ORGANOPHOSPHATE-INDUCED
DELAYED NEUROPATHY
Case report
Luiz Felipe R Vasconcellos
1, Ana Cláudia Leit e
1, Osvaldo J M Nasciment o
2ABSTRACT - Organophosphat e induced delayed neuropat hy (OPIDN) is an uncommon clinical condit ion. It occurs in associat ion w it h t he ingest ion of great amount s of organophosphat e aft er t he st imulat ion of cholinergic recept or. The clinical pict ure is charact erized by a dist al paresis in low er limbs associat ed w it h sensit ive sympt oms. Elect rodiagnost ic st udies show a mot or axonal neuropat hy. Involvement of t he cent ral nervous syst em may occur. We describe a 39 years-old female pat ient w ho developed hyperest hesia associat ed w it h lo w er lim b s p ar esis, f o u r t een d ays af t er sh e h ad in g est ed a Dich lo r vo s-b ased in sect icid e. Elect rophysiological st udy w as charact erized by an axonal polyneuropat hy pat t ern. Pyramidal t ract dysfunct ion w as observed lat er in upper limbs. Considering t hat bot h peripheral and cent ral nervous syst ems are involved w e believe t hat t he more appropriat ed t erm w ould be organophosphat e induced delayed neuropat hy (OPIDN) inst ead of organophosphat e induced delayed polyneuropat hy (OPIDP).
KEY WORDS: neuropat hy, polyneuropat hy, organophosphat e.
Neuropatia tardia por organofosforado: relato de caso
RESUM O - A neuropat ia t ardia dos organofosforados (NTOF) é condição clinica incomum. Geralment e ocorre após a int oxicação aguda por organofosforados, seguindo-se a fase de hiperest imulação colinérgica. O quadro clínico é caract erizado por déficit mot or dist al nos membros inferiores associado a sint omas sensit ivos. O est udo elet roneuromiográfico t em demonst rado padrão axonal mot or na maioria dos casos. Podem ocorrer sinais de compromet iment o do sist ema nervoso cent ral. Descrevemos o caso de uma pacient e de 39 anos que ingeriu inset icida a base de Dichlorvos e quat orze dias após apresent ou quadro de hiperest esia associado a paresia distal nos membros inferiores. Realizou eletroneuromiografia que se caracterizou por padrão compatível com polineuropat ia axonal. Sinais piramidais, de apareciment o mais t ardio, foram observados nos membros superiores. Diant e do compromet iment o do sist ema nervoso periférico e cent ral, t ambém consideramos o t ermo neuropat ia t ardia por organofosforado (NTOF) mais adequado do que t ão soment e polineuropat ia t ardia por organofosforado (PTOF).
PALAVRAS-CHAVE: neuropat ia, polineuropat ia, organofosforados.
Inst it ut e of Neurology Deolindo Cout o, Federal Universit y of Rio de Janeiro (INDC-UFRJ), Rio de Janeiro RJ, Brasil:and Depart ment of Neurology, Federal Fluminense Universit y (UFF), Nit eroi RJ, Brasil; 1M edical Doct or (INDC-UFRJ),2Full Professor (UFF).
Received 17 June 2002, received in final form 4 July 2002. Accept ed 18 July 2002.
Dr. Luiz Felipe Rocha Vasconcellos - Rua Barão da Torre, 209/102 B – 22411-001 Rio de Janeiro RJ - Brasil. FAX: 55 21 2284 3698. E-mail: luizf [email protected]
Organophosphat e induced delayed neuropat hy (OPIDN) is a sensory-mot or dist al axonopat hy w hich usually occurs aft er t he ingest ion of large doses of cert ain organophosphat e insect icides. M ost of t he pat ient s developed a mixed polyneuropat hy, mainly mot or1. The neurot oxic effect s of organophosphat es
have been w ell know n since t he dramat ic out break of “ Ginger Jake Paralysis” , w hich crippled as many as 50 000 in the USA in the 1930’s2. Since then several
ot her epidemics have occurred in different regions such as in Sri Lanka3. In this epidemic area, adolescent
Tamil girls at t aining menarche or w omen right aft er
childbirt h w ere affect ed and developed polyneuro-pat hy bet w een fourt een and t hirt y days aft er gingili oil ingest ion, follow ing local cust oms and t radit ion. Recovery from OPIDN is considered t o be generally poor. It is possible t hat several ot her fact ors such as the age of the patients, the difference in the chemical st ruct ure of t he organophosphat e and t he durat ion of initial intoxication in some w ay contribute tow ards a favorable out come4.
dela-suicide, t ook a large amount of an organophosphat e insec-t icide around insec-t hree w eeks before being admiinsec-t insec-t ed insec-t o insec-t he hospit al. She developed a st rong abdominal pain, saliva-t ion, diarrhea and lacrimasaliva-t ion a few hours afsaliva-t er saliva-t he inges-t ion of inges-t he insecinges-t icide. Ainges-t inges-t he inges-t ime of inges-t he suicide ainges-t inges-t empinges-t t he pat ient w as show ing miot ic pupils and received at ro-pine as t reat ment w it h part ial improvement of sympt oms; 24 hours aft er t he appearance of t he init ial sympt oms t he pat ient present ed respirat ory fat igue follow ed by respira-t ory insufficiency, and mechanical venrespira-t ilarespira-t ion w as requi-red. She st ayed for 48 hours under assist ed vent ilat ion w it hout respirat ory drive. Aft er t hat , she w as submit t ed w it h success t o a discont inuat ion of t he mechanical ven-t ilaven-t ion. She received hospiven-t al discharge w iven-t houven-t show ing any sympt oms. How ever, t w o w eeks aft er t he first dis-charge she st art ed having cramping calf pain and hyperes-t hesia in hyperes-t he planhyperes-t ar area follow ed by dishyperes-t al w eakness in t he low er limbs and, t w o days aft er, in t he upper limbs. Wit h t hose neurological deficit s t he pat ient w as referred t o INDC-UFRJ hospit al and admit t ed. At t his t ime t he
pa-w hereas t he Achilles t endon reflex pa-w as absent . Babinski sign w as not observed. Cranial nerves w ere not involved. There w as loss of t emperat ure discriminat ion and nocicep-t ion in disnocicep-t al low er limbs. Touch pressure, vibranocicep-t ory and joint posit ion senses w ere not involved.
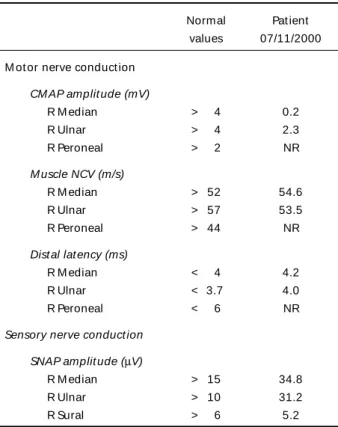
Electrophysiological examination (Table 1) disclosed po-sit ive sharp w aves and f ibrillat ion in t he f our lim bs. Reduced amplit udes of t he compound muscle act ion po-t enpo-t ials (CM AP) w ipo-t h m ildly reduced m opo-t or nerve con-duct ion velocit y (M NCV) of ulnar nerve in t he upper limbs. Sensory nerve act ion pot ent ials (SNAP) w ere normal in t he upper and mildly reduced in t he low er limbs. CM APs w ere not elicited in the low er limbs. These findings are consistent w it h a predominant mot or axonal polyneuropat hy invol-ving most ly t he low er limbs. She w as t reat ed w it h ami-t ripami-t yline (50mg/d), carbamazepine (600mg/d), capsaicin, t hiamin (300mg/d) and physiot herapy, w hich result ed in a part ial cont rol of t he hyperst het ic pain.
DISCUSSION
Organophosphat e est ers are used as insect icides, pet roleum addit ives, modifiers of plast ics, lubricant s, antioxidants and flame-retardants. They may be ab-sorbed via skin or respirat ory and gast roint est inal tracts5.The liposolubility allow s a penetration in the
central and peripheral nervous systems6.The
organo-phosphorus associated w ith neuropathy are tri-o-cresyl phosphat e (TOCP), lept ophos, mipafox, chlorphos, t richlorfon, malat ion, parat ion, met riphonat e and metamidophos7. The most dangerous OP ester is TOCP.
The clinical sequence could be divided in three steps:
Type I syndrome: Excessive st imulat ion of
mus-carinic receptors is responsible for intense cholinergic effect s, w hich are alw ays apparent w it hin a day of exposure, oft en w it hin hours. Cholinergic sympt oms include t achycardia or bradycardia, diarrhea, vomi-t ing, fasciculavomi-t ion, sw eavomi-t ing, salivavomi-t ion and micvomi-t uri-t ion. Excessive exposure causes emouri-t ional irriuri-t abiliuri-t y, nervousness, fat igue, diminished alert ness, cognit ive impairment , coma and convulsion. The t reat ment in all cases is at ropine in varying doses depending on t he clinical st at e5.
Type 2 syndrome (int ermediat e syndrome): It
follow s the intense cholinergic crisis of organophos-phorus poisoning and occurs in up 20%-50% of cases depending on the severity of poisoning, its duration, and on the type of organophosphorus compound.
Table 1. Elect rophysiological st udy.
Normal Pat ient values 07/11/2000
M ot or nerve conduct ion
CM AP amplit ude (mV)
R M edian > 4 0.2
R Ulnar > 4 2.3
R Peroneal > 2 NR
M uscle NCV (m/s)
R M edian > 52 54.6
R Ulnar > 57 53.5
R Peroneal > 44 NR
Dist al lat ency (ms)
R M edian < 4 4.2
R Ulnar < 3.7 4.0
R Peroneal < 6 NR
Sensory nerve conduct ion
SNAP amplit ude (µV)
R M edian > 15 34.8
R Ulnar > 10 31.2
R Sural > 6 5.2
Fig 1. Dorsal surf ace of hands show ing int erosseous at rophy.
Fig 2. Palmar surf ace show ing t enar and hypot enar at rophy.
There are no associat ed aut oimmune phenomena. Some authors propose that poor regulation of acetyl-choline receptors (AChRs) could explain the syndrome and neurophysiological findings8.Ot her sympt oms
occur usually 24 to 96 hours after the poisoning on the recovery from the cholinergic crisis. The cardinal f eat ures com prise m uscular w eakness, af f ect ing predominantly the proximal limbs muscles and neck flexors. Cranial-nerve palsies are common. Unlike the delayed polyneuropathy, this syndrome carries death
risk due t o associat ed respirat ory depression. The clinical courses may last from 5 to 18 days9.
Type III syndrome (organophosphat e induced de-layed neuropathy-OPIDN): many organophosphorus
eak-xicat ion by organophosphat e, a fact t hat show s t hat t he quant it y ingest ed w as subst ant ial. Rarely, some OPs produce delayed neurot oxicit y w it h t he onset of clinical sympt oms occurring one or t w o w eeks aft er t he exposure. This delayed effect is t he result of phosphorylat ion of nervous t issue prot ein w it h result ing w allerian axonal degenerat ion.
Fisher described a pat ient w ho w as exposed t o OPs and had no acut e manifest at ions of OPs t oxicit y but developed polyradiculit is, cranial nerve invol-vement , elevat ed cerebral spinal fluid (CSF) prot ein level, and elect romyography (EM G) pat t ern charac-t erischarac-t ics of charac-t he Guillain-Barré syndrome11.Ot her rare
clinical present at ion aft er int ense organophosphat e poisoning w as also described by Bekarovski et al.12.
These aut hors present ed a complet e out line of par-kinsonism w hich persist ed aft er recovery from cho-linergic symptoms. The patient ingested an unknow n dose of OPs in a suicide at t empt and developed all phases of OP int oxicat ion. Aft er t w o w eeks of poiso-ning he developed t remor and rigidit y t hat disappe-ared under t reat ment w it h Biperiden.
OPIDN is an uncommon cause of polyneuropat hy (PNP). Therefore, during invest igat ion of t he causes of peripheral neuropat hy it is import ant t o review t he hist ory of exposure t o t oxic subst ances. These int oxicat ions should also be part of t he different ial diagnost ic of paraparesis since t he part icipat ion of CNS on t he int oxicat ion by OPs only becomes evident aft er several years of exposit ion t o OPs10.
The pathogenesis of OPIDN involves the phospho-rylat ion and inhibit ion of neuropat hy t arget est erase (NTE). This enzyme is present in brain, spinal cord and peripheral nerve, as w ell as in non-neural t issues and cells such as spleen, muscle and lymphocyt es10.
The funct ion of NTE is unknow n. The abilit y t o inhibit NTE does not necessarily charact erize an OP as neu-rot oxic because some OPs inhibit t he NTE but do not produce OPIDN10.
The OPIDN is predominant ly mot or. Weakness ap-pears early and init ially involves legs muscles before t hose of t he hands. Despit e t he paucit y of sensory complaint s, object ive evidence of t he sensory loss is almost alw ays present . Sensit ive sympt oms as w ell as parest hesia and hyperest hesia are frequent .
Pro-Pat ient s w it h severe deficit s may not recover com-plet ely. There may be residual claw hand deformit y, persistent atrophy, and foot drop, as w ell as spasticity and ataxia5.The most important differential diagnosis
t hat should be considered in OPIDN include Guillain-Barré syn d ro m e an d acu t e d issem in at ed en ce-phalomyelit is7.
Elect rodiagnost ic st udies of OPIDN demonst rat e an axonal neuropat hy w it h acut e and chronic dener-vat ion in dist al and occasionally proximal limb mus-cles. Despit e sympt oms being predominant ly mo-t or, diminished sensory pomo-t enmo-t ial amplimo-t udes appear t o be more sensit ive t han mot or conduct ion changes in screening for OPIDN. M ot or conduct ion st udies are eit her normal or minimally slow ed. The CSF is usually acellular, and prot ein levels are eit her nor-mal or slight ly elevat ed5.Consequent ly, t his
exami-nation procedure is not relevant for diagnosis. The ele-trodiagnosis examination carried out in our patient indicated axonal neuropathy, mainly in the low er limbs, involving motor nerves w ith signs of denervation.
The incidence of pyramidal t ract dysfunct ion is high but t he present at ion is delayed. In t he Senana-yake’ s series4, nearly 50% of pat ient s had som e
evidence of pyramidal tract dysfunction although the signs w ere relat ively mild. In t he st udy carried out by Agapejev et al6, in patients w ith a history of
exoge-nous int oxicat ion, it w as proved t hat t he cent ral le-sion w as more frequent , probably due t o t he lipos-solubilit y of t hese subst ances.
For t his reason Khurana and Prabhakar13
sug-gest ed t hat t his syndrome, alt hough know n as orga-nophosphat e-induced delayed polyneuropat hy, is inappropriat ely labeled because pyramidal involve-ment is usually present ; init ially, peripheral nerve in-volvement predominat es, w hile cort icospinal t ract signs evolve more slow ly. Our pat ient show ed hyper-reflexia of t he upper limbs, w it h signs of pyramidal t ract involvement . Thus, our suggest ion of t he t erm Organophosphat e Induced Delayed Neuropat hy-OPIDN seem s m ore suit able. There is no specif ic t reat ment for OPIDN. The use of t hiamin is recom-mended by some aut hors but it does not alt er t he ap p ear an ce o f OPIDN6.Hyp er est h esi a can b e
carbama-zepine and capsaicin, associat ed or not . Our pat ient recovered slight ly from hyperest hesic pain in plan-t ar areas. Physioplan-t herapy is also indicaplan-t ed in plan-t hese cases. In a st udy carried out by Senanayde4 w it h
t w ent y pat ient s, t he only f orm of t reat m ent w as physiot herapy, mainly w alking exercises from t w o t o six w eeks during t he init ial period in hospit al. The low er m ot or neuron signs and sensory f indings began t o improve and almost complet ely disappe-ared at t he end of one year.
It is possible t hat several ot hers fact ors such as age of pat ient s, t he difference in t he chemical st ruc-t ure of OPs and ruc-t he duraruc-t ion of iniruc-t ial inruc-t oxicaruc-t ion had also, in some w ay, cont ribut ed t ow ards t he fa-vorable out come4. The degree of pyramidal t ract
da-mage had been a major determinant of the prognosis for funct ional recovery in previous episodes. Aft er recovering from t he acut e effect s t he pat ient s may develop spast ic paraparesis. The follow up of t hese pat ient s should be done over at least four w eeks aft er t he acut e int oxicat ion14.Recovery in most
ca-ses is incomplet e. Our pat ient w as discharged from t he hospit al five w eeks aft er init ial exposure t o t he OPs. Aft er t hree mont hs she present ed a part ial con-t rol of con-t he pain. The mocon-t or funccon-t ion improved gradu-ally. There are brisk reflexes in t he upper limbs.
Ingest ion of organophosphat e, eit her accident al or suicidal should be considered in cases of neuro-pat hy, even if t he init ial phases of int oxicat ion are not clinically w ell defined.
Acknowledgment - The authors w hish to thank Dr. Gló-ria Penque for her help w ith the electromyography measu-rements and Dr. João Klescoski for his help w ith the photos.
REFERENCES
1. Moretto A, Lotti M. Poisoning by organophosphorus insecticides and sensory neuropathy. J Neurol Neurosurg Psychiatry 1998;64:463-468. 2. Morgan JP, Penovich P. Jamaica ginger paralysis: forty-seven year
follow-up. Arch Neurol 1978;35:530-532.
3. Senanayake N, Jeyaratnam J. Toxic polyneuropathy due to gingili oil contaminated with tri-cresyl phosphate affecting adolescent girls in Sri Lanka. Lancet 1981;1:88-89
4. Senanayake N. Tri-cresyl phosphate neuropathy in Sri Lanka: a clinical and neurophysiological study with a three year follow up. J Neurol Neurosurg Psychiatry 1981;44:775-780.
5. Berger AR. Toxic peripheral neuropathies. In Samuels MA, Feske, S, (eds). Office practice of neurology. New York: Churchill Livinsgtone, 1996:538-539.
6. Agapejev S, Vassiliev I, Lima MMF. Neurologic manifestations in 93 patients with exogenous intoxication by non-medicamentous chemical substances. Arq Neuropsiquiatr 1986;44:232-242.
7. Araújo AQ-C. Organophosphorus polyneuropathy. Rev Bras Neurol Psiq 1997;1:75–77.
8. Sedgw ick EM, Senanayake N. Pathophysiology of the intermediate synd ro me o f o rgano pho spho rus po iso ning. J Neuro l Neuro surg Psychiatry 1997;62:201-202.
9. Senanayake N, Karalliedde L. Neurotoxic effects of organophosphorus inseticide - an intermediate syndrome. N Engl J Med 1987;316:761–763. 10. Schaumburg HH, Berger AR. Toxic neuropathy due to industrial agents. In Dyck PJ, Thomas PK, Griffing Jw, Low PA, Poduslo JF (eds). Peripheral neuropathy. 3.Ed. Philadelphia: W B Saunders; 1993:1541-1548. 11. Fisher JR. Guillain-Barré synd ro me fo llo w ing o rgano pho sphate
poisoning. JAMA 1977;238:1950-1951.
12. Bekarovski N, Radulovic S. Parkinsonism after organophosphate poisoning. J Neurol Sci 2001;187(Suppl 1):S101(P0286).
13. Khurana D, Prabhakar S. Organophosphorus intoxication . Arch Neurol 2000;57:600-602.