www.jped.com.br
ORIGINAL
ARTICLE
Prevalence
and
risk
factors
of
anemia
in
children
夽
,
夽夽
Cristie
Regine
Klotz
Zuffo
a,
Mônica
Maria
Osório
b,
Cesar
Augusto
Taconeli
c,
Suely
Teresinha
Schmidt
a,
Bruno
Henrique
Corrêa
da
Silva
c,
Cláudia
Choma
Bettega
Almeida
a,∗aPostgraduatePrograminFoodandNutritionSecurity,DepartmentofHealthSciences,UniversidadeFederaldoParaná(UFPR),
Curitiba,PR,Brazil
bPostgraduatePrograminNutrition,UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil cDepartmentofStatistics,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
Received12June2015;accepted22September2015 Availableonline15February2016
KEYWORDS
Anemia; Riskfactors; Infantnutrition; Iron
Abstract
Objective: Toidentifytheprevalenceandfactorsassociatedwithanemiainchildrenattending MunicipalEarlyChildhoodEducationDayCareCenter(CentrosMunicipaisdeEducac¸ãoInfantil [CMEI])nurseriesinColombo-PR.
Methods: Analytical, cross-sectional study with a representative sample of 334 children obtained bystratified clustersampling,withrandom selectionof26 nurseries.Data collec-tionwasconductedthroughinterviewswithparents,assessmentofironintakebydirectfood weighing,andhemoglobinmeasurementusingthefinger-sticktest.Bivariateassociationtests wereperformedfollowedbymultiplelogisticregressionadjustment.
Results: Theprevalenceofanemiawas34.7%.Factorsassociatedwithanemiawere:maternal age youngerthan28years old(p=0.03),malechildren (p=0.02),children youngerthan24 months (p=0.01),andchildren who didnot consumeironfood sources (meat+beans+dark green leafy vegetables)(p=0.02). Therewas noassociation betweenanemia andiron food intakeinCMEI.However,ironintakewaswellbelowtherecommendedlevelsaccordingtothe NationalEducationDevelopmentFundresolution,higherprevalenceofanemiawasobservedin childrenwhoseintakeofiron,hemeiron,andnonhemeironwasbelowthemedian.
Conclusions: Intermsofpublichealth,theprevalenceofanemiaischaracterizedasamoderate probleminthestudiedpopulationanddemonstratestheneedforcoordinationof interdisci-plinaryactionsforitsreductioninCMEInurseries.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
夽 Pleasecitethisarticleas:ZuffoCR,OsórioMM,TaconeliCA,SchmidtST,daSilvaBH,AlmeidaCC.Prevalenceandriskfactorsofanemia
inchildren.JPediatr(RioJ).2016;92:353---60.
夽夽Thearticleispartofthefirstauthor’sMaster’sDegreedissertationinPostgraduatePrograminFoodandNutritionSecurity,Department
ofHealthSciences,UniversidadeFederaldoParaná,Curitiba,PR,Brazil.
∗Correspondingauthor.
E-mail:[email protected](C.C.B.Almeida).
http://dx.doi.org/10.1016/j.jped.2015.09.007
PALAVRAS-CHAVE
Anemia;
Fatoresderisco; Nutric¸ãodolactente; Ferro
Prevalênciaefatoresderiscodaanemiaemcrianc¸as
Resumo
Objetivo: Identificaraprevalênciaeosfatoresassociadosàanemiaemcrianc¸asque frequen-tamberc¸áriosdeCentrosMunicipaisdeEducac¸ãoInfantil(CMEI)deColombo-PR.
Métodos: Estudoanalítico,decarátertransversal,comamostrarepresentativade334crianc¸as obtidaporamostragemestratificadaporconglomerados,comselec¸ãoaleatóriade26berc¸ários. Acoletadedadosfoirealizadapormeiodeentrevistacomospais,avaliac¸ãodaingestãode ferroporpesagemdiretadealimentosedosagemdehemoglobinaporpunc¸ãodigital.Foram realizadostestesdeassociac¸ãobivariadosseguidopeloajustedeumaregressãologística múlti-pla.
Resultados: Aprevalênciadeanemiafoide34,7%.Osfatoresassociadosàanemiaforam:idade maternainferiora28anos(p=0,03),crianc¸asdosexomasculino(p=0,02),comidadeinferior a24meses(p=0,01)equenãoconsumiamfontesalimentaresdeferro(carne+feijão+verduras verdesescuras)(p=0,02).Nãohouveassociac¸ãoentreanemiaeingestãodeferronoCMEI. Porém,aingestãodeferrofoibemabaixodoquerecomendaaresoluc¸ãodoFundoNacional deDesenvolvimentodaEducac¸ão,sendopossívelobservarmaiorprevalênciadeanemianas crianc¸ascujaingestãodeferro,ferrohemeeferronão-hemeapresentava-seabaixoda medi-ana.
Conclusão: Emtermosdesaúdepública,aprevalênciadeanemiaencontradasecaracteriza comoumproblemamoderadonapopulac¸ãoestudadaedemonstraanecessidadedearticulac¸ão deac¸õesinterdisciplinaresparaasuadiminuic¸ãonosCMEIs.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Anemiais aglobal public health problem,withimportant consequences for human health and the social and eco-nomicdevelopmentofeach nation.1 Itresults fromsingle
ormultiplecausesthatactsimultaneously,influencing chil-dren’shealth,2 their cognitive andphysical development,
andimmunity, increasingthe risk of infections andinfant mortality.3
Aglobalanalysisoftheprevalenceofanemiaworldwide hasshownthatpreschool-agechildrenarethemostaffected agerange,withaprevalencerateof47.4%.1
Duetoitscomplex anddifficult-to-control characteris-tics,severalstudieshavesoughttoidentifythereasonsfor itshighprevalenceandpotentialassociatedfactors.4,5,6The
identification ofthese factorscontributesto implementa-tionofactionsaimedatthepreventionandminimizationof theproblem.
Theperiodbetweenconception and2yearsof ageisa criticalstageof development,makingchildren vulnerable toanemia.Atthisage,theystartattendingEarlyChildhood EducationDayCareCenternurseries,whichareresponsible fortheirfull-timehealthandnutritioncare.
ThemunicipalityofColomboandthemetropolitanregion of Curitiba lack studies on the prevalence of anemia in children attending Municipal Early Childhood Education Day CareCenters (Centros Municipais de Educac¸ão Infan-til [CMEI]). Thus, such studies are justified due to the greater vulnerabilityof these children and the identifica-tion of amounts of iron supplied in the meals at these institutions.Obtainingaprofileofanemiastatusmay con-tributetotheimplementationandconsolidationofactions
thatwillcontributetoitspreventionandreductioninthis population.
The objectiveof thestudy wastoestimate the preva-lenceofanemiaandtoidentifyassociatedfactorsinchildren attending CMEI nurseriesin the municipality of Colombo, stateofParana,Brazil.
Material
and
methods
Thisisacross-sectionalanalyticalstudyof334childrenaged 6---36months,attendingCMEInurseriesthecityofColombo ---PR,inthemetropolitanregionofCuritiba.Colombohas38 CMEIs,attendedby6852childrenregularlyenrolledin2012, with816inthenurseries.
Theselectedsamplewasrepresentativeofchildrenfrom CMEInurseriesandwasdefinedby stratifiedcluster samp-lingwithasinglestep,withrandomselectionof26ofthe 38CMEIsinColombo.Thesewereseparatedbycityhealth district according to their location, while respecting the proportionof studentsenrolledin eachhealth district.As areferencetocalculatethesample,a prevalenceof ane-miaof29.7%wasadoptedfromastudycarriedoutinCMEI nurseries of Cascavel, state of Parana, with a represen-tative sample of children between 6 and 24 months,7 as
The questionnaire included questions about the socio-economic, environmental, biological, maternal and birth characteristics, feeding practices, and iron supplemen-tation.Thequestionnaireswerepreviouslytestedinapilot studyinaCMEIthatwasnotpartofthesample.Interviews wereconducted withparents and guardiansfromJune to December2013.
Hemoglobin levels were measured in a blood sample obtainedbydigitalpuncture,collectedin amicrocuvette, andreadingwasperformedin portablehemoglobinmeter. Ahemoglobinconcentrationbelow11g/dLwasconsidered anemia andclassified as mild (10.0---10.9g/dL),moderate (7.0---9.9g/dL),orsevere(<7.0g/dL),accordingtotheWorld HealthOrganization(WHO)criteria.8
The anthropometric assessment was performed with weightandheightmeasurement.Weightwasmeasuredusing adigitalpediatricscalewith5gaccuracyand15kgcapacity. Childrenwereweighednakedusingacleandisposable dia-per,afterthescalewaspreviouslycalibratedandinstalled onaflat,smooth,firmsurface.Childrenweighingmorethan 15kgwereweighedonaportabledigitalscalewithcapacity of150kgand100gaccuracy.9
The length was measured using a portable wooden anthropometer,withamplitudeof 100cm and0.5cm sub-divisions.Childrenyoungerthan2yearsweremeasuredin the supine positionon the anthropometer. Childrenolder than2yearsweremeasuredinthestandingpositionwitha woodenanthropometer.
The nutritional status was classified using the World HealthOrganization (WHO) Anthro program, version 3.2.2 (WHO,GE,Switzerland)for weight/age(W/A),height/age (H/A),andbodymassindex/age(BMI/A).10
Iron intakewas obtained by individual directweighing ofthefoodprovidedat theCMEI,carriedoutontwo non-consecutivedays.The nutritional compositionofthe food wasobtainedusingtheAVANUTRI®program(AVANUTRI®,RJ, Brazil).Ironintakewasexpressedasdietaryintakeoftotal iron,hemeiron,andnonhemeiron.Hemeironwas consid-ered as40% oftheironcontainedinmeat,and non-heme iron asthe remaining 60%, addedto the total ironfound inotherfoods.The densitiesoftotaliron,hemeiron,and nonhemeironwereobtainedbydividingthetotalofeachof thesenutrientbythetotalcaloriesingestedbythechildon theday,expressedinmgofironper1000kcalofthediet.11
The independentvariableswere distributedasfollows: (1)biologicalfactors:genderandageofthechild;(2) feed-ingpractice:durationofmaternalbreastfeeding,exclusive breastfeedinguntilsixmonths,consumptionoffruitjuice, fruit,milk, beans,meat, liver, legumes, darkgreen leafy vegetables,iron-richfoods(meat+beans+darkgreenleafy vegetables);totaliron,hemeiron,andnon-hemeironintake at CMEI; density of total iron, heme iron,and non-heme iron;(3)morbidities:feveranddiarrheainthelast15days, historyofanemia;(4)nutritionalstatus:lowbirthweight, underweight,overweight,shortstature,overweight accord-ingtoBMIforage;(5)healthcare:prenatalcare,numberof prenatal consultations, ironsupplementation during preg-nancy,typeofdelivery,prematurity;(6)maternal factors: age,ethnicity,numberofchildren;(7)socioeconomic fac-tors: maternal level of education and employment, per capitaincome,welfareprogrambeneficiariesandChildren’s MilkProgram;homeownership,numberofresidentsinthe
household,numberofrooms,cleanwater,sewagetreatment andgarbagecollectionservices.
The variables were categorized according to studies investigatinganemiainchildren.2,4,11,12Ironintakewas
cat-egorizedinrelationtotheobservedmeanvalues.
Data were entered in duplicate into a Google Drive® onlineformand afterverification, theywere exported to SPSSsoftware,version19.0(IBMCorp.Released2010.IBM SPSSStatisticsforWindows,NY:USA).
A descriptiveanalysis of the variables was performed. TheassociationwithanemiawasverifiedusingFisher’sexact test and thechi-squared test. The variables withp<0.20 wereselectedtocomposethe multiple logisticregression model. The multivariate analysis was performed by con-structingtheconceptualmodelbasedonandadaptedfrom Osórioetal.13
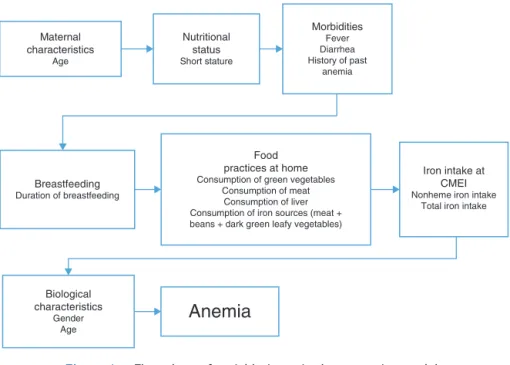
Seven hierarchical levels were defined according to thefollowing order: maternal characteristics (age); nutri-tionalstatus(shortstature), morbidity(presence of fever and/ordiarrheaintheprevious15days,historyofanemia); maternal breastfeeding (breastfeeding duration), feeding practicesathome(consumptionofdarkgreenleafy vegeta-bles, meats, liver andiron-rich foods (meat+beans+dark greenleafyvegetables);ironintakeatCMEI(non-hemeiron andtotaliron);biologicalcharacteristicsofthechild (gen-derandage).Thevariableswereenteredintothemodelone byone,andthosethatdidnotshowstatisticalsignificance ofp<0.05were removed.Crude andadjusted oddsratios (OR)wereestimated.
This work is part of the ResearchProjecton Foodand NutritionSecurityintheSchoolEnvironment,approvedby theEthicsCommitteeforResearchinHumanBeings(CAAE 11312612.5.0000.0102).
Results
Theestimatedprevalenceofanemiais34.7%.Oftheanemic children,56.9%hadmild,42.2%moderate,and0.9%severe anemia.Themeanhemoglobinlevelwas11.3g/dL(±1.34). The meanage of the childrenwas 21.2(±5.7)months and50.3%weremales.Themediandurationof breastfeed-ingwas180daysandof exclusivebreastfeeding,90 days. Thisstudyfound5%shortstature,0.6%underweight,3.4% overweight,and8.4%overweightaccordingtoBMI.Family incomepercapitawaslessthanoneminimumwagein76.7% ofhouseholds.
ThemedianintakeoftotalironattheCMEIwas3.01mg, withalargercontributionofnon-hemeiron.Themedianiron density was5.64mg/1000kcal. The prevalence of anemia washigherinchildrenthathadtotaliron,hemeiron, non-hemeironintake,andhemeirondensitybelowthemedian levels(Table1).
Table1 Totaliron,hemeiron,andnonhemeironintake,inadditiontototaliron,hemeiron,andnonhemeirondensityinthe dietofchildrenattendingMunicipalEarlyChildhoodEducationCenters,Colombo,2013.
Variables Mean(Standard
deviation)
Median Minimum---Maximum
%anemia (<median)
%anemia (≥median)
Totaliron(mg) 3.10(1.46) 3.01 0.12---8.81 39.9 31.1 Hemeiron(mg) 0.13(0.12) 0.09 0.00---0.68 38.9 32.9 Nonhemeiron(mg) 2.97(1.40) 2.89 0.09---8.71 39.8 31.1 Totalirondensity(mg/1000kcal) 5.64(1.85) 5.41 0.70---15.89 35.7 35.7 Hemeirondensity(mg/1000kcal) 0.25(0.20) 0.18 0.00---1.27 39.1 32.5 Nonhemeirondensity(mg/1000kcal) 5.40(1.78) 5.17 0.61---15.89 35.1 36.4
consumption(OR:4.83;95%CI:1.22---19.12)and consump-tion of dark green leafy vegetables (OR: 0.58; 95% CI: 0.34---1.01).Fourteenfactorsshowedp<0.20inthe bivari-ate analysis and were considered for inclusion in the multiplelogisticregressionmodel(Table2).
Theentryorderofthevariablesintothemultiplelogistic regressionmodelisshowninFig.1.
Table3showstheresultofthemultiplelogisticregression model adjustment.After runningthe selection algorithm, thefollowingvariablesremainedinthemodel:child’s gen-der, estimating an 82% higher chance of anemia in male children(OR:1.82;95%CI:1.08---3.06);child’sageyounger than24months(OR:2.12;95%CI:1.19---3.75);maternalage youngerthan28 years(OR:1.72; 95% CI:1.03---2.87),and non-consumption of iron food sources (OR: 1.91; 95% CI: 1.06---3.44).
Discussion
A 34.7% prevalence of anemia was identified, as well as a positive association with younger maternal age, male gender, child’s age younger than 24 months, and non-consumptionofiron-richfoods(beans,meat,anddarkgreen leafyvegetables)athome.
In publichealth, the prevalence of anemiaof 34.7% is consideredamoderateprobleminthestudiedpopulation.3
This prevalenceis higher tothatfound in a studycarried outinCascavel---PR,7whichinvestigatedchildrenyounger
than24monthsthatattendeddaycare(29.7%).TheWoman andChildNationalDemographicandHealthSurvey(Pesquisa Nacional de Demografia e Saúde da Crianc¸a e da Mulher [PNDS])of2006assessedtheprevalenceofanemiain chil-dren at the national level, for the first time and found a prevalence rate of 20.9% in children younger than 59 months,and35.8%inchildrenyoungerthan24months,close towhatwasfoundinthisstudy.14
ThisresultisconsistentwiththatofLealetal.12(32.8%)
inchildrenaged0---59monthsfromthestateofPernambuco andCastroetal.15 (29.2%)inpreschoolers,andlowerthan
thatidentifiedinVitória(ES)(15.7%)inchildrenaged1---5 years.16 Twootherstudiesinvestigatinganemiaindaycare
centernurseriesfound higherprevalencerates,51.9%and 46.6%.2,17 Ameta-analysis performed by Vieira & Ferreira
foundahigherweightedmeanprevalencethanthatfoundin thepresentstudy:52%anemiaindaycarecenters,60.2%in healthservices,and66.5%indisadvantagedpopulations.18
Althoughmostchildrenhavemildanemia,moderate ane-miawasfoundin 42.2%of theanemic children;suchrate
deservesattention,asanemianegativelyaffectscognitive development,physicalcapacity,productionofthyroid hor-mones, bodytemperature regulation, andimmune status, increasingtheriskofinfectionandcausingeffectsthatlast foralifetime.14 Konstantyneretal.4 found9.9%moderate
anemiainchildrenyoungerthan24monthsfromallregions ofBrazil.
Theassociationbetweenanemiaandageyoungerthan24 monthshasbeenverifiedinstudiesconductedinday care centers.15,19,20This vulnerabilityisrelatedtoanincreased
growth velocity,wherein the weighttriplesandbody sur-faceareadoubles.Thisfactgeneratesincreasednutritional needs,whichcoincideswithmajorchangesinfeeding, intro-ductionofcomplementaryfeeding,weaning,andexposure tothefamilyfeedingpractices.
Early cessation of breastfeeding associated to a poor complementarydietwithlowironcontentaddsamultiplier effecttotheanemiariskincrease.Thisriskisaggravatedby thegreaterexposuretocontagionfrominfectiousand par-asitic diseases, duetoincreasedcontactwiththe outside environment.11,15,20 Only13.2% ofchildren werebreastfed
exclusively for 6 months, 33% had meat introduced at 6 monthsof age,andtheironintake,especiallyhemeiron, waswell belowthe intakeobserved inolder children and corresponded to 35.2% of what is recommended by the NationalSchoolFeedingProgram.
Braingrowthishigherinthefirsttwoyearsoflife,when thecentralnervoussystemmembranesaremorepermeable toiron,representingthemostcriticaltimeforitsuse.Iron deficiency has consequences such as the loss of physical andcognitive development,whichimpairslearning ability anddecreasesworkcapacity.Promotingbetternutritionin thefirst1000daysoflifehasbeenoneofthestrategiesto improvethe healthstatus inadulthood, aswell ashuman development,andreinforcestheimportanceofprevention ofnutritionaldeficiencies,suchasirondeficiencyanemiain firsttwoyearsoflife.21
Thehigherprevalenceof anemiainmalesisrelatedto thehighergrowthrateinboys,resultingingreaterneedfor ironbythebody,notsuppliedbythediet.15,22,23
Table2 DistributionofanemiainchildrenfromMunicipalEarlyChildhoodEducationCenters,Colombo,2013.
VARIABLES na Prevalenceofanemia Chi-squared CrudeOR p
n(%) (95%CI)
Gender
Male 168 70(41.7%) 7.17 1.86(1.17---2.94) 0.00
Female 166 46(27.7%)
Child’sage
<24months 198 79(39.9%) 6.46 1.88(1.15---3.09) 0.01 ≥24months 123 32(26.0%)
Maternalage
<28years 156 65(41.7) 6.42 1.80(1.14---2.84) 0.01 ≥28years 176 50(28.4)
Shortstatureforage
Yes 16 8(50.0) 1.77 1.96(0.71---5.37) 0.18
No 305 103(33.8)
Feverinthelast15days
Yes 157 64(40.8%) 4.60 1.64(1.04---2.58) 0.03
No 176 52(29.5%)
Previoushistoryofanemia
Yes 229 25(44.6%) 4.01 1.83(1.01---3.33) 0.04
No 56 70(30.6%)
Diarrheainthelast15days
Yes 73 31(42.5) 2.46 1.52(0.89---2.60) 0.11
No 261 85(32.6)
Durationofmaternalbreastfeeding(days)
≤180days 156 44(28.2) 4.06 0.70(0.36---1.36) 0.13 >180to≤360days 62 26(41.9) 1.29(0.60---2.74)
>360days 53 19(35.8) 1
Consumptionofmeat
Yes 292 95(32.4%) 6.06 4.83(1.22---19.12) 0.03
No 10 7(70.0%)
Consumptionofdark-greenleafyvegetables
Yes 229 70(30.7) 3.74 0.58(0.34---1.01) 0.05
No 72 31(43.1) 1
Consumptionoffoodsthataresourcesofiron(meat+beans+dark-greenleafyvegetables)
Yes 223 68(30.5%) 3.61 1 0.05
No 78 33(42.3%) 1.67(0.98---2.84)
Consumptionofbovineliver
Yes 163 48(29.6) 2.57 1.48(0.91---2.39) 0.10
No 138 53(38.4) 1
TotalironintakeatCMEI
<3.10mg 163 65(39.9) 2.61 1.46(0.92---2.33) 0.10
≥3.10mg 151 47(31.1)
NonhemeironintakeatCMEI
<2.97mg 166 66(39.8) 2.56 1.46(0.91---2.33) 0.10
≥2.97mg 148 46(31.1)
a Rateofnon-response:0.9---15.7%.
Older mothersarebetterabletomeet thehealthcare demands of theirchildren. The risk ofanemia inchildren of youngermothers suggests thatthese areless prepared tomeetthenutritionalneedsoftheirchildrenandto per-formthe dutiesof motherhood.This mayreflect thelack
offinancialresources,lackofknowledgeaboutanemiaand childcare,andlackofadequateguidance.11,12,20,24
Maternal characteristics
Age
Nutritional status
Short stature
Morbidities
Fever Diarrhea History of past
anemia
Breastfeeding
Duration of breastfeeding
Food practices at home
Consumption of green vegetables Consumption of meat
Consumption of liver Consumption of iron sources (meat + beans + dark green leafy vegetables)
Iron intake at CMEI
Nonheme iron intake Total iron intake
Biological characteristics
Gender Age
Anemia
Figure1 Flowchartofvariableinputintheregressionmodel.
Table3 LogisticregressionmodelforfactorsassociatedwithanemiainchildrenfromMunicipalEarlyChildhoodEducation Centers,Colombo,2013.
Variables CrudeOR(CI) p AdjustedOR(CI) p
Child’sgender
Male 1.86(1.17---2.94) 0.00 1.82(1.08---3.06) 0.02
Female 1 1
Child’sage
<24months 1.88(1.15---3.09) 0.01 2.12(1.19---3.75) 0.01
>24months 1 1
Maternalage
<28years 1.80(1.14---2.84) 0.01 1.72(1.03---2.87) 0.03
>28years 1 1
Consumptionoffoodsthataresourcesofiron(meat+beans+dark-greenleafyvegetables)
Yes 1 0.05 1 0.02
No 1.67(0.98---2.84) 1.91(1.06---3.44)
dark green leafy vegetables, and especially meat and viscera, as they are sources of heme iron, with better bioavailability.Childrenwhose parents reported consump-tionofthese foodsat home weremore protectedagainst anemia.
TheironintakeattheCMEIshowednoassociation with anemia.However,thereisahigherprevalenceofanemiain childrenthatshowedintakeoftotaliron,hemeiron, non-hemeiron,andhemeirondensity belowthemedian.This associationprobablydoesnotoccurbecauseattheCMEI,as allchildrenbasicallyreceivethesamediet.
TheNationalSchoolFeedingProgram(ProgramaNacional deAlimentac¸ãoEscolar, PNAE)recommends that thefood servedatschoolshouldinclude7.7mg/dayofironfor chil-dren aged7---11 monthsand 4.9mg/day for children aged 1---3years.25 The medianintake ofiron foundin the CMEI
(3.10mg)iswellbelowthisrecommendation.Astudyof chil-drenaged6---59monthsinthestateofPernambucofounda
significant linear trendwitha reductionin anemia preva-lencewiththeincreasein thedensityof totaliron,heme iron, and nonheme iron in the children’s diet.11 The low
amount of iron consumed in the CMEI, together with the low supply of iron food sources, reflects the difficulty of implementing the PNAE recommendations andshows that school feeding has not been sufficient to contribute to the prevention of anemia in thechildren attending these schools.
Thisstudyattemptedtoassessallconditionsthatmight berelatedtoanemiadescribedinthescientificliterature, but thescope of thisstudy wastoinvestigate ironintake variables,whichareseldominvestigatedinmoststudiesdue tothedifficultyinobtainingsuchdata.
As limitations of the study, the fact that it is cross-sectionalshouldbementioned, whichmakesitimpossible tounderstand thecauseandeffectassociation ofanemia. Moreover, iron intake at home was not quantified. How-ever,considering thatthechildrenspentthewholedayat theCMEIandhadmostoftheirmealsthereallowsfor the assumptionthat the participationof thefood receivedat schoolispredominantinthesechildren’slives.Theauthors interviewedthemotherstoinvestigatethechildren’s feed-ingpracticesregardingthe consumptionofiron-richfoods athome.
Anemia,a resultof foodinsecuritypresent in the chil-dren’slives,reflectstheviolationoftherighttoregularand permanentaccesstoqualityfoodinsufficientquantity.The CMEImustpromotefoodandnutritionsecurity,with strate-giesthatpermeatehealth careandadequatefoodintake, becauseanemiaaffectedmorethan1/3ofthechildren,who showedlowfoodcontributionofiron.
TheCMEIarepotentialsitesforthecarryingoutof inter-ventions, considering thechildren remain therefull-time. Interdisciplinaryactions--- therolesofhealthandeducation professionalstogetherwithfamilies---canbethefoundation thatwillsupportbetterhealth forthechildren.The plan-ningofstrategiesandtrainingofinvolvedprofessionalsfor betterfoodironsupplyinCMEIareencouraged.
Factorsassociatedwithanemiaarealsoa resultof the influence of social, economic, and behavioral conditions of thepopulation that reflectonthe healthand nutrition of these individuals. Every action that benefits the chil-dren’shealthalsodependsoneconomic,political,andsocial restructuringofthecountry,whichcanstimulateadvances thatwillaffecteducation,employment,income,andaccess to health care. The strengthening and investing in such strategiesandprogramstopromotethefamilies’household foodsecuritywillindirectlypreventanemia.
Funding
Theresearchispartof thePROCAD/CasadinhoUFPR-UFPE projectofConselhoNacionaldeDesenvolvimentoCientifico e Tecnológico (CNPq), process No. 552448/2011-7. Capes Fellow.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.World Health Organization (WHO). Worldwide prevalence of anaemia 1993---2005: WHO Global database on anaemia. Geneva:WHO;2008.
2.KonstantynerT,TaddeiJA,PalmaD.Fatoresderiscodeanemia emlactentesmatriculadosemcrechespúblicasoufilantrópicas deSãoPaulo.RevNutr.2007;20:349---59.
3.World Health Organization (WHO). Iron deficiency anaemia: assessment, prevention and control: a guide for programme managers.Geneva:WHO;2001.
4.Konstantyner T, RomaOliveiraTC, de Aguiar Carrazedo Tad-dei JA. Risk factors for anemia among Brazilian infants from the2006NationalDemographicHealth Survey.Anemia. 2012;2012:850681.
5.AustinAM,FawziW,HillAG.AnaemiaamongEgyptianchildren between2000 and2005:trendsand predictors.MaternChild Nutr.2012;8:522---32.
6.Ayoya MA, Ngnie-Teta I, Séraphin MN, Mamadoultaibou A, Boldon E,Saint-Fleur JE, et al. Prevalence and risk factors ofanemiaamongchildren6---59monthsoldinHaiti.Anemia. 2013;2013:502968.
7.RodriguesVC,MendesBD,GozziA,SandriniF,SantanaRG, Mati-oliG.Irondeficiencyandprevalenceofanemiaandassociated factorsinchildrenattendingpublicdaycarecentersinwestern Paraná,Brazil.RevNutr.2011;24:407---20.
8.WorldHealthOrganization(WHO).Haemoglobinconcentrations forthediagnosisofanaemiaandassessmentofseverity.Vitamin andMineralNutritionInformationSystem.Geneva:WHO;2011.
9.Brasil. Ministério da Saúde. Secretaria de Atenc¸ão à Saúde. DepartamentodeAtenc¸ãoBásica.ProtocolosdoSistemade Vig-ilânciaAlimentareNutricional---SISVANnaassistênciaàsaúde. Brasília:MinistériodaSaúde;2008.
10.WorldHealthOrganization(WHO).TheWHOchildgrowth stan-dards.Geneva:WHO;2006.
11.OliveiraMA,OsórioMM,RaposoMC.Socioeconomicanddietary riskfactorsforanemiainchildrenaged6to59months.JPediatr (RioJ).2007;83:39---46.
12.LealLP,BatistaFilhoM,LiraPI,FigueiroaJN,OsórioMM. Preva-lenceofanemiaandassociatedfactorsinchildrenaged6---59 monthsinPernambuco,NortheasternBrazil.RevSaudePublica. 2011;45:457---66.
13.Osório MM, Lira PI, AshworthA. Factors associated with Hb concentrationin children aged 6---59 monthsin the Stateof Pernambuco,Brazil.BrJNutr.2004;91:307---15.
14.Brasil.Ministério daSaúde. PesquisaNacionalde Demografia eSaúdedaCrianc¸aedaMulher ---PNDS 2006:dimensõesdo processoreprodutivoedasaúdedacrianc¸a.Brasília:Ministério daSaúde;2009.
15.deCastroTG,Silva-NunesM,CondeWL,MunizPT,CardosoMA. AnemiaandirondeficiencyamongschoolchildrenintheWestern BrazilianAmazon:prevalenceandassociatedfactors.CadSaude Publica.2011;27:131---42.
16.SaraivaBC,Soares MC,SantosLC,PereiraSC,HortaPM.Iron deficiency and anemia are associated with low retinol lev-elsinchildrenaged1 to5years.JPediatr(RioJ). 2014;90: 593---9.
17.KonstantynerT,TaddeiJA,OliveiraMN,PalmaD,ColugnatiFA. Isolatedand combinedrisksforanemiainchildrenattending thenurseries ofdaycare centers.JPediatr (RioJ). 2009;85: 209---16.
18.Vieira RC, Ferreira HS. Prevalência de anemia em crianc¸as brasileiras, segundodiferentescenáriosepidemiológicos.Rev Nutr.2010;23:433---44.
19.CottaRM,OliveiraFdeC,MagalhãesKA,RibeiroAQ,Sant’Ana LF,PrioreSE,etal.Socialandbiologicaldeterminantsofiron deficiencyanemia.CadSaudePublica.2011;27:S309---20.
20.GondimSS,DinizAdaS,SoutoRA,BezerraRG,AlbuquerqueEC, PaivaAdeA.Magnitude,timetrendsandfactorsassociatewith anemiainchildreninthestateofParaíba,Brazil.RevSaude Publica.2012;46:649---56.
22.SpinelliMG,MarchioniDM,SouzaJM,SouzaSB,SzarfarcSC.Risk factorsforanemiaamong6-to12-month-oldchildreninBrazil. RevPanamSaludPublica.2005;17:84---91.
23.PessoaMC,JansenAK,Velásquez-MeléndezJG,LopesJD, Bein-nerMA.Prevalênciadeanemiaemcrianc¸asefatoresassociados emregiãourbana.REME.2011;15:54---61.
24.Vasconcelos PN, Cavalcanti DS, Leal LP, Osório MM, Batista Filho M. Time trends in anemia and associated factors in two age groups (6---23 and 24---59 months) in Pernambuco State, Brazil, 1997---2006. Cad Saude Publica. 2014;30: 1777---87.
25.FundoNacionaldeDesenvolvimentodaEducac¸ão(FNDE). Pro-grama Nacionalde Alimentac¸ãoEscolar ---PNAE. Referências
NutricionaisparaoProgramaNacionaldeAlimentac¸ãoEscolar DocumentoFinal.Brasília:FNDE;2009.
26.MattaIE,VeigaGV,BaiãoMR,SantosMM,LuizRR.Anemiaem crianc¸asmenoresdecincoanosquefreqüentamcreches públi-cas do município do Rio de Janeiro, Brasil. RevBras Saúde MaternInfant.2005;5:349---57.
27.CamilloCC,AmancioOM,VitalleMS,BragaJA,JulianoY. Ane-miaand nutritionalstatusofchildrenin day-carecentersin Guaxupé.RevAssocMedBras.2008;54:154---9.