w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Usefulness
of
early
colonoscopy
in
the
diagnosis
and
treatment
of
moderate
or
severe
lower
gastrointestinal
bleeding
Paulo
Correa
∗,
Carolina
Teixeira,
Rodrigo
R.
Zago,
Giulio
Rossini,
Jose
Luiz
Paccos,
Pedro
Popoutchi,
Jarbas
F.
Loureiro,
Jose
Luiz
Borges,
Marcelo
Averbach
HospitalSírioLibanês,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12July2016 Accepted14September2016 Availableonline28September2016
Keywords:
Lowergastrointestinalbleeding Colonoscopy
Endoscopictreatment Bowelprep
a
b
s
t
r
a
c
t
Atotalof38,686colonoscopieswereperformedbetweenJanuary1985andDecember2012 atHospitalSírio-Libanês,inSãoPaulo,Brazil.Twohundredthirty-fourpatients(0.6%)had acutelowergastrointestinalbleedingofmoderateorsevereintensity.Adefinitivediagnosis waspossiblein151cases,64.5%ofthesepatients.
ThisstudywasapprovedbytheInstitutionalReviewBoard.Medicalchartswerereviewed. Allexaminationsweredoneundersedationbythesamemedicalteam.
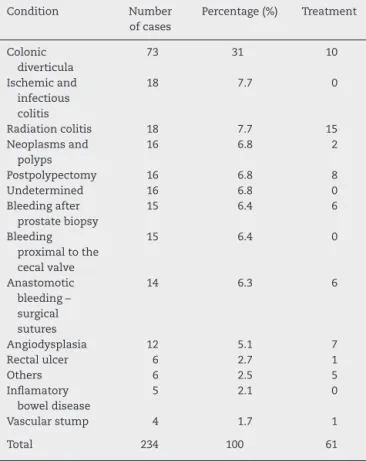
Thepredominantsourcesofbleedingwerecolonicdiverticula(73patients;31%),ischemic orinfectiouscolitis(18patients;7.7%)andradiationproctitis(18patients;7.7%).
Aspecifictherapeuticinterventionwasperformedon61ofthe151patientswhohadthe diagnosisconfirmed(40.4%),accordingtothesourceofbleeding.Mostpatientswith post-polypectomybleedingweretreatedwithinjectionofepinephrine(40%)andclipping(40%). Patientswithangiodysplasiaweretreatedpredominantlywithargonplasmacoagulation (42%).
Injectionofepinephrinewasthemostfrequenttreatment,regardlessofthesourceof bleeding(34.4%),followedbyargonplasmacoagulation(31.1%).
Controlofactivehemorrhagewasachievedendoscopicallyin98.8%ofthepatients. Ourdatashowsthatearlycolonoscopyinthemanagementofpatientswithsuspected acutelowergastrointestinalbleedingisausefultoolfordiagnosisandtreatment.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](P.Correa).
http://dx.doi.org/10.1016/j.jcol.2016.09.002
Utilidade
da
colonoscopia
precoce
no
diagnóstico
e
tratamento
do
sangramento
gastrointestinal
baixo
moderado
ou
grave
Palavras-chave:
Sangramentogastrointestinal baixo
Colonoscopia
Tratamentoendoscópico Preparac¸ãointestinal
r
e
s
u
m
o
Nototal,38.686colonoscopiasforamrealizadasentrejaneirode1985edezembrode2012no HospitalSírio-Libanês,emSãoPaulo,Brasil.234pacientes(0,6%)sofriamdesangramento gastrointestinalbaixoagudo(SGIBA)deintensidademoderadaougrave.Em151casos(64,5% dessespacientes)foipossívelestabelecerumdiagnósticodefinitivo.
OestudofoiaprovadopeloComitêdeRevisãoInstitucional.Osprontuáriosclínicosforam revisados.
Todososexamesforamrealizadoscomopacientesedadoepelamesmaequipeclínica. Asorigenspredominantesdesangramentoforamdivertículoscolônicos(73pacientes; 31%),coliteisquêmicaouinfecciosa(18pacientes;7,7%)eproctiteporradiac¸ão(18pacientes; 7,7%).
Umaintervenc¸ãoterapêuticaespecíficafoirealizadaem61dos151pacientescom diag-nósticoconfirmado(40,4%),deacordocomaorigemdosangramento.Emsuamaioria,os pacientescomsangramentopós-polipectomiaforamtratadoscominjec¸ãodeadrenalina (40%)eporclipping(40%).Ospacientescomangiodisplasiaforamtratados predominante-mentecomcoagulac¸ãocomplasmadeargônio(42%).
Otratamentomaisfrequentementeadministradofoiainjec¸ãodeadrenalina, indepen-dentementedaorigemdosangramento(34,4%),seguidapelacoagulac¸ãocomplasmade argônio(31,1%).
Ocontroledahemorragiaativafoiobtidoporviaendoscópicaem98,8%dospacientes. Nossosdadosrevelamqueousoprecocedacolonoscopianotratamentodepacientescom suspeitadeSGIBAéinstrumentoútilparaodiagnósticoetratamento.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Acutelowergastrointestinalbleeding(ALGIB)isstilla diag-nosticand therapeuticchallenge.Inclinicalpractice,ALGIB canbedefinedasanygastrointestinalbleedingofrecentonset (withinthelast12–24h)originatingbeyondtheileocecalvalve. Thisbleedingmayleadtosystemicmanifestations,suchas hemodynamic instability, anemia, and the need for blood transfusion.1 PatientswithALGIBpresentwithrectal
bleed-ing or melena, depending on the volume of bleeding and thespeedofcolonictransit.Insomepatients,theremaybe abdominalpainandhemodynamicinstability.Anemia char-acterizesmoreseverecases.Therearesomedatafromclinical history thatmay suggest the cause ofbleeding. For exam-ple, the use of aspirin or non-steroidal anti-inflammatory drugsisoftenassociatedwithALGIB,duemainlyto divertic-ulardisease,aswellaswithuppergastrointestinalbleeding (UGIB).Patientswithacutecolonicischemiausuallypresent rapidonsetofmildabdominalpainandtendernessoverthe affected bowel, most often involving the left side. Mild to moderateamountsofrectalbleedingorbloodydiarrhea usu-allydevelopwithin24hofthe onsetofabdominalpain.In patientswithahistoryofprostatecancerorcervicalcancer,it mayberelatedtoactinicproctitis,evenifirradiationpreceded thebleedingbymanyyears.Ahistoryofrecentpolypectomy shouldguidetheinvestigationofALGIBtowardthepointof resection.2
The clinical consequences of ALGIB are variable and dependentupontheintensityofthebleedingandonpatient baseline clinical conditions. About half ofpatients present anemia and hemodynamic compromise; however, these changes are less evident in patients with ALGIB than in thosewithUGIB.3StudiesdescribeclinicalpredictorsofALGIB
severity: heart rate >100beats/min, systolic blood pressure <100mmHg,activerectalbleedingduringthefirst4hof obser-vation,andinitialhematocrit<35%.4,5
TheincidenceofALGIBisestimatedat20casesper100,000 adults,whichrepresentsonequartertoonethirdofpatients hospitalized for gastrointestinal bleeding.6 However,ALGIB
morecommonlyaffectstheelderly,withanincidenceashigh as200per100,000ofthoseintheirninthdecadeoflife.The case-fatalityrateforpatientswithALGIBis3.6%andpatients withactivebleedingduringhospitalizationhaveahigherrisk ofdeath.7
Bleedingtendstobeself-limitedandtostopspontaneously in about 80% of cases.8 Once the bleeding stops
sponta-neously,electivecolonoscopyisindicated.Inthosepatients whokeepbleeding,thediagnosisshouldbedoneregardlessof thehemorrhage.Althoughcolonoscopyhasbeenconsidered impracticableduetothefrequentimpossibilityofcolon clean-ing,morerecentdatashowthatthisprocedureisfeasibleand allowsfordiagnosisinmostcases.9Colonoscopyhas
repeat-edlybeenshowntobesafe,effective,anduseful,especially whendoneinthefirst12–24hafteradmission.10Colonoscopy
diagnostic utility in identifying the source of ALGIB.10–12
The optimal timing for endoscopic examination has not been determined. However, recent data demonstrates that colonoscopyperformedwithinthefirst24hfromadmission mayresultinadefinitivediagnosisinupto96%ofpatients.13
TheaccuracyofcolonoscopyininvestigatingcasesofALGIB variesfrom 72%to86%,andcecalintubationisachievedin 95%ofthecases.8,14
Early reports of successful hemostasis in patients with diverticulardiseaseandnon-bleedingvisiblevessels encour-agedmore frequent use of this modality to treat ALGIB.15
A prospective study was conducted by Jensen et al. with 10patientswithsevereALGIBwhoweretreatedwith endo-scopicmaneuvers.They foundthatendoscopichemostasis wasachievedinall10patients,withnoepisodesofearly re-bleeding.At30monthsoffollow-up,noneofthepatientshad latebleeding.16Arecentreviewofallpublishedseriesfounda
lowcomplicationrate,aswellasalowrecurrencerate(<10%) inpatientstreatedwithendoscopicmethods.17
InthecourseofastudyontheprevalenceofALGIBinour practice,wehavealsoassessedtheroleofearlycolonoscopy astheprimarymethodofevaluationandtreatmentinthese patients.
Patients
and
methods
Patients were eligible for inclusion if they presented with hematochezia(redormaroonrectaloutput)andhadoneofthe followinghigh-riskfeatures: heartrate>100beats/min, sys-tolicbloodpressure<100mmHg,needofbloodtransfusionor dropinhemoglobin>1.5g/dlwithina6hperiod,accordingto informationfromthemedicalrecords.
A total of 38,686 colonoscopies were performed at our practiceduringtheperiodexaminedbythisstudy.Two hun-dred thirty-four patients (0.6%) had ALGIB of moderate or severeintensity.Amongthese234patients,adefinitive diag-nosiswaspossiblein151cases,64.5%ofthesepatients.
Allcolonoscopies wereperformedbetweenJanuary1985 andDecember2012intheendoscopyunitofHospital Sírio-Libanês,inSãoPaulo,Brazil.WedefinedpatientswithALGIB ofmoderateorsevereintensityasthosehavinglower gastroin-testinalbleedingofrecentonset(<6h).Ouranalysisreviewed themedicalchartsandcolonoscopyresultsofthesepatients retrospectively.Allpatientsweretreatedwithinthecontextof routinecare.Resuscitationwastobeperformedonallpatients withinstability(shock,orthostatichypotension)orevidence ofseverebleedingoractivebleedingandthesepatientswere thentobeadmittedtotheintensivecareunit.Volume expan-sionrequiredtwoperipheralvenousaccesscaliberorcentral venousaccess.Patients withheart failureorvalvularheart diseasemay havebenefitedfrom monitoringofpulmonary arterypressurewithaSwan-Ganzcatheter,minimizingthe riskofover-hydration.Upperendoscopy,ingeneral,ispartof theinitialapproachforthesepatients,especiallythosewith severebleeding,inordertoexcludeaproximalcauseofthe bleeding.
The study protocol was approved by the Institutional ReviewBoardofHospitalSírio-Libanês;writteninformed con-sentwasabsentduetotheretrospectivenatureofthestudy.
After clinical stabilization and an upper GI endoscopy withoutsignsofbleeding,thepatientsunderwentan antero-gradepreparationofthecolonwithamanitol(sorbitol)10% solution, receiving750–1500mlwithinaperiodof1–2h. All examinations were done under sedation performed by an anesthesiologist. All colonoscopies were performed by the samemedicalteam,usingOlympus(OlympusOpticalCo,Ltd., Tokyo,Japan)orFujinon(FujifilmCorporation,Tokyo,Japan) colonoscopes.
Patients’ demographic and clinical characteristics were tabulatedforanalysis,and95%confidenceintervals(CI)were constructedwhenappropriate.
Results
Of the 234 patients, 63.2% (148) were male, 33% (77)were femaleand3.8%wereunknown.Mostpatientswhopresented withALGIBwere70ormoreyearsold(47.4%;111)and18.4% were between60 and 69 yearsold (43).All patients under-wentcolonoscopyunderhospitalization;noneofthemwere outpatients.
All colonoscopies were performed within 6h after pre-sentation at the hospital. Concerning bowel preparation, 66.7%(156) weredonewithmanitolsolutionand22.2%(52) underwent retrogradepreparation.Accordingtothe Boston preparationscale,67.5%(158)wereclassifiedashavinggood preparationand9.4%(22)ashavinginappropriatepreparation. Theileumwasreachedinall patientsinwhomadistal sourceofbleeding, suchasbleedingduetoanastomosisor diverticulableedingfrom theleft colon,was notidentified. Thepredominantsourcesofbleedingwerecolonicdiverticula (73patients;31%),followedbyischemicorinfectionscolitis(18 patients;7.7%)andradiationcolitis(18patients;7.7%).Other causesobservedarelistedinTable1.Aspecifictherapeutic intervention wasperformedon 61ofthe 151patientswho hadthediagnosisconfirmed(40.4%),accordingtothe under-lyingsourceofbleeding(Table2).Suchinterventionsincluded electrocauterization,endoscopicepinephrineinjection,argon plasmacoagulation(APC),mechanicalclippingandlaser.Most patients with postpolypectomy bleeding were treated with injection of epinephrine (40%) and clipping (40%). Patients withangiodysplasiaweretreatedpredominantlywithargon plasmacoagulation(42%).Injectionofepinephrinewas the mostfrequenttreatment,regardlessofthesourceofbleeding (34.4%),followedbyargonplasmacoagulation(31.1%).Control ofactivehemorrhagewasachievedendoscopicallyin98.8% ofthepatientswhounderwentatherapeuticmethod.Only onepatient,whopresentedwithALGIBsecondarytocolonic diverticula,didnothavesuccesswithendoscopictreatment (epinephrineinjection)andwasreferredtosurgery.
Discussion
Table1–Mainsourceofbleedingfoundatcolonoscopy.
Condition Number
ofcases
Percentage(%) Treatment
Colonic diverticula
73 31 10
Ischemicand infectious colitis
18 7.7 0
Radiationcolitis 18 7.7 15
Neoplasmsand polyps
16 6.8 2
Postpolypectomy 16 6.8 8
Undetermined 16 6.8 0
Bleedingafter prostatebiopsy
15 6.4 6
Bleeding proximaltothe cecalvalve
15 6.4 0
Anastomotic bleeding– surgical sutures
14 6.3 6
Angiodysplasia 12 5.1 7
Rectalulcer 6 2.7 1
Others 6 2.5 5
Inflamatory boweldisease
5 2.1 0
Vascularstump 4 1.7 1
Total 234 100 61
treatmentcosts,aswellasimprovethediagnosisofthesource ofbleeding.2,9Colonoscopythusseemstobeoneofthebest
therapeuticoptionsfordiagnosis ofALGIBandlocalization ofbleedingsources. Althoughurgentcolonoscopypresents arecurrence rate ofearlyre-bleeding ranging from 15% to 22%,thismethodhastheadvantageofbeingpotentially ther-apeutic,asthediagnosisratevariesfrom60%to97%inthe literature.18,19
Identificationofthebleedingsourceremainsadiagnostic challenge.Approximately10%ofallpatientswillneverhave asourceidentifiedandupto40%ofpatientswithALGIBhave morethan onepotential bleedingsource.10,20 Inour study,
35.4%ofthepatients(83patients)hadnosourceofbleeding identifiedbeforecolonoscopy.
Accordingtothe literature,themainsourceofALGIBis diverticulosis.1Themajority(>75%)ofcolonicdiverticulaare
foundinthe leftcolon; usingcolonoscopy, 60%ofcasesof diverticulableedingcanbeobservedonthissideofthecolon.7
Inourstudy,diverticulableedingwasthemostfrequentcause ofALGIB,followedbyischemicandinfectiouscolitis.
Bleeding after prostate biopsy is a significant cause of ALGIBinourpractice(6.4%),astheUrologyCenterexcelsin thediagnosisandtreatmentofprostatecancer.
Elderly patientsare mostlikely toexperience ischemia-related colitis because of underlying risk factors such as relativehypotension,heartfailure,andarrhythmias–all clin-icalcharacteristicsofpatientswithheartdisease.
Postpolypectomybleeding isanother frequent sourceof ALGIBinthe literature, and hasbeen foundto occur after 0.2–1.8% of colonoscopic polypectomies.21,22 In regard to
Table2–Maintherapeuticmethods.
Epinephrineinjection
Diverticularbleeding 8
Postpolypectomy 4
Anastomoticbleeding 2
Afterprostatebiopsy 3
Vascularstump 2
Radiationcolitis 1
Angiodysplasia 1
21(34.4%)
APC
Radiationcolitis 13
Angiodysplasia 3
Postpolypectomy 1
Anastomoticbleeding 1
Neoplasmsandpolyps 1
19(31.14%)
CLIP
Afterprostatebiopsy 4
Postpolypectomy 4
Anastomoticbleeding 3
Neoplasmsandpolyps 2
Vascularstump 1
Rectalulcer 1
15(24.6%)
Esclerosis
Angiodysplasia 3
Radiationcolitis 1
Post-elasticbandligation 1
5(8.2%)
Laser
Radiationcolitis 2
2(3.3%)
Non-specifiedtreatment
Diverticularbleeding 2
Vascularstump 1
Afterprostatebiopsy 1
Postpolypectomy 1
Perforatinglesionofthecolon 1
Other 1
7(11.5%)
angiodysplasias,ourdataiswithintherangecitedinthe lit-erature(approximately4.5%)12asasourceofALGIB.
ThemanagementofALGIBisnotstandardized.Although thereareseveralstrategiesforthediagnosisandtreatmentof patientswithALGIB,webelievethatcolonoscopywithin6h afterpresentationcanbeperformedsafelywithahighrateof successinidentifyingandoftentreatingthespecificcauseof bleeding.Withthecontinuedadvancesinendoscopic technol-ogy,colonoscopyhasbecomenotonlyadiagnosticbutalsoa usefultherapeutictoolinthemanagementofALGIB.
collectedfromthelast26years;inthepast,onlyepinephrine injectionormonopolarcoagulationwereavailable,butasthe risk of perforation was too high with monopolar coagula-tion,epinephrineinjectionwasthepreferredoption.Recently, there has been a preference for mechanical methods of hemostasis, such as the use of metal clips. Data on the recurrence rate of bleeding after endoscopic therapy are inconsistent:Jensenetal.16observednorecurrence,whereas
Bloomfeld et al.23 reported an early recurrence in 38% of
patients.Onlyonepatientinourseries,intheendoscopically treatedgroup,relapsedandwasreferredtosurgery.
Thediagnosticyieldforurgentcolonoscopywithregardto ALGIBisreportedintheliteratureas48–90%.6,12
Two publications report diagnostic yields of 89–97%11,24
which perhaps is a reflection of more consistent use of urgent colonoscopy. Two other studies demonstrated that earlycolonoscopyissignificantlyassociatedwith ashorter hospitalstay.4,25Inmoststudies,earlycolonoscopyisdefined
asbeingdonewithin12–24hofadmission.Somephysicians performcolonoscopyonanunprepared bowelasbloodisa laxativeand thelocationofblood inthe coloncanprovide informationaboutthebleedingsite.Chaudhryetal.11showed
that, in patients withALGIB, a high diagnostic yield (97%) and effective hemostasis could be obtained even without bowelpreparation.Theywereabletocontrolactivebleeding in17of27patients(63%)byendoscopicintervention. How-ever,currentrecommendations13advisecleansingthecolon
asthoroughlyaspossibleinALGIB,asthisimprovesthe eval-uationofthe mucosa, which inturn enhances recognition ofsmaller lesionsand minimizesthe riskofcomplications resulting from poor visualization. Bowel cleansing is usu-allyperformedwithanelectrolytesolution(manitolsolution inourstudy).Theendoscopistshouldattempttoreachthe caecumwheneverpossible.Thisisimportantbecausea sub-stantialproportionofbleedingsitesarelocatedintheright colon.Inaddition,theendoscopistshouldtrytointubatethe terminalileum.Flowingblood fromaboveisaclear indica-tionofamoreproximalbleedingsite.Ohyamaetal.24report
thatevenunderconditionsofurgentcolonoscopy,the cae-cumwasinspectedin56%ofpatients,andthatterminalileum insertionwasachievedin27%.Fordiagnosinghaemorrhoidal bleedingitisimportanttoinspecttheanaltransitionalzone witha retroflexed instrument and to perform proctoscopy (anoscopy).
Thesecond aimofcolonoscopyin casesofacute lower bleedingshouldbetoidentifypatientswithactivebleeding orwithariskofre-bleeding.Byanalogywithendoscopicrisk stratificationinbleedingulcers,Jensenetal.16 haveshown
thatevidenceofactivebleeding,visiblevessels,and adher-entclotsisassociatedwithaseverecourseorahigherrate ofre-bleeding.Diagnosticinterventionsaloneareunlikelyto altersignificantoutcomessuchasre-bleedingandneedfor surgery.However,stigmataareinfrequentlyidentifiedinthe colon.Studies reportstigmata ofhemorrhagein7.7–43%of cases.26
Webelievethatourdatalendsfurthersupporttotheroleof earlycolonoscopyinthemanagementofpatientswithALGIB; thisprocedureallowsforaspecificdiagnosisandappropriate treatmentinatleasttwo-thirdsofpatientswithsuspected ALGIB.Theretrospectivenatureofourclinicalseriesonthis
topic allowsfortheassessmentofthetrueimpactof com-monlyutilizedinterventions,suchascolonoscopy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BarnertJ,MessmannH.Diagnosisandmanagementoflower gastrointestinalbleeding.NatRevGastroenterolHepatol. 2009;6:637–46.
2.BoundsBC,KelseyPB.Lowergastrointestinalbleeding. GastrointestEndoscClinNAm.2007;17:273–88,vi.
3.PeuraDA,LanzaFL,GostoutCJ,FoutchPG.TheAmerican CollegeofGastroenterologyBleedingRegistry:preliminary findings.AmJGastroenterol.1997;92:924–8.
4.StrateLL,SyngalS.Timingofcolonoscopy:impactonlength ofhospitalstayinpatientswithacutelowerintestinal bleeding.AmJGastroenterol.2003;98:317–22.
5.VelayosFS,WilliamsonA,SousaKH,LungE,BostromA, WeberEJ,etal.Earlypredictorsofseverelower
gastrointestinalbleedingandadverseoutcomes:a
prospectivestudy.ClinGastroenterolHepatol.2004;2:485–90.
6.DavilaRE,RajanE,AdlerDG,EganJ,HirotaWK,LeightonJA, etal.ASGEguideline:theroleofendoscopyinthepatient withlower-GIbleeding.GastrointestEndosc.2005;62:656–60.
7.LongstrethGF.Epidemiologyandoutcomeofpatients hospitalizedwithacutelowergastrointestinalhemorrhage:a population-basedstudy.AmJGastroenterol.1997;92:419–24.
8.EdelmanDA,SugawaC.Lowergastrointestinalbleeding:a review.SurgEndosc.2007;21:514–20.
9.EltaGH.Urgentcolonoscopyforacutelower-GIbleeding. GastrointestEndosc.2004;59:402–8.
10.CaosA,BennerKG,ManierJ,McCarthyDM,BlessingLD, KatonRM,etal.ColonoscopyafterGolytelypreparationin acuterectalbleeding.JClinGastroenterol.1986;8:46–9.
11.ChaudhryV,HyserMJ,GraciasVH,GauFC.Colonoscopy:the initialtestforacutelowergastrointestinalbleeding.AmSurg. 1998;64:723–8.
12.ZuckermanGR,PrakashC.Acutelowerintestinalbleeding. PartII.Etiology,therapy,andoutcomes.GastrointestEndosc. 1999;49:228–38.
13.StrateLL.LowerGIbleeding:epidemiologyanddiagnosis. GastroenterolClinNAm.2005;34:643–64.
14.BoundsBC,FriedmanLS.Lowergastrointestinalbleeding. GastroenterolClinNAm.2003;32:1107–25.
15.SavidesTJ,JensenDM.Colonoscopichemostasisforrecurrent diverticularhemorrhageassociatedwithavisiblevessel:a reportofthreecases.GastrointestEndosc.1994;40:70–3.
16.JensenDM,MachicadoGA,JutabhaR,KovacsTO.Urgent colonoscopyforthediagnosisandtreatmentofsevere diverticularhemorrhage.NEnglJMed.2000;342:78–82.
17.PilichosC,BobotisE.Roleofendoscopyinthemanagementof acutediverticularbleeding.WorldJGastroenterol.
2008;14:1981–3.
18.GreenBT,RockeyDC,PortwoodG,TarnaskyPR,GuariscoS, BranchMS,etal.Urgentcolonoscopyforevaluationand managementofacutelowergastrointestinalhemorrhage:a randomizedcontrolledtrial.AmJGastroenterol.
2005;100:2395–402.
19.LaineL,ShahA.Randomizedtrialofurgentvs.elective colonoscopyinpatientshospitalizedwithlowerGIbleeding. AmJGastroenterol.2010;105:2636–41.
21.KimHS,KimTI,KimWH,KimYH,KimHJ,YangSK,etal.Risk factorsforimmediatepostpolypectomybleedingofthecolon: amulticenterstudy.AmJGastroenterol.2006;101:1333–41.
22.ConsoloP,LuigianoC,StrangioG,ScaffidiMG,GiacobbeG,Di GiuseppeG,etal.Efficacy,riskfactorsandcomplicationsof endoscopicpolypectomy:tenyearexperienceatasingle center.WorldJGastroenterol.2008;14:2364–9.
23.BloomfeldRS,RockeyDC,ShetzlineMA.Endoscopictherapy ofacutediverticularhemorrhage.AmJGastroenterol. 2001;96:2367–72.
24.OhyamaT,SakuraiY,ItoM,DaitoK,SezaiS,SatoY.Analysis ofurgentcolonoscopyforlowergastrointestinaltract bleeding.Digestion.2000;61:189–92.
25.SchmulewitzN,FisherDA,RockeyDC.Earlycolonoscopyfor acutelowerGIbleedingpredictsshorterhospitalstay:a retrospectivestudyofexperienceinasinglecenter. GastrointestEndosc.2003;58:841–6.