www.jped.com.br
ORIGINAL
ARTICLE
Colonic
transit
in
children
and
adolescents
with
chronic
constipation
夽
,
夽夽
Rafael
L.M.L.
Carmo
a,
Raquel
P.M.
Oliveira
a,
Antonio
E.A.
Ribeiro
a,
Mariana
C.L.
Lima
b,
Bárbara
J.
Amorim
b,
Antonio
Fernando
Ribeiro
c,
Celso
D.
Ramos
b,
Joaquim
M.
Bustorff-Silva
d,
Elizete
A.
Lomazi
c,∗aSchoolofMedicalSciences,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
bDepartmentofRadiology,SchoolofMedicalSciences,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
cDepartmentofPediatrics,SchoolofMedicalSciences,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil dDepartmentofSurgery,SchoolofMedicalSciences,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
Received9July2014;accepted22October2014 Availableonline15May2015
KEYWORDS Children; Adolescents; Constipation; Diagnosis
Abstract
Objective: Theaimofthisstudywastoassessclinicalfeaturesandcolonictransitpatternsin
Brazilianchildrenwithrefractoryconstipation.
Methods: From2010to 2013,79 constipatedpatients received follow-upcareina tertiary
hospital.Ofthesepatients,28(aged8---14years)wererefractorytoconventionaltherapyand underwentasimplifiedvisualmethodofnuclearcolonictransitstudy,byingestionofaliquid mealcontaining9.25MBq/kgof99mTc-phytate.Abdominalstaticimagesweretakenimmediately andattwo,six,24,30,and48hafteringestionfor qualitativeanalysisoftheradiomarker progressionthroughthecolon.
Results: Twopatternsofcolonictransit werefound:slowcolonictransit(SCT,n=14),when
imagesat48hshowedalargerpartofthetracerremainedinproximalandtransversecolon, anddistalretention(DR,n=14),whenafter30h,theradioisotopepassedthetransversecolon andwasretainedintherectosigmoidupto48h.TheSCTandDRgroupincluded,respectively, nineandtenmales;medianagesinthenuclearstudy of11and10years,p=0.207;median durationofconstipationofsevenandsixyears,p=0.599.Constipationappearingduringfirst yearage (p=0.04) andreportofsoft stools(p=0.02) were morecommon inSCT patients. PalpableabdominalfecalimpactionwasfoundonlyinDRgroup.Appendicostomyforantegrade continenceenemawassuccessfulin4/12(30%)ofSCTpatients(medianfollow-up:2.4years).
夽 Pleasecitethisarticleas:CarmoRL,OliveiraRP,RibeiroAE,LimaMC,AmorimBJ,RibeiroAF,etal.Colonictransitinchildrenand
adolescentswithchronicconstipation.JPediatr(RioJ).2015;91:386---91.
夽夽StudyconductedatHospitaldeClínicas,FaculdadedeCiênciasMédicas,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,
Brazil.
∗Correspondingauthor.
E-mail:[email protected](E.A.Lomazi).
http://dx.doi.org/10.1016/j.jped.2014.10.007
Conclusion: Nucleartransitstudydistinguishedtwocolonicdysmotilitypatternsandwasuseful forguidingrefractorypatientstospecifictherapies.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Crianc¸as;
Adolescentes; Constipac¸ão; Diagnóstico
Trânsitointestinalemcrianc¸aseadolescentescomconstipac¸ãocrônica
Resumo
Objetivo: Oobjetivodesteestudofoiavaliarascaracterísticasclínicaseospadrõesdetrânsito
colônicoemcrianc¸asbrasileirascomconstipac¸ãorefratária.
Métodos: De2010a2013,79pacientesconstipadosreceberamacompanhamentoemum
hos-pitalterciário.Dessespacientes,28(comidadeentre8---14anos)foramidentificadoscomoe realizaramestudonecleardotrânsitocolônicopormétodovisualsimplificado,comingestão deumarefeic¸ãolíquidacontendo9.25MBq/Kgdefitato−99mTc.Imagensestáticasabdominais foramtomadasimediatamenteeem2,6,24,30e48horasapósaingestãoparaumaanálise qualitativadaprogressãodomarcadorradioativopelocólon.
Resultados: Foramencontradosdoispadrõesde trânsitointestinal: trânsito intestinallento
(STC,N=14),quandoasimagensde48horasmostraramquegrandepartedomarcador per-maneceunocólonproximaletransverso,eretenc¸ãodistal(DR,N=14),quando,após30horas, o radioisótopo haviapassado ocólontransverso epermaneceu retido noretossigmoide até 48horas.OgrupoSTCeogrupoDRincluíram,respectivamente,9e10meninos;idademédia nomomentodo:11e10anos,p=0.207;durac¸ãomédiadeconstipac¸ão:7e6anos,p=0.599. Sintomasdeconstipac¸ãoduranteoprimeiroanodei(p=0.04)erelatosdefezes(p=0.02)foram maiscomunsempacientescomSTC.Observou-seimpactac¸ãofecalpalpávelnoabdomen ape-nasnogrupoDR.Aapendicostomiaparaenemaanterógradofoibem-sucedidaem4/12(30%) pacientescomSTC(acompanhamentomédio:2.4anos).
Conclusão: Oestudonucleardotrânsitocolônicodiferencioudoispadrõesdedismotilidadee
foiútilparaorientarterapiasespecíficasparapacientesrefratários.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Constipation is a common complaint in children and improvementisseeninthemajorityofpatientswhoadhere totreatmentrecommendedbyconsensusguidelines, includ-ing osmotic laxatives and intake of a fiber-rich diet.1 However,inapproximatelyone-thirdofchildren,symptoms aremoreintenseandthereisrefractorinesstoregular ene-masandmaximumdosesoflaxatives.2Theconstipationmay besevereenough toresultincomplete cessationof spon-taneousbowelmotions.3 Toexplainsuchaclinicalcourse, themain hypothesisis colonictransitdysfunction.Studies ofcolonicmotorfunctioninpediatricpatientswith refrac-tory constipation have recorded dysfunctionalpatternsof colonictransit.4Recentstudiessuggestthatseverechronic constipation in children may be due to slowed colonic transit; different patterns of delayed transit have been described4---6 andspecific therapies have beensuccessfully proposed.7
There is a lack ofdata onrole ofcolonic transit stud-iesinclinicalpractice,mainlyconcerningitsreproducibility indifferentpopulations,standardizationoftechnical proce-dures,andpurposeforinvestigatingrefractoryconstipation. Theaimofthecurrent studywastogrouprefractory con-stipatedpatientsaccordingcolonictransitpattern,usinga simplifiedmethodofnucleartransitstudy(NTS).
Case
study
and
methods
FromSeptember2010toDecember2013,79patients diag-nosed with functional constipation according to Roma III criteria8 received tertiary outpatient follow-up care in a pediatricgastroenterologyunitat theUniversityof Camp-inasMedicalSchoolHospitalinSãoPaulo,Brazil.Ofthese, 28 patients (aged 8---14 years; ages at the time of NTS) wereidentifiedasrefractorytoconventionaltherapy,after aprospectivefollow-upof2.8±1.7years(mean±SD).This groupparticipatedinacolonictransitstudy,afterwritten informedconsenttermwasobtainedfromtheparents/legal guardiansandpatients.Themaindemographic characteris-ticsof28childrenwithclinicalrefractorinessincludedmale gender (n=19) and median duration of symptoms longer thanfiveyears(rangingfrom2to12years).
cramps;expressed signs of osmotic intolerance;and con-sumed18goffibers/day(one-halfcupofFibraMais®,Nestlé,
Brazil).Adherencetotherapyandclinicalfeatureson cons-tipation symptoms were systematically evaluated during last6monthsbeforecolonictransitstudy,byweekly tele-phone contactand clinical consultation every 15 days. If thepediatricgastroenterologistwasuncertainregardingthe presenceof retentivesoiling, a plainabdominal radiogra-phy wastaken toconfirm or exclude fecal impactionand Barr score9 was defined. Adherence to treatment was an inclusioncriterion.
Aftermedicalhistoryandphysicalexamination, anorec-tal manometry and barium enema were performed for excludingHirschsprungdiseaseandotherorganiccausesof constipation.Anorectal manometry wasperformed witha continuousperfusionsystem,andalow-complacency pneu-matic hydraulic system of continuous capillary perfusion (Arndorfer,Inc.,WI,USA),interfacedwithacomputerized systemusingcommerciallyavailable software(Gastrosoft, PolygramLowerGI,version6.4and,Windows,Synetics Medi-cal Inc., TX, USA and Dynapack MPX 816, Dynamed, SP, Brazil)andan8-channelaxialmanometryprobe(Dynamed Pro-lifetechnology,Prolifetechnology,SãoPaulo,SP,Brazil). NTSwasperformed during afour-dayadmission period scheduled exclusively for this purpose. Laxatives were discontinuedfivedaysbeforehospitaladmission.Rectal dis-impaction was performed by rectal infusion of 20mL/kg of 12% glycerin solution, at a maximum dose of 500mL. Anorectal manometry was performed after rectal disim-paction.Normalmanometry valueswereconsidered those reportedbyKumaretal.10Then,patientsremained12hwith no medication, maintaining a normal diet and activities. On the morning of the first day, a liquid meal contain-ing9.25 MBq/kg(amaximumof370MBq)of99mTc-phytate
diluted in 20mL of milk was ingested. Static images of theanteriorabdominalviewweretakenimmediatelyafter radioactivedrugingestionandaftertwo,six,24,30and48h. Imagesacquiredimmediatelyandattwoand6hafterdrug ingestion were used toassess gastric emptying and small boweltransit.Imagesacquiredbetweensixand48hallowed assessmentofcolonictransit.
Colonic transitanalysiswasbasedonqualitative visual assessment of the images acquired at each time interval and considering progression of the radioisotope through the colon. Two nuclear medicine physicians reviewed the NTSimageswhile blinded toclinicaldetails. Images were groupedby visualanalysis; classificationwasaccording to appearanceoftheactivitypatternwithinthecolonatsix, 24,30and48h.Twotypesofcolonicmotorpatternswere found:thefirstwastermedslowcolonictransit(SCT)when thetracerinthemainremainedintheproximaland trans-verse colon, at 48-hour scans. The second pattern was classifiedasdistalretention(DR)whentheradioisotopehad passedthetransversecolonat30hafterthestudy,but per-sistedintherectosigmoidregionupto48h.
Age,durationofconstipation,follow-uptimebeforeNTS, andclinical featuresin thegroups were comparedbythe Mann---Whitneytest,andPearson’schi-squaredtestwasused tocompareclinicalfeaturestest.p-values<0.05were con-sideredsignificant.
This research project was presented to the Research EthicsCommittee of theUNICAMP School of Medicine, on
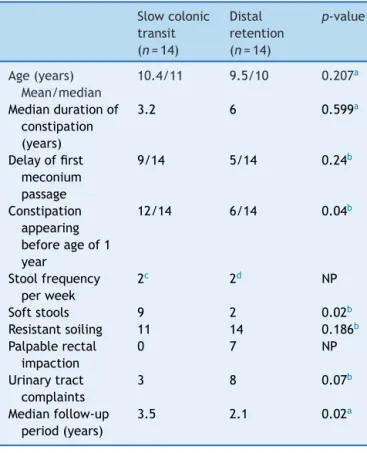
Table1 Comparisonoftheclinicalfeaturesin28patients managedinaspecializedoutpatientfacilitywithrefractory constipation and presenting with two patterns ofcolonic transit scintigraphy: slow colonic transit (SCT) and distal retention(DR).
Slowcolonic transit (n=14)
Distal retention (n=14)
p-value
Age(years) Mean/median
10.4/11 9.5/10 0.207a
Mediandurationof constipation (years)
3.2 6 0.599a
Delayoffirst meconium passage
9/14 5/14 0.24b
Constipation appearing beforeageof1 year
12/14 6/14 0.04b
Stoolfrequency perweek
2c 2d NP
Softstools 9 2 0.02b
Resistantsoiling 11 14 0.186b
Palpablerectal impaction
0 7 NP
Urinarytract complaints
3 8 0.07b
Medianfollow-up period(years)
3.5 2.1 0.02a
NP,notperformed.
a Mann---Whitneytest. b Pearson’schi-squaredtest. c n=6.
d n=2.
4/16/2010andapprovedbyprocess322/2010,CAAEnumber 02450146000-10,on4/27/2010.Asignedinformedconsent from patients and legal guardians was required to fulfill inclusioncriteriainthestudy.
Results
NTSshowedtwomotordysfunctionpatterns:isotope reten-tion in the proximal colon (SCT group, n=14) or in the rectosigmoid region (DR group, n=14). Clinical data are shown at Table 1. The SCT and DR groups showed fol-lowing characteristics, respectively: nine and ten males; medianageatthetimeofNTSof11and10years,p=0.207, Mann---Whitney; median duration of constipation accord-ingdata recordedin medicalhistory, seven andsixyears,
p=0.599,Mann---Whitney;andmediandurationoffollow-up atthespecializedserviceuntiltheperformanceofNTS,3.5 and2.2years,p=0.02,Mann---Whitney.Constipation symp-toms appearing during first year age and report of soft stools were more common in SCT patients (p=0.04 and
S
R
S
0h
A
B
2h 6h
24h 30h 48h
R
24h 30h 48h
0h 2h 6h
Figure1 Scintigraphicimagesofboweltransit inapatient exhibiting motor pattern defined as slow colonic transit (A) anddistalretention(B). (A)Theprogressoftheradioisotope isobservedforaperiodof48h:stomach(S,0h),smallbowel (2h),cecumandascendingcolon(6h).Theimageat24hshows thatalmostalltheradioactivematerialisdistributed through-outtheentire colon.Theslowtransitpatternisconfirmedin thefollowing images (30hand48h), withminimumprogress ofthematerialtotherectum(R). (B)Nuclearcolonictransit withretentionpatternintherectosigmoidregion.After admin-istration ofthe material,the stomach (S), smallbowel, and ascendingcolonaresequentiallyimagedatzero,two,and6h, respectively.Progressoftheradioisotopethroughoutthecolon isclearlyseeninscansat24and30h.At48h,thematerialis retainedintherectum(R),withalmostnoradioactivity remain-inginthecolon.
NTS was well tolerated and no adverse events were observed.Twospecialistsinnuclearmedicinereviewedthe images, separately. Inter-observer reliability with kappa coefficient was 0.727, p<0.001. Photographs of the two colonictransitpatterns(SCTandDR)areshowninFig.1.
BeforeNTS,allsubjectsunderwentanorectal manome-try.Rectoanalinhibitoryreflexwasidentifiedinallpatients; other parameters were unable to differentiate groups. Patients in both groups referred hyposensitivity during balloon insufflationwithvolumes from20mLto 60mL in-rectum,andmostchildren referredballooninsufflationas imperceptible. There are no differences between groups considering anal sphincter length, maximum resting pres-sure,andmaximumsqueezepressure.
Bariumenemaofpatientsshowednostrictureor malfor-mation.
Duringthe study,64 plainabdominalradiographs were takentoinvestigatefecalimpaction.Barrscoreswere cal-culated toassess severity of stool retention. Radiographs wereretrospectivelyreviewedbytwopediatricradiologists andcorrelatedtoNTSreports.Theagreementbetweenpairs ofobserverswasassessedbythekappacoefficientandwas good for the Barr score: 0.59. There was no association betweenstoolretentionseverityandNTSimages,p=0.08, test.
TwelvepatientswithSCTunderwenttoappendicostomy. Soilingwaspreventedinallcasesandfourpatients recov-ered spontaneous bowel passage without using laxatives, afteramedianfollow-upperiodof2.4years(min:1.9years; max:2.6years),theotherscontinuedtorequirestomafor antegradecleansingenemas,medianfollow-upperiod:1.5 years (min: 1.3 years; max: 4.9 years). During the same follow-up period, no DR patients recovered spontaneous bowelmovementswithoutlavage.
Discussion
Toallowforcomparisonsandreproducibilityofclinical tri-als,researchstudiesofnewtherapiesordiagnostictestsin pediatricpatientswithconstipationmustbecarefulto spec-ify thetype ofpatient tested, sinceconstipation is nota disease,butratherasymptomwithdifferentdeterminative factors. The pediatric population of constipated patients consistsofaheterogeneousgroup,ranginginage,severity, anddurationofsymptoms.Untilnow,aconsensusdefinition ofrefractoryconstipationhasnotbeendefinedin interna-tional guidelines;this representsone of the most widely foundclinicalpresentationsofconstipationinpediatric ter-tiarycenters.
Consideringthatcolonictransitdysfunctionispresentin 60%ofchildrenwithrefractoryconstipation4andthat spe-cifictherapieshavebeenproposedfordysfunctionalcolonic patterns,11 it would be useful to distinguish them on a clinicalbasis.Aretrospectivestudycorrelatedconstipation symptomswith transit times to determine clinical differ-encesbetweenSCTandDR,authorsconcludedthatthiswas notpossibleonasymptomaticbasis.12However,despitethe factthatthefrequency ofeachsymptomis notenough to definethetransitpattern,somecomplaintsarefoundmore commonly in SCT patients: soft stools despite infrequent bowelmovements;delayedpassageofmeconium;veryearly onset of constipation, generally during first year of life; andabsenceof ahardpalpablestool massondistal colon and rectum sigmoid.11---13 The clinical picture of the cur-rentlyexaminedgroupsdidnotallowdistinctionofcolonic patterns, despite the fact that reports of soft stoolsand earlyonsetconstipationweremorefrequentinSCT.Reports onstoolfrequency in thecurrent groups were considered a weak symptom for differentiation purposes, since most ofpatientswereprescribedcleansingenemasonaregular basis.
timewithradiopaquemarkersinchildren;norelationwas found.14
Colonic motilityNTSperformed in healthyindividuals15 demonstratedthat theproximalanddistalportionsofthe colon have different motor functions. The radioisotope persists in the ascending colon for up to 12h. At 24h, radioactivity is equally distributed among the ascending colon,transversecolon,anddistalportionofthebowel.At 48h, mostof thetracerhasalreadybeen evacuated. The transverse colon appears tofunction asa reservoir, while theleftcolonperformsasaconduit.Camilleri&Zinsmeister concludedthatevaluation ofcolonicsegmenttransittime within24h afterthe testhas ahigh sensitivityfor detec-tionofcolonicmotordisorders,sincetheemptyingrateof theproximalcolonissignificantlydifferentbetweenhealthy andconstipatedindividuals.16
Studies oncolonicmotor function inpediatric patients withrefractoryconstipationhave recordednormalor dys-functionalpatternsofcolonictransit.Yiketal.4identified patientswithnormalcolonictransit(noevidenceofcolonic dysmotility), anorectal retention, rapid proximal colonic transit(rapidtransitthroughproximalcolonat6and24h), andslowproximalcolonictransit.Onestudyobserveda pre-dominanceofslowtransitpatients.17Anotherdemonstrated ahigherpercentageofchildren withDR.18 Thisvariability mayberelated todifferencesin criteriatosendpatients for test (initial reports only sent patients without fecal retention)19;techniquefortheperformanceofNTS, involv-ingpreparationofthepatient,andtypeandmodeofmeal ingestion;andfinally,differencesinphasesofimage acqui-sition.Thecurrent studyprescribedacleansingenemafor fecal impaction before the NTS; this decision was based onthe understanding that a hard fecal mass could inter-ferewithgastrointestinaltransitstudies,sincechildrenwith hard fecal mass usually avoid stool passage due to pain or discomfort.20,21 Other researchers have not performed rectaldisimpactionbeforethetest.Studiesonconstipated adultsdidnotconfirmarelationbetweenrectalevacuation andcolonictransittime.22
To thebestofthe authors’knowledge,NTSis not per-formedinBrazilianhealth centers,sotheseresultscannot representageneralpatterninBrazilianchildren,and cer-tainly the choice of children sent to scintigraphy may interferewiththepatternsfoundinthisstudy.Theauthors only considered such an evaluation on a research basis becauseonlythemostseverecasesinfollow-upwere stud-ied.Aclinicalconsensusguidelineisrequired.
The colonictransitpatternsfoundherein werevisually identified.Reproducibilityof visual evaluationof patterns ofcolonictransitwaspreviously demonstrated,aswell as highratesofinter-observeragreement.Visualevaluationof nuclearimageswascomparedtoanalysisofthegeometric center.23 Visual inspection was considered adequate for general appreciation of transit pattern, while analysis of thegeometriccenterindicatesthesiteofgreatestintensity of the radioisotope, but does not permit a clear view of transit,failures, andretropulsive movements that canbe assessed by the visual technique.23 In clinical practice, visualassessment maybeadequate for groupingpatients. Asusersofsuchnuclearmethodology,theauthorstriedto proposeamorepractical andlowcosttechniquefordaily use in most of centers with a nuclear medicine service.
Camilleri & Zinsmeister16 described that slow colonic transitmaybediagnosed24hafterradioisotopeingestion. Inpractice,imagesassessedbetween24and48hwerealso consideredthebestindexfordiagnosisinclinicaltrials.24
Different therapies have been recommended to SCT and DR patients. While patients with DR are counseled to maintain the use of oral laxatives and supplemental intakeofdietaryfiber,therapeuticproposalsforslowtransit patientsincludemainlysurgicaltreatment,moreusuallyby appendicostomy for theperformance of anterograde ene-mas and a new technique with transcutaneous electrical stimulation.3,7,25,26 The authorstreated asmallnumber of patientssurgicallyandtheirevolutionmightbeconsidered relatively better than those with DR on drug therapy, in terms of achieving spontaneous stool passage. In a study onresistantpediatric constipation,80patientsunderwent the Malone procedure and the authors found 12 children were able cease use of appendicostomy becauseof reso-lution of their symptoms; the probability of the child to stopcoloniclavagewas20%6.2yearsafterconstructionof thestoma;however,colonictransitpatternswerenot con-sidered beforesurgicaltreatment inmost patients.27 King etal., however,found that antegradecontinence enemas weresuccessfulin34(81%)of42childrenwithradiologically provenSCT.28
Inconclusion,thisstudyshowedsimilarresultstothose conducted in other pediatric populations, a relevant fact for its eventual application in Brazilian children.29 These resultscorroboratethepotentiallyrelevantroleoftheNTS asaguideinclinicalpracticeformanagementofconstipated patientsrefractorytoconventionaltherapy.
Funding
This study obtained financing support from the FAEPEX (FundodeApoioaoEnsino,àPesquisaeExtensão)da UNI-CAMP,Solicitationnumber:149/09.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.TabbersMM,DiLorenzoC,BergerMY,FaureC,LangendamMW, NurkoS,etal.Evaluationandtreatmentoffunctional constipa-tionininfantsandchildren:evidence-basedrecommendations fromESPGHAN and NASPGHAN.JPediatrGastroenterolNutr. 2014;58:258---74.
2.BongersME,vandenBergMM,ReitsmaJB,VoskuijlWP,Benninga MA.Arandomizedcontrolledtrialofenemasin combination withorallaxativetherapyforchildrenwithchronic constipa-tion.ClinGastroenterolHepatol.2009;7:1069---74.
3.WongSW,LubowskiDZ. Slow-transitconstipation: evaluation andtreatment.ANZJSurg.2007;77:320---8.
4.YikYI,CookDJ,VeyseyDM,RutkowskiSJ,TudballCF,BrookeS, etal.Targetingthecausesofintractablechronicconstipationin children:thenucleartransitstudies(NTS).In:SinghN,editor. Radioisotopes-applicationsinbiomedicalscience.Manhattan, NY:InTechOpenAccessPublisher;2011.p.305---20.
constipationrevealasubgroupwithrapidproximalcolonic tran-sit.JPediatrSurg.2011;46:1406---11.
6.DinningPG,DiLorenzoC.Colonicdysmotilityinconstipation. BestPractResClinGastroenterol.2011;25:89---101.
7.SouthwellBR.Treatmentofslowtransit constipationin chil-dren.JPediatrGastroenterolNutr.2011;53:S51---3.
8.RasquinA,DiLorenzoC,ForbesD,GuiraldesE,HyamsJS, Sta-ianoA,etal.Childhoodfunctionalgastrointestinal disorders: child/adolescent.Gastroenterology.2006;130:1527---37.
9.Barr RG, Levine MD, Wilkinson RH, Mulvihill D. Chronicand occultstoolretention:aclinicaltoolforitsevaluationin school-agedchildren.ClinPediatr(Phila).1979;18:674---9.
10.KumarS,RamadanS,GuptaV,HelmyS,AttaI,AlkholyA. Mano-metric testsof anorectal function in 90healthy children: a clinicalstudyfromKuwait.JPediatrSurg.2009;44:1786---90.
11.HutsonJM,Chase JW, Clarke MC, King SK, Sutcliffe J, Gibb S,etal.Slow-transitconstipationinchildren:ourexperience. PediatrSurgInt.2009;25:403---6.
12.ShinYM,SouthwellBR,StantonMP,HutsonJM.Signsand symp-tomsofslow-transitconstipationversusfunctionalretention.J PediatrSurg.2002;37:1762---5.
13.HutsonJM,McNamaraJ,GibbS,ShinYM.Slowtransit consti-pationinchildren.JPaediatrChildHealth.2001;37:426---30.
14.CunhaTB,TahanS,SoaresMF,LedermanHM,MoraisMB. Abdom-inalradiographintheassessmentoffecalimpactioninchildren withfunctionalconstipation:comparingthreescoringsystems. JPediatr(RioJ).2012;88:317---22.
15.ProanoM,CamilleriM,PhillipsSF,BrownML,Thomforde GM. Transitofsolidsthroughthehumancolon:regional quantifica-tionintheunpreparedbowel.AmJPhysiol.1990;258:G856---62.
16.CamilleriM,ZinsmeisterAR.Towardsarelativelyinexpensive, noninvasive,accuratetestforcolonicmotilitydisorders. Gas-troenterology.1992;103:36---42.
17.Sutcliffe JR, King SK, Hutson JM, Cook DJ, Southwell BR. Gastrointestinaltransitinchildrenwithchronicidiopathic cons-tipation.PediatrSurgInt.2009;25:465---72.
18.MugieSM,PerezME,BurgersR,HingsbergenEA,PunatiJ,Mousa H, et al. Colonic manometry and colonic scintigraphy as a
diagnostictoolforchildrenwithsevereconstipation.JPediatr GastroenterolNutr.2013;57:598---602.
19.CookBJ,LimE,CookD,HughesJ,ChowCW,StantonMP,etal. Radionucleartransittoassesssitesofdelayinlargebowel tran-sitinchildrenwithchronic idiopathicconstipation.JPediatr Surg.2005;40:478---83.
20.Devanarayana NM, Rajindrajith S. Bowel habits and behav-iors related to defecation in 10- to 16-year-olds: impact of socioeconomiccharacteristicsandemotionalstress.JPediatr GastroenterolNutr.2011;52:569---73.
21.Tjeerdsma HC, Smout AJ, Akkermans LM. Voluntary sup-pression of defecation delays gastric emptying. Dig Dis Sci. 1993;38:832---6.
22.KarlbomU,PåhlmanL,NilssonS,GrafW.Relationshipsbetween defecographic findings, rectal emptying, and colonic transit timeinconstipatedpatients.Gut.1995;36:907---12.
23.FreedmanPN,GoldbergPA,FataarAB,MannMM.Acomparison ofmethodsofassessmentofscintigraphiccolontransit.JNucl MedTechnol.2006;34:76---81.
24.MaurerAH,ParkmanHP.Updateongastrointestinal scintigra-phy.SeminNuclMed.2006;36:110---8.
25.YikYI,LeongLC,HutsonJM,SouthwellBR.Theimpactof tran-scutaneouselectricalstimulation therapyonappendicostomy operationratesforchildrenwithchronicconstipation–a single-institutionexperience.JPediatrSurg.2012;47:1421---6.
26.YikYI,Ismail KA,HutsonJM,SouthwellBR. Home transcuta-neouselectricalstimulationtotreatchildrenwithslow-transit constipation.JPediatrSurg.2012;47:1285---90.
27.JaffrayB.Whathappenstochildrenwithidiopathic constipa-tionwhoreceiveanantegradecontinentenema?Anactuarial analysisof80consecutivecases.JPediatrSurg.2009;44:404---7.
28.King SK, Sutcliffe JR, Southwell BR, Chait PG, Hutson JM. Theantegradecontinenceenemasuccessfullytreatsidiopathic slow-transitconstipation.JPediatrSurg.2005;40:1935---40.