w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
Report
Acute
myeloid
leukemia
with
e1a2
BCR-ABL1
fusion
gene:
two
cases
with
peculiar
molecular
and
clinical
presentations
Fernanda
Borges
da
Silva
a,
João
Agostinho
Machado-Neto
a,
Luisa
Corrêa
de
Araujo
Koury
a,
Virginia
Helena
Leira
Lipoli
Bertini
a,
Cristina
Alonso
Ratis
b,
Maria
de
Lourdes
Lopes
Ferrari
Chauffaille
c,
Elvira
Deolinda
Rodrigues
Pereira
Velloso
b,d,
Belinda
Pinto
Simões
a,
Eduardo
Magalhães
Rego
a,
Fabiola
Traina
a,∗aFaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo(FMRPUSP),RibeirãoPreto,SP,Brazil bHospitalIsraelitaAlbertEinstein,SãoPaulo,SP,Brazil
cEscolaPaulistadeMedicinadaUniversidadeFederaldeSãoPaulo(EPMUnifesp),SãoPaulo,SP,Brazil
dHospitaldasClínicasdaFaculdadedeMedicinadaUniversidadedeSãoPaulo(HCFMUSP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17May2017 Accepted6July2017
Availableonline3August2017
Introduction
Acutemyeloidleukemia(AML)diseaseentitiesareclassified bytheWorldHealthOrganization(WHO)basedonsignificant cytogeneticand moleculargeneticfindings.1,2 Thecategory of acute myeloid leukemia not otherwise specified (AML-NOS)includescaseswith≥20%myeloblastsintheperipheral
blood(PB)orbonemarrow(BM)intheabsenceofrecurrent geneticabnormalities,myelodysplasia-relatedchangesor pre-viouscytotoxictherapy.CasesofAMLwithdysplasiain≥50%
∗ Correspondingauthorat:DepartmentofInternalMedicine,FaculdadedeMedicinadeRibeirãoPretodaUniversidadedeSãoPaulo(FMRP USP),Av.Bandeirante3900,RibeirãoPreto,SP,Brazil.
E-mailaddress:[email protected](F.Traina).
of the cells in two or more myeloid cell lineages or cases preceded byawell-documented history ofmyelodysplastic syndromes (MDS) or MDS/myeloproliferative neoplasm are definedasAMLwithmyelodysplasia-relatedchanges (AML-MRC).1,2 AML-MRC developsin approximately one-third of MDS andgenerally hasapoorprognosis.3,4 Cytogeneticsis amandatorytoolinthediagnosisofAMLwithchromosome abnormalitiesbeingpresentinapproximatelyhalfoftheadult AML cases; chromosome abnormalities have an important prognosticvalue.5
http://dx.doi.org/10.1016/j.bjhh.2017.07.001
A
C
E
J
K
F
H
I
D
B
G
Chromosome 2
Chromosome 9 Chromosome 19
Chromosome 22 Chromosome 20
Chromosome 7
1 2 3 4 5
1
1
1 6
6
6 13
13
13 19
19
19 14
14
14 20
20
20
21
21
21 22
22
22 15
15
15 7
7
7 8
8
8 9
9
9 16
16
16 11
11
11 10
10
10 4
4
4 5
5
5 12
12
12 18
18
18 17
17
17 2
2
2 3
3
3
X
X
X Y
Y
Y
Metaphase cytogenetics has proven to bean extremely valuable clinical toolin the management ofhematological malignancies.Thismethodology candetect balanced chro-mosomalchanges,includingtranslocationorinversion,and unbalancedchromosomalchanges,includingtrisomy, dupli-cation,anddeletion.Thesuccessofmetaphasecytogenetics requirescellularproliferationandchromosomespreads;the sensitivityand the resolutiondependon the proportionof clonal cells in the tested sample and on the size of the lesion,respectively.6 Single nucleotidepolymorphism array (SNP-A),alsoreferredtoaschromosomalmicroarray,hasbeen appliedasahigh-resolutionwholegenomescanningtoolto detectunbalancedchromosomalchanges.Themajor advan-tageofSNP-Aovermetaphasecytogeneticanalysisisitsability todetecthiddenchromosomaldefects,including submicro-scopic(cryptic)aberrationsandthedistinctionofindividual genotypestodetectcopynumber-neutrallossof heterozygos-ity(CN-LOH),alsodefinedasuniparentaldisomy.7
ThePhiladelphia(Ph)chromosomeresultsfromabalanced translocationt(9;22)(q34;q11.2)thatleadstotheformationof thefusionproteinBCR-ABL1withconstitutivetyrosinekinase activity.ThreedifferentbreakpointclusterregionsintheBCR gene (M-bcr, m-bcr, and -bcr) are reported: 8.5kb hybrid
mRNA(b2a2orb3a2)encodesthe210kDaprotein(p210),7.5kb hybridmRNA(e1a2)encodesthe190kDaprotein(p190)and 9kbhybridmRNA(c3a2)encodesthe230kDaprotein(p230).8 Thet(9;22)(q34;q11.2)isfoundin90–95%ofcasesofchronic myeloid leukemia and around 20% of acute lymphoblastic leukemia.Incontrast,thePhchromosomeisveryrareinAML, accountingforapproximately1–2%ofthecases.9Neuendorff etal.10recentlyreviewedcasereportsandcaseseriesofAML withBCR-ABL1intheliteraturesince1975,aswellascases fromtheirowninstitution.Theauthorsreportedthatamong the 126confirmed casesofAMLwithBCR-ABL1, 38% were definedbyWHO2008asAML-NOS,32.5%asAML-MRC,and 16.7%ascorebindingfactorleukemia.10
Recently,theWHO2016classificationincludedanew pro-visionalcategoryfordenovoAMLwithBCR-ABL1,recognizing this rare diagnostic entity that may benefit from tyrosine kinaseinhibitortherapy.11Thepatientsarestratifiedas inter-mediateII riskaccording toEuropeanLeukemiaNet and in thepoor-riskgroupaccordingtotheNationalComprehensive CancerNetwork.5,12
Herein,wepresenttwounusualcasesofAMLwith BCR-ABL1. In accordance with WHO 2008 definitions, Case 1 was diagnosed as AML-MRC and presented with complex karyotypeandthee1a2BCR-ABL1genefusion.Case2was diag-nosedasdenovoAML-NOSandpresentedanear-tetraploidy karyotype and the e1a2 BCR-ABL1 gene fusion. Both cases
wereinvestigatedbyconvectionalcytogeneticsandmolecular approaches.
Methods
Patients
Patientsdescribedinthisreportwerefollowedupatthe Hos-pitaldasClínicasoftheUniversidadedeSãoPauloinRibeirão Preto,SãoPaulo,Brazil.TheEthicsCommitteeofthe institu-tionapprovedthestudy,andwritteninformedconsentwas obtained.ThealgorithmproposedbyNeuendorffetal.10was usedtoexcludethe diagnosisofchronicmyeloidleukemia blastcrisis.
Metaphasecytogenetics
MetaphasecytogeneticswasperformedonBMaspirateusing standardmethodsandthekaryotypewasdescribedaccording totheInternationalSystemforHumanCytogenetic Nomen-clature(ISCN)2013.13
Singlenucleotidepolymorphismarray
FortheSNP-A,genomicDNAwasextractedfromBM accord-ing to the manufacturer’s instructions (QIAGEN DNA Kit, Valencia,CA,USA). SNP-AwasperformedusingAffymetrix Genome-Wide HumanSNPCytoscanHD (Affymetrix,Santa Clara,CA,USA).ThefileswereanalyzedusingChromosome AnalysisSuite(ChAS)software.Regionsofcopynumber vari-ants(CNVs)largerthan1MbandCN-LOHlargerthan10Mb were denoted as true aberrations. In order to detect the somaticorigin copy number alterationsdistinguishedfrom constitutionalpolymorphicCNVs,thelesionsidentifiedusing SNP-A were comparedwiththeDatabaseofGenomic Vari-ants(DGV;http://projects.tcag.ca/variation).Aberrationsthat were identifiedbySNP-Aweredescribed accordingtoISCN 2013.13
Reversetranscriptase-polymerasechainreactiontodetect BCR-ABL1
TotalRNA(1g) wasobtainedfrom thepatient’speripheral
bloodcellsandsubmittedtoreversetranscriptionpolymerase chainreaction(RT-PCR)usingtheHighCapacitycDNAReverse TranscriptionKit(LifeTechnologies,Carlsbad,CA,USA).The first PCRwas performed on avolume of 25L containing:
1× reaction buffer, 1.5mM MgCl2, 200M dNTPs, 10pmol
of each primer (Mbcr1: 5′
-GAAGTGTTTCAGAAGCTTCTC-3′; 2oabl1: 5′-TGATTAAGCCTAAGACCC GGA-3′; mbcr1: 5′
-CCATCGTGGGCGTCCGCA-3′),0.5UTaqDNApolymerase(Life
Technologies) and 1.5L cDNA. The first PCR conditions
were an initial phase of 2min at 94◦C, then 25 cycles
at 94◦C for 30s, 51◦C for 40s, 72◦C for 1min, followed
by a final extension step at 72◦C for 7min. The second
PCR was performed on a volume of 25L containing: 1×
reaction buffer, 1.5mM MgCl2, 200M dNTPs, 10pmol of
each primer (Mbcr2: 5′
-TGGAGCTGCAGATGCTGACCAACTC-3′;mbcr2:5′-AGATCTGGCCCAACGATGGCGAGGGC-3′;2iabl2:
5′-ATCTCCAGTGGCCAGAAAATCATAC-3′),0.5UTaqDNA
poly-merase(LifeTechnologies)and1LofPCRproductsfromthe
firstreaction.SecondPCRconditionswereaninitialphaseof 2minat94◦C,then35cyclesat94◦Cfor30s,60◦Cfor30s,72◦C
for1min,followedbyafinalextensionstepat72◦Cfor7min.
ThePCRproductswereanalyzedon2%agarosegelstained withethidiumbromide.
Case
1
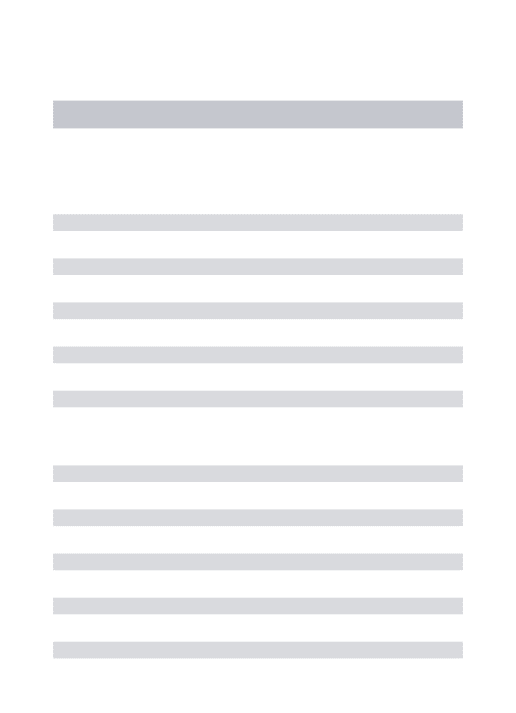
An 82-year-old male with systemic hypertension, with-out other relevant medical history and good performance status(Easterncooperativeoncologygroup: 0)sought med-ical attention complaining of weight loss, asthenia, and petechiaeduringtheprevious45days.Physicalexamination revealed pallor, petechiae and absence of hepatomegaly andsplenomegaly.Thecomplete blood countshowed pan-cytopenia (hemoglobin 7.2g/dL, white blood cell count 2.5×109/L, neutrophil count 0.3×109/L, lymphocyte count
2.2×109/L, and platelet count 8×109/L). BM aspiration
revealed20%myeloblasts,anddysplasticalterationsin70% of erythroid and megakaryocytic lineages (Figure 1A–F). The immunophenotypic analysis showed that the blasts were positive for human leukocyte antigens – (HLA)-DR, CD13,CD33,CD34,CD117,CD7, CD133,and CD56and neg-ative for CD19, CD15, CD11c, CD42a, CD22, CD2, CD11b, CD64, CD14, and CD36. The patient was started on sub-cutaneous low dose cytarabine immediately after the diagnosisofAML.Metaphasecytogeneticsanalysisrevealed 46,XY,t(9;22)(q34;q11),del(20)(q11)[2]/46,idem,inv(7)(q22q36) [6]/47,idem,inv(7)(q22q36),+19[12] (Figure 1G–I). An RT-PCR assay for BCR-ABL1 confirmed the presence of t(9;22) and revealedap190BCR-ABL1isoform(e1a2BCR-ABL1)(Figure1J). The SNP-A identified the loss of 2q36 not identified by metaphase cytogenetics: arr[hg19] 2q36.3q37.3(229,385,664-239,698,667)x1, and confirmed the loss of 20q11: arr[hg19] 20q11.21q13.13(30,955,339-49,197,975)x1. As expected, the SNP-Adidnotdetectthebalancedtranslocationt(9;22), nei-thertheinversionof7q.SNP-Aallowedfortheidentification ofthelossof7q36notidentifiedbymetaphasecytogenetics: arr[hg19]7q36.3(155,607,058-156,777,458)x1.However,SNP-A failed to identifythe trisomy ofchromosome 19, probably explained bythe limited sensitivity ofthe test forlesions presentinlessthan30%oftheunculturedcells(Figure1K). ThepatientwasclassifiedasAMLwithBCR-ABL1according toWHO2016andasAML-MRCaccordingtoWHO2008.The patient presented persistent pancytopenia and increased BM blasts following two cycles of subcutaneous low dose
cytarabine and was started on imatinib. No hematologic responsewasobservedaftertwomonthsofimatinibandthe patientsubsequentlydiedofinfectiouscomplications.
Case
2
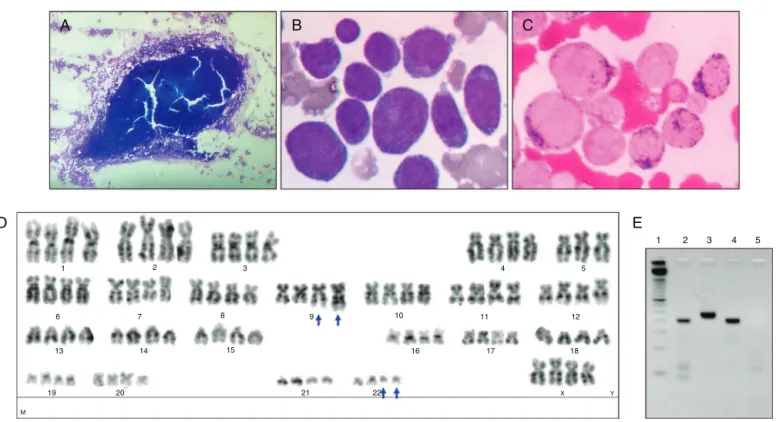
A 28-year-old woman presented with leukocytosis (white blood cell count47.8×109/L, myeloblasts 66%,
metamyelo-cytes 1%, neutrophil band 1%, segmented neutrophils 4%, lymphocytes28%),anemia(hemoglobin6.9g/dL),and throm-bocytopenia(33×109/L).Thepatienthadbeensufferingfrom
weakness and fatigue associated with febrile episodes for onemonth.Therewasnopastmedicalhistoryofany hema-tologicaldisorder.Physicalexaminationrevealed pallorand absence ofhepatomegaly andsplenomegaly. BMaspiration showedmyeloblastscomprising88%ofallcells(Figure2A–C). Theimmunophenotypicanalysisshowedthattheblastswere positiveforCD34,CD117,CD33,CD13,HLA-DR,CD38,CD11b, CD4, CD133, CD15,CD11c and CD64and negativefor CD7, CD56,CD19,CD41andNG2.Thepatientwasdiagnosedwith
de novo AML-NOS and classified as acute myelomonocytic leukemia according to WHO 2008 or AML with BCR-ABL1 according to WHO 2016. The cytogenetic analysis showed 92<4n>,XXXX,−4,−5,+6,−7,−11,+12,−13,−14,+15,−17,−21,
t(9;22)(q34;q11)x2[cp20] (Figure 2D) and a RT-PCR assay for
BCR-ABL1revealedap190isoform(e1a2BCR-ABL1)(Figure2E). The patient received two cycles of inductiontherapy with daunorubicin and cytarabine, associated with intrathecal chemotherapy (methotrexate, cytarabine and dexametha-sone).Atthesecondcycleofinduction,thepatientwasstarted on dasatinib. Thepatient achievedcomplete hematological remissionandreceivedmatchedrelatedmyeloablative allo-geneichematopoieticstemcelltransplantation.Atthetime ofthisreport,twentymonthsafterdiagnosis,sheremainsin completeremission.
Discussion
Herein,wedescribedthecharacteristicsoftwocasesofAML withBCR-ABL1. Althoughveryrare, thepresenceofthePh chromosomehasbeenreportedinsomeMDScasesat diagno-sisoratthetimeofdiseaseprogression,andbothBCR-ABL1
variants,p210andp190,havebeenpreviouslydescribed.9,14,15 Inacohortcontaining148patientswiththePhchromosome, Keungetal.9reportedonlytwocasesofdenovoAML(1%)and threecasesofMDS(2%).Fukunagaetal.14reportedacaseof MDSthatpresentedanabruptevolutiontoAML-MRCandthe acquisition ofthe Phchromosome(p210BCR-ABL1).Inthat report, thepatienthadhematological responsetonilotinib, whichwaslostwiththeacquisitionoftheBCR-ABL1Y253H mutation. Subsequently,thepatient hadtransient hemato-logicalresponsetodasatinib,butresponsewaslostwiththe acquisitionoftheBCR-ABL1T315IandE255Kmutations.
A
D
B
C
E
1
4 5
12 11
10
21 15
14
20 13
19
8 9
3 2
1
6 7
22
16 17 18
X M
Y
2 3 4 5
Figure2–Bonemarrowmorphological,cytogeneticsandmolecularanalysisofCase2.(A)Hypercellularbonemarrow fragment.(B)ThebonemarrowwasstainedbyWright-Giemsastainandahighfrequencyofmyeloblastswasobserved.(C) Thebonemarrowwasstainedbymyeloperoxidasestain.(D)Illustrativemetaphase:91<4n>,XXXX,−5,t(9;22)(q34;q11)x2.
Thet(9;22)(q34;q11.2)isindicatedwithbluearrows.(E)Polymerasechainreactionassayforb2a2/b3a2ande1a2BCR-ABL1
transcripts–1:ladder50basepairs(LifeTechnologies);2:Case#2;3:positivecontrolforb2a2/b3a2BCR-ABL1transcript
(p210);4:positivecontrolfore1a2BCR-ABL1transcript(p190);5:negativecontrolforb2a2/b3a2ande1a2BCR-ABL1
transcripts.
chromosomebandisinvolvedinmostcaseswith7qdeletions inMDSandAML.16,17Deletionofthelongarmofchromosome 20isacommonrecurringchromosomalabnormality associ-atedwithmyeloidmalignancies.18
In AML, the near-tetraploidy karyotype is a rare cyto-genetic alteration and its prognostic relevance is not well defined.19 Yamaguchi et al.15 reported a case of AML withBCR-ABL1whopresentedmetaphasecytogeneticswith 92,XXYY,t(9;22)(q34;q11)x2[20]andRT-PCRpositivityforp190
BCR-ABL1;thepatientachievedcompleteremissionafterthe firstcycleofinductionchemotherapyandwasconsolidated withallogeneichematopoieticstemcelltransplantation.15
Inconclusion,cytogeneticabnormalitiesidentifiedby kary-otypingremainanimportantprognosticfactorinAML.The report of these rare cases of AML with the presence of e2a1BCR-ABL1 and futureanalyses forthesealterations in AMLpatientsareimportanttodefinethelocalincidence,to improvediagnosisandclassification,andtobetterassessthe impactofthesemolecularalterationsontheoutcomesofAML patients.
Funding
ThisworkreceivedfinancialsupportfromConselhoNacional de Desenvolvimento Científico e Tecnológico (CNPq) and
Fundac¸ão de Amparo à Pesquisa do Estado de São Paulo (FAPESP).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
The authors would like to thank Andy Cumming for the English review,and Amélia Góes and ClaudiaHelena Mag-nanifortheirvaluabletechnicalassistancewithRT-PCRfor BCR-ABL1detection.
r
e
f
e
r
e
n
c
e
s
1.SwerdlowSH,CampoE,HarrisNL,JaffeES,PileriSA,SteinH, etal.WHOclassificationoftumoursofhaematopoieticand lymphoidtissues.4thed.Lyon:IARC;2008.
2.ArberDA,OraziA,HasserjianR,ThieleJ,BorowitzMJ,LeBeau MM,etal.The2016revisiontotheWorldHealthOrganization classificationofmyeloidneoplasmsandacuteleukemia. Blood.2016;127(20):2391–405.
4. DellaPortaMG,MalcovatiL,StruppC,AmbaglioI,Kuendgen A,ZippererE,etal.Riskstratificationbasedonbothdisease statusandextra-hematologiccomorbiditiesinpatientswith myelodysplasticsyndrome.Haematologica.2011;96(3):441–9. 5. DohnerH,EsteyEH,AmadoriS,AppelbaumFR,BuchnerT,
BurnettAK,etal.Diagnosisandmanagementofacute myeloidleukemiainadults:recommendationsfroman internationalexpertpanel,onbehalfoftheEuropean LeukemiaNet.Blood.2010;115(3):453–74.
6. MaciejewskiJP,TiuRV,O’KeefeC.Applicationofarray-based wholegenomescanningtechnologiesasacytogenetictoolin haematologicalmalignancies.BrJHaematol.
2009;146(5):479–88.
7. TiuRV,GondekLP,O’KeefeCL,HuhJ,SekeresMA,ElsonP, etal.Newlesionsdetectedbysinglenucleotide
polymorphismarray-basedchromosomalanalysishave importantclinicalimpactinacutemyeloidleukemia.JClin Oncol.2009;27(31):5219–26.
8. PaneF,IntrieriM,QuintarelliC,IzzoB,MuccioliGC,Salvatore F.BCR/ABLgenesandleukemicphenotype:frommolecular mechanismstoclinicalcorrelations.Oncogene.
2002;21(56):8652–67.
9. KeungYK,BeatyM,PowellBL,MolnarI,BussD,PettenatiM. Philadelphiachromosomepositivemyelodysplastic syndromeandacutemyeloidleukemia-retrospectivestudy andreviewofliterature.LeukRes.2004;28(6):579–86. 10.NeuendorffNR,BurmeisterT,DorkenB,WestermannJ.
BCR-ABL-positiveacutemyeloidleukemia:anewentity? Analysisofclinicalandmolecularfeatures.AnnHematol. 2016;95(8):1211–21.
11.ArberDA,OraziA,HasserjianR,ThieleJ,BorowitzMJ,LeBeau MM,etal.The2016revisiontotheWorldHealthOrganization
(WHO)classificationofmyeloidneoplasmsandacute leukemia.Blood.2016;127(20):2391–405.
12.NCCN,FortWashingtonNCCNClinicalPracticeGuidelinesin Oncology(NCCNGuidelines®):AcuteMyeloidLeukemia, Version1.2016;2016.
13.ShafferLG,McGowan-JordanJ,SchmidM.ISCN(2013):an internationalsystemforhumancytogeneticnomenclature. Basel:SKarger;2013.
14.FukunagaA,SakodaH,IwamotoY,InanoS,SuekiY,Yanagida S,etal.AbruptevolutionofPhiladelphia
chromosome-positiveacutemyeloidleukemiain
myelodysplasticsyndrome.EurJHaematol.2013;90(3):245–9. 15.YamaguchiH,InokuchiK,YokomizoE,MiyataJ,WatanabeA,
InamiM,etal.Philadelphiachromosome-positiveacute myeloidleukemiawithtetraploidy.IntJHematol. 2002;75(1):63–6.
16.LeBeauMM,EspinosaR3rd,DavisEM,EisenbartJD,Larson RA,GreenED.Cytogeneticandmoleculardelineationofa regionofchromosome7commonlydeletedinmalignant myeloiddiseases.Blood.1996;88(6):1930–5.
17.JohnsonEJ,SchererSW,OsborneL,TsuiLC,OscierD,MouldS, etal.Moleculardefinitionofanarrowintervalat7q22.1 associatedwithmyelodysplasia.Blood.1996;87(9):3579–86. 18.HuhJ,TiuRV,GondekLP,O’KeefeCL,JasekM,MakishimaH,
etal.Characterizationofchromosomearm20qabnormalities inmyeloidmalignanciesusinggenome-widesingle
nucleotidepolymorphismarrayanalysis.Genes ChromosomesCancer.2010;49(4):390–9.