www.jped.com.br
ORIGINAL
ARTICLE
Portuguese
cultural
adaptation
and
validation
of
the
Activities
Scale
for
Kids
(ASK)
夽
,
夽夽
Daniela
Paixão
a,∗,
Luís
Manuel
Cavalheiro
a,b,
Rui
Soles
Gonc
¸alves
a,b,
Pedro
Lopes
Ferreira
b,caPolytechnicInstituteofCoimbra,CoimbraHealthSchool,Coimbra,Portugal bCentreforHealthStudies&Research,UniversityofCoimbra,Coimbra,Portugal cSchoolofEconomics,UniversityofCoimbra,Coimbra,Portugal
Received24May2015;accepted23September2015 Availableonline3May2016
KEYWORDS
Child; Disability; Performance; Capability; Outcomemeasures
Abstract
Objectives: Themainpurposeofthecurrentstudywastoperformthecrosscultural
adapta-tionandvalidationoftheActivitiesScaleforKids(ASK)bothinitscapabilityandperformance
versionstotheEuropeanPortugueselanguagesoitcanbeusedinPortugalbyhealthcare
pro-fessionalsinchildrenfrom5to15yearsofagewithfunctionaldisabilitiesrelatedtospecific
healthconditions.
Methods: The cross-culturaladaptation ofASKfollowed theclassic sequentialmethodology
for linguistic equivalence.To test itsvalidity, internal consistency,and reproducibility,the
PortugueseversionofASKwasadministeredtogetherwiththeKINDLQuestionnaire(KINDL)to88
children(10±3yearsofage)withfunctionallimitations.Thetest---reteststudywasconducted
twoweeksapart.
Results: After obtaining the semantic and content validity, the Portuguese version ofASK
demonstrated goodlevels ofreproducibility(performance: intraclasscorrelationcoefficient
[ICC]=0.99;capability:ICC=0.98)andinternalconsistency(performance:˛=0.98;capability:
˛=0.97).ThecorrelationsbetweenASKandKINDLwerepositiveandmoderate.
Conclusions: ThePortugueseversionofASKshowedacceptablelevelsofvalidity,internal
con-sistency,andreproducibility;theauthorsrecommenditsuseinclinicalsettings.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
夽
Pleasecitethisarticleas:PaixãoD,CavalheiroLM,Gonc¸alvesRS,FerreiraPL.Portugueseculturaladaptationandvalidationofthe ActivitiesScaleforKids(ASK).JPediatr(RioJ).2016;92:367---73.
夽夽
StudyconductedatPolytechnicInstituteofCoimbra,CoimbraHealthSchool,Coimbra,Portugal. ∗Correspondingauthor.
E-mail:[email protected](D.Paixão). http://dx.doi.org/10.1016/j.jped.2015.09.010
PALAVRAS-CHAVE
Crianc¸a; Deficiência; Desempenho; Capacidade; Medidasdos resultados
Adaptac¸ãoàculturaportuguesaevalidac¸ãodaEscaladeAtividadesparaCrianc¸as (ASK)
Resumo
Objetivos: Oprincipalobjetivodesteestudofoirealizaraadaptac¸ãotransculturalparao
por-tuguêseuropeueavalidac¸ãodasversõesdecapacidadeedesempenhodaEscaladeAtividades
paraCrianc¸as(ActivityScaleforKids (ASK)),de formaquepossaserutilizada em Portugal
porprofissionaisdasaúdecomcrianc¸asde5a15anosdeidadecomdeficiênciasfuncionais
relacionadasadoenc¸asespecíficas.
Métodos: Aadaptac¸ãotransculturaldaASKseguiuametodologiasequencialclássicaparaobter
equivalêncialinguística.Paratestarsuavalidade,coerênciainternaereprodutibilidade,a
ver-sãoemportuguêsdaASKfoiadministradajuntamentecomoQuestionárioKINDL(KINDL) em
88 crianc¸as(10±3anosde idade)comlimitac¸ões funcionais.Oestudo deteste-retestefoi
realizadocomumintervalodeduassemanas.
Resultados: Após obter a validade semântica e de conteúdo, a versão em português da
ASK demonstrou bons níveis de reprodutibilidade (desempenho: coeficiente de correlac¸ão
intraclasse (CCI)=0,99; capacidade: CCI=0,98) e coerência interna (desempenho: ␣=0,98;
capacidade:␣=0,97).Ascorrelac¸õesentreaASKeoKINDLforampositivasemoderadas.
Conclusões: AversãoemportuguêsdaASKapresentouníveisaceitáveisdevalidade,coerência
internaereprodutibilidade,erecomendamosseuusoemambientesclínicos.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo
OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
The WorldHealth Organization estimated that 15%of the world population lives with disabilities.1 Therefore,
mea-suring disability is essential for developing programs and policies to promote the integration and participation of theseindividuals.1Similarly,toassesstheeffectivenessof
healthcare interventions, it is necessary to quantify the impactoffunctionallimitationsonactivityandparticipation oftheindividuals.2
Despite the efforts and the published studies, no measurement instrument covered all components of functionality.3,4 Recently, several outcome measures have
beendeveloped specificallyfor childrenwithdisabilities5;
however,fewareadaptedforthePortugueseculture. TheActivityScaleforKids(ASK)isaspecificmeasurefor thepediatricpopulation,intendedtoassessthedegreeof disabilityinchildrenaged5---15yearswithfunctional limi-tations,withinawiderangeofhealthconditions.Moreover, this measure has been shown to have good psychometric propertiesandsignificantclinical utility.2,5Itsclinical
util-ity is important, being a valid measure with correlation values between 0.82 (ASK---Performance [ASKp]) and 0.85 (ASK---Capability[ASKc])withtheChildhoodHealth Assess-mentQuestionnaire---CHAQ.Itpresentsgoodreproducibility values at 2 weeks (ICC=0.97 for ASKp and ICC=0.98 for ASKc) and a Cronbach alpha value of 0.99. It was also shown to be able to discriminate among different lev-els of disability.6 It has been widely referenced in the
literature.7---19
Oneofthefewchildoutcomemeasuresadaptedforthe PortuguesecultureistheKINDLquestionnaire.Itisageneric instrumentconceivedtomeasurequalityof lifeof sickor healthychildrenandadolescents,from4to17yearsofage.
Itisavailabletobeusedinthreeagegroups(4---6,7---13,and 14---17)andhasfiveversions,depending ontheage ofthe respondentandtheinformationsource(childrenorparents version).20
ThePortugueseversionofKINDLwasshowntobe seman-tically equivalent to the original measure; it offers good levelsofreliabilityandacceptablelevelsofvalidity.20
Themainobjectiveofthisstudywastoculturallyadapt theASKcandASKpmodulestoEuropeanPortugueseandto evaluatetheirvalidityandreliability.
Methods
Thepresentstudyproceededintwophases
Thefirstphasefollowedthesequentialapproach,commonly usedinthesetypeofstudiestoobtainalinguistically equiv-alent version.9,21,22 It includes the authorization given by
the author of the original instrument2 and its adaptation
forEuropeanPortugueselanguageandculture.
Aformalpermissionforthecross-culturaladaptationto PortuguesewasobtainedfromNancyYoung,thedeveloper ofASK.Thisprocesswasperformedaccordingtothestages guidelineusedinself-reportmeasures.6
• Forwardtranslation.TheoriginalversionofASKwas trans-lated into Portuguese by two independent Portuguese translatorsfluentinEnglish.
• Back-translation. Atranslator, native in Englishand flu-entinPortuguese,translatedtheconsensusversionback intoEnglish.Thisback-translationandallprevious trans-lations ofASK weretakenintoconsideration toreacha consensus,obtainingthesecondpreliminaryversion.This processwasdocumentedinawrittenreport.
• Contentvalidity.Anexpertreviewcommittee,composed bytwopediatricphysicaltherapistsandaphysician spe-cializedinpediatricphysicalmedicineandrehabilitation, reachedaconsensusonthetranslationofASK.Thisexpert committee meetingresulted in apre-final version. The finalstageofthecross-culturaladaptationofASKwasto cognitivelypre-testthequestionnaire.Childrenand par-entswereinterviewedtoassesswhethertheitemswere understandable.Toobtainageneralrepresentationofthe population,theinitialpanelwascomposedby15children withdifferentcharacteristicsandaparents’panel com-posedbyfourparentsofchildrenlessthan10yearsold; twoofthesechildrenwerehealthy.Afterfillingthe ques-tionnaire, each participant was asked topoint out any difficultiesinunderstandingorambiguitiesinthe transla-tion.
ThisstagecompletedthecreationofthePortuguese ver-sionofbothASKpandASKc.
The second phaseexamined the validityandreliability tests of the Portuguese version. Specifically, the authors assessedconstructvalidity,internalconsistency,and repro-ducibility.
Participants
A convenience sample collected at 11 healthcare institu-tions(hospitalsandpatientassociations)wasused,including 88 children aged between 5 and 15 years with various types of functional disorders (neuromuscular, orthope-dic/traumatologyand/orrheumatology,cardio-respiratory, orothers).Childrenwithcognitivedeficitsandchildrenwith sensorial changes that would prevent them from answer-ingorunderstandingthemeasurewereexcludedfromthe analysis.2
Thehealthcareinstitutionsobtainedapprovalfromtheir respective institutional review boards, and consent was obtainedfromthedifferentparticipants.Beforeeach face-to-face interview there was a explanation of the study, includingitsgoals,confidentiality andparticipation condi-tions.
Datacollection
The protocols were mailed to the institutions that had agreed toparticipate, along with pre-stamped envelopes for the answers. One physiotherapist of each institution wasresponsiblefor selectingthesampleelementsandfor administeringtheprotocolsduringthedefinedperiods.
Childrenupto10yearsrespondedtothequestionnaire in the presence of adults (physical therapist, parents, or caregivers);nonetheless,theansweralwayscamefromthe child.Childrenolderthan10yearsreadandrespondedby themselves,exceptinthecase ofthosewhohadvisualor motordisabilitiesthatwouldpreventthemfromresponding.
The data collectionprotocol containedboth ASK mod-ules,thePortugueseversionofKINDL,andaformtocollect some questions of patient characteristics, including two clinical questions (regarding mobility needs and health conditions).The ASK wasapplied twice tothe same par-ticipants withan interval of one totwo weeks, toassess reproducibility.
Instruments
ThePortugueseversionsofbothASKandKINDLwere admin-istered.
TheASKisaspecificpediatricmeasurecomposedoftwo modules:ASKc,whichreflectswhatthechildisabletodo inhis/herdailyenvironment,andASKp,whichreflectswhat thechildactuallydoesonhis/herdailyenvironment.
Both modules are organized in seven domains (per-sonalcare,dressing,otherskills,locomotion,play,standing skills, and transfers) containing 30 items each, identical butwithdifferentansweroptions.5Thisinstrumentis
self-administeredforchildren aged10 yearsor older. Children under10yearsofagehavetobehelpedbytheircaregivers, buttheanswershavetobeexclusivelygivenbythechildren. TheASK cannotbeappliedonchildren thatareunableto understandwhatisbeingasked.
Inbothmodules,thesummaryscoreswerecalculatedby themeanofthe answers(0---4points),andthe resultwas reportedasapercentagescore(range0---100),where100% indicatesfullphysicalfunction.6
The KINDL measures six dimensions of quality of life (physical and emotional well-being, self-esteem, family, friends,andschool).Regardingtheagegroup,threeversions ofthequestionnairewereused:Kiddy,forchildrenaged4---6 years(interview);Kid,forchildrenaged7---13;andKiddo,for teenagers(14---17).20
Individualdimensionscorescanbecalculatedbyadding theresponsesgiventothequestionstransformedtoa pos-itivescaleof0---100,accordingtotheKINDLmanual.23 The
totalscore can beobtained by the sumof the dimension scores,wherehighervaluesindicatedbetterqualityoflife. Reversescoring wasappliedtosome items,sothathigher itemscoresrepresentbetterqualityoflife.20
Statisticalanalysis
Thecharacteristicsofstudyparticipantsweresummarized usingdescriptivestatisticsofcentraltendency,dispersion, frequencies, and percentages, according to the type of variables.
TheconstructvaliditywasassessedanalyzingPearson’s correlation coefficients (r) obtained between the dimen-sionsofKINDLandASK.Theinterpretationofthecorrelation valueswasperformed basedonCohen’scriteria: verylow correlation(≤0.19);low(between0.20and0.39);moderate (between0.40and0.69);high(between0.70and0.89),and veryhigh(forvalues≥0.90).24Student’st-testwasalsoused
tocompare themeans of ASKdimensions between groups formedbythetwoclinicalquestions.
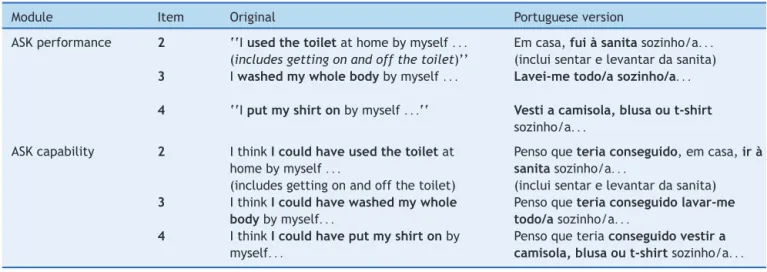
Table1 Exampleofasub-sampleoftheoriginalASKandadaptedASKitems.
Module Item Original Portugueseversion
ASKperformance 2 ‘‘Iusedthetoiletathomebymyself...
(includesgettingonandoffthetoilet)’’
Emcasa,fuiàsanitasozinho/a...
(incluisentarelevantardasanita)
3 Iwashedmywholebodybymyself... Lavei-metodo/asozinho/a...
4 ‘‘Iputmyshirtonbymyself...‘‘ Vestiacamisola,blusaout-shirt sozinho/a...
ASKcapability 2 IthinkIcouldhaveusedthetoiletat
homebymyself...
(includesgettingonandoffthetoilet)
Pensoqueteriaconseguido,emcasa,irà
sanitasozinho/a...
(incluisentarelevantardasanita)
3 IthinkIcouldhavewashedmywhole
bodybymyself...
Pensoqueteriaconseguidolavar-me
todo/asozinho/a...
4 IthinkIcouldhaveputmyshirtonby
myself...
Pensoqueteriaconseguidovestira
camisola,blusaout-shirtsozinho/a...
ASK,ActivitiesScaleforKids.
individuals withneuromuscularconditions and/or needing supporttomoveshouldhaveworseASKscores.
To calculate the reproducibility we used the intra-classcorrelation coefficient (ICC)for agreement,formula 2.1.Values higher than or equal to0.70 were considered acceptable.25 The internal consistency of ASK was tested
usingCronbach’salpha.Valueshigherthanorequalto0.70 wereconsideredacceptable.25
Forthestatisticalanalysis,SPSSversion18.0forWindows wasused(Inc.Released2009.PASWStatisticsforWindows, version18.0,IL,USA).p-Valueslowerthan0.05were con-sideredstatisticallysignificant.
Results
Cross-culturaladaptation
ASKwassuccessfullycross-culturallyadaptedintoEuropean Portuguese.Thechildrenpanelwascomposedof15children (eightfemales),andnineofwhomhadunilateralor bilat-eralspasticcerebral palsy.The ASKwascompletedbythe children in 34±9min. However, during thisprocess some minordifficulties wereobservedregardingthemeaningof theterms‘‘blouse,’’‘‘shirt,’’and‘‘brace’’.Inthesecases, multiplesynonymswereused,toincludealloptions,forboth
Portuguese versions of ASK. The item 29 of ASKccreated somedisagreementinthetranslationprocessconcerningthe sentencestructure.Astherecommendationsofthe transla-torswerenotfullyaccepted,itwasdecidedtocombinethe proposalsintoanewsolution,moresimpleandclear.Finally, allthemembersoftheexpertcommitteeagreedwiththe pre-finalversion.
Nochangesresultedfromeithertheexpert committee, childrenpanel,orparentspanel(Table1).Thelengthofthe protocolmighthavebeen,insomecases,considered incon-venient,butitwasgenerallyconsideredeasytounderstand andrespond.
Constructvalidity
For the validity study, a sample of 88 children aged 10.2±3.2yearswasused.Table2presentsthemain char-acteristicsofthesample.
Toaddressconstructvalidity,theASKscoreswere com-paredwithtwoclinicaloutcomes:needformobilitysupport andhealthconditions,aswellasthecorrelationsbetween ASKandKINDLdifferentdimensions.
ThestudyoftherelationshipbetweenASKresponsesand theneedforsupport(Table3)showedthatindividualswith
Table2 Samplevalidationstudy(n=88).
Characteristics Frequencies Percentage
Gender Male 48 54.5%
Female 40 45.5%
Educationallevel Prescholar 13 14.8%
Firstcycle 30 34.1%
Secondorthirdcycle(secondaryschool) 45 51.1%
Formcompletion Autoadministrated 39 44.3%
Byinterview 49 55.7%
Healthcondition Neuromuscular 76 87.4%
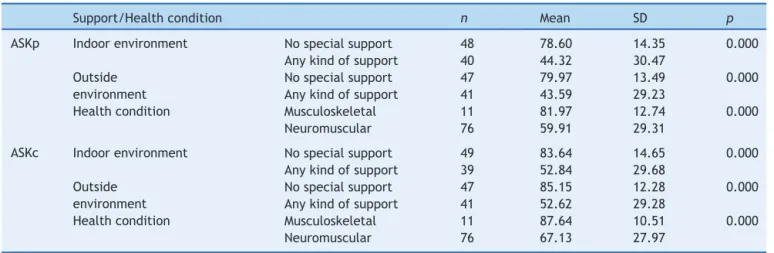
Table3 ASKvsneedofsupportandhealthcondition(n=88).
Support/Healthcondition n Mean SD p
ASKp Indoorenvironment Nospecialsupport 48 78.60 14.35 0.000
Anykindofsupport 40 44.32 30.47
Outside environment
Nospecialsupport 47 79.97 13.49 0.000
Anykindofsupport 41 43.59 29.23
Healthcondition Musculoskeletal 11 81.97 12.74 0.000
Neuromuscular 76 59.91 29.31
ASKc Indoorenvironment Nospecialsupport 49 83.64 14.65 0.000
Anykindofsupport 39 52.84 29.68
Outside environment
Nospecialsupport 47 85.15 12.28 0.000
Anykindofsupport 41 52.62 29.28
Healthcondition Musculoskeletal 11 87.64 10.51 0.000
Neuromuscular 76 67.13 27.97
ASK,ActivitiesScaleforKids.
Table4 ASKvsKINDL(n=57).
Kindla PWB EWB SE FM FR SC TT
ASKp r 0.023 0.559 0.538 0.386 0.624 0.343 0.631
p 0.867 0.000 0.000 0.003 0.000 0.009 0.000
ASKc r 0.093 0.464 0.396 0.386 0.440 0.292 0.523
p 0.493 0.000 0.002 0.003 0.001 0.027 0.000
ASK,ActivitiesScaleforKids.
a KINDLdimensions:PWB,physicalwell-being;EWB,emotionalwell-being;SE,self-esteem;FM,family;FR,friends;SC,school;TT,
KINDLtotal.
higherASKscores(ASKpandASKc)werelesslikelytorequire anytypeofsupporttomove.
Table3alsopresentstherelationshipbetweenASKscores andindividuals’healthcondition.Itwasevidentthatthose whohad higherASK scores were alsomore likelytohave musculoskeletaldisorders.
When confronting ASKand KINDL, positive correlations wereobserved between ASKpand ASKcandall theKINDL dimensions, withtheexception ofthe physical well-being dimension.Mostofthesecorrelationswerelowand/or mod-erate(Table4).
Reliability
Regardingthe internal consistency ofASK Portuguese ver-sion,acceptable valueswerefound forboth for ASKpand ASKc.
The reproducibility valuesof ASKpand ASKcwere also foundtobeacceptable (Table5),afterthequestionnaires werecompletedtwice,oneortwoweeksapart.
Table 5 ASK Internal consistency and reproducibility of
PortugueseASK(n=88).
ASK Cronbach˛ ICC Lowerbound Upperbound
ASKp 0.980 0.986 0.979 0.991
ASKc 0.972 0.978 0.967 0.986
ASK,ActivitiesScaleforKids.
Discussion
Consideringtheresultsfromtheconsensuspanels,clinical reviewpanel,andthepanelsofchildrenandparents,itcan beaffirmedthatsemanticandcontentequivalencebetween thetranslatedversionofASKandtheoriginalversionwere reached.
In general, this measure was considered clear, under-standable,andappropriateforapediatricpopulation.The onlydownsidewasthefactthatitisarelativelyextensive measure,especiallywhenapplyingbothversionstogether, asshownbythemeantimeforcompletionofthetwo ver-sions(33.4min).TheauthorsconcludethatthePortuguese versionofASKpresentsanacceptablelevelofcontent valid-ity.
Regardingtheexistenceofsupportreceivedbychildren tomove,itwasobservedthatbothinASKpandASKc,the majorityofindividuals(between53%and56%)reportednot touse any support for moving both indoors and outside. These findings appear to indicate a correlation between whatchildrenreallydoin theirday-to-dayand whatthey thinktheycando.
toshowalowerdegreeoffunctionalityandthereforehave lowerscoresinASK(Table3).
Itwasalsoexpectedtofindstatisticallysignificant differ-encesbetweenchildrenwithmusculoskeletaldisordersand childrenwithneuromuscularconditions,assumingthat neu-romuscularconditionsresultinmoreincapacitatingstages.5
TheresultsobtainedforbothversionsofASKdidnotreject thishypothesis.
For the assessment of validity, the relations between ASK and KINDL were also analyzed. The assumption was the existence of positive correlation values between the confrontedconstructs,supportingthehypothesisthatmore favorablehealthconditionsshouldcorrespondtobetter lev-elsofcapacityandperformance.
The choiceof KINDLwasduetothelack ofa standard measuresuitableforthePortugueselanguageandculture. Furthermore,aPortugueseversionoftheKINDLisavailable, coveringtherequiredages.Additionally,asimilarstrategy wasusedinthestudyoftheoriginalversion.2
When analyzingthevaluesof thecorrelationsbetween KINDLTotalandbothASKpandASKcscores,theexistenceof positiveandmoderatecorrelationswasobserved(Table5), thus confirming the hypothesis that children with better degreeoffunctionalityalsopresentabetterlevelof qual-ityof life. A correlation of the two versions of ASK with alldimensionsof theKINDLwasalsoobserved,exceptfor the physical well-being dimension. To try to explain this finding, the authors compared the questionsof the phys-ical well-being dimension of KINDL and the items of the ASK,andobservedthatthefourquestionsofphysical well-being dimension of KINDL regard feeling ill, body aches, tired,orstrong,whiletheitemsofASKarerelatedwiththe performanceof dailyactivities. However,the KINDL phys-icaldimensioncan matchconcepts in somewaydifferent fromASKones.Inturn,thefactthatthesamplecomprised approximately18%individualswithcerebralpalsymay rep-resentabiasintheresults.Itisknownthatchildrentendto overvaluetheirhealthstatus,inparticularthosewith cere-bralpalsy,whohaveadifferentexpectationinrelation to theirphysicalabilitiesincomparisontoindividualswhohave anacquireddisability.
Despite not including questions related to KINDL emotionalwell-beingandself-esteemdimensions,the cor-relation values obtained for both ASKp and ASKc, albeit weaktomoderate, wereacceptable (Table 4).These val-uescanbejustifiedbythedifferenceofconstructsandby the fact that the sample was composed of children who perceivedtheirincapacitiesasslighttomoderate,leadingto thehypothesisofgoodlevelsofself-esteemandemotional well-being.Bjorson13corroboratesthisassumption,
evidenc-ingthat theperformanceof activities positivelyinfluence physicalhealth,behavior, andemotional conditionin chil-drenwithcerebralpalsy.
In the familydimension, therewasa weak correlation forbothASKpandASKc(r=0.386).Thistypeofcorrelation wasalreadyexpected,since ASK does notconsiderissues directlyrelatedtothefamily.Inthefriendsdimension, mod-eratecorrelationvalues(rbetween0.624and0.440)were observedforbothASKcandASKp.Thisresultwasexpected, giventhatASKhasquestionsthatdirectlyfocusonthechild’s friends.Finally,intheschooldimension,onlyaweak corre-lationwithASKpwasobserved (r=0.343), somethingthat
was also expected, sinceASK does not present questions relatedtoschoolperformance.
Regarding the internal consistency and reproducibility of ASK, theresults showed acceptable values.The values of the ICC obtained for both ASKc (ICC=0.978) and ASKp (ICC=0.986)wereinagreement,representingahigh repro-ducibilityaccordingtothecriteriapreviouslylisted.25When
comparedwiththereproducibilitylevelsoftheoriginal ver-sion,itwasverifiedthattheresultsofthetest---retestwere consistent,sincethevalueoftheICCin theoriginal study was0.97forbothversions.2,6Itcanbeconsideredthatthe
PortugueseversionofASKshowsgoodlevelsof reproducibil-ity.
Regardinginternalconsistency,resultsforeachASK ver-sion(˛=0.980forASKpand˛=0.972forASKc)weresimilar
totheoriginalresults,whichwereconsideredtobehigh.25
Thesefiguressuggestthatallitemsofthescalemeasurethe sameconstructs.
The main limitations of this studywere related tothe extensionoftheprotocolused,includingbothASKversions, KINDLquestionnaire,andsocio-demographicquestions. Fur-thermore,thesamplesizedidnotallowfortheperformance ofafactoranalysistotesttheconstructvalidity.
Given the results, the authors conclude that the Portuguese ASK versions present semantic and content equivalenceswiththeoriginalversion,aswellasacceptable valuesofvalidityandreliability.Finally,theypropose fur-therstudies todeepen thepresentfindingsandtofurther explore the psychometric characteristics of the measure, includingtheassessmentofitsresponsiveness.
The authors considerthat thePortuguese ASK versions canbeusedbothinclinicalpracticeandresearch.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The authorswouldliketothankthestafffromthehealth careinstitutions.Furthermore,thechildrenandparentswho participatedinthisstudydeservedeeprecognition.
References
1.WorldHealthOrganization(WHO).Worldreportondisability. Geneve:WHO;2011.p.7---8.
2.Young NL, WilliamsJI, YoshidaKK, Wright JG. Measurement propertiesof theActivities Scalefor Kids. JClinEpidemiol. 2000;53:125---37.
3.WhiteneckG,DijkersMP.Difficulttomeasureconstructs: con-ceptualandmethodologicalissuesconcerningparticipationand environmentalfactors.ArchPhysMedRehabil.2009;90:S22---35. 4.HolsbeekeL,KetelaarM,SchoemakerMM,GorterJW.Capacity, capability,andperformance:differentconstructsorthreeofa kind.ArchPhysMedRehabil.2009;90:849---55.
5.PlintAC,GabouryI,OwenJ,YoungNL.ActivitiesScaleforKids: ananalysisofnormals.JPediatrOrthop.2003;23:788---90. 6.YoungNL.TheActivitiesScaleForKids©(ASK©).ManualUser’s
7.HarveyA,RobinJ,MorrisME,GrahamHK,BakerR.A system-aticreviewofmeasuresofactivitylimitationforchildrenwith cerebralpalsy.DevMedChildNeurol.2008;50:190---8. 8.Capio CM, Sit CH, Abernethy B, Rotor ER. Physical activity
measurementinstrumentsforchildrenwithcerebralpalsy:a systematicreview.DevMedChildNeurol.2010;52:908---16. 9.vonKeyserlingk C, BoutisK, Willan AR, Hopkins RB, Goeree
R.Cost-effectivenessanalysisofcastversussplintinchildren withacceptablyangulatedwristfractures.IntJTechnolAssess HealthCare.2011;27:101---7.
10.PostansN,WrightP,BromwichW,WilkinsonI,FarmerSE,Swain I.ThecombinedeffectofDynamicsplintingandneuromuscular electrical stimulation in reducing wrist and elbow contrac-turesinsixchildrenwithcerebralpalsy.ProsthetOrthotInt. 2010;34:10---9.
11.Groen WG, van der Net J, Helders PJ, Fischer K. Devel-opment and preliminary testing of a Paediatric Version of the Haemophilia Activities List (PEDHAL). Haemophilia. 2010;16:281---9.
12.Boutis K, Willan A, Babyn P, Goeree R, Howard A. Cast versussplint in children withminimally angulated fractures of the distal radius: a randomized controlled trial. CMAJ. 2010;182:1507---12.
13.MoreauNG,SimpsonKN,TeefeySA,DamianoDL.Muscle archi-tecturepredictsmaximumstrengthandisrelatedtoactivity levelsincerebralpalsy.PhysTher.2010;90:1619---30.
14.Bjornson KF, Belza B, Kartin D, Logsdon R, McLaughlin J, ThompsonEA.Therelationship ofphysical activitytohealth statusandqualityoflifeincerebralpalsy.PediatrPhysTher. 2008;20:247---53.
15.PalisanoRJ, CopelandWP,GaluppiBE.Performanceof phys-icalactivities byadolescentswithcerebral palsy.Phys Ther. 2007;87:77---87.
16.Wai EK,Young NL, FeldmanBM,Badley EM, Wright JG. The relationship between function, self-perception, and spinal
deformity:implications fortreatmentofscoliosisinchildren withspinabifida.JPediatrOrthop.2005;25:64---9.
17.StephensS,Singh-GrewalD,Bar-OrO,BeyeneJ,CameronB, Leblanc CM, et al. Reliability of exercise testing and func-tionalactivityquestionnairesinchildrenwithjuvenilearthritis. ArthritisRheum.2007;57:1446---52.
18.KingG,LawM,KingS,RosenbaumP,KertoyMK,YoungNL.A conceptualmodelofthefactorsaffectingtherecreationand leisureparticipationofchildrenwithdisabilities.PhysOccup TherPediatr.2003;23:63---90.
19.WrightJG,SmithPL,OwenJL,FehlingsD.Assessingfunctional outcomes of childrenwithmuscular dystrophy and scoliosis: theMuscularDystrophySpineQuestionnaire.JPediatrOrthop. 2008;28:840---5.
20.FerreiraPL,AlmeidaM,PiscoM,CavalheiroL. Qualityoflife ofchildrenandadolescents.Culturaladaptationandvalidation of the Portuguese version of the KINDL. Acta Pediatr Port. 2006;37:125---44.
21.KlingbeilH,BaerHR,WilsonPE.Agingwithadisability.Arch PhysMedRehabil.2004;85:S68---73,quizS74-5.
22.BeatonDE,BombardierC,GuilleminF,FerrazMB.Guidelines fortheprocessofcross-culturaladaptationofself-report meas-ures.Spine(PhilaPa1976).2000;25:3186---91.
23.Ravens-Sieberer U, Bullinger M. KINDLR - Questionnaire for MeasuringHealth-RelatedQualityofLifeinChildrenand Ado-lescents--- RevisedVersion---Manual,2000.[cited15Jan2014]. Available from: http://www.kindl.org/english/language-versions/portuguese/.
24.Cohen L, Holliday MG. Statistics for social scientists: an introductorytext withcomputer programs in basic. London: Hagerstown:Harper&Row;1982.