips and knees associated with
http://dx.doi.org/10.1016/j.rbre.2015.01.003
480
r e v b r a s r e u m a t o l . 2017;57(5):479–482recurrentsinusinflammation,fever,malaise,headachesand dailyabdominalpain.Aftertwomonthsatadmissioninour University Hospital, hepresented arthritisin the left knee and morning stiffness of 2h with spontaneous remission. Laboratorytestsshowederythrocytesedimentationrate(ESR) 81mm/1sthour,C-reactiveprotein(CRP)63mg/L,hemoglobin 11.2g/dL, hematocrit 32%, white blood cell count (WBC) 11,400/mm3(neutrophils60%,lymphocytes35%,eosinophils
1%and monocytes 4%) and platelets counts 523,000/mm3.
Serologic tests for hepatitis A, B and C, cytomegalovirus, humanimmunodeficiencyvirus,Epstein–Barrvirus, toxoplas-mosis,denguevirusandantistreptolysinOwereallnegative. Ophthalmologicalexamination, bonescintigraphy, echocar-diogram,colonoscopy,skull computertomography(CT)and bonemarrowaspiratewerenormal.Abdomenmagnetic res-onance imaging (MRI) revealed moderate ascites in pelvis andsinusesMRIshowedpansinusitis.Antinuclear antibod-ies (ANA)were1/80.Antineutrophil cytoplasmicantibodies (c-ANCA)werepositiveontwodifferentoccasions(1/80and 1/20) at 6 years old, and were systematically negative on an annual basis. The anti-proteinase 3 antibody was not evaluated. Therheumatoid factorand anti-DNA antibodies were negative. Serum levels of IgG were 1988mg/dL (nor-malrange970–1710),IgA301mg/dL(normal69–382)andIgM 340.5mg/dL(normal53–145).Lymphocyte immunophenotyp-ingshowed: CD3+ 1614cells/mm3 (normal1000–2200),CD4+
1136cells/mm3(normal 530–1300),CD8+412cells/mm3
(nor-mal330–920),CD16+/56+ 135cells/mm3(normal70–480)and
CD19+246cells/mm3(normal110–570).C4was38mg/dL
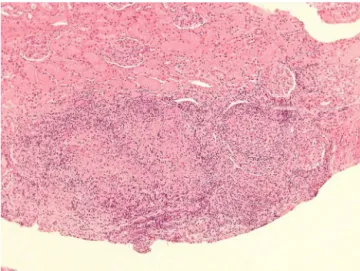
(nor-mal10–40)andC3164mg/dL(normal90–180).Atthatmoment, childhoodGPAwassuspected,howeverhehadspontaneous regressionofsymptoms,normalizationofacutephase reac-tantsand absence offever for5years. At11years and 10 months,hepresentedacute sinusitis and pneumoniawith pleural effusion, which improved after benzylpenicillin for 10 days. At 11 years and 11 months, he had epididymi-tis confirmedbytesticular ultrasound.At12years,hewas hospitalized dueto persistent headache,ocular hyperemia and left palpebral edema. MRI showed left eye proptosis degree1.Thecerebrospinalfluidanalysiswasnormal, includ-ingnegativefungusandtuberculosiscultures.Indirecttests (detectionofantigenorcell-wallconstituents)foraspergilosis, histoplasmosis and paracoccidioidomycosis were negative. Noepidemiology for histoplasmosis was reported. c-ANCA was negative. Urinalysis was normal and proteinuria was 0.007g/24h. At the age of12 years and 2months, hewas hospitalizedduetolumbarpain.ThoraxCTshowedthe pres-enceofpulmonarynoduleinrightlung andabdominalCT presentedheterogeneous mass with 2.5cm ofdiameter in parenchymaoftherightkidney.Atthatmoment,eventhough thepatientfulfilledtheEULAR/PRINTO/PRESchildhoodGPA criteria,6 the renal biopsy showed a focal granulomatous interstitialnephritiswithyeastfungalcellscompatiblewith Histoplasma sp. (Figs. 1 and 2). He was treated only with liposomalamphotericinB(4.0mg/kg/day)for12 days, with improvement of ocular proptosis, epididymitis and renal mass.Afterthat, hereceiveditraconazole(300mg/dayfor3 days)and continued with200mg/day in two doses ofthis antifungaltherapyforthelast6monthswithoutanysignsor symptoms.
Fig.1–YeastfungalcellscompatiblewithHistoplasmasp. accordingtoGrocotcoloring.
Discussion
To our knowledge, this was the first caseof disseminated histoplasmosisinpediatricpopulation,mimickingGPA.5,7
Histoplasmosis is caused byHistoplasma sp. which is a dimorphic fungal pathogen8 and usually affects the respi-ratory tract.9 This mycosis has been reported in Brazil, especiallyintheMidwesternandSoutheasternregions.10The disease can be classified in three subtypes: disseminated histoplasmosis (generally in immunosuppressed patients), acutepulmonaryhistoplasmosis(mainlyin immunocompe-tenthost)andchronicpulmonaryhistoplasmosis(associated withanatomicdefect).11
This fungal infection is mostly asymptomatic and self-restrictive in normal children. However it can cause dis-seminated and acute formin immunocompromised hosts, such as those who receive corticosteroids and immuno-suppressive agents, after transplantation and in acquired immune-deficiency syndrome(AIDS) patients.9 Our patient
Fig.2–Focalgranulomatousinterstitialnephritisaccording
r e v b r a s r e u m a t o l . 2017;57(5):479–482
481
had a long disease duration, probably due to adequate immuneresponse.Healsohadapossiblespontaneous remis-sionand not requiring immunosuppressivetherapy during thisperiod.Indeed,disseminatedformofhistoplasmosiswas onlyconfirmed6yearsaftertheinitialmanifestations.
Histoplasmosiscanleadtospectrumofclinical manifesta-tions,generallyincludesfever,malaiseandrespiratory,aswell asgastrointestinalsymptoms,asobservedherein.4 Addition-ally,epididymitiswasrarelyreportedinadultpatientsinfected byHistoplasmasp.12Ofnote,acutemigratorypolyarthritisis also seldom described in adulthistoplasmosis population, generally self-limited and disappears without sequelae, as observedinourpatient.13Nevertheless,onlyonecaseof pedi-atrichistoplasmosiswithpolyarthritiswasreported.14
There are rare cases of histoplasmosis mimicking vas-culitis.Generalizedlymphadenopathyandrenalinvolvement, mainlyglomerulonephritisandchronicrecurrentabscessof urogenital tract, were the main clinical manifestations of disseminated histoplasmosis in the twocases reported.5,11 Inaddition,associationofdisseminatedhistoplasmosiswith GPAwasdiagnosedatnecropsyintheotherpatient.7
Importantly,the confirmeddiagnosis wasobtainedafter fungus isolation in renal tissue, fulfilling “proven invasive fungaldisease”fordisseminatedhistoplasmosisaccordingto NationalInstituteofAllergyandInfectiousDiseasesMycoses StudyGroup.15Indirecttestsoffungishowedlowsensitivityto histoplasmosisdiagnosisandHistoplasmaserologypositivity variedfrom20%to80%.4Ourpatienthadpositivec-ANCA,a wellknownbiomarkerofGPA,inlowtitersandthis autoanti-bodywasrarelyreportedinhistoplasmosispatients.16
Interestingly, our patient had three out of the six EULAR/PRINTO/PREScriteriaforGPA,includingupperairway involvement,pulmonaryinvolvementand positivec-ANCA. Thesensitivityandspecificityforthesecriteriawere93.3%and 99.2%,respectively.6Inspiteofthehighspecificity,these vali-datedcriteriawereestablishedforchildrenandadolescentsby comparingGPAwithotherprimaryvasculitis,thusreinforcing therelevanceofthedifferentialdiagnosiswithgranulomatous infectiouschronicdiseasesinpediatricpopulation,asshown inthepresentcase.
GPAisfrequentlyamoreseveresystemicprimary vasculi-tisthatmayleadtosinusitis,pulmonarynodules,cavitations oralveolarhemorrhageandseriouspauci-immune glomeru-lonephritis, in contrast tothe satisfactory outcome ofour patient.17
Thetreatmentofpediatricandadulthistoplasmosisis per-formedaccordingtoInfectiousDiseasesSociety ofAmerica guidelines.AmphotericinBandafteritraconazolare recom-mended,asadministeredinourpatient.18
Inconclusion,wereportedapatientwithprogressive dis-seminated histoplasmosis mimicking GPA. Histoplasmosis infection should also be considered in immunocompetent childrenandadolescentswithuncommonclinical manifes-tations,suchasjoint,kidneyandgenitalinvolvements.
Funding
ThisstudywassupportedbyFundac¸ãodeAmparoàPesquisa doEstadodeSãoPaulo(FAPESP–grants2008/58238-4toCAS),
byConselhoNacionaldoDesenvolvimentoCientíficoe Tec-nológico (CNPQ – grant 302724/2011-7 to CAS),by Federico FoundationtoCASandbyNúcleodeApoioàPesquisa“Saúde daCrianc¸aedoAdolescente”daUSP(NAP-CriAd).Wethank Dr.VarniforprovidingthePediatricQualityofLifeInventory 4.0(PedsQL4.0)instrument.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.Franc¸aCM,CavalcanteEG,RibeiroAS,OliveiraGT,LitvinovN, SilvaCA.Disseminatedhistoplasmosisinajuvenilelupus erythematosuspatient.ActaReumatolPort.2012;37:276–9. 2.SilvaMF,RibeiroAS,FiorotFJ,AikawaNE,LotitoAP,Campos
LM,etal.Invasiveaspergillosis:asevereinfectioninjuvenile systemiclupuserythematosuspatients.Lupus.
2012;21:1011–6.
3.SizemoreTC.Rheumatologicmanifestationsof histoplasmosis:areview.RheumatolInt.2013;33:2963–5. 4.AssiMA,SandidMS,BaddourLM,RobertsGD,WalkerRC.
Systemichistoplasmosis:a15-yearretrospectiveinstitutional reviewof111patients.Medicine(Baltimore).2007;86:162–9. 5.PapoT,BoisnicS,PietteJC,FrancesC,BeaufilsH,LeTH,etal.
Disseminatedhistoplasmosiswithglomerulonephritis mimickingWegener’sgranulomatosis.AmJKidneyDis. 1993;21:542–4.
6.OzenS,PistorioA,IusanSM,BakkalogluA,HerlinT,BrikR, etal.EULAR/PRINTO/PREScriteriaforHenoch-Schönlein purpura,childhoodpolyarteritisnodosa,childhoodWegener granulomatosis,andchildhoodTakayasuarteritis:Ankara 2008.PartII:finalclassificationcriteria.AnnRheumDis. 2010;69:798–806.
7.ManepalliAN,RushL.Disseminatedhistoplasmosisand Wegener’sgranulomatosis.SouthMedJ.1998;91:1156–8. 8.DarlingST.Aprotozoangeneralinfectionproducing
pseudotuberclesinthelungsandfocalnecrosisintheliver, spleen,andlymphnodes.JAMA.1906;46:1283.
9.FischerGB,MocelinH,SeveroCB,deMattosOliveiraF,Xavier MO,SeveroLC.Histoplasmosisinchildren.PaediatrRespir Rev.2009;10:172–7.
10.GuimarãesAJ,NosanchukJD,Zancopé-OliveiraRMN. Diagnosisofhistoplasmosis.BrazJMicrobiol.2006;37:1–13. 11.UbesieAC,OkafoOC,IbeziakoNS,OnukwuliVO,MbanefoNR,
UzoigweJC,etal.DisseminatedHistoplasmosisina 13-year-oldgirl:acasereport.AfrHealthSci.2013;13:518–21. 12.TichindeleanC,EastJW,SarriaJC.Disseminated
histoplasmosispresentingasgranulomatous epididymo-orchitis.AmJMedSci.2009;338:238–40. 13.CuéllarML,SilveiraLH,EspinozaLR.Fungalarthritis.Ann
RheumDis.1992;51:690–7.
14.VerhaertK,RodriguezM,MendozaG,DelgadilloJL,CasaerP. Polyarthritisandhumeralepiphysialseparationinaninfant withacutedisseminatedhistoplasmosis.PediatrInfectDisJ. 2002;21:352–3.
482
r e v b r a s r e u m a t o l . 2017;57(5):479–48216.MeadGE,WilksD,McLarenK,FergussonRJ.Oral histoplasmosis:acasereport.JInfect.1998;37:73–5. 17.TwiltM,BenselerS,CabralD.Granulomatosiswith
polyangiitisinchildhood.CurrRheumatolRep. 2012;14:107–15.
18.WheatLJ,FreifeldAG,KleimanMB,BaddleyJW,McKinseyDS, LoydJE,etal.Clinicalpracticeguidelinesforthemanagement ofpatientswithhistoplasmosis:2007updatebytheInfectious DiseasesSocietyofAmerica.ClinInfectDis.2007;45: