JPediatr(RioJ).2016;92(4):374---380
www.jped.com.br
ORIGINAL
ARTICLE
Neonatal
screening
for
severe
combined
immunodeficiency
in
Brazil
夽
,
夽夽
Marilia
Pyles
Patto
Kanegae
a,
Lucila
Akune
Barreiros
a,
Juliana
Themudo
Lessa
Mazzucchelli
b,
Sonia
Marchezi
Hadachi
c,
Laura
Maria
de
Figueiredo
Ferreira
Guilhoto
c,
Ana
Lúcia
Acquesta
d,
Isabel
Rugue
Genov
b,e,
Silvia
Maia
Holanda
f,
Regina
Sumiko
Watanabe
Di
Gesu
g,
Ana
Lucia
Goulart
b,
Amélia
Miyashiro
Nunes
dos
Santos
b,
Newton
Bellesi
h,
Beatriz
Tavares
Costa-Carvalho
b,
Antonio
Condino-Neto
a,∗aDepartmentofImmunology,InstitutodeCiênciasBiomédicas,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil bDepartmentofPediatrics,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
cAPAE-SP,SãoPaulo,SP,Brazil
dHospitalGeraldePirajussara,SãoPaulo,SP,Brazil eHospitalPimentasBonsucesso,Guarulhos,SP,Brazil
fAmparoMaternal,SãoPaulo,SP,Brazil
gHospitalNossaSenhoradaConceic¸ão,PortoAlegre,RS,Brazil
hClínicadeMedicinaPreventivadoPará(CLIMEP),Belém,PA,Brazil
Received1July2015;accepted5October2015 Availableonline18May2016
KEYWORDS
SCID;
Neonatalscreening; TRECs;
Tlymphocytes; Combined
immunodeficiency; Primary
immunodeficiency
Abstract
Objective: Toapply,inBrazil,theT-cellreceptorexcisioncircles(TRECs)quantification tech-nique usingreal-time polymerasechain reaction innewborn screeningfor severe combined immunodeficiencyandassessthefeasibilityofimplementingitonalargescaleinBrazil. Methods: 8715newbornbloodsampleswerecollectedonfilterpaperand,afterDNAelution, TRECswerequantifiedbyreal-timepolymerasechainreaction.Thecutoffvaluetodetermine whetherasamplewasabnormalwasdeterminedbyROCcurveanalysis,usingSSPS.
Results: Theconcentration of TRECs in8,682 samples rangedfrom 2to 2,181TRECs/L of blood,withmeanandmedianof324and259TRECs/L,respectively.Forty-nine(0.56%)samples werebelowthecutoff(30TRECs/L)andwerereanalyzed.Four(0.05%)sampleshadabnormal results(between16and29TRECs/L).Samplesfrompatientspreviouslyidentifiedashaving severecombinedimmunodeficiencyorDiGeorgesyndromewereusedtovalidatetheassayand
夽 Pleasecitethisarticleas:KanegaeMP,BarreirosLA,MazzucchelliJT,HadachiSM,GuilhotoLM,AcquestaAL,etal.Neonatalscreening
forseverecombinedimmunodeficiencyinBrazil.JPediatr(RioJ).2016;92:374---80.
夽夽ThisstudywascarriedoutattheDepartmentofImmunology,InstitutodeCiênciasBiomédicas,UniversidadedeSãoPaulo(USP),São
Paulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](A.Condino-Neto).
http://dx.doi.org/10.1016/j.jped.2015.10.006
allofthemshowedTRECsbelowthecutoff.PreterminfantshadlowerlevelsofTRECsthan full-termneonates.TheROCcurveshowedacutoffof26TRECs/L,with100%sensitivityfor detectingseverecombinedimmunodeficiency.Usingthisvalue,retestandreferralrateswere 0.43%(37samples)and0.03%(3samples),respectively.
Conclusion: Thetechniqueisreliableandcanbeappliedonalargescaleafterthetrainingof technicalteamsthroughoutBrazil.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradePediatria.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
PALAVRAS-CHAVE
SCID;
Triagemneonatal; TRECs;
LinfócitosT; Imunodeficiência combinada; Imunodeficiência primária
TriagemneonatalparaimunodeficiênciacombinadagravenoBrasil
Resumo
Objetivo: aplicarnoBrasilatécnicadequantificac¸ãodeT-cellReceptorExcisionCircles(TRECs) porpolymerasechainreactionemtemporealparatriagemneonataldeimunodeficiência com-binadagrave(SCID)eavaliarseépossívelrealizá-laemlargaescalaemnossopaís.
Métodos: foramcoletadas8.715amostrasdesanguederecém-nascidosempapelfiltroe,após eluic¸ãodoDNA,osTRECsforamquantificadosporpolymerasechainreactionemtemporeal. Ovalordecorteparadeterminarseumaamostraéanormalfoideterminadopelaanálisede curvaROCutilizando-seoprogramaSSPS.
Resultados: aconcentrac¸ãodeTRECs em 8.682 amostrasanalisadas variouentre 2e2.181 TRECs/L de sangue, com média e mediana de 324 e 259 TRECs/L, respectivamente. 49 (0,56%) amostras ficaram abaixo do valor de corte (30 TRECs/L) e foram requantifi-cadas.Quatro(0,05%)mantiveramresultados anormais(entre 16 e29TRECs/L).Amostras depacientescomdiagnósticoclínicopréviodeimunodeficiênciacombinadagraveesíndrome deDiGeorgeforamutilizadasparavalidaroensaioetodasapresentaramconcentrac¸ãodeTRECs abaixodovalordecorte.Recém-nascidosprematurosapresentarammenoresníveisdeTRECs comparadosaosnascidosatermo.UtilizandoacurvaROCemnossosdados,chegamosaovalor decortede26TRECs/L,comsensibilidadede100%paradetecc¸ãodeimunodeficiência combi-nadagrave.Utilizandoestevalor,astaxasderepetic¸ãoeencaminhamento,ficaramem0,43% (37amostras)e0,03%(3amostras),respectivamente.
Conclusão: A técnicaé factível e pode ser implantada em larga escala, após treinamento técnicodasequipesenvolvidas.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileiradePediatria.Este ´
eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
Introduction
Severe combined immunodeficiencies (SCID) comprises a heterogeneous group of diseases characterized by severe defectsinthedevelopmentandfunctionofT,B,andNK lym-phocytes.Theyarerecognizedaspediatricemergencies,as theyleadtosevere andrecurrentinfectionsandarefatal inthefirsttwoyearsoflife,ifnotdiagnosedand treated adequately.1,2
Due to the disease severity and the urgency in diag-nosis and treatment, in 2005, United States researchers developedthenewbornscreening(NBS)forSCID,which con-sistsofquantifyingT-cellreceptorexcisioncircles(TRECs) using real-time polymerase chain reaction (PCR) (qRT-PCR).3,4 TRECs are small circular pieces of DNA formed duringnormalthymicprocessing,whenT-cellreceptorgene rearrangementoccurs.Astheydonotreplicateduringcell division,theyworkasmarkers forthenumberof‘‘naïve’’ T-cellsrecentlyemigratedfromthe thymus, andtheyare reducedinallformsofSCID.5
Inmostcases,NBSistheonlywaytodetectSCIDbefore infectionsoccur,asmorethan80%ofcaseshavenofamily historyofprimaryimmunodeficiency.6
A significant altered finding observed after the devel-opmentof neonatal screening was the diseaseincidence. As many children die before the diagnosis is attained, theincidenceofSCIDwasestimatedat0.10/10,000;after theAmerican experience,this figure is currently close to 0.17/10,000(1:58,000),oralmosttwo-foldhigher.6,7
InBrazil,thereisnoneonatalscreeningtestforprimary immunodeficienciesappliedduringmedicalroutine assess-mentandthediagnosisofthesediseasesfallsshortofwhat isrequired.8---10 For thisreason,the aimof this study was to apply the TRECs quantification technique by qRT-PCR in the NBS for severe combined immunodeficiencies and assess whether it is possible to do soon a large scale in Brazil.
Methods
376 KanegaeMPetal.
partofthecurrentroutinefornewbornscreening.Samples fromchildrenborninthreematernityservicesofhospitals andAPAEdeSãoPaulo(APAE-SP),locatedinthe metropoli-tan region of São Paulo, aswell as samples collected at ClínicadeMedicinaPreventivadoPará(CLIMEP)were ana-lyzed.
Disksmeasuring3.2mm indiameter werecut from fil-terpaperandwereaddedtoa96-wellpolypropyleneplate, wheretheDNAelutionprocedurewascarriedout,as pre-viouslydescribed.3Allplates,inadditiontotheneonates’ samples,hadapositivecontrol(adult bloodwithlow lev-elsofTRECs),andano-targetcontrol(pieceoffilterpaper withno sample). The qRT-PCR reaction for TRECs and/or beta-actin was performed as described.3,11 All reagents werepurchasedfromLifeTechnologies®(LifeTechnologies,
USA).
Initially,acutoffvalueof30TRECs/Lofbloodwas arbi-trarily used to determine whether a sample wasnormal, basedonthevalueprovidedbyBakeretal.of25TRECs/L. In cases where the result was below this value, a new pieceofthesamesamplehaditsTRECsanalysisrepeated, accompanied by beta-actin analysis, as extraction con-trol. After the second analysis, the samples with values <30TRECs/L and beta-actin >8000/L were considered abnormal,andpatientswerereferredtoapediatric immu-nologistforconsultation andconfirmatorytests(complete bloodcountandmeasurementofT,BlymphocytesandNK cells).Those withTRECs <30/Land beta-actin<8000/L wereclassifiedasinconclusiveresultandanewsamplewas requested.
Dataanalysiswascarriedoutusingdescriptivestatistics. AfterapplyingtheKolmogorov---Smirnovtest,thedatawere notnormallydistributedandwerethusshownasmedianand interquartile values. Comparison of TREC concentrations betweenfull-term and pretermnewborns wasestablished usingtheMann---Whitneytest, utilizing GraphPadPrism5.0 software(GraphPadPrism,USA).Thecutoffvalueto deter-minewhethera sample wasabnormalwasdeterminedby theROC curve analysis(area underthe curve) usingSSPS software(IBMCorp.Released 2013,IBMSPSSStatisticsfor Windows,Version22.0,NY,USA).
Results
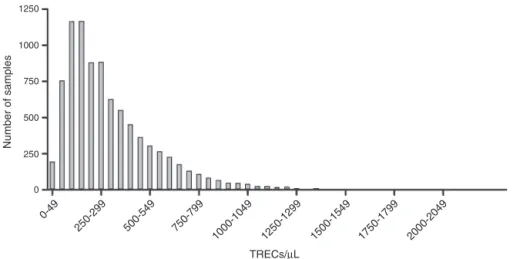
Samples were collected from 8,715 newborns, of whom 3,353(38%)werefromCLIMEPandtherestfromhospitals locatedinthemetropolitanregionofSãoPaulo.Ofthetotal, 33 were considered inadequate as they were inappropri-atelycollected.Thus,8,682sampleswereanalyzedforthe concentration of TRECs, and the valuesin the first quan-tificationvariedfrom2to2,181TRECs/Lofblood,witha meanandmedianvalue of324and259TRECs/L, respec-tively. Following the established protocol, samples below the cutoff value (30TRECs/uL) were reanalyzed. Thus, 49(0.56%)sampleswererequantifiedandonlyfour(0.05%) hadabnormalresults,withTRECs between16 and29/L. Among thesefoursamples,onewasfroma 27-weekmale newborn(24TRECs/L),whichcouldnotbelocatedforthe protocoltobecompleted.Thethreeremaininginfantswere assessedandsubmittedtothelymphocytenumber evalua-tion,whose resultswerenormalin allcases.Fig.1shows thedistributionofsamplesaccording totheconcentration ofTRECsobtainedatthefirstanalysis.
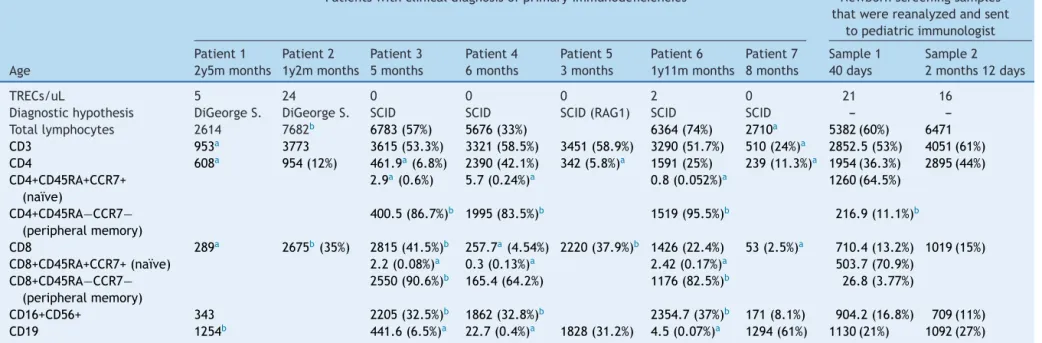
Toverifyassayefficacy,samplesfrompatientspreviously diagnosed withSCID (n=5)and DiGeorge syndrome(n=2) wereanalyzedandusedascontrols.AllSCIDsamplesshowed TRECsvaluesbelow3TRECs/L,andtheDiGeorgesamples showedresultsof5and24TRECs/L(Table1).
PartofthesamplesfromCLIMEP(2,416)containeddata ongestationalage:9.9%(239)ofthenewbornswerepreterm (30---36weeksgestationalage).Thatallowedthe compari-son of the TRECs concentration between the twogroups, which allowed the conclusion that preterm infants have lowerTRECslevelsthanfull-termnewborns(Fig.2).
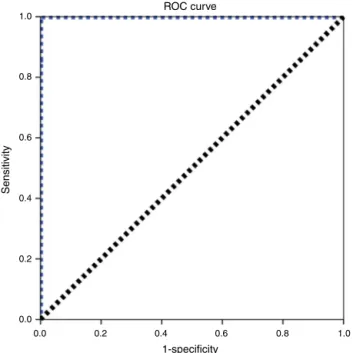
Arbitrarilyusing30TRECs/Lastheinitialcutoffvalue, a repetition rate of 0.56% wasfound (49 samples). After the second measurement, only 4 samples remained with abnormal values, which resulted in a referral rate to a specializedpediatricserviceof0.05%.When analyzingthe ROCcurvefortheseconditions(Fig.3),thecutoffvalueof 26TRECs/L wasobtained, withan areaunder the curve of 1.00and100% sensitivityfor detecting SCID.Using this value, theretesting andreferral rates wererecalculated,
1250
1000
750
500
Number of samples
250
0
0-49
250-299 500-549 750-799
1000-1049 1250-1299 1500-1549 1750-1799 2000-2049
TRECs/µL
screening
for
SCID
377
Table1 Immunophenotypingoflymphocytesinpatientswithclinicaldiagnosisofprimaryimmunodeficienciesandsamplessenttopediatricimmunologistforevaluationafter alteredneonatalscreening.
Patientswithclinicaldiagnosisofprimaryimmunodeficiencies Newbornscreeningsamples thatwerereanalyzedandsent
topediatricimmunologist
Patient1 Patient2 Patient3 Patient4 Patient5 Patient6 Patient7 Sample1 Sample2
Age 2y5mmonths 1y2mmonths 5months 6months 3months 1y11mmonths 8months 40days 2months12days
TRECs/uL 5 24 0 0 0 2 0 21 16
Diagnostichypothesis DiGeorgeS. DiGeorgeS. SCID SCID SCID(RAG1) SCID SCID ---
---Totallymphocytes 2614 7682b 6783(57%) 5676(33%) 6364(74%) 2710a 5382(60%) 6471
CD3 953a 3773 3615(53.3%) 3321(58.5%) 3451(58.9%) 3290(51.7%) 510(24%)a 2852.5(53%) 4051(61%)
CD4 608a 954(12%) 461.9a(6.8%) 2390(42.1%) 342(5.8%)a 1591(25%) 239(11.3%)a 1954(36.3%) 2895(44%)
CD4+CD45RA+CCR7+ (naïve)
2.9a(0.6%) 5.7(0.24%)a 0.8(0.052%)a 1260(64.5%)
CD4+CD45RA−CCR7−
(peripheralmemory)
400.5(86.7%)b 1995(83.5%)b 1519(95.5%)b 216.9(11.1%)b
CD8 289a 2675b(35%) 2815(41.5%)b 257.7a(4.54%) 2220(37.9%)b 1426(22.4%) 53(2.5%)a 710.4(13.2%) 1019(15%)
CD8+CD45RA+CCR7+(naïve) 2.2(0.08%)a 0.3(0.13%)a 2.42(0.17%)a 503.7(70.9%)
CD8+CD45RA−CCR7−
(peripheralmemory)
2550(90.6%)b 165.4(64.2%) 1176(82.5%)b 26.8(3.77%)
CD16+CD56+ 343 2205(32.5%)b 1862(32.8%)b 2354.7(37%)b 171(8.1%) 904.2(16.8%) 709(11%)
CD19 1254b 441.6(6.5%)a 22.7(0.4%)a 1828(31.2%) 4.5(0.07%)a 1294(61%) 1130(21%) 1092(27%)
TRECs,T-cellreceptorexcisioncircles;DiGeorgeS.,DiGeorgesyndrome;SCID,severecombinedimmunodeficiency;RAG1,recombinationactivationgene1;CD,clusterofdifferentiation;
CCR7,chemokine(C-Cmotif)receptor7.
a Belowthe10thpercentileforBrazilianchildren.24
378 KanegaeMPetal.
2000
1500
1000
500
0
30 to 36 w eeks
37 to 42 w eeks
TRECS/
µ
L of b
lood
Figure 2 Concentration of T-cell receptor excision circles (TRECs)/L for preterm and full-term infants. TRECs were quantified by qRT-PCR in dried blood spots of 239 preterm (30---36 weeks) and 2177 full-term newborns (37---42 weeks). PretermnewbornsshowedlowerTRECsconcentrationsthanthe full-termones(237TRECs/L vs. 300TRECs/L,respectively; *p<0.05, Mann---Whitneytest).The concentrationofTRECsis showninaboxplotshowingmedian,25thand75thpercentiles, andminimumandmaximumvalues.
ROC curve
1-specificity 1.0
0.8
0.6
0.4
Sensitivity
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0
Figure3 Receiveroperatingcharacteristics(ROC)curvefor T-cellreceptorexcisioncircles(TRECs)cutoffvalueof26/L, withanareaunderthecurveof1.00.
whichresultedin0.43%(37samples)and0.03%(3samples), respectively.
Discussion
SCID resultsfrom avariety of molecular defects, andthe defectsinbothcellularandhumoralimmunityleadto sim-ilar clinical presentations. In most cases, symptoms start between the second and third months of life, and infec-tious complications arethe predominantcharacteristic of
the disease,witha preponderanceofopportunistic infec-tions (e.g., by P. jirovecii). Clinical signs are nonspecific and include respiratory tract infections, mucocutaneous candidiasis resistant to topical therapy, eczematous der-matitis,andlocalandsystemicbacterialinfections(otitis, mastoiditis,purulentrhinitisandconjunctivitis,septic dis-ease,meningitis,arthritis,andlocalabscesses).Veryoften, thefirstsign isa reactiontotheBCGvaccine, whichmay presentasalocalizedordisseminatedreaction.12Severeand recurrent infections leadto inadequategrowth. Addition-ally,intracellularparasites(Listeria,Legionella)aswellas viruses(Epstein---Barrvirusandcytomegalovirus)cancause fatalcomplications.13
Onemulticenterstudydisclosed thesevereproblem of underdiagnosis of SCID inBrazil. In 15years (1996---2010), only70caseswerediagnosedin23centerscontactedinthe country. Consideringthe probableincidence of0.17 cases of SCID per10,000 livebirths(1:58,000) andthemean of 2,900,000livebirths/yearfrom1996to2010,750casesof SCID wereexpectedin thisperiod.As only70 were docu-mented,morethan90%ofcasesoccurredwithoutadequate diagnosis.6,10
These numbers clearly show the difficulty in attaining thediagnosisofSCIDinBrazil.Aspreviouslymentioned,the signsandsymptomsarenonspecific,rangingfromcommon infectionsintheneonatalstagetogrowthdifficulties. Chil-drenborntofamilieswithpreviouscasesofSCIDcanbenefit fromthepositivehistoryandhavethepossibilityofattaining anearlydiagnosis.However,80%ofcaseshavenoprevious history6anddiagnosisoftenoccursonlywhentherecurrent infectionshavealreadyresultedinsequelae.
Duetotheurgencyindiagnosisandtreatment,thisstudy aimed to validate the TRECs quantification technique by qRT-PCRforNBSofSCIDandtoapplythetechniqueinBrazil. The results showed that after analyzing samples from 8,682newborns,acutoffvalueof26TRECs/Lwasreached, whichinvolved theretestingof0.43%ofthesamples.The techniqueaccuracywasvalidatedthroughthequantification of TRECs in five previously diagnosed cases of SCID, with resultsvarying from0to2TRECs/L(Table1).The retest rateof0.43%iswithintherangereportedintheliterature (0.20---3.26%)andcanbeconsideredan appropriatevalue, importantfortheimplementationofafull-scaletest,which preventsincreasedcostsandunnecessaryexpectationsand stress forthefamilies.14 The percentageofsamplestobe retestedisdirectlyrelatedtothecutoffvalueused,ranging from7to252TRECs/Lin thestudiesperformed todate. ThisisduetothedifferentmethodologiesusedforbothDNA extractionandforthePCRreaction.14
Thecutoffvalueobtainedforthesamples(26TRECs/L) isveryclosetothevalueusedbyBakeretal.(25TRECs/L), on which this study was based to validate the tech-nique in the present laboratory.3 It is noteworthy that this cutoff value had 100% sensitivity for detecting SCID, but recent studies have reported that several other T-lymphopenias couldalso be detected by this methodol-ogy:DiGeorgesyndrome,trisomy21,ataxia-telangiectasia, trisomy18,CHARGEsyndrome,andcardiacabnormalities, amongothers.6
adjustedgestationalageof37weeks.7,15Thus,theseresults are consistent with the international literature and were validatedbypositivediseasecontrols.
TRECs quantificationby RT-PCRwasappliedona small scale and had an estimated cost of US$ 4 per sample in thisstudy.Thisvalue,althoughitonlyconsidersthecostsof reagents,canbecomparedtothecostofNBSforcongenital adrenal hyperplasia(CAH),calculatedaccording toapilot studyconductedin thestateof Goiás,of US$7.16 Consid-ering thenumber oflivebirthsin Brazilin 2013of nearly 3millionchildren,17 thetotalcostwouldbeapproximately US$ 12 million, less than the NBS for CAH, a pathol-ogy recently included in the National Neonatal Screening Program.18Itisnoteworthythatitisnecessarytoadd addi-tionalcosts (active search andconfirmatory tests)to this valueandonalargescale,thisvaluetendstodecrease.
Among theT-lymphopeniaswiththepossibilityofbeing diagnosed through the quantification of TRECs, SCID are undoubtedlythemostsevere. Mostchildren withSCID are not diagnosed until several severe infections have mani-fested,orthechildshowsfailuretothriveand,unlessthere isafamilyhistoryofSCID,thediagnosisisoftendelayedand chancesofacurearediminished.Moreover,anirrefutable argumentfortheinclusionofSCIDinneonatalscreeningis thefactthatSCIDaretheonlyconditionsidentifiedthrough neonatalscreeningthatcanbecuredbytreatmentwhenthe diagnosisismadeatanearlystage.19
Hematopoieticstemcelltransplantation(HSCT)is cura-tive and is available in Brazil.5 When carried out before 3.5monthsoflife,itresultsina95%survivalrate;afterthat age,long-termsurvivaldecreasesto60---70%,andthe inci-dence of infectious complications and sequelae increases dramatically.20EvenworseconsequencesoccurwhenHSCT iscarriedoutwithactiveinfectionsduringtheprocedure: thesurvivalratedecreasesto50%,againshowingthatearly diagnosissubstantiallyimprovestheoutcome.14,20
Regarding theeconomicaspects,itis alsonecessary to considerthecostsofHSCTandofcomplicationsfromseveral infectionstowhichpatientswithSCIDaresubject.Several studieshavecomparedthecostsofearlyvs.lateHSCT:the full early treatment, performed up to3.5 months of age (before the infections occur) costs up to four times less thanwhenperformed afterthatage (US$365,785vs.US$ 1.43million).21Whenconsideringonlythecostofthe trans-plantation,thedifferencewasUS$120,000vs.US$360,000 when HSCT was performed before and after 3.5 months of age, respectively.22 These values, calculated for the UnitedStates,showthegreatbenefitofneonatalscreening for SCID to the detriment of high costs resulting from late diagnosis and the complications that this delay may cause.21
When analyzing HSCT values beforeand after the age of 3.5 months,there is an approximatecost reductionof US$ 240,000when thetransplantation is performed early. Considering the cost obtained for this study of US$ 4, it wouldbepossibletoscreenapproximately60,000children. Thus,the introduction ofthis test ona large scale would practicallypay for itself,asthe costreductiongenerated withthediagnosis ofa child withSCID referred toearlier HSCTwould coverthecoststoperformthetestsrequired todiagnoseotherchild(whenconsideringtheincidenceof 0.17/10,000).
Itshouldbenotedthatthedatapresentedhereinreflect theeconomic costsin theUS anditis necessary for cost-benefitstudies tobeconducted inBrazil, considering the Brazilianpublichealthsystem.
The implementation of the newborn screening test for SCID is increasing worldwide. Several countries have included SCID in their routine newbornscreening or have ongoingpilotstudies(UnitedStates,Canada,Iran,Taiwan, Israel,Spain,France,Sweden,andtheUnitedKingdom).19,23 TheimplementationasaroutineinBrazilcouldsignificantly improve the aforementioned tragic scenario, without the needforanewplatform.
TheapplicationofquantificationofTRECsinthe neona-talscreeningof 8,682newbornsresulted inacutoffvalue of26TRECs/L,witharetestratesimilartothatin inter-nationalstudies. This study showedthat the technique is feasible and can be implemented on a large scale after technicaltrainingoftheinvolvedteams.
Funding
This work was funded by FAPESP, CNPq, and Baxter Bio-science.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The authorswould liketothank thevolunteers, patients, andtheirfamilieswhoagreed toparticipateinthe study. TheyalsothankDr.John RoutesandDr.MeiBaker forthe training, Dr. Daniel Douek for the donated plasmids, the employees of the participating hospitals and clinics, and APAE-SPemployeesforhelpingwiththenecessarydata.
Appendix.
Supplementary
data
Supplementary data associated with this article can be found, in the online version, at doi:10.1016/j.jped.
2015.10.006.
References
1.BuckleyRH.Moleculardefectsinhumanseverecombined immu-nodeficiencyand approachestoimmunereconstitution.Annu RevImmunol.2004;22:625---55.
2.DvorakCC,CowanMJ,LoganBR,NotarangeloLD,GriffithLM, Puck JM, et al. The natural history of children withsevere combinedimmunodeficiency:baselinefeaturesofthefirstfifty patientsoftheprimaryimmunedeficiencytreatment consor-tiumprospectivestudy6901.JClinImmunol.2013;33:1156---64.
3.BakerMW,GrossmanWJ,LaessigRH,HoffmanGL,BrokoppCD, KurtyczDF,etal.Developmentofaroutinenewbornscreening protocolforseverecombinedimmunodeficiency.JAllergyClin Immunol.2009;124:522---7.
380 KanegaeMPetal.
5.BorteS,vonDobelnU,FasthA,WangN,JanziM,WiniarskiJ, etal.Neonatalscreeningforsevereprimaryimmunodeficiency diseases using high-throughput triplex real-time PCR. Blood. 2012;119:2552---5.
6.Kwan A, Abraham RS, Currier R, BrowerA, AndruszewskiK, AbbottJK,etal.Newbornscreeningforseverecombined immu-nodeficiency in 11screening programs in the UnitedStates. JAMA.2014;312:729---38.
7.BakerMW,LaessigRH,KatcherML,RoutesJM,GrossmanWJ, VerbskyJ,etal.Implementingroutinetestingforsevere com-binedimmunodeficiencywithinWisconsin’snewbornscreening program.PublicHealthRep.2010;125Suppl.2:88---95.
8.Carneiro-Sampaio M, Moraes-Vasconcelos D, Kokron CM, JacobCM,Toledo-BarrosM,DornaMB,etal.Primary immuno-deficiencydiseasesindifferentagegroups:areporton1,008 casesfromasingleBrazilianreferencecenter.JClinImmunol. 2013;33:716---24.
9.Dantas EO, Aranda CS, Rego Silva AM, Tavares FS, SeveroFerreiraJF, de Quadros Coelho MA, et al. Doc-tors’ awareness concerning primary immunodeficiencies in Brazil.AllergolImmunopathol(Madr).2015;43:272---8.
10.Mazzucchelli JT, Bonfim C, Castro GG, Condino-Neto AA, Costa NM, Cunha L, et al. Severe combined immuno-deficiency in Brazil: management, prognosis, and BCG-associated complications. J Investig Allergol Clin Immunol. 2014;24:184---91.
11.Douek DC, Vescio RA, Betts MR, Brenchley JM, Hill BJ, Zhang L, et al. Assessmentofthymic outputinadults after haematopoieticstem-celltransplantationandpredictionof T-cellreconstitution.Lancet.2000;355:1875---81.
12.RoutesJ,AbinunM,Al-HerzW,BustamanteJ,Condino-NetoA, DeLaMorenaMT,etal.ICON:theearlydiagnosisofcongenital immunodeficiencies.JClinImmunol.2014;34:398---424.
13.DeVillartayJP,SchwarzK,VillaA.V(D)Jrecombinationdefects. In:OchsHD,EdvardSmithCI,PuckJM,editors.Primary immu-nodeficiencydiseases:amolecularandgeneticapproach.2nd ed.NewYork:OxfordUniversityPress;2007.p.153---68.
14.van der Spek J, Groenwold RH, van der Burg M, vanMontfransJM.TREC based newborn screeningfor severe
combined immunodeficiency disease: a systematic review. J ClinImmunol.2015;35:416---30.
15.WardCE,BaptistAP.Challengesofnewbornseverecombined immunodeficiency screeningamong premature infants. Pedi-atrics.2013;131:e1298---302.
16.Silveira EL [Thesis] Hiperplasia adrenal congênita no Brasil: incidência,custos datriagemneonataleaplicac¸ãoclínicada biologiamolecular.PortoAlegre,RS:UniversidadeFederaldo RioGrandedoSul;2005.
17.IBGE. Estatísticas de Registro Civil; 2013. Available from:
http://www.ibge.gov.br/home/estatistica/populacao/ registrocivil/2013/defaultxls.shtm[cited18.09.15].
18.Brasil.MinistériodaSaúde.PortariaN◦2.829,de14de dezem-brode2012.
19.GasparHB,HammarstromL,MahlaouiN,BorteM,BorteS.The casefor mandatory newborn screening for severe combined immunodeficiency(SCID).JClinImmunol.2014;34:393---7.
20.Puck JM. Population-based newborn screening for severe combinedimmunodeficiency:stepstowardimplementation.J AllergyClinImmunol.2007;120:760---8.
21.Kubiak C,Jyonouchi S, Kuo C, Garcia-Lloret M, Dorsey MJ, SleasmanJ,etal.Fiscalimplicationsofnewbornscreeningin thediagnosisofseverecombinedimmunodeficiency.JAllergy ClinImmunolPract.2014;2:697---702.
22.Chan K, Davis J, Pai SY, Bonilla FA, Puck JM, Apkon M. A Markovmodel to analyzecost-effectiveness of screeningfor severecombinedimmunodeficiency(SCID).Mol GenetMetab. 2011;104:383---9.
23.OlbrichP,deFelipeB,Delgado-PecellinC,RoderoR,RojasP, AguayoJ,etal.Afirstpilotstudyontheneonatalscreening of primary immunodeficiencies in Spain: TRECS and KRECS identifysevereT-andB-celllymphopenia].AnPediatr(Barc). 2014;81:310---7.