SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Evaluation
of
suspected
physical
abuse
in
children:
a
500-case
study
夽
Marcos
Picini
a,
João
Rodolfo
Radtke
Gonc¸alves
a,
Thagla
Bringhenti
b,
Edilson
Forlin
a,∗aHospitalPequenoPríncipe,Curitiba,PR,Brazil
bPontifíciaUniversidadeCatólica,FaculdadedeMedicina,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4June2016 Accepted25July2016 Availableonline11May2017
Keywords:
Woundsandinjuries Childabuse Fractures,bone Orthopedics
a
b
s
t
r
a
c
t
Objective:Thisstudyevaluatedtheepidemiologicalprofileofpatientswithsuspected phys-icalabuse,especiallyregardingtheoccurrenceoffractures,treatedinareferralhospital.
Methods:Theauthorsreviewedall reportsofsuspectedabuseagainstchildrenand ado-lescents(AACA)inthishospitalfromJanuary2005toDecember2015.Theywereassessed andseparatedbymonthandyear.Thecharacteristicsofthevictimsofphysicalabusewith occurrenceoffractureswerestudied.Thefeaturesofthefractureswereevaluatedinthose patientswithavailableradiographs.
Results:Ofthe3125notifications,500wereclassifiedasphysicalinjuries;ofthese,63had fractures.Anannualprogressiveincreaseinnotificationswasobserved.Asforagegroup,50 patients(80.6%)wereuptothreeyearsoldand36(58%)uptooneyear.Mostweremale(60%) andthelikelyaggressorsweremotheraloneandbothparents(27.5%each).In30patients withavailableimages,fracturesoflongbones(femur,tibia,andhumerus)predominated (71%),aswellasasinglefractureline(74%),diaphyseallocation(73%),andatransverseline (57%).Thereweretwodeathsinfracturecases(3%).
Conclusion:AllorthopedistsshouldbealerttosuspectedAACAinchildrenwithtrauma belowtheageofthree,evenwithoutclassicsignsofabuse.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Avaliac¸ão
de
crianc¸as
com
suspeita
de
maus-tratos
físicos:
um
estudo
de
500
casos
Palavras-chave:
Ferimentoselesões Maus-tratosinfantis Fraturasosséas Ortopedia
r
e
s
u
m
o
Objetivo:Esteestudotemobjetivodeavaliaroperfilepidemiológicodepacientes atendi-dosemhospitaldereferênciacomsuspeitademaus-tratosfísicos,emespecialquantoà ocorrênciadefraturas.
Métodos:Todasasnotificac¸õesdesuspeitademaus-tratoscontracrianc¸aseadolescentes (MTCAA)feitasentrejaneirode2005edezembrode2015foramavaliadaseseparadaspor
夽
StudyconductedatHospitalPequenoPríncipe,Curitiba,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](E.Forlin).
http://dx.doi.org/10.1016/j.rboe.2017.05.004
mêseano.Dentreasvítimasdemaus-tratosfísicos,váriascaracterísticasdospacientes queapresentavamfraturasforamavaliadas.Quandoasradiografiasestavamdisponíveis, analisaram-seascaracterísticasdasfraturas.
Resultados: De3.125notificac¸ões,500foramclassificadascomolesõesfísicasedentreessas 63apresentavamfraturas.Observou-seumaumentoprogressivoanualdasnotificac¸ões. Quantoà idade,50pacientes(80,6%)tinham até3anose36(58%)até1ano.Amaioria eradogêneromasculino(60%)eoprovávelagressoreraamãeisoladamenteeambosos pais(27,5%cada).Em30pacientescomimagensdisponíveis,predominaramasfraturasde ossoslongos(fêmur,tíbiaeúmero,71%),únicas(74%),diafisárias(73%)etransversas(57%). Ocorreramdoisdeóbitosnoscasosdefraturas(3%).
Conclusão: TodososortopedistasdevemestaralertasparasuspeitadeMTCAAemcrianc¸as comtraumasabaixode3anos,mesmosemsinaisclássicosdemaus-tratos.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
DespiteTardieu’spioneeringstudyin1860,itwasonlyinthe secondhalfofthelastcenturythatviolenceagainstchildren and adolescents began to be studied more consistently.1–3
Nowadays,abuseagainstchildrenandadolescents(AACA)is recognizedas acomplex public health problem, withhigh financial, social,and emotionalcosts tosociety.4 In Brazil,
althoughcoveredinpreviouslegislation,notificationbythe healthcareprofessionalofsuspected orconfirmed casesof AACAonlybecamecompulsoryin1990,withthe implemen-tation ofthe Statue ofthe Child and Adolescent (Estatuto daCrianc¸aedoAdolescente[ECA]),throughtheFederalLaw No.8069.3 Even withthe obligationtonotify,the increased
interestinthesubject,andthedatashowingthatBrazilhas high levels ofviolence,there are few concrete statistics of theincidenceofAACAinBrazil.Thisisduetothe difficul-ties in definition, recognition, and reporting by healthcare professionals.5
Becausefracturesareoneofthemostcommonformsof abusepresentation,theorthopedistisoftenthefirstphysician toevaluatethesechildren.4Nevertheless,fewstudiesonthese
fracturesandontheroleoftheorthopedicsurgeonhavebeen publishedinthenationalorthopedicliterature;theyconsist ofcasereports5,6ortraumaseriesinwhichsuspectedcasesof
AACAwereidentified.7,8Onlyonepublicationthatspecifically
addressedtheoccurrenceoffracturesinpatientsvictimsof abusewasretrieved,inanon-indexedjournal.9
Thisstudy aimedtoevaluatetheepidemiologicalprofile ofchildrenwhoweresuspectedvictimsofAACA,specifically physicalabuse withoccurrenceoffractures,attended toat apioneering referral service in the MetropolitanRegion of Paraná,Brazil.
Material
and
methods
AllreportsofsuspectedAACAwereassessedbetweenJanuary 2005and December2015,subdividedintophysical, psycho-logical, and sexual abuse, aswell asneglect. Ofthe cases ofphysicalabuse, allthose witharecord offractures were
separated forevaluation.Exclusion criteriawereincorrectly completednotification,illegibility,orlossofmedicalchart.
Themonthlyandannualdistributionofnotificationswere assessed,aswellastheproportionbetweentotalnumberof victims ofphysicalabuse and occurrenceoffractures.The followingdatawerecollectedfrompatientsvictimsof physi-calabuseandwithfractures:age,gender,probableaggressor, topography,numberoffracturesperpatient,andoccurrence ofdeath.
For patientswhose radiographs were available for eval-uation inthe electronicor medicalrecord system, fracture characteristicswerecollected,includinglocation,and classi-fiedusingtheMüllerAOclassificationassimple(A),wedge(B), andcomplex(C)diaphysealfractures.
ThestudywasapprovedbytheInstitutionReviewBoard; underNo.47209215.0.0000.0097.
Results
A totalof3125reportsofabusebetween January2005and December 2015 were retrieved.Amongthe forms, the vast majoritywasrelatedtosexualaggression,2144cases(68.6%). Physicalviolencewasidentifiedin500patients(16%),mostly minor musculoskeletal injuries (bruises, contusions, abra-sions);ofthese,12.4%(n=62)presentedfractures(Table1).
Therehasbeenasteadyincreaseinnotificationsoverthe years,asshowninFig.1.Anincreaseinphysicalaggression wasobserved,from11%in2005to23%in2015,aswellasin thenumberoffractures,from4%to10%.Somefluctuationsin relationshiptothenumberofcaseswereobserved,withpeaks insomeyears,suchas2008,butthemainincreasewasfrom 2011onwards.
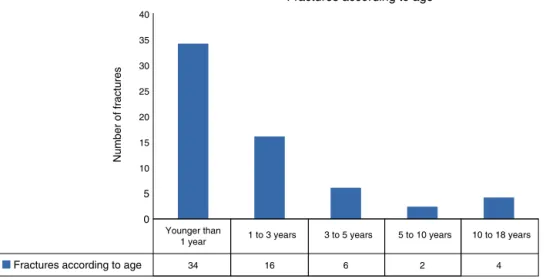
AsshowninFig.2,youngchildrencomprisedmostofthe victimsofabuse.Atotalof50cases(80.6%)wereobservedin theagerangeofupto3years,and36cases(58%)intheage rangeofupto1year.Asageincreases,thesefracturesbecome lessprevalent,withanewpeakinadolescence.
Table1–Formofviolenceanditsmonthlydistribution,from2005to2015.
Formofviolence Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physical 34 53 58 31 42 33 34 48 39 45 39 44 500
Psychological/Moral 5 4 2 6 5 3 2 7 5 5 5 7 56
Sexual 188 168 177 178 155 188 163 173 201 186 170 197 2144
Neglect/Abandonment 28 49 37 29 34 35 25 32 43 39 25 45 421
Totalpermonth 255 274 274 244 236 259 224 260 288 275 239 293 3121
Fractures Number 62
Notifications x physical aggression x fractures
450
400
350
300
250
200
150
100
Number of cases
50
0 2005
221 191 191 320 179 285 346 313 347 335 397
92
9 8 11 5 5 7 7 4 4 25
Physical
Fractures Total of notifications
18 15 35 20 44 37 39 89 101
1 1
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Fig.1–Annualdistributionofnotifications.
alonewasindicatedineightepisodes(13%),andothers (rel-ative,neighbor, caregiver,colleague and, non-informed), in tencases(15.8%).Datawerenotenteredintennotifications (15.8%).
Forty-fourpatients(71%)hadfracturesofthelongbones, with19 inthefemur(30%),followedbyhumerusandtibia, withtenpatientseach(16%).Fracturesoftheribsandskull wereobservedin14patients(22%;Fig.3).
Astothenumber offractures perpatient, 46 (74%) pre-sentedasinglefracturedbone.Only16patientshadmultiple
fractures,nine(15%)intwobones,andseven(11%)inthreeor more.Twopatientswithfracturesdied(3.2%).Bothhad mul-tiplefractures,includingseveretraumaticbraininjury(TBI), whichwasthecauseofdeath.
Radiographswereavailablefor30patients;26cases(87%) consistedofsimplefractures.Two(6%)hadcomplexfractures andtwo(6%)hadincompletefracturelines,withabsenceof wedge.Astothedirectionofthesimplefractures,17cases (57%)had transversefractures,five(17%),oblique,and four (13%),spiral.Regardingthelocationinthebone,26(87%)were
40
35
30
25
20
15
10
5
0
34
Fractures according to age
Fractures according to age
16 6 2 4
10 to 18 years 5 to 10 years
3 to 5 years 1 to 3 years
Younger than 1 year
Number of fractures
Femur Humerus Leg Skull
Rib Forearm Others
16%
16% 10%
12% 9%
7%
30%
Fig.3–Topographyoffractures,from2005to2015.
diaphysealandfourmetaphyseal–epiphyseal(13%),including acaseoftransepiphysealdetachment.
Discussion
Tardieuwasoneofthefirsttoaddress theissueinastudy in 1860, describing 18 deaths of children under 5 years whoseinjurieswerenotsatisfactorilyexplainedbytheir par-ents/guardians.Despitethisstudy,onlyinthesecondhalfof the lastcentury didthe theme gainimportance. Theterm battered-childsyndrome,coinedbyKempein1961,andthe publication of other major studies drew attention to the problem.1–4
AACAhasgainedgreaterinterestinBrazilonlyinthelast 20 years. This is especially surprising, as the country has someof the highest rates of violence worldwide.4 Despite
being addressed in previous legislation, it was only with theimplementationoftheECAthattherewasachange in the understanding of society’s responsibility to minors,1–4
especiallyinArticle13,whichestablishesmandatoryreport, byphysicians, ofcasesofsuspectedchild abuse.For cases ofnon-compliance,afineofthreeto20Brazilianminimum wagesisestablished,whichisdoubledintheeventofarepeat offense.3Nonetheless,thereiswidespreaddifficultybothin
identifyingandmanagingsuspectedcases.Reasonsmaybe thelackofknowledgeaboutthecharacteristicsoftheclinical pictureoraboutthenecessarymeasures,aswellasafearof involvementofprofessionalsinthissituation.6,10
Inordertoadequatelyaddresstheproblem,insomecities, protectionnetworkshavebeencreatedtoaddresssituations ofviolence; thesenetworkstrainhealthcareandeducation professionalsandcreatecareandreferralssystems.Curitiba wasoneofthefirstcitiestoestablishthisnetwork,in2003; initsearlystages,over10,000peopleweretrainedto iden-tifyandmanagecasesofsuspectedAACA.11Therefore, the
numberofsuspectedcaseshasincreaseddramatically,anda morerealisticpictureofthesituationcouldbeidentified.But evenincenterswherethereisabetteridentificationand man-agement,underreportingisthoughttobehigh.11,12According
toRolimetal.,13themainfactorsforunderreportingarethe
inexperienceofthehealthcareprofessional,withlessthanfive yearsofwork,andunfamiliaritywiththenotificationform. Pascolatetal.14estimatedthat,inBrazil,foreachcaseof
physi-calabuse,10–20casesgounreported.HermanandMcCarthy15
indicatedthatintheUnitedStates,lessthan8%ofcasesof abusearereportedbyhealthcareprofessionals.
Due to the frequency of physical abuse and fractures, theorthopedististheprofessionalwhofirstcaresforthese patients(in30%–50%ofthecases).6,16 Althoughthisimplies
thatorthopedistsshouldbepreparedtodiagnoseandmanage thesecases,theseprofessionalshardlyeverreportthecases. Oneoftheaspectsthatdemonstratethisfactisthesmall num-berofstudiespublishedinBrazilianorthopedicjournals.Only twostudies5,6thatdirectlyaddressAACAwereretrieved;both
consistofcasereportsandliteraturereview.Anotherstudy byBergamaschietal.7assessedthecauseoffemoralfracture
inchildrenunder3years;ofthe18casesevaluated,sixwere consideredtobephysicalabuseandthree,neglect.Francioziet al.8assessed182pediatricpatientstreatedfortraumaata pub-lichospitalandobservedtwodeaths(1%)byAACA.Theonly studythatincludedaseriesofcasesoffractureswasthatby Diranietal.,9publishedinanon-indexedjournal,which
Fig.5–Femurfracturesinachildaged1month.
uated122casesofsuspectedphysicalabuse,amongwhom25 patientspresentedfractures.
Therefore, thisisthe firstBrazilian studyin thefield of orthopedicsthataddressesalargenumberofsuspectedcases ofabuse.In the literature,thefrequencyofphysicalabuse rangesfrom20%to30%.6,7,11Thelowerrateobservedinthe
presentstudy(16%)canbeexplainedbythefactthatthis hos-pitalisthe referencein thecity forcases ofsexualabuse, whichexplainsthelargenumberofcasesofthistypeofabuse. Regardingtrauma,patientscanbeattendedtoinother emer-gencytertiarycenters.Therefore,theauthorsbelievethatthe number ofcases ofabuse may be muchgreater than that found.Thisreinforcestheneedfortheorthopedisttobe pre-paredtoappropriatelyidentifyandreferthesecases.Itwas observedthatmostofthevictimsofphysicalabusewereboys (60%).Intheliterature,theprevalencebetweengendersdiffer betweenstudies,whichsuggestbothahigherprevalenceof males14andoffemales.9,17AccordingtotheAACAdefinition,
theaggressorsareindividualswhoarecloseandknowntothe victims.Inthepresentstudy,aswellasinthatbyDiranietal.,9
itwasobservedthatthemotheralone,thenbothparents,were themostfrequentsuspects.Inturn,Pascolatetal.14indicated
themotherasthemainsuspect,andMenezesetal.,17 both
parents.
Internationalstudiesshowthatupto36%ofpatients suf-feringfromphysicalabusehavefractures.4,18Inthestudyby
Diranietal.,9theonlyBraziliancaseseriesretrieved,thisrate
was21%.Inthepresentstudy,thisratewaslower(12%);once again, this may bejustified bythe fact that, althoughthis hospitalhaspediatricemergencyservices,thecityalsohas atleastfourhospitalswithhigh-volumetraumaemergency roomsthatcantreatpatientswithfractures.
Regardingfracture pattern,althoughmany expectAACA fractures to have typicalfeatures, suchas transepiphyseal detachmentinyoungchildren(Fig.4),thepresentstudy,in linewithseveralothers,hasshownthatthemostcommon pattern(observedinatleast50%ofcases)isisolated diaphy-sealandtransversefractureoflongbones(Fig.5).6,19–21Inthe
presentseries,71%ofthecasespresentedanisolatedfracture; themostcommonlyfracturedbonewasthefemur,followed bythehumerus, andbonesofthelegand forearm.Canale
andBeaty19observedfiguressimilartothoseofthepresent
study.Inturn,Schwendetal.16andKingetal.20observedno
prevalencedifferencesregardingfemur,tibia,andhumerus. However, it isimportantto note that, inthe vast majority of cases, a typical AACA fracture characteristic cannot be observed.Asforthefractureline,weobservedthatthegreat majority(87%)presentedasingleline, mainlyinthe trans-verseplane(57%).ThesedatacorroboratethestudiesbyKing etal.,20LoderandBookout,21andespeciallythatbyMurphy
etal.,22inwhichastrongcorrelationbetweensimple
trans-versefracturesandsuspectedAACAwasestablished.Inthe presentstudy,thepercentageoffractureslocatedinthe dia-physis(73%)washigherthanthatfoundinotherseries.18,19
Therewasalowprevalenceoffractureswithspecial char-acteristics,whichareclassicallyassociatedwithAACA,such assternumandscapulafracturesandpresenceoffracturesin multiplesites.4Only11%ofthepresentpatientshadmultiple
fractures(Fig.6),whichcorroboratesotherstudies.9Forthese
reasons,theauthorsbelievethatthepresentdatasupportthe recommendationthatsuspicionofAACAshouldnotbebased on specificcharacteristics offractures.None ofthe present patientshadahistoryofviolence,anditwasnotpossibleto establishthetimeofevolution.Therefore,twofactors consid-eredasfundamental,whicharetheincompatibilitybetween historyandinjuryandthedelayinseekingtreatment,were notevaluated.Anotherimportantaspectnotaddressedinthis studyistheriskofrecurrenceoftheaggression;thisisanother factor that alerts tothe need forproper identification and managementofcasesofabusetotriggermeasurestoprotect thepatient.
Inattendingtothesepatients,it isessential toevaluate possibleassociatedlesions,especiallyTBI,duethehighrisk ofserioussequelaeandevendeath.8,23 Studieshaveshown
thatAACApatientswithskullfracturehaveahigherincidence ofintracranialhematomasthanthoseinwhomthefracture hadanaccidentalcause.4,23Amongthepresentpatients,two
Fig.6–ClassicAACAsigns,fracturesatdifferentstagesofconsolidationinachildaged15months.
intheprotectionandsurvivalofchildrenandadolescentswho arevictimsofabuse.
Conclusion
Thisstudyreinforcesthetheorythatcasesofabuseusually present single,diaphyseal and transverse fractures oflong bonesinyoungchildren,predominantlymale,andthe aggres-sorisclosetothevictim.Patientswhoarevictimsofabuseare atriskofTBI-associateddeaths.
Theorthopedist, who isoftenthe firstto evaluatesuch patients, should be prepared toidentify and appropriately managechildandadolescentvictimsofAACA.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Tothe SocialService ofthis institution, forthe transferof informationsheets,andtoSAME,forthemedicalrecords.
r
e
f
e
r
e
n
c
e
s
1.GuerraVNA.Violênciadepaiscontrafilhos:atragédia revisitada.4a
edSãoPaulo:Cortez;2001.
2.MinayoMCS.Violênciacontracrianc¸aseadolescentes: questãosocial,questãodesaúde.RevBrasSaudeMater Infant.2001;1(2):91–102.
3.Estatutodacrianc¸aedoadolescente.Availablefrom:
http://www.planalto.gov.br/ccivil03/leis/L8069.htm[accessed 09.04.16].
4.ForlinE,PfeifferL.Maus-tratosnainfânciaeadolescência. ProgramadeAtualizac¸ãoemTraumatologiaeOrtopedia (Proato).PortoAlegre:Artmed;2004.
5.RuaroAF,MeyerAT,AguilarJAG,HelluJJ,CustódioMD. Síndromedacrianc¸aespancada.Aspectoslegaiseclínicos– Relatodeumcaso.RevBrasOrtop.1996;32(10):835–8.
6.TerraBB,FigueiredoEA,TerraMPO,AndreoliCV,EjnismanB. Maus-tratosinfantis.Revisãodaliteratura.RevBrasOrtop. 2013;48(1):11–6.
7.BergamaschiJPM,AlcântaraT,SantilC,BragaSR,WaisbergG, AkkariM.Análisedefraturasdiafisáriasdofêmuremcrianc¸as menoresde3anosdeidade.ActaOrtopBras.2007;15(2):72–5.
9. DiraniM,FonsecaN,DiraniCC.Maus-tratosnainfância: análisede122casos.RevMedStaCasa.1989;1(1):84–8.
10.FerreiraLAM,PenhaJA.Aresponsabilidademédicaem relac¸ãoaosmaus-tratosdecrianc¸aedoadolescenteea legislac¸ãomenorista.Promotoriadejustic¸adainfânciaeda juventudeedapessoacomdeficiênciadePresidente Prudente;2013.Availablefrom:http://www.pjpp.sp.gov.br/ wp-content/uploads/2013/12/31.pdf.
11.MuraroHMS,TrovãoB,Sant’anaAS.Protocolodaredede protec¸ãoàcrianc¸aeaoadolescenteemsituac¸ãoderiscopara violência.3a
ed.Curitiba:SecretariaMunicipaldaSaúdede Curitiba;2008.
12.BazonMR.Violênciascontracrianc¸aseadolescentes:análise dequatroanosdenotificac¸õesfeitasaoConselhoTutelarna cidadedeRibeirãoPreto,SãoPaulo,Brasil.CadSaúdePública. 2008;24(2):323–32.
13.RolimACA,MoreiraGAR,CorrêaCRS,VieiraLJES.
Subnotificac¸ãodemaus-tratosemcrianc¸aseadolescentesna atenc¸ãobásicaeanálisedefatoresassociados.SaúdeDebate. 2014;38(103):794–804.
14.PascolatG,SantosCFL,CamposECR,ValdezLCO,BusatoD, MarinhoDH.Abusofísico:operfildoagressoredacrianc¸a vitimizada.JPediatr(RioJ).2001;77(1):35–40.
15.HermanMJ,McCarthyJJ.Theprinciplesofpediatricfracture andtraumacare.In:WeinsteinSL,FlynnJM,editors.Lovell andWinter’spediatricorthopaedics.7thed.Philadelphia:
WoltersKluwerHealth;2014.p.1680–3.
16.SchwendRM,BlakemoreLC,FickenscherKA.Theorthopedic recognitionofchildmaltreatment.In:FlynnJM,SkaggsDL,
WatersPM,editors.RockwoodandWilkinsfracturesin children.8thed.Philadelphia:WoltersKluwerHealth;2015.
p.231–58.
17.MenezesMGP,OliveiraMC,OsmoAA,SetinSMC,Spinelli MAS,PahlMMC,etal.Acrianc¸avítimademaus-tratos atendidaemservic¸osdeemergência.Pediatr(SãoPaulo). 1996;18(2):75–81.
18.BlakemoreLC,LoderRT,HensingerRN.Roleofintentional abuseinchildren1to5yearsoldwithisolatedfemoralshaft fractures.JPediatrOrthop.1996;16(5):585–8.
19.CanaleST,BeatyJH.Fracturesanddislocationsinchildren.In: CanaleST,BeatyJH,editors.Campbell’soperative
orthopaedics.12a
ed.Philadelphia:Mosby/Elsevier;2012.p. 1368–9.
20.KingJ,DiefendorfD,ApthorpJ,NegreteVF,CarlsonM. Analysisof429fracturesin189batteredchildren.JPediatr Orthop.1988;8(5):585–9.
21.LoderRT,BookoutC.Fracturepatternsinbatteredchildren.J OrthopTrauma.1991;5(4):428–33.
22.MurphyR,KellyDM,MoisanA,ThompsonNB,WarnerWCJr, BeatyJH,etal.Transversefracturesofthefemoralshaftarea betterpredictorofnonaccidentaltraumainyoungchildren thanspiralfracturesare.JBoneJointSurgAm.
2015;97(2):106–11.