w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Perceptions
of
ostomized
persons
due
to
colorectal
cancer
on
their
quality
of
life
Cristilene
Akiko
Kimura
a,b,∗,
Ivone
Kamada
c,
Dirce
Bellezi
Guilhem
c,
Karina
Ribeiro
Modesto
b,
Breno
Silva
de
Abreu
baUniversidadedeBrasília(UnB),Brasília,DF,Brazil
bFaculdadedeCiênciaseEducac¸ãoSenaAires(Facesa),ValparaísodeGoiás,GO,Brazil
cUniversidadedeBrasília(UnB),FaculdadedeCiênciasdaSaúde,ProgramadePós-Graduac¸ãoemEnfermagem,Brasília,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received19April2016 Accepted7May2016 Availableonline12July2016
Keywords: Qualityoflife Ostomy
Colorectalneoplasms
a
b
s
t
r
a
c
t
Introduction:Thesignificanceofthechangeinthephysicalbodyandsufferingasthenew conditionoflifeofstomaoncologicalpersonaffectthephysical,psychological,social rela-tionshipsandenvironment.
Objective:Toknowtheperceptionofqualityoflifeandtheinterpretationofthe biopsy-chosocialrealityofintestinalostomyduetocolorectalcancerclinicsoftheAmbulatory CareProgramostomypatientsoftheHealthSecretariatoftheFederalDistrict,Brazil. Methods:Epidemiological basedstudy,analyticalcharacter,withcross-sectional descrip-tivedesignwithquantitativeandqualitativeapproachinthelightofthecontentanalysis. Sampleconsistedofconvenience,included120participants.Theyusedthequestionnaires sociodemographic,clinical,andWHOQOL-BREFandanindividualinterview.Datawere ana-lyzedbyMicrosoftOfficeExcel2010andSPSS20.0software.Statisticalsignificancewas acceptedat5%.
Results:PhysicalDomains,SocialAffairsandEnvironmentarecorrelatedwiththemean score,statisticallysignificant(p<0.0001),thecontentanalysisresultedinfourcategories: WellnessPhysical,PsychologicalWellness,WellnessandSpiritualWelllivingSocial. Conclusion: Ostomyandcolorectalcancermayrepresentsufferedmutilation,lossof produc-tivecapacityresultinginthelossofqualityoflife.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](C.A.Kimura). http://dx.doi.org/10.1016/j.jcol.2016.05.007
Percepc¸ões
das
pessoas
estomizadas
intestinais
em
razão
do
câncer
colorretal
sobre
a
qualidade
de
vida
Palavras-chave: Qualidadedevida Ostomia
Neoplasiascolorretais
r
e
s
u
m
o
Introduc¸ão: Osignificadodaalterac¸ãonocorpofísicoeosofrimentoquantoànovacondic¸ão devidadapessoaoncológicaestomizadaafetamosaspectosfísico,psicológico,relac¸ões sociaisemeioambiente.
Objetivo: Conhecerapercepc¸ãodaqualidadedevidaeainterpretac¸ãodarealidade biop-sicossocialdeestomizadosintestinaisemrazãodocâncercolorretaldosambulatóriosdo ProgramadeAssistênciaAmbulatorialdoEstomizadodaSecretariadeSaúdedoDistrito Federal,Brasil.
Métodos: Estudodebaseepidemiológica,decaráteranalítico,comdelineamento transver-saledescritivo,comabordagemquantitativaequalitativaàluzdaanálisedeconteúdo. Amostrafoiconstituídaporconveniência,incluídos120participantes.Utilizou-seos ques-tionáriossóciodemográfico,clínico,eoWHOQOL-brefeumaentrevistaindividual.Osdados foramanalisadospelosprogramasMicrosoft®OfficeExcel2010eSPSS20.0.Asignificância estatísticaaceitafoide5%.
Resultados: OsDomíniosFísico,Relac¸õesSociaiseMeioAmbienteestãocorrelacionadas comoescoremédio,significânciaestatística(p<0,0001),aanálisedeconteúdoresultouem quatrocategorias:BemEstarFísico,BemEstarPsicológico,BemEstarEspiritualeBemEstar Social.
Conclusão:Aestomiaintestinaleocâncercolorretalpodemrepresentaramutilac¸ãosofrida, aperdadacapacidadeprodutivaresultandonoprejuízodaqualidadedevida.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
TheWorldHealthOrganizationdefinesqualityoflifeas“the individual’sperceptionofhis/herpositioninlifeinthe con-textofthecultureandvaluesystemsinwhichhe/shelives andinrelationtohis/hergoals,expectations,standards,and concerns”.1Fromthisperspective,qualityoflifeisasubjective
conceptthatbringspersonalsatisfactioninvariousaspects, especiallythoseconsideredbasicforthelifeoftheindividual. Themaintenanceofthephysicalintegrityisextremelyvital forthepersontofeelgoodabouthim/herselfandhis/hersocial life.Inthissense,thediscontinuationofthisintegrity,likea surgeryforastomaduetocolorectalcancer,canresultin seri-ousproblemsforphysical,psychological,socialandspiritual well-being.2,3
Thus, the ostomized person, although resisting against cancer,isfacedwithchangesinhis/herbodyimage,withlow self-esteem,adesireofrejectionandchangesindaily activi-ties,whicharefactorsthathindertheprocessofacceptance ofarealityuntilthenunknown,compromisingthequalityof life.3–5
Thisstudyaimedtoacknowledgetheperceptionof qual-ity oflife and the interpretation ofbiopsychosocial reality ofthe ostomizedperson duetocolorectal cancerin outpa-tientclinicsoftheAmbulatoryCareProgramforOstomized Patients of the Health Department, Federal District (DF), Brazil.
Material
and
methods
Studymethodology
This is an analytical, cross-sectional, descriptive, epidemiological-based studywith aquantitativeand quali-tativeapproach,inlightofthecontentanalysis.Participants includedinthestudybelongedtoagroupofpeoplewitha stoma dueto colorectalcancer. Theobservation and mea-surementofthevariablesofinterestwerecarriedoutatthe sametime,constitutingastatisticalsnapshotofwhatoccurs atagiventime.
Thedataobtainedwiththeinterviewswereanalyzedbased ontheBardinContentAnalysis,whichisbasedonthephase ofmaterialdescriptionorpreparation,inferenceordeduction, andinterpretation.6
ThestudyprotocolwasapprovedbytheResearchEthics CommitteeoftheFundac¸ãodeEnsinoePesquisaem Ciên-ciasdoSaúde,HealthDepartment,DF,Brazil,underProtocol 418/200.Peoplewhoagreedtoparticipateinthestudysigned theFreeandInformedConsentformafterreceivingdetailed explanationsoftheproposedobjectivesandprocedures.The confidentialityofthesourceofdataandtheanonymityofthe volunteerswereguaranteed,asstatedinBrazilianregulations forresearchinvolvinghumansubjects.7Inordertorespectthe
Cases
Thiswasaconveniencesample,takingintoaccountthe spon-taneousdemandforparticipationinthestudy.120patients ostomized due to colorectal cancer and registered in the AmbulatoryCareProgramforPatientsOstomizedoftheHealth Department,DF,Brazil,wereincluded.
Theinclusion criteriawere:patientswithadiagnosis of colorectalcancerwithasurgeryforcreationofanostomy,aged >20 years. Children, adolescents,pregnant women, breast-feedingmothers, bedridden individuals, people with other disabilities,andthosewhorefusedtoparticipateinthestudy wereexcluded.
Datacollection
Data were collected from March2010 toAugust 2012. Two instrumentswereused:asociodemographicandclinical ques-tionnaire,andWHOQOL-BREF,initsversionvalidatedforthe Portuguese, which consistsof 26 items: two questions are generalandrefertotheperceptionofqualityoflifeand satis-factionwithhealth.Thefourdomains(Physical,Psychological, SocialRelationshipsandEnvironment)wereobserved.8
Thedatacollectionbasedontheinterviewswasanalyzed based on the Bardin Content Analysis,6 which began by a
study-drivingquestion:“Tellmeaboutwhatmeanstobean ostomizedpeople.”Followingeachnarration,theinterviews weretranscribedverbatim.Thereadingofthespeecheswas heldinitsentiretyseveraltimesandatvariousoccasions,to makeitpossibletounderstandthespeechesandtoidentify centralideasand keywords,withtheobservationof repeti-tionsandsimilaritiesamonginterviews.Thenextstagewas thatofstatementclipping,inordertobeginthecategorization.
Statisticalanalysis
Adescriptive statisticalanalysis ofdataobtainedfrom the socio-demographic and clinical questionnaires was carried out,inaddition to theinterview. Data from the WHOQOL-brefquestionnairewere analyzed bycalculating the mean, standarddeviationandproportionsandaninferential anal-ysisthroughthefollowingstatisticalprocedures:aconfidence intervalof95%,theStudent’st-test,andthelinearcorrelation coefficientofPearson.
ThestatisticalanalysiswasperformedwithSPSSsoftware (StatisticalPackagefortheSocialSciences,SPSSInc.,Chicago, USA)forWindowsversion20.0,asrecommendedbytheWorld HealthOrganization.Statisticalsignificancewasacceptedat 5%.
Results
Amongthe120ostomizedparticipants(duetocolorectal can-cer)in this study,it wasobserved that the mean age was 58.72±12.56 years, and most participants belonged to the 50–59-yearagegroup(n=35,29.2%). Ahigherprevalenceof females,representedby53.3%(n=64),wasobserved.
A predominance of the Catholic religion was observed, 56.7% (n=68); taking into account other sociodemographic
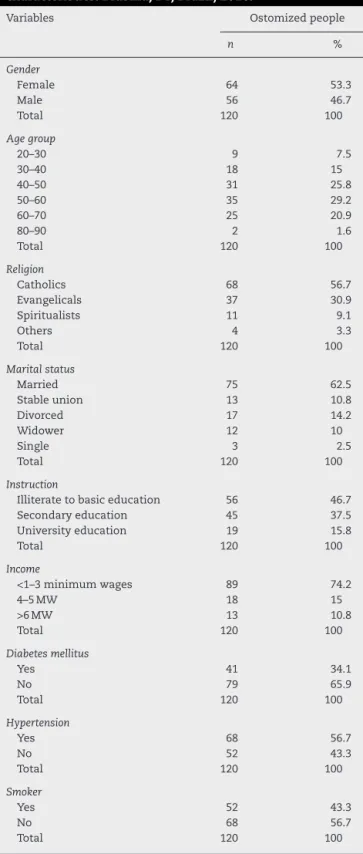
Table1–Sampleofostomizedpersonsduetocolorectal cancer,accordingtosociodemographicandclinical characteristics.Brasilia,DF,Brazil,2016.
Variables Ostomizedpeople
n %
Gender
Female 64 53.3
Male 56 46.7
Total 120 100
Agegroup
20–30 9 7.5
30–40 18 15
40–50 31 25.8
50–60 35 29.2
60–70 25 20.9
80–90 2 1.6
Total 120 100
Religion
Catholics 68 56.7
Evangelicals 37 30.9
Spiritualists 11 9.1
Others 4 3.3
Total 120 100
Maritalstatus
Married 75 62.5
Stableunion 13 10.8
Divorced 17 14.2
Widower 12 10
Single 3 2.5
Total 120 100
Instruction
Illiteratetobasiceducation 56 46.7
Secondaryeducation 45 37.5
Universityeducation 19 15.8
Total 120 100
Income
<1–3minimumwages 89 74.2
4–5MW 18 15
>6MW 13 10.8
Total 120 100
Diabetesmellitus
Yes 41 34.1
No 79 65.9
Total 120 100
Hypertension
Yes 68 56.7
No 52 43.3
Total 120 100
Smoker
Yes 52 43.3
No 68 56.7
Total 120 100
variables,astomaritalstatus,marriedpeopleprevailed,62.5% (n=75). Withregard toformal education,46.7%(n=56) had completed elementary school. As formonthly income, the mostoftenreportedbythe participants,4.2%(n=89), stood intherangeof1–3minimumwages.
Table2–MeanscoresofdomainsandqualityoflifeofWHOQOL-BREFforostomizedpersonsduetocolorectalcancer, Brasilia,DF,Brazil,2016.
Ostomizedpeopleduetocolorectalcancer
Domains n Mean SD CI95% p-Value
Physical 120 12.06 2.48 11.61–12.51 <0.0001
Psychological 120 12.40 2.94 11.87–12.93 <0.0001
Socialrelationships 120 12.64 2.97 12.10–13.18 <0.0001
Environment 120 12.22 2.43 11.78–12.66 <0.0001
Generalqualityoflife 120 12.26 2.28 11.85–12.67 <0.0001
weresmokers.Allvariablesofthesocio-demographicand clin-icalquestionnairearelistedinTable1.
Table2liststhestatisticallysignificantdifferencesinthe meanscoresforthedomains:Physical,Psychological,Social Rela-tionships,andEnvironment,andqualityoflifeingeneral,with statisticalsignificance(p<0.0001).
TheresultsshowninTable3indicatethattheostomized group due tocolorectal cancer had affected subcategories, namely:negativesubcategory–physicalstrength(p≤0.0001), andnegativesubcategory–sexualactivity(p≤0.0001),aswell asthecategorySocialWell-Being.
Table4listsfourcategories,namely:PhysicalWell-Being, Psy-chologicalWell-Being,SpiritualWell-Being,andSocialWell-Being; positiveandnegativesubcategoriesarelistedinTables4and5.
Discussion
Themeanage was58.72±12.56years.Studies indicatethe prevalenceofcolorectalcancerintheagegroupover50years, notingthatmorethan90%ofthesecancersoccurin individ-ualsagedover50.3,4 Inrelationtogender,womenprevailed,
whichisinlinewiththestudiesconductedbytheNational CancerInstituteinBrazil.9
Astoreligion,Catholicsprevailed,56.7%(n=68),followed byevangelicalcults,30.9%(n=37);77.5%(n=93)ofparticipants practicedsomereligion.Studiesshowthat,inthepresenceof illness,thereligiousinvolvementmayleadtospiritualgrowth sinceitinducesthepersontomeditateonhis/herfragilityand proximitytohumanfinitude.4,5
Regarding the variable “marital status,” 62.5% (n=75) of participants were married, and 10.8% (n=13) held a stable union.Thisresultshowsthat,regardlessofmarital classifi-cation,beingmarriedisaprotectivefactorforthesepeople. Inaddition, studiesindicate thatmarriedindividualsenjoy higherlevelsofphysicalandpsychologicalwell-beingversus unmarried,separatedordivorcedpeople.4,10–12
Regardingeducation andmonthlyfamily income,itwas observedthat the participantshad little formal education, whichrestrictstheinsertionopportunitiesinthelabor mar-ketandreflectsthelowwagesreceived(mean,2.25minimum wages).
Withregardtocomorbidities,itwasobservedthat,inmost cases,the participantssufferedfrom diabetes mellitusand hypertension.Theassociationofthesediseases contributes tothehighriskofdevelopingcolorectalcancer.4,10,12In
addi-tion,43.3%(n=52)ofparticipantsweresmokers.Althoughthe colonisnotdirectlyaffectedbythetobaccocompositionand bythosecarcinogenicsubstancescarriedbythebloodstream,
thishasanegativeimpactasregardstheriskofdeveloping colorectalcancer.3,4,13
Themean scores ofthe domains andfor qualityoflife of the WHOQOL-bref, listed in Table 2, give proof of sta-tistically significantdifferences inmeanscoresforPhysical, Psychological,SocialRelationships,andEnvironmentdomains,and
Table3–Distributionofcategorizationsofreportsfrom ostomizedpeopleduetocolorectalcancer,Brasilia,DF, Brazil,2016.
Subcategories Ostomizedpeopledue
tocolorectalcancer (n=120)
Physicalwell-being Negative
Leakage,odor,andgasses 74.1%(25.9%)
Physicalstrength 74.5%(25.5%)
Complicationswiththeostomy 65%(35%)
Sleep 60%(40%)
Positive
Familysupport 90.83%(9.17%)
Careprocessinhealth 51.67%(48.33%) Psychologicalwell-being
Negative
Self-concept 64%(36%)
Stigma 55%(45%)
Self-care 65%(35%)
Positive
Familysupport 63%(37%)
Acceptanceandadaptation 66%(34%)
Socialwell-being Negative
Personalrelationships 53.4%(46.6%)
Recreational/sportsactivities 58%(43%)
Socialisolation 52%(48%)
Sexualactivity 73%(27%)
Positive
Familyandfriends’support 68%(32%)
Companionship 59%(41%)
Spiritualwell-being Negative
Indifference 12%(88%)
Religiousness 12%(88%)
Positive
Religiousness 68%(32%)
Table4–Distributionofthecategorizationsphysicalandpsychologicalwell-beingofostomizedpeopleduetocolorectal cancer,Brasilia,DF,Brazil,2016.
Ostomizedpeopleduetocolorectalcancer
Category:PhysicalWell-being Category:PsychologicalWell-being
Subcategory Report Subcategory Report
Negative
Leakage,odorand gases
“WhenIgooutIhaveaconcerntotakeabag, becausesometimesIcanuseitasmybag alreadyleaked...so,imaginethesmell.The
gasesarealsoveryworrying[...].”(Azalea).
Self-concept “Iamabodywithoutapart,Iamnotlike otherpeople[...](cries).Ihavetolivewithit
anditishard(cry).”(Camellia).
Physicalstrength “Mylifechangedalotafterthatbag,Ihaveno strength[...]Icannotworknordomy
homeworkservices[...].”(Angelica).
Self-care “Atfirstitwasverydifficult,mywifehelped mechangethebag,Ialwaysdependedonher, nowIcleanandexchangethebag,butIstill feeldifficult.”(Pacova).
Complicationsof ostomy
“Ihadalotofirritationonmyskin[...].”(Liz
Flower).
Stigma “Thisistheworstfeelingthatapersoncan feel,thatis,thatpeopledonotwantyou around.”(Tulip).
Sleep “Ihadgreatdifficultywithsleep.”(Palmtree). Acceptanceand adaptation
“Iacceptedit.Itisbettertolivewiththisbag thandiefromcancer[...].”(Orchid).
Positive
Familysupport “ThankGodIdidnothaveanytrouble,andI hadandhaveagreatfamilysupport.” (Jacinto).
Familysupport WithoutmywifeInevercouldlivewiththat bag,shehelpstocleanitup[...].”(Aloe).
Careprocessin health
“Theoutpatientclinicnurseguidesmehowto takecareofthebag,andithelpsme[...].”
(Lavender).
Acceptanceand adaptation
“Iacceptedit.Itisbettertobewiththisbag thandiefromcancer[...].”(Orchid).
inthemeanscoreforqualityoflifeingeneral.Studiesonthe qualityoflifeofoncologicalostomizedpatientsindicatethat thecreationoftheostomyisacauseofadulterationofthe physicalbodyandofsufferingastothenewlifestyle,which affectsthePhysical,Psychological,SocialRelationships,and Envi-ronmentdimensions,thereforeaffectingthequalityoflife.14,15
InanalyzingtheresultsofTable3,thestudyparticipants reportedthat,proportionally,thesubcategoryphysicalstrength fromthecategoryPhysicalWell-Being,andthesubcategory sex-ualactivityfromthecategorySocialWell-Beingarenegatively compromised, especially forfemale subjects agedbetween 40 and60 years.These findingswere confirmedinanother
Table5–DistributionofcategorizationsSpiritualWell-beingandSpiritualWell-beingofostomizedpeopledueto colorectalcancer,Brasilia,DF,Brazil,2016.
Ostomizedpeopleduetocolorectalcancer
Category:SpiritualWell-being Category:SocialWell-being
Subcategory Report Subcategory Report
Negative
Indifference “I’mstillthesameperson.”(Violet) Personal relationships
“Ifeelveryashamedoffamilyandfriends,the colostomybag,donotleavemeatease.”(Ipe). Religiosity “Godwillhealme,I’msureIwillnotneedthe
ostomytreatment.”(Acacia).
Social,
recreationaland sportsactivities
“Icannottravelbybusbecauseofthebag.I amveryconcernedaboutthebag.”(Begonia).
Socialisolation “Ihadmanydifficulties,andtheworseitwas thechangeinmylife,nowIdonotliketogo out.”(Narcissus).
Sexualactivity “Mysexuallifechangedalot[...]Ifeelthat
myhusbandtouchesmeandlooksatme differently.”(Jasmine).
Positive
Religiosity “Myfaithstrengthened,I’malwayssaying thatifitwerenotforGod,Iwouldnotbe here.”(Giantwaterlily).
Familyand friends’support
“Myrelationshipwithfamilyandfriendsis verygood.Ihaveawonderfulsupport,and thisbringsmeconfidence[...].”(Hortensia).
Religiouspractice “Istarted(sic)toattendthechurchmore often.”(ThreeMarias).
study,whichdescribestheimpairmentofphysicalforcein30 stomizedwomen,whowerecolorectalcancersurvivors.16A
studyonsexual activityindicatedthatinolderwomenthe sexualpleasure(i.e.,sexualactivity)isaffected.2
TheanalysisofTables4and5shows thattheobstacles facedbyourparticipantssignificantly affecttheir physical, psychological,socialandspiritualwell-being.Thus,through thecontentanalysis,wecouldobservethatagreaternumber ofnegativeversuspositivesubcategoriesoccurred,whichis confirmedbelowbythementionedanalysis.
InthePhysicalWell-Beingcategory,reportsofparticipants described in the negative subcategory – leakage,odor and gasses–wereidentified.Studieshavebeenpublishedthat dis-cussthemeaningofphysicalbodychangeandofsuffering withrespecttothenewlifestyleoftheostomizedperson;thus, thephysicalwell-beingisgreatlyaffected,becauseofhis/her concernwith gasses,odors, fecalelimination,and leakage, resultinginphysicaldiscomfort.14,17,18
Intermsofphysicalstrength,theparticipantsstressedthat theirquality oflifeisimpaired. Itisworthnoting thatthe difficultyaboutphysicalstrengthwithrespecttodaily activ-itieswasmainlyidentifiedbywomen,whoreportadecrease inhouseholdchores;thisfindingwasalsodescribedinone study.19
Sleep was considered a negative subcategory. Studies reportthatthecollectorequipmentcausessleepdisturbances, impairingconsiderablythequalityoflife.Itwasalsonoted thatthesleep disturbanceisrelatedtothepresenceofthe ostomy,especiallyinthefirstmonthsaftersurgery,andtothe fearaboutthefuture.3,17
Educationinhealthiscriticalandfundamentaltothe pro-cessofcaringforhealth,resultinginaquality care.Health professionalsshouldrecognizethatthefamilyisacare/help unitforthesepeople,andthusitshouldbeincludedinhealth carepractices.14,20
Regarding Psychological Well-Being category, the reports showed how the change in self-concept, i.e., changes in bodyimageand self-esteem,influencespsychological well-being. Participants reported that, among their difficulties, stands the self-care. The correct guidance on the tech-nique of collector equipment changes, as well as on the inspection of the stoma during the change, shows the importanceofthehealthprofessionalinhelpingtoprevent complications,andinmakingmoreeasierthelifewiththe ostomy.5,14
Moreover,itwasalsoobservedinthereportsofthe partic-ipantsthatoftenthecolostomyincorporatesasocialstigma, i.e.,theostomizedpeoplefeelsdifferenttowardhisfamilyand society,thushinderingtheirownacceptanceandprocessof adaptation,whichleadstochangesinsociallife.Thiscauses theostomizedpersonfeeldifferent,excluded,and experienc-ingasenseofrejection.14,18,20
Ontheotherhand,averystrikingaspectwasthe accep-tanceperceivedinthereports.Manyparticipantsacceptedthe ostomyforlackofchoice,emphasizingthatifitisdifficultto livewiththecollectorequipment,atleasttheyarealiveandno longerfeelsick,inpainorwiththepossibilityofanimminent death.5
InthecategorySpiritualWell-Being,thereportsshowedthat religiositycanproduceanegativeimpact.Religiousfaithcan
alsoinfluencenegativelyinthepatient’srecovery,especially when,forexample,theindividualattributestoGodall respon-sibilityforhis/herfuture,failingtocarryoutthetreatmentor tocarehim/herselfandfightforlife.21
Fromtheevidencegiven,itappearsthatreligionisthe spir-itualsupportsought mostoftenbyostomized people.This factorfunctionsasareferencetotheirgeneralconceptions, and underliesthe meaningsofintellectual, emotional and moralexperience,bothfortheindividualandforthegroup.22
Furthermore,thepracticeofreligionmayappearasan ele-mentthathelpsincopingwiththedisease,allowingabetter adherencetotreatment,adecreaseofstressandanxiety, seek-ingameaningtothenewsituation.14,20
RegardingthecategorySocialWell-Being,itwasconfirmed thatthemanisasocialbeing;butforthepersontofeelgood withhimandwithothers,thepresenceofphysicaland psy-chologicalintegrityisindispensable.5
Forstomizedpeople,activitiesliketravelingandpracticing somekindofsport,areuncommon,whichleadstoidleness. Thereasons fortheserestrictionsrelatetothe uncertainty derivedfromthequalityofthecollectorequipment,physical problems,difficultytosanitizingtheequipment,shame,and fearofgastrointestinalproblems.5,14
Reports of sexual activities show that this practice is affected,bybeingcloselyrelatedtothenotionofself-concept andtheconsequentchangeinbodyimage,andtoadecreased self-esteemandperceptionofsexualattraction.
Alsoregardingsexualactivity,companionshipwas consid-eredapositivesubcategory;thus,sexualityisabroadfunction that covers biological, psychologicaland social aspects. In addition, thesexualpartnershipisanessentialpartof sex-uality, and can be a positive or a negative element in strengtheningtherelationandinthecomplicityofthe cou-ple’swell-being.18,23
Familysupportbecomesessential,becausetheostomized peoplepresentamedicalconditionaffectedbythe underly-ingpathologyandbythemajorsurgery,besidestheneedof specificcarefortheequipment.Boththefamilyandfriends oftheostomizedpersonconstitutehis/hersocialprotection, whichadmittedly hasafundamental roleintheprocessof constitution, development, crisis and resolution of health problems.5,24
Conclusions
Thestudyshowstheinterfacesofostomizedpersonsdueto colorectalcancerwiththechallengesfacedfromthemoment of discovery of the diagnosis, when they will undergo an ostomy,till theiradaptationtoanewlifestyle.These chal-lenges canbeunderstood asbodilychanges thatinfluence their self-concept, self-care, and relationshipsinsociallife – i.e., Physical, Psychological, Social Relations and Environment domains.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. WorldHealthOrganization,TheWHOQOLGroup.Qualityof lifeassessment(WHOQOL):positionpaperfromtheWorld HealthOrganization.SocSciMed.1995;41:1403–9. 2. MahjoubiB,MirzaeiR,AziziR,JafariniaM,ShoolamiLZ.A
cross-sectionalsurveyofqualityoflifeincolostomates:a reportfromIran.HealthQualLifeOutcomes.2012;10:136. 3. KimuraCA,KamadaI,JesusCAC,GuilhemD.Qualityoflifeof
colorectalcancerpatientswithintestinalstomas.JCarcinog Mutagen.2014;S10:007.
4. KimuraCA,KamadaI,GuilhemD.Qualityoflifeofindividual ostomydueoncologicalreasons:anapproachofintegrality fromBrazilianUnifiedHealthSystem.JColoproctol. 2016;36:34–9.
5. KimuraCA.Qualidadedevidadepacientesoncológicos estomizados.149f.Dissertac¸ão(MestradoemEnfermagem)– UniversidadedeBrasilia;2013.
6. BardinL.AnálisedeconteúdoLisboa:Edic¸ões;2008. 7. BrazilMinistryofHealth,NationaldHealthCouncil.
ResolutionNo.466/2012.Guidelinesandregulatingnormsfor researchinvolvinghumansubjects.Brasilia:CNS;2012. Availableat:
http://conselho.saude.gov.br/resolucoes/1996/Res196en.pdf 8. FleckMPA,LouzadaS,XavierM,ChachamovichE,VieiraG,
SantosL,etal.Aplicac¸ãodaversãoemportuguêsdo instrumentoabreviadodeavaliac¸ãodaqualidadedevida WHOQOL-bref.RevSaúdePública.2000;34:178–83. 9. MinistériodaSaúde(BR),SecretariadeAtenc¸ãoàSaúde,
InstitutoNacionaldeCâncer.Estimativas2015:incidênciade câncernoBrasil.INCA:RiodeJaneiro;2015.
10.SchneiderEC,MalinJL,KahnKL,KoCY,AdamsJ,EpsteinAM. Survivingcolorectalcancer:patient-reportedsymptom4 yearsafterdiagnosis.Cancer.2007;110:2075–82.
11.KaufmanG,TaniguchiH.Genderandmaritalhappinessin laterlife.JFamIssues.2006;27:735–57.
12.HawkinsD,BoothA.Unhappilyeverafter:affectsof long-term,lowqualitymarriagesonwell-being.SocForces. 2005;84:451–75.
13.StürmerT,GlynnRJ,LeeIM,ChristenWC,HennekensCH. Lifetimecigarettesmokingandcolorectalcancerincidencein thePhysicians’HealthStudyI.JNatlCancerInst.
2000;92:1178–81.
14.KimuraCA,KamadaI,GuilhemD,MonteiroPS.Qualityoflife analysisinostomizedcolorectalcancerpatients.J
Coloproctol.2013;33:216–21.
15.BaldwinCM,GrantMRN,WendelC,HornbrookMC,Herrinton LJ,McMullenC,etal.Genderdifferencesinsleepdisruption andfatigueonqualityoflifeamongpersonswithostomies.J ClinSleepMed.2009;5:335–43.
16.RamirezM,McMullenC,GrantM,AltschulerA,Hornbrook MC,KrouseRS.Figuringoutsexinareconfiguredbody: experiencesoffemalecolorectalcancersurvivorswith ostomies.WomenHealth.2009;49:608–24.
17.DabirianA,YaghmaeiF,RassouliM,TafreshiMZ.Qualityof lifeinostomypatients:aqualitativestudy.PatientPrefer Adherence.2011;5:1–5.
18.KimuraCA,KamadaI,GuilhemD,FortesRC.Perceptionof sexualactivitiesandthecareprocessinostomizedwomen.J Coloproctol.2013;33:145–50.
19.AlmeidaSSL,RezendeAM,SchallVT,ModenaCM.Os sentidosdacorporeidadeemostomizadosporcâncer.Revista Paraná.2010;15:761–9.
20.FortesRC,MonteiroTMTC,KimuraCA.Qualityoflifefrom oncologicalpatientswithdefinitiveandtemporary colostomy.JColoproctol.2012;32:253–9.
21.SilvaAL,ShimizuHE.Osignificadodamudanc¸anomodode vidadapessoacomestomiaintestinaldefinitiva.Rev Latino-AmEnfermagem.2006;14:483–90.
22.FornazariSA,FerreiraRE.Religiosidade/Espiritualidadeem pacientesoncológicos:qualidadedevidaesaúde.Psicologia: TeoriaePesquisa.2010;26:265–72.
23.SilvaAL,FaustinoAM,OliveiraPG.Asexualidadedopaciente comestomiaintestinal:revisãodeliteratura.Revenferm UFPEonline.2013;7:879–87.